


Parenthood
Parenthood, pregnancy and childbirth are life transitions that require new solutions and affect the wellbeing and health of the whole family (Meleis, Reference Meleis1997). Building a parenting identity and preparing for parenthood are very important processes already during pregnancy. Images or representations of parenthood begin to build on the parent’s own early childhood experiences of being cared for. They are reinforced by the desire to become a parent, especially during pregnancy. During pregnancy, parenting is concretised in thoughts about children, hearing their heartbeats, watching their movements, seeing pictures of the fetus, and preparing for the child’s arrival (Cline et al., Reference Cline, Dimmitt and Gann2022; Damato, Reference Damato2004a).
Parenting in a Multiple-Birth Family
In a multiple-birth family, more than one child of the same age is expected or has been born, that is, twins or triplets. (Diverse Families, 2023; Finnish Multiple Births Association, 2023; International Council of Multiple Birth Organisation [ICOMBO], 2023) The biology of multiple pregnancies is complex and may be influenced by factors such as an older age of the mother and the number of previous pregnancies. Twins are either identical (genetically identical, monozygotic [MZ]) or nonidentical (dizygotic, [DZ]) (Kaprio, Reference Kaprio, Kumpula, Kaprio, Lavikainen and Moilanen2020; Kaprio et al., Reference Kaprio, Karttunen and Kerppola-Pesu2022; Kerppola-Pesu et al., Reference Kerppola-Pesu, Haahtela, Heinonen, Herranen, Herrgård, Kaistinen, Karttunen, Kivilaakso, Siivola, Siivonen, Suomalainen, Tuunanen, Vainio, Ojaluoto, Matala and Kumpula2022; Tiitinen, Reference Tiitinen2023). According to statistics from the Finnish Institute for Health and Welfare (Terveyden-ja hyvinvoinnin laitos; THL), there were 43,882 births in Finland in 2024, of which 549 were multiple births. Twins were born in 543 families and triplets in six families (Hauhio et al., Reference Hauhio, Heino and Gissler2025).
Multiple births account for 1.3% of all births in Finland. The number of multiple births in Finland has remained relatively stable over the years (Hauhio et al., Reference Hauhio, Heino and Gissler2025; Finnish Multiple Births Association, 2023). Multiple-birth families are families with special needs that require attention from health and social care professionals (Heinonen, Reference Heinonen2013; Heinonen & Kerppola, Reference Heinonen and Kerppola-Pesu2024; Raussi-Lehto et al., Reference Raussi-Lehto, Jouhki and Kaijomaa2021; Rissanen et al., Reference Rissanen, Jernman and Räsänen2024; Tiitinen, Reference Tiitinen2023).
Information on Multiple-Birth Families and the Lack of It
Maternity and child health clinic and hospital staff play a key role in the delivery of services for multiple-birth families and the provision of information on such families (Heinonen, Reference Heinonen2013; Turnville et al., Reference Turville, Alamad, Denton, Cook and Harvey2021). Multibirth family information is specific information needed to support the parenting of multiples and care for more than one child of the same age. The dissemination of information on multiple-birth families and the promotion of the rights of these families is among the key objectives of the International Council of Multiple Birth Organisations (ICOMBO), to which the Finnish Multiple Births Association belongs (ICOMBO, 2023; Finnish Multiple Births Association, 2023). Health promotion programs are needed for multiple-birth families at a very early stage (Crugnola et al., Reference Crugnola, Ierardi, Prino, Brustia, Cena and Rolle2020).
With the specific information needed on multiple-birth families, maternity and child health midwives and nurses can support parenting and the growth and development of multiples, as well as promote the health and wellbeing of the family.
