


Introduction
The death of a loved one is a profoundly painful experience and is widely regarded as one of the most stressful events in an individual’s life (Noone Reference Noone2017). Grief, a universal response to loss, is defined as a psychological and physical reaction that may manifest in cognitive, behavioral, and somatic symptoms (Shear Reference Shear2015). The immediate aftermath of a loss is often marked by a disruption in emotional regulation, which gradually gives way to a process of adaptation (Maciejewski et al. Reference Maciejewski, Zhang and Block2007; Szuhany et al. Reference Szuhany, Malgaroli and Miron2021). However, not all individuals respond in the same way; different trajectories of grieving have been identified (Nielsen et al. Reference Nielsen, Carlsen, Neergaard, Bidstrup and Guldin2019). In the most common trajectory, transient episodes of emotional dysregulation persist but tend to normalize over time without causing significant impairment (Szuhany et al. Reference Szuhany, Malgaroli and Miron2021). When such responses become persistent and lead to marked deterioration in daily functioning beyond what is culturally expected, the condition is considered abnormal and has been described in the literature under various labels – including pathological, traumatic, complicated, or prolonged grief (Zisook et al. Reference Zisook, Iglewicz and Avanzino2014). The current consensus is to refer to this maladaptive form of grief as prolonged grief disorder (PGD) (Prigerson et al. Reference Prigerson, Horowitz and Jacobs2009; Maercker et al. Reference Maercker, Brewin and Bryant2013) a diagnosis recently incorporated into the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) and The International Classification of Diseases, 11th Revision (ICD-11) (Prigerson et al. Reference Prigerson, Boelen and Xu2021). PGD is characterized by intense, persistent grief that endures longer than what is typically expected by social norms and significantly impairs daily functioning (Simon and Shear Reference Simon and Shear2024). Moreover, the association between prolonged grief and increased medical morbidity and mortality underscores its significance as a public health issue (Prigerson et al. Reference Prigerson, Horowitz and Jacobs2009; Rostila et al. Reference Rostila, Saarela and Kawachi2013; Shah et al. Reference Shah, Carey and Harris2013).
Prevalence studies of PGD have reported substantial heterogeneity, attributable to the diverse contexts of sample collection, differences in sampling procedures, response biases, and the use of various instruments and cut-off points (Lundorff et al. Reference Lundorff, Holmgren and Zachariae2017). For example, a meta-analysis involving 8,035 bereaved individuals yielded a pooled prevalence rate of 9.8% among adults (Lundorff et al. Reference Lundorff, Holmgren and Zachariae2017), suggesting that approximately 1 in 10 bereaved adults might be at risk of developing PGD. Furthermore, the risk of prolonged grief increases markedly when the cause of death is unnatural – such as in sudden or violent deaths – with some studies reporting prevalence rates as high as 49% (Djelantik et al. Reference Djelantik, Smid and Mroz2020).
In a systematic review of instruments designed to evaluate prolonged grief (Treml et al. Reference Treml, Kaiser and Plexnies2020), researchers identified 11 measures developed since 1995. Although most exhibited acceptable psychometric properties, their objectives varied; some were crafted to assess symptom severity, while others were intended for screening or diagnostic purposes. Among these, the Prolonged Grief Disorder (PG-13) Scale has emerged as a valid and reliable tool for the dimensional assessment of grief symptoms. It was initially introduced during the development of diagnostic criteria for PGD – proposed for inclusion in both the DSM-5 and ICD-11. Since its introduction, the PG-13 has been translated and validated in several countries, including Spain (Burdeus et al. Reference Burdeus, De miguel and Prigerson2017), Turkey (Işıklı et al. Reference Işıklı, Keser and Prigerson2020), Sweden (Sveen et al. Reference Sveen, Bondjers and Heinsoo2020), Korean (Hwang et al. Reference Hwang, Lee and Prigerson2023), Portuguese (Esperandio et al. Reference Esperandio, Rosas and Viacava2025), and in Iran (Ashouri et al. Reference Ashouri, Yousefi and Prigerson2024; Mirhosseini et al. Reference Mirhosseini, Khajeh and Sharif-Nia2024) among other languages and nationalities. More recently, a revised version (the PG-13-R) was developed to align with the criteria for PGD outlined in the DSM-5-TR. Based on data collected from Yale University (N = 270), Utrecht University (N = 163), and Oxford University (N = 239), the PG-13-R has established a cut-off score of 30 or higher for identifying syndromic levels of prolonged grief symptomatology (Prigerson et al. Reference Prigerson, Horowitz and Jacobs2009).