Risk in Pregnancy
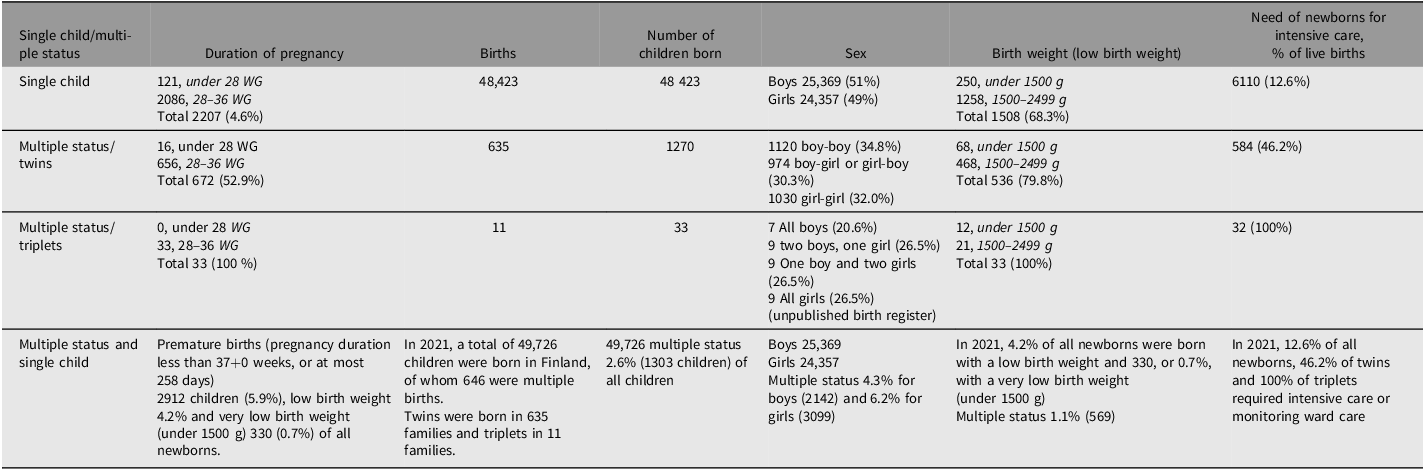
Midwives and nurses working in maternity and child health clinics provide care that affects all pregnant women and families with children. Multiple-birth pregnancies are always high-risk pregnancies (Raussi-Lehto et al., Reference Raussi-Lehto, Jouhki and Kaijomaa2021; Tiitinen, Reference Tiitinen2023), and the risks associated with both the expectant mother and the fetuses are more common than in single-foetus pregnancies (Tingleff et al., Reference Tingleff, Räisänen, Vikanes, Dansvik, Sugulle, Murzakanova and Laine2023). Risks during pregnancy include pregnancy complications, pregnancy symptoms and pre-eclampsia (Purho et al., Reference Purho, Nuutila and Heikinheimo2006; Tingleff et al., Reference Tingleff, Räisänen, Vikanes, Dansvik, Sugulle, Murzakanova and Laine2023). Major fetal problems include fetal developmental disorders (Purho et al., Reference Purho, Nuutila and Heikinheimo2006), fetal growth retardation (40%) (Raudaskoski & Hartikainen, Reference Raudaskoski, Hartikainen, Ylikorkiala and Kauppila2011) and low birth weight (Monden et al., Reference Monden, Pison and Smits2021). Multiple gestation is also associated with premature fetal birth (Purho et al, Reference Purho, Nuutila and Heikinheimo2006; Tiitinen, Reference Tiitinen2023), increased uterine mortality and an increased risk of neonatal and maternal death. (Monden et al., Reference Monden, Pison and Smits2021; Tingleff et al., Reference Tingleff, Räisänen, Vikanes, Dansvik, Sugulle, Murzakanova and Laine2023). Even though perinatal, neonatal and infant mortality is increased for twins, their mortality is paradoxically lower than for singletons if adjusted for gestational age (Cheung et al., Reference Cheung, Yip and Karlberg2000). Taking gestational age into account, twins have fewer RDS (respiratory distress syndrome) symptoms than singletons (Marttila et al., Reference Marttila, Kaprio and Hallman2004). The shared placenta and fetal membranes of fetuses are associated with an increased need for intensive care for the B-twin (Rissanen et al., Reference Rissanen, Gissler, Nupponen, Nuutila and Jernman2022). Costello-Harris and Segal (Reference Costello-Harris and Segal2018) have also identified developmental delays in multiple births. Awareness of the risks of a multiple-birth pregnancy increases parental concern and the need for support during pregnancy (Heinonen, Reference Heinonen2013; Heinonen & Kerppola, Reference Heinonen and Kerppola-Pesu2024). Pre-term birth brings additional challenges (Turville et al., Reference Turville, Alamad, Denton, Cook and Harvey2021). Table 1 summarises information related to twins and triplets.
Comparison of multiples and single children (Kiuru et al., Reference Kiuru, Heino and Gissler2021; THL, 2023; Gissler Reference Gissler2023)

Table 1 Long description
The table compares various aspects of single child and multiple child pregnancies. It has 10 rows and 7 columns. The columns are labeled Single child/multiple status, Duration of pregnancy, Births, Number of children born, Sex, Birth weight (low birth weight), and Need of newborns for intensive care, % of live births. The rows provide data for single child, multiple status/twins, multiple status/triplets, and multiple status and single child. Each row lists specific details under each column header. For example, the single child row shows a duration of pregnancy of 121 for under 28 weeks and 2086 for 28-36 weeks, totaling 2207. It also shows 48423 births, 48423 children born, sex distribution of boys 25369 and girls 24357, birth weight details, and 6110 newborns needing intensive care, which is 12.6 percent of live births. Similar detailed data is provided for multiple status/twins, multiple status/triplets, and multiple status and single child rows.
The Challenges of Interaction and Care
Parenting more than one child of the same age is often perceived as a privilege and a source of happiness for multiple-birth families, but it is also associated with challenges and strain (Beck, Reference Beck2002; Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013; Heinonen, Reference Heinonen2015a, Reference Heinonen2015b, Reference Heinonen2015c). Early interactions with the fetus and unborn children begin during pregnancy (Cline et al., Reference Cline, Dimmitt and Gann2022; Mackie et al., Reference Mackie, Pattison, Jankovic, Morris and Kilby2020) and continue after delivery. Parents have experienced challenges in forming early attachment and interaction relationships (Bryan, Reference Bryan2003; Chang, Reference Chang1990; Damato, Reference Damato2004a, Reference Damato2004b; Ionio et al., Reference Ionio, Mascheroni, Lista, Colombo, Ciuffo, Landoni, Daniele and Gattis2022; Josse & Robin, Reference Josse and Robin1986; Moilanen, Reference Moilanen and Alkio2007; Moilanen & Pennanen, Reference Moilanen and Pennanen1997). According to Gowling et al. (Reference Gowling, McKenzie-McHarg, Gordon and Harrison2021), forming attachment relationships takes time, requires adaptation and often differs from mothers’ expectations. Challenges are also introduced by caring for more than one child of the same age (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013; Heinonen et al., Reference Heinonen, Häggman-Laitila and Moilanen2016; Jonsdottir et al., Reference Jonsdottir, Flacking and Jonsdottir2022; Leonard, Reference Leonard2000; Robin et al., Reference Robin, Corroyer and Casati1996; Robin et al., Reference Robin, Josse and Tourette1988). Achieving maternal confidence in breastfeeding contributes to the continuity of breastfeeding of multiples (Anjarwati et al., Reference Anjarwati, Waluyanti and Rachmawati2019), but the support received for breastfeeding has been perceived as insufficient (Cinar et al., Reference Cinar, Alvur, Kose and Nemut2013; Jonsdottir et al., Reference Jonsdottir, Flacking and Jonsdottir2022). The late start and early finish of breastfeeding may be related to maternal stress associated with breastfeeding, the time required for breastfeeding, and the needs of children. The need for neonatal intensive care for newborns also affects the situation (Withford et al., Reference Whitford, Wallis, Dowswell, West and Renfrew2017). Although some positive elements of the postpartum period were noted, most parents described this time as stressful, overwhelming, and exhausting (Wenze et al., Reference Wenze, Miers and Battle2020). Many families with multiples wish for more outside help than they can get (Heinonen, Reference Heinonen2013). Parents find nighttime especially stressful and look to the child health clinic for advice on how to consider the children’s different rhythms (Heinonen, Reference Heinonen2013). Factors affecting sleep intertwined with parents’ uncertainty, dissatisfaction with professional services, and lack of information (Heinonen, Reference Heinonen2013; Hsu et al., Reference Hsu, Wu, Tung, Thomas and Tsai2017). Fatherhood is strengthened by participation in childcare and personal moments with the twins. However, fathers expect more attention and support from the clinic and peer support (Heinonen, Reference Heinonen2013, Reference Heinonen2022). Attention to fathers’ wellbeing is important, as it also affects the children’s health and wellbeing (Challacombe et al., Reference Challacombe, Pietikäinen and Kiviruusu2022).