Although a Spanish validation of the PG-13 exists, it was conducted in Spain – a member of the European Union. Grief, as an individual process, is influenced by social, cultural, religious, economic, political, and historical contexts (Silverman et al. Reference Silverman, Baroiller and Hemer2021). Moreover, applying a translation in the same language (in this case, Spanish) across different countries can lead to potential issues, such as ambiguous terminology or stylistic differences that may affect comprehension. Conducting a translation and validation tailored to a specific region – here, Latin America – offers the advantage of employing terminology that is more accessible to local populations (Wild et al. Reference Wild, Eremenco and Mear2009). This is particularly important in Latin America, where average education levels tend to be lower than in Europe (World Bank n.d.). Addressing the need for instruments with evidence of score validity and reliability to assess grief is crucial for advancing cross-cultural research.
The present study aims to examine the psychometric properties of the Mexican version of the PG-13-Revised Scale.
Methods
Participants and procedure
We followed the recommended steps for translating, adapting, and validating instruments for use in cross-cultural healthcare research (Sousa and Rojjanasrirat Reference Sousa and Rojjanasrirat2011).
1. Translation of the Original Instrument into the Target Language. The original PG-13-Revised Scale (Prigerson et al. Reference Prigerson, Boelen and Xu2021) was translated into Spanish by 2 independent, bilingual, and bicultural certified translators whose native language is Spanish. One translator, a psychologist, possessed specialized knowledge in healthcare terminology and grief, while the other was well-versed in Spanish colloquial phrases, idiomatic expressions, and emotional nuances.
2. Comparison of the 2 Translated Versions: Synthesis I. The instructions, items, and response formats of the 2 forward-translated versions were initially compared with those of the original English version by a third independent bilingual translator. The investigator, along with other research team members, discussed and resolved any ambiguities or discrepancies in words, sentences, and meanings.
3. Blind Back-Translation of the Preliminary Version. The Spanish version produced in Step 2 was back-translated into English by 2 independent translators whose native language is English. Both translators were blind to the original PG-13-R. One was a certified translator, and the other was knowledgeable about healthcare terminology.
4. Comparison of the 2 Back-Translated Versions: Synthesis II. A committee compared the instructions, items, and response formats of the 2 back-translated versions with the original instrument in English. The review focused on wording, grammatical structure, semantic equivalence, and relevance. The committee comprised the principal investigator, research group members, a methodology expert, and a healthcare professional with expertise in the construct. Dr. Holly Prigerson, the developer of the original instrument, reviewed and approved the pre-final version.
5. Pilot Testing of the Pre-Final Version in the Target Language: Cognitive Debriefing. A panel of grief experts was convened to evaluate the items for clarity (i.e., conceptual equivalence), content, and relevance to prolonged grief. The experts also provided suggestions for enhancing the language. In total, 12 experts reviewed the questions and instructions – considering modifications for colloquialisms, potential cultural misconceptions, and overall conceptual clarity. All panel members worked in healthcare settings and had at least 6 months of experience dealing with grief, depression, and/or anxiety. Their varied perspectives ensured a comprehensive evaluation of the multifaceted symptoms associated with grief, not only those resulting from complex chronic illnesses.
Following the expert review, cognitive testing was conducted to further assess the conceptual, semantic, and content equivalence of the translated instrument. This step also refined the sentence structure in the instructions and items to ensure they were easily understood by the target population prior to psychometric testing. Cognitive interviewing provided crucial insights into how respondents interpreted the translated questions and the cognitive processes they used when answering, in comparison to their interpretation of the source-language questions (Schoua-Glusberg and Villar Reference Schoua-Glusberg, Villar, Miller, Willson, Chepp and Padilla2014). The pre-final version was pilot tested with 11 Mexican participants of diverse sociodemographic backgrounds, who evaluated the instructions, response format, and items for clarity and offered suggestions to improve the terminology to make it of relevance to a Mexican sample.
6. Psychometric Testing of the Translated Instrument with the Target Population. Participants were recruited via 2 channels: (1) Family Members of Patients: Individuals whose relatives had died from advanced cancer and received supportive care through a patient navigation program at a public hospital in Mexico City were contacted by phone if the death had occurred more than 1 year prior. (2) General Public: Invitations were extended through social media platforms (e.g., X, Facebook). Inclusion criteria required participants to be at least 18 years of age, Mexican nationals residing in Mexico, and to have lost a loved one at least 12 months before the study. Interested individuals accessed an online questionnaire after reviewing the study’s objectives and confidentiality assurances and providing informed consent. Participants then completed a brief electronic survey collecting sociodemographic information, details regarding the time elapsed since the death and the cause of death, as well as the pre-final version of the PG-13-R, the PHQ-9, and the GAD-7. Data collection occurred between January and July 2022. The study adhered to the latest version of the Declaration of Helsinki was approved by the local Institutional Review Board, and all participants provided informed consent. The characteristics of the sample are presented in Table 1.
Sample characteristics (N = 397)

Measures
Sociodemographic information. Sociodemographic data reflect self-reported information on gender/sex, educational level, cause of death of the deceased person and time since death.
PG-13-Revised Scale (PG-13-R). This 13-item scale was developed during the formulation of diagnostic criteria for PGD, proposed for inclusion in the DSM-5 and ICD-11. It assesses whether a significant person has died (Q1), the time elapsed since the loss (Q2), associated functional impairment (Q13), and the intensity of grief symptoms (Q3–Q13). Items Q2 through Q13 are rated on a 5-point Likert scale ranging from “1 = Not at all” to “5 = Overwhelmingly.” It allows for both dimensional assessment of grief intensity and diagnosis of PGD according to proposed criteria. Findings from the original study suggest that grief symptoms constitute a unidimensional construct, demonstrating high internal consistency (Cronbach’s α = 0.83, 0.90, and 0.93 for Yale, Utrecht, and Oxford, respectively) (Prigerson et al. Reference Prigerson, Boelen and Xu2021).
The Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 (Kroenke et al. Reference Kroenke, Spitzer and Williams2001) is a 9-item self-report instrument used to assess the severity of depressive symptoms. Items correspond to the DSM-IV criteria for major depressive disorder. Participants rate how often they have experienced each symptom over the past 2 weeks using a 4-point Likert scale: 0 = “Not at all,” 1 = “Several days,” 2 = “More than half the days,” and 3 = “Nearly every day.” Total scores range from 0 to 27, with higher scores indicating more severe depression: 0–14 = minimal, 15–19 = moderate, and ≥20 = severe depression.
The Generalized Anxiety Disorder-7 (GAD-7) (Spitzer et al. Reference Spitzer, Kroenke and Williams2006). The GAD-7 is a self-administered questionnaire designed to screen for and assess the severity of generalized anxiety disorder. It consists of 7 items that evaluate how often participants have experienced specific anxiety symptoms during the past 2 weeks. Responses are rated on a 4-point Likert scale from 0 = “Not at all” to 3 = “Nearly every day.” The total score ranges from 0 to 21, with higher scores reflecting greater symptom severity.
Data analysis
The distribution of responses and descriptive statistics were obtained for all items. The performance of the PG-13-R symptom items (Q3–Q13) was assessed by examining item means and variances, the percentage of responses at the syndromal level (scores of 4 or 5), and item–total correlations.
To examine the dimensionality of the scale, a confirmatory factor analysis (CFA) was conducted using Mplus 8.5 (Muthén and Muthén Reference Muthén and Muthén2016). In contrast to the validation study by Prigerson et al. (Reference Prigerson, Boelen and Xu2021) which employed a principal components analysis, CFA was selected because factor analysis is generally recommended when a latent variable is hypothesized (Fabrigar et al. Reference Fabrigar, Wegener and MacCallum1999; Schmitt Reference Schmitt2011). Based on previous findings, a 1-factor model was tested (Prigerson et al. Reference Prigerson, Boelen and Xu2021). Full information maximum likelihood estimation was used to address missing data (Enders Reference Enders2023). Model fit was evaluated using the chi-square (χ 2) test, where non-significant values indicate good fit. Additional indices included the comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Values above .90 for CFI and TLI and below .08 for RMSEA and SRMR suggest acceptable fit; values above .95 for CFI and TLI and below .06 for RMSEA and SRMR indicate good fit (Browne and Cudeck Reference Browne, Cudeck, Bollen and Long1993; West et al. Reference West, Taylor, Wu and Hoyle2012). To assess evidence of score validity via relationships with external criteria, Pearson correlation analyses were conducted between the total PG-13-R scores and the scores of related but distinct constructs such as depression as assessed by the PHQ-9 and generalized anxiety disorder as assessed by the GAD-7.
Cronbach’s alpha was calculated to evaluate the internal consistency (reliability) of the symptom items.
Results
Steps 1–4. Translation and expert review
Following the translation and back-translation of the instrument, the expert panel identified that Item 5 (addressing identity disruption) encompassed 2 distinct concepts: (1) confusion about one’s role and (2) the feeling that a part of oneself has died. Consequently, Item 5 was divided into 2 separate items (Items 5 and 6). Dr. Holly Prigerson, the developer of the original instrument, reviewed and approved the pre-final version. Her only recommendation was to replace the term “lost” (“¿has perdido a alguien importante para ti?”) with the more direct term “died.”