Parents’ Ability to Cope
Parents expect support from health professionals such as the child health clinic to maintain resources and ensure coping in the daily life of a multiple-birth family (Heinonen, Reference Heinonen2015c, Reference Heinonen2013, Reference Heinonen2019). The parents of multiples have been found to be at increased risk of depression, and attention should be paid to providing psychological support, especially in situations where the course of pregnancy is abnormal (e.g., twin-to-twin transfusion syndrome [TTTS]; Mackie et al., Reference Mackie, Pattison, Jankovic, Morris and Kilby2020; see also Wenze et al., Reference Wenze, Battle and Tezanos2015). Multiple-birth parenting also affects the quality of newborn–mother interactions. Compared to single mothers, the mothers of twins were less responsive to their newborn’s needs, and were anxious and experienced stress (Crugnola et al., Reference Crugnola, Ierardi, Prino, Brustia, Cena and Rolle2020). However, Mönkediek et al. (Reference Mönkediek, Schulz, Eichhorn and Diewald2020) found that twins may receive even more nurturing and emotional warmth from their parents than nontwins. Parents have also raised concerns about other children in the family receiving less parental attention (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2015c). Parental concerns can be focused on different ways: in the study by Kotera et al. (Reference Kotera, Kaluzeviciute and Bennett-Viliardos2022), mothers’ concerns were focused on health, while fathers’ concerns were focused on work and family finances. Fatherhood was described by fathers and health care professionals as an observer, spouse supporter, partner, and head of the family. Fathers from different families can be encouraged to adopt different ways of being a father or discouraged from adopting a certain way (Kaila-Behm & Vehviläinen-Julkunen, Reference Kaila-Behm and Vehviläinen-Julkunen2000).
The aims of the study were to develop the multiple-birth family competence of midwives and public health nurses by utilizing the results of the research in social and health care education, to identify areas of multiple-birth family knowledge that should be strengthened in education, and to develop evidence-based nursing at maternity and child health clinics and to respond to the special needs for information and support of multiple-birth families.
Purpose of the Study and Research Problems
The specific purpose of this study was to describe the knowledge of multiple-birth families among midwives and public health nurses working in maternity and child health clinics, that is, knowledge needed to support multiple-birth parenthood and caring for more than one child of the same age.
The research questions were:
-
1. What knowledge do midwives and public health nurses have of multiple-birth families?
-
2. How is the participant’s background (age, education and work experience) connected to their multiple-birth family knowledge?
Materials and Methods
Research Design
The study was carried out in a cross-sectional setting, and data were collected at a single timepoint from midwives and public health nurses at maternity and child health clinics in southern, central and northern Finland with a questionnaire. The clinics form part of the primary care health centres in local communities, who at that time were responsible for health services in primary care. Where necessary, the local clinics consult obstetrical units at the regional hospitals. Most births take place in regional hospitals. Mothers expecting multiples are considered high-risk pregnancies and their births are often directed to university hospitals; university hospitals also act as regional hospitals for their own immediate region.
Regional leaders were contacted to inform them about the upcoming research and the research permit process. Most births take place in regional hospitals. After the research permit was granted, negotiations with the supervisors of the maternity and child health clinics provided information on which maternity and child health clinics would participate in the study. One municipality did not respond to the permit application, despite being contacted, and one municipality responded negatively.
Target Group and Data Collection
According to the information provided by the persons in charge, a total of 144 midwives and public health nurses out of 156 were invited to attend the events. An information session on the study was arranged in connection with maternity clinic staff meetings, and 12 of these sessions were held at staff meetings. The information session consisted of a presentation by the principal investigator, the content of which consisted of the presentation of and participation in the study, the processing of personal data and the grounds for processing, data protection, the significance of the research, the voluntary nature of participation and informed consent. Participants were able to ask questions and received the researcher’s contact information. The participants also received information about the international continuation of the study.
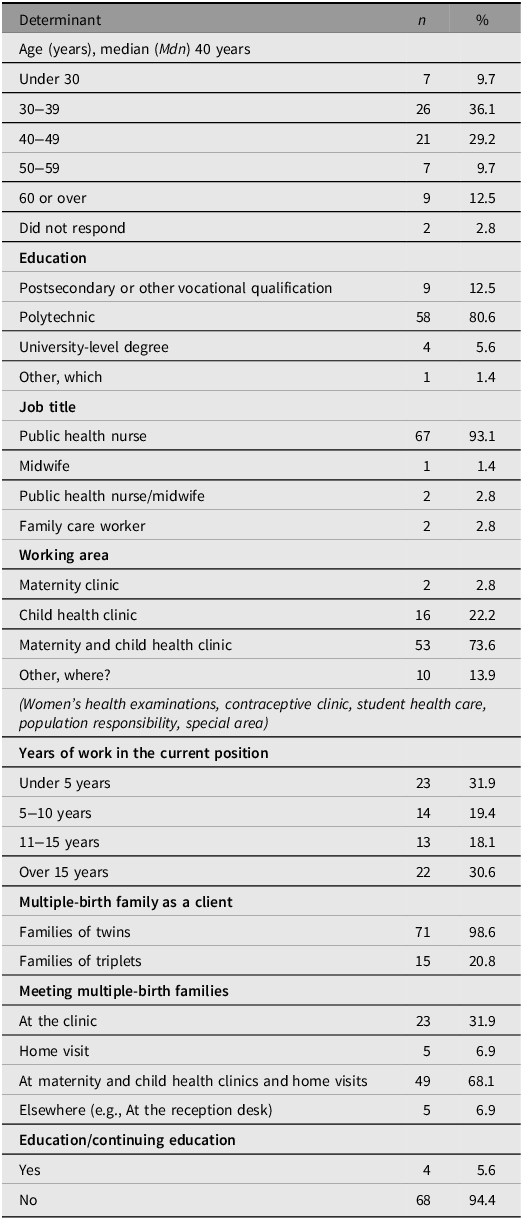
After each information session, the participants received an email with a link to the survey from their supervisor. To reach the target group, the questionnaire began with the statement: ‘We have assessed that you are suitable for the study because you are a midwife or public health nurse and have worked with multiple-birth families.’ The data were collected from maternity and child health clinics (n = 33), with a questionnaire using the RedCap web-based data collection software between March 21, 2022, and April 30, 2022 across the Southern, Middle and Norther Finland regions (RedCap, 2023). Altogether, 76 participants, all women, responded to the questionnaire. Not all participants gave their informed consent, and the final number of participants was 72. The response rate was 50%, calculated based on the number of participants in the information session. The background information of the participants is described in Table 2.
Background information on the midwives and nurses (n = 72)

Table 2 Long description
A table summarizing background information of midwives and nurses. The table has 18 rows and 3 columns. The columns are labeled Determinant, n, and %. The table includes data on age, education, job title, working area, years of work in the current position, multiple-birth family as a client, meeting multiple-birth families, and education/continuing education. Each row provides specific details under these categories. For example, the age category includes ranges like Under 30, 30-39, 40-49, 50-59, 60 or over, and Did not respond with corresponding values for n and %. The education category lists Postsecondary or other vocational qualification, Polytechnic, University-level degree, and Other, which. The job title category includes Public health nurse, Midwife, Public health nurse/midwife, and Family care worker. The working area category lists Maternity clinic, Child health clinic, Maternity and child health clinic, and Other, where. The years of work in the current position category includes Under 5 years, 5-10 years, 11-15 years, and Over 15 years. The multiple-birth family as a client category lists Families of twins and Families of triplets. The meeting multiple-birth families category includes At the clinic, Home visit, At maternity and child health clinics and home visits, and Elsewhere. The education/continuing education category lists Yes and No.