Step 5. Pilot testing and cognitive debriefing
In the cognitive debriefing phase, a first panel of 5 judges reviewed the preliminary version of the questionnaire and made adjustments to promote clarity and simplicity, recommending the use of plain language and straightforward terminology. In alignment with the use of brief and concrete sentences, the response options were also revised. While the original version measured symptom intensity, this panel suggested evaluating symptom frequency instead, as it was considered more intuitive and less ambiguous for respondents.
The introductory instructions were also modified to improve participants’ understanding of key terms. Additionally, judges noted that Item 5 was unclear due to its double-barreled phrasing – it appeared to address 2 concepts simultaneously. As a result, they recommended either splitting the item or consulting the literature to refine it into a more concise expression.
The Scale Content Validity Index (S-CVI) for this panel was 1.0. Since the S-CVI ranges from 0 to 1, with values above 0.80 considered acceptable (Polit and Beck Reference Polit and Beck2006), this result indicates that all items were rated as relevant and conceptually aligned with the construct, though some required revisions. Based on the panel’s feedback, a second review was conducted to assess the revised version, which included the splitting of Item 5 – resulting in 1 additional item in the Mexican adaptation of the scale.
The revised response format and updated instructions were retained, as judges assessed these changes positively. Additionally, they agreed to use the word “died” instead of “lost,” citing that euphemisms could cause confusion among respondents.
Item 7 (Item 8 for us) continued to receive feedback regarding its conceptual clarity and phrasing, and its content validity. Nonetheless, judges agreed that the component related to attachment should be preserved. A final version was compiled based on their observations, pending further confirmation from cognitive testing. The question evolved from “¿Evitas cualquier cosa que te recuerde que la persona que falleció ya no está?” to “¿Evitas cualquier cosa que te recuerde que la persona que murió ya no está?,” preserving the semantic content while subtly reflecting a shift from euphemistic to more direct language. It is worth noting that Item 7 has also posed difficulties in previous samples, as it assesses avoidant behavior – a construct not exclusive to grief or attachment and related to psychological trauma (e.g., PTSD) (Prigerson et al. Reference Prigerson, Boelen and Xu2021).
As results of the cognitive testing, the proposed changes to the questions and instructions were evaluated considering the doubts and observations that the second judges suggested, i.e.: is this question hard to answer? Do you consider answering these questions emotionally challenging? Participants were also asked to give suggestions whenever the item was not clear. A total of 11 people with the same inclusion criteria from Step 5 participated in this first cognitive assessment. Table 2 shows the socioeconomic characteristics of the participants in the first cognitive test.
Socioeconomic characteristics of the participants of the cognitive testing (n = 11)

This step confirmed the appropriateness of certain terms, such as *anhelar*, and supported the decision to divide Item 5 into 2 distinct items. Participants also demonstrated adequate understanding of Item 7. While some found specific items to be too direct, they were unable to offer alternative phrasings, and overall performance on the items was satisfactory.
Step 6. Psychometric testing of the pre-final version of the translated instrument of the target population
Table 3 presents the comparison of the original items, and the items proposed in the pre-final version. The sample consisted of 397 individuals.
Item performance and internal consistency

The CFA indicated poor model fit according to χ 2(44) = 179.787, p < .001 and RMSEA = .088 95% C.I. (.075, .102); adequate fit according to CFI = .948, TLI = .935; and good fit according to SRMR = .039. Modification indices were examined to evaluate the source of the lack of fit and high values were found for the correlation between Q3 and Q6, and Q7 and Q9.
A subsequent model (Model B) was run where the correlation between the unique variances of Q3 and Q6 was added. Overall, model fit improved, but both χ 2 and RMSEA continued to indicate poor model fit: χ 2(43) = 152.258, p < .001; RMSEA = .080 95% C.I. (.066, .094), while the rest of the fit indices indicated adequate or good model fit, CFI = .958, TLI = .946, SRMR = .036.
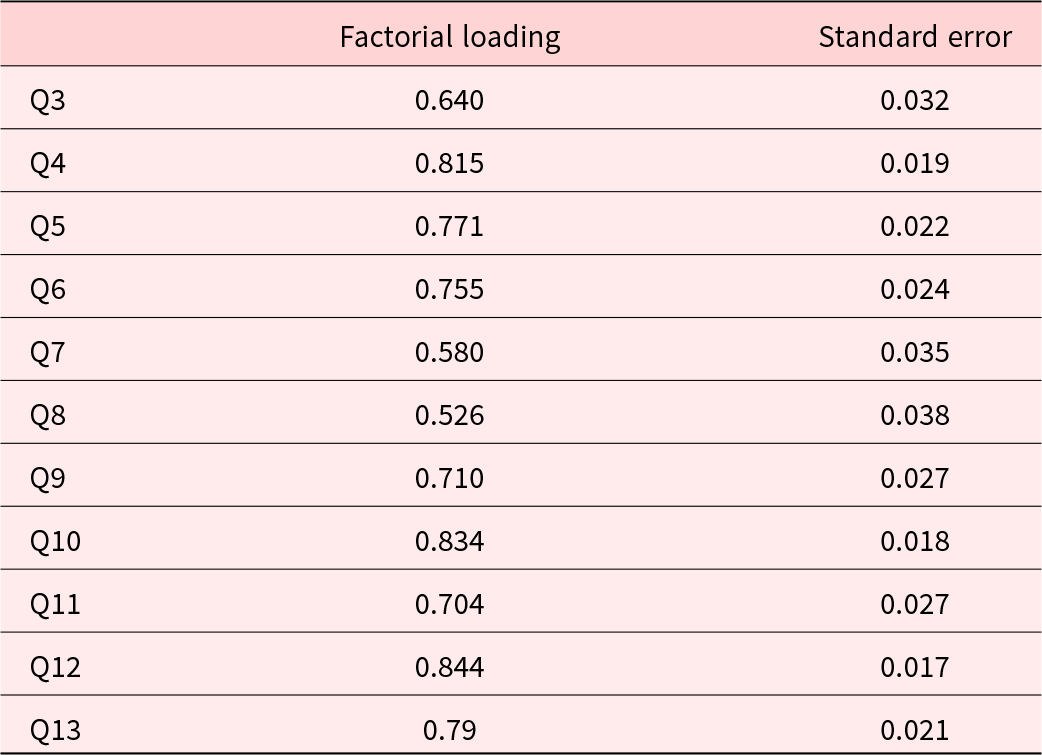
A third model (Model C) was run where the correlation between the unique variances of Q7 and Q9 was added. RMSEA indicated adequate fit (RMSEA = .071 95% C.I. (.056, .085), while CFI, TLI, and SRMR indicate good fit to the data (CFI = .968, TLI = .958, SRMR = .033). Although χ 2 indicates lack of fit, χ 2(42) = 124.896, p < .001, Model C was chosen as the final model due to the improvement in model fit according to the other indices. This final model includes 2 correlations between unique variances: between Q6 “You feel that a part of you died” and Q3 “You miss or long for the deceased person” with a correlation of .277; and between Q7 “You find it difficult to believe that the deceased person is no longer here” and Q9 “You feel emotional pain related to the death” with a correlation of .271. The standardized factor loadings according to Model C are high (Table 4).
Model C
Considering that the original item Q5 was split into Q5 and Q6 in the new version, we paid close attention to the psychometric properties of these 2 items in Model C. Both show high factor loadings and there was no statistical evidence favoring one over the other. An observed correlation of 0.561 was found between these 2 items, suggesting that while they are related, there is not much redundancy between them. Given that item Q6 was associated with a lack of fit due to its correlation with item Q3, an additional model was run eliminating item Q6 as a possible criterion for choosing between Q5 and Q6. However, the χ 2 and the RMSEA indicated lack of fit (χ 2 (44) = 179.787, p < .001; RMSEA = .088, 95% C.I. (.075, .102), CFI = .948, TLI = .935, SRMR = .039).
Final score
The article by Prigerson et al. (Reference Prigerson, Boelen and Xu2021) indicates that the PG-13-R scale has a range of values from 10 to 50. However, as it has a new item, the descriptive statistics of our version have values from 11 to 55.
Relationships with external criteria
Correlations with depression and anxiety scales were examined to assess evidence of validity with external criteria. The results show statistically significant correlations between PG-13-R new version and the anxiety and depression scales. These high correlations indicate that PG-13-R is positively associated with depression and anxiety. Furthermore, since the correlations are not greater than .70 (Hodson Reference Hodson2021), this suggests that PG-13-R measures a construct conceptually distinct from depression and anxiety. For the new version of PG-13-R, the correlation with depression is r = 0.62 and with anxiety is r = 0.59. The correlation between depression and anxiety is r = 0.77.
Discussion
The aim of the present study was to evaluate the psychometric properties of the PG-13-Revised Scale in the Mexican population, given the need for culturally adapted instruments to assess prolonged grief. Establishing the validity and reliability of this version is essential to ensure accurate measurement in clinical and research contexts.
A distinctive contribution of this study lies in the robust expert review process, which identified that the original item on identity disruption encompassed 2 conceptually different aspects: confusion about role and the sense that part of oneself has died. Based on this theoretical distinction and supported by statistical analyses, the item was divided into 2 separate questions (Q5 and Q6). Importantly, the statistical evidence confirmed that these items are not redundant but rather capture complementary dimensions of identity disruption. This refinement underscores the novelty of the adaptation, as it integrates both conceptual clarity and empirical validation to strengthen the measurement of prolonged grief in the Mexican context.
Identity disruption, also known as identity confusion, is a central construct of several theoretical models of complicated grief (Bellet et al. Reference Bellet, LeBlanc and Nizzi2020). There is no clear definition of this concept, but it is often explained as being related to the sensation that part of oneself has died along with the deceased.
Although not clearly defined, it is often described as the sensation that part of oneself has died along with the deceased. Within the Cognitive Attachment Model, individuals whose goals and plans were closely intertwined with the deceased – particularly when the deceased was a primary attachment figure – are at higher risk of developing complicated grief. For those with a “fused identity,” life goals and daily activities may become incompatible with the reality of the loss, leading to the termination of entire life domains. Bellet et al. (Reference Bellet, LeBlanc and Nizzi2020) introduced the concept of self-concept complexity, referring to the range of self-descriptions a person can provide. Reduced self-concept complexity has been identified as a predictor of prolonged grief, and this aligns with the item retained in our study that captures confusion about role. In the Mexican population, such role confusion may be particularly salient in relation to culturally embedded, gender-based activities.
Similarly, the Meaning Reconstruction Model of Grief proposed by Gillies and Neimeyer (Reference Gillies and Neimeyer2006) suggests that the narrative of the loss event disrupts preexisting assumptions in the grieving person’s self-narrative. This discrepancy results in identity confusion and loss of meaning. The item “part of you has died” resonates with this theoretical perspective, reflecting the profound disruption of identity that accompanies bereavement.
Future studies should investigate how the phrase “part of me has died” is interpreted within the Mexican cultural context, exploring its meaning in relation to the loss of a loved one and the resources available to adapt to this experience. A qualitative approach may be particularly useful to deepen understanding of the components involved in this construct and to capture culturally specific nuances of identity disruption.
The inclusion of an additional item in the Mexican version increases the total possible score compared to the original PG-13-R. Therefore, future research is needed to establish culturally appropriate cut-off points for the Mexican population to ensure diagnostic accuracy. This step is essential to ensure that the adapted instrument maintains its diagnostic accuracy and clinical utility, reflecting cultural and contextual differences in the experience of prolonged grief.
We noticed that both, the translators and the Mexican panel of experts suggested the word “lost,” instead of “died” for the item 1 during the phase of Steps 1–4. Euphemisms serve as a linguistic tool to make daily conversations about sensitive or difficult subjects more palatable, with death being a particularly notable instance (Al-Laith et al. Reference Al-Laith, Conroy, Bjerring-Hansen, Rambow, Wanner, Apidianaki, Al-Khalifa, Eugenio B and Schockaert2025). It has been found that in medical contexts, replacing a word or phrase with a euphemism to make it less distressing is often a deliberate decision. However, euphemistic expressions intended to soften the impact for patients (e.g., “pass on” instead of “die”) or to address potentially unpleasant topics more tactfully (e.g., “voided” instead of “peed”) can cause confusion among patients(Pitt et al. Reference Pitt, Hendrickson and Marmet2022). For this reason, Dr. Prigerson suggested changing “lost” for “died,” so the final question 1 is: “¿Ha muerto alguien importante para ti?.” In a subsequent decision, judges expressed their agreement with the proposal to adopt a clearer and more direct terminology. They endorsed the use of the term “died” as a standard expression, emphasizing its straightforwardness and precision over the use of euphemisms, which might obscure the reality of the situation.
Two rounds of revision and evaluation of items by judges regarding clarity, content and relevance were conducted. The final version of the instrument achieved a high level of agreement among them. The cognitive interview conducted afterward strengthened these results. Through this process, we ensured that the items were comprehensible to individuals with the characteristics targeted by the instrument and that they would find it user-friendly. The sample in this study differed from those in Europe and the United States, as participants from those countries had attained higher levels of education – ranging from high school to postgraduate studies – whereas the Mexican sample predominantly reported completed or incomplete basic education. We consider this step highly relevant, as it is not commonly undertaken in most studies involving the translation or adaptation of an instrument. However, it significantly enhances the items from the perspective of content validity.
Regarding item performance, our analysis of the percentage of individuals who responded at a syndromic level (scores of 4 or 5) revealed a higher prevalence in items assessing worry (92%), the perception that “Life is meaningless” (91%), and avoidance (86%). While the expert panel noted that avoidance is not exclusively linked to grief or attachment – an assertion that holds true – these findings underscore its significance in the assessment of prolonged grief, given its high prevalence.
When comparing these prevalence rates with those reported in the original validation (Prigerson et al. Reference Prigerson, Boelen and Xu2021) (which includes the studies from Yale, Utrecht, and Oxford), we find that they are significantly higher than in any of those studies. The study with the highest symptom prevalence was conducted in Utrecht, where “Yearning” was the most frequently reported symptom (68.1%). In contrast, symptom prevalence among Mexican participants was at least 60% across all symptoms, except for “Yearning,” which was present in 38.9% of the participants. A study comparing bereavement experiences among Mexican American and white college students revealed that Mexican Americans tended to express their grief more outwardly and showed stronger physiological responses to the loss (Oltjenbruns Reference Oltjenbruns1998). A separate study focusing on the concept of yearning – defined as persistent, unmet longings for the presence of the deceased and involving a mental-emotional process of repeatedly contrasting current reality with an unattainable one – examined data from German-speaking countries, other European nations, Israel, and China to compare prolonged grief symptoms across cultures. The findings suggested that yearning is not necessarily tied to culturally shaped expressions of distress and, therefore, did not emerge as the most prominent symptom of PGD in all regions (Mazza et al. Reference Mazza, Maercker and Forstmeier2025). On the other hand, our sample is significantly younger. Some studies have attempted to find associations between grief symptoms and age groups. It appears that the symptom of yearning is more characteristic of older adults, possibly because grief in later life may be shaped by age-related cognitive changes that influence emotional processing, memory, and coping mechanisms (Hoffmann et al. Reference Hoffmann, Blair and McAuliffe2024). Additionally, a large proportion of participants in our sample lost their loved ones due to COVID-19 – deaths that were likely unexpected and in which mourners probably lacked the usual resources for processing grief, such as funerals or the support of close friends (van Schaik et al. Reference van Schaik, Brouwer and Knibbe2025).
It is important to highlight that our sample consisted of individuals whose relatives died more than a year ago, with some experiencing a loss over 5 years ago. The idea that grief may endure due to the causal interplay among its components is grounded in the network theory of psychopathology, which asserts that symptom interactions play a fundamental role in the development of various mental disorders (Robinaugh et al. Reference Robinaugh, Toner and Djelantik2022). Network analyses suggest that the most central symptoms play a pivotal role in shaping symptom expression and influencing the progression of the disorder. Consequently, targeting these core symptoms in interventions may be particularly effective, as mitigating them could help reduce distress in interconnected symptoms. The data obtained suggest that a primary intervention target in our sample may be preoccupation with thoughts or memories of the deceased person, the sense of loss of meaning in life, and avoidance. In contrast, a study conducted in Africa (Robinson et al. Reference Robinson, Armour and Levin2024) identified feelings of loss – a concept seemingly linked to identity disruption – and difficulty moving on as potential key targets for intervention. Grief expressions vary across cultures, with certain reactions deemed pathological in some societies while considered normal mourning processes in others. Cultural norms shape these differences, influencing symptom prevalence, emotional responses, and coping mechanisms across ethnic groups (Hilberdink et al. Reference Hilberdink, Ghainder and Dubanchet2023). In Latin cultures, spirituality plays a vital role (Gonzalez et al. Reference Gonzalez, Nuñez and Wang-Letzkus2016). When individuals face a terminal diagnosis, trusting that their future rests in God’s hands can offer meaningful comfort to both patients and their families. Religious and spiritual elements are profoundly embedded in end-of-life care and mourning practices, shaping the kinds of support that are both preferred and considered appropriate (Campesino and Schwartz Reference Campesino and Schwartz2006).
The Mexican version of the PG-13-R demonstrated good internal consistency reliability, as indicated by a Cronbach’s alpha of 0.89. No item removal was required to enhance the scale’s consistency, aligning with findings from studies conducted in other countries (Hwang et al. Reference Hwang, Lee and Prigerson2023; Ashouri et al. Reference Ashouri, Yousefi and Prigerson2024). Our findings on construct validity indicate that the one-factor structure demonstrates an acceptable fit. Both in studies with community-based samples in which the previous version of the PG-13 was validated (He et al. Reference He, Tang and Yu2014; Sveen et al. Reference Sveen, Bondjers and Heinsoo2020), and in the validation studies of the PG-13-R, it is confirmed that the PG-13-R is composed of a single factor (Prigerson et al. Reference Prigerson, Boelen and Xu2021; Ashouri et al. Reference Ashouri, Yousefi and Prigerson2024). Only 2 studies that have used the PG-13-R (Kang and Donghun Reference Kang and Donghun2017; Hwang et al. Reference Hwang, Lee and Prigerson2023) have reported results consistent with a 2-factor structure, which has been proposed as 2 distinct aspects: traumatic distress and separation distress. The authors attribute this to cultural differences, as the studies were conducted in China and Korea and may reflect the nature of the society’s relationship with Confucian culture. If this hypothesis were true, the way our sample behaved would show more similarities with Western cultures. Further research is essential to better understand the mental health, cultural, social, and familial needs of Latino/a groups, as well as the role of religious rituals and other cultural influences that may facilitate or hinder psychological adjustment (Falzarano et al. Reference Falzarano, Winoker and Burke2022). Studies are also needed to explore protective factors that help bereaved individuals avoid negative mental health outcomes. Cultural values such as fatalism, simpatia, personalism, familism, and allocentrism are believed to shape how grief is perceived and expressed within Latino/a communities (Nuñez et al. Reference Nuñez, Holland and Beckman2019). Our final model includes 2 correlations between unique variances. From a theoretical perspective, the correlation between Q6 and Q3 reflects the intertwined nature of identity disruption and yearning in prolonged grief. The sense of having lost a part of oneself is conceptually linked to the persistent longing for the deceased, as both experiences highlight the deep attachment bond and the difficulty in reconstructing one’s identity after the loss. Although the correlation is modest (.277), it is consistent with models of grief that emphasize how yearning is not only about the absence of the loved one but also about the perceived fragmentation of the self. Similarly, the correlation between Q7 and Q9 underscores the theoretical connection between disbelief and emotional suffering. Difficulty in accepting the reality of the loss often sustains the intensity of emotional pain, as cognitive denial or shock prevents the integration of the loss into one’s life narrative. The observed correlation (.271) aligns with conceptual frameworks of prolonged grief that describe disbelief as a mechanism that perpetuates distress, thereby maintaining the cycle of emotional pain.
On the other hand, as has been the case in all other validation studies of the instrument (Sveen et al. Reference Sveen, Bondjers and Heinsoo2020; Prigerson et al. Reference Prigerson, Boelen and Xu2021; Ashouri et al. Reference Ashouri, Yousefi and Prigerson2024), our study found a significant correlation between the total PG-13-R score and the scales measuring depressive (PHQ-9) and anxious (GAD-7) symptomatology. Earlier research has indicated a moderate positive link between depression and anxiety symptoms and those associated with prolonged grief (Tsai et al. Reference Tsai, Kuo and Wen2018). However, the degree of correlation suggests that prolonged grief is associated with these symptoms but constitutes a distinct entity, providing evidence for the concurrent validity of the instrument.
The main strength of the study lies in it being the first translation and validation into Spanish of this specific version of the PG-13: the PG-13-R. The process followed meticulous steps to ensure that the instrument was well understood by individuals with varying educational backgrounds. Additionally, it underwent a thorough expert review, which allowed us to confirm its content validity. PGD is a recently recognized condition, and awareness of its symptoms and treatments remains limited. Many clinicians may lack the training to identify or address it effectively. Hence the importance of having a valid and reliable instrument that can be used in Spanish-speaking populations.
One of the study’s limitations is the use of convenience sampling. The data presented here reflect only those who agreed to participate; however, we cannot determine whether among those who declined participation there is a significant proportion of individuals experiencing grief with characteristics different from those reported in this study. On the other hand, the study relied on self-reports, a large proportion of which were completed online, which may increase the likelihood of data errors. We recommend that upcoming studies recruit a larger proportion of individuals with lower educational attainment, as these groups may encounter barriers to mental health care and have more limited social support networks. Furthermore, our sample – similar to most international samples – primarily reflects grief in female populations; thus, it would be valuable to specifically examine bereavement experiences among men (Stroebe et al. Reference Stroebe, Schut and Boerner2010). Finally, the final PG-13-R scores were not compared against any gold standard, making it impossible to establish specific cutoff points for our population in this study. This remains an area for future research.
Significance of results: The Mexican version of the PG-13-R is culturally appropriate, valid, and reliable for assessing prolonged grief.
Acknowledgments
We want to thank Carolina García, Elisa Pérez, Sandra Sierra, Karime Adame, Virginia Monserrat Martínez, Daniela Ramírez, Ariana Jiménez, and Leslie Meza who were part of the committee that reviewed the different versions of the instrument at various stages. We also thank Sonia García Navarro, Carolina Díaz Sánchez, Gloria Alhelí Chávez Juárez, Joél Flores Juárez, Dr. Édgar Landa Ramírez, Dra. Natasha Alcocer Castillejos, Paulina Quiroz Friedman, Lorena González, Susana Ruiz, Leticia Ascencio, Nancy Rangel, Mónica Ramírez Orozco, and Jazmín Edith Hernández Marín for their valuable feedback as part of the panel of expert judges.
Competing interests
The author(s) declare none.
AI contributions to research content
AI tools were employed solely for language editing purposes, specifically to improve clarity, coherence, and style in English. No AI was used for generating content, analyzing data, or interpreting results. All scientific work, including study design, data collection, statistical analysis, and conclusions, was performed entirely by the authors.





 Open access
Open access