Questionnaire
In the absence of a questionnaire on the subject, a questionnaire was initially developed using multidisciplinary data. The development work was also based on the researcher’s previous familiarity with the subject (Heinonen, Reference Heinonen2013). The survey took shape in an examination of the nursing framework, which took into account maternity and child health clinic nursing, multiple-birth parenting and its support, childcare, special features of multiple-birth family interaction, the relationship between multiple birth siblings, support for the growth and development of multiple-birth children, and the promotion of family health. The studies that were most closely related to multiple-birth family data and multiple-birth family care were selected. The statements and open-ended questions in the questionnaire were based on relevant information and previous studies for each statement (e.g., Bryan, Reference Bryan2008; Chang, Reference Chang1990; Goshen-Gottstein, Reference Goshen-Gottstein1980; Harvey et al., Reference Harvey, Athi and Denny2014; HeinonenReference Heinonen2019, Reference Heinonen2013; Kaprio, Reference Kaprio and Alkio2007, Reference Kaprio, Kumpula, Kaprio, Lavikainen and Moilanen2020; Robin et al., Reference Robin, Josse and Tourette1988; Trias, Reference Trias2006).
The first version of the questionnaire was evaluated by an expert in family nursing science, health science teachers, midwives, public health nurses, and nurses from different backgrounds working at maternity and child health clinics. The statements in the form were clarified and refined because respondents indicated that the statements were not expressed clearly enough. The second version of the questionnaire was evaluated by midwives and public health nurses experienced in multiple-birth family nursing. Respondents noted that the statements were clear but contained repetition. A couple of respondents gave feedback about the length of the form, although the time required to complete it was generally considered reasonable. Repetitive items were removed from the form, and the content of the statements was reviewed again. The revised form was then tested again with midwives and public health nurses. They reported that the statements were clear, easy to respond to, and that the overall completion time was appropriate. During the development work, the form was tested three times. The feedback focused on the content, the clarity and quantity of questions and arguments, as well as the use of time. Based on the feedback, the indicator was developed, a few questions were clarified, and the form was shortened.
The final version of the questionnaire consisted either of open-ended questions or questions with a symmetric Likert-type scale of five response options (1. Totally agree; 2. Partially agree; 3. Neither agree nor disagree; 4. Somewhat disagree; 5. Strongly disagree). The first part of the questionnaire asked for the participant’s background information and the respondents were asked about their experience of caring for multiple-birth families, training related to multiple-birth family information and the need for information (questions 1–12). This part of the questionnaire included seven open-ended questions and some of the open-ended questions related to the possibility of supplementing one’s own answer. The second part of the questionnaire covered three domains created on the basis of previous literature as mentioned above: multiple-birth parenting, pregnancy and childbirth (13–43); interaction in the multiple-birth family (44–86); and the relationship between and care for children of the same age also with three open-ended questions (87–126). Finally, in the third part the participant’s feedback and assessment of the importance of the study were requested (127–128). The questionnaire contained a total of 128 questions. Explanatory variables were age, education and work experience.
In the data collection phase, the first 20 responses served as pretesting, after which the question regarding informed consent was written more clearly, as the answer to this question was missing from one form. The responses collected during the pretesting were part of the final data.
Data Analysis
The data were statistically analyzed with SPSS 27. The study measured the multiple-birth family knowledge of midwives and public health nurses working in maternity and child health clinics. The median (Mdn) and interquartile intervals (IQR) were calculated from the average of responses to the questionnaire topics. The differences between the two groups — for example, between maternity clinics and child health clinics — were examined using the Mann–Whitney U-test. The topics were compared between different background groups using one-way analysis of variance (ANOVA) and the Kruskall–Wallis test. Correlations between two groups of sum variables were examined using the Pearson correlation coefficient r. The distributions were described with a box-and-whisker plot. A median of less than 4 indicates that the participant has a lack of knowledge. A median close to three means that the participant does not know the answer. In this study, the most used limit for statistical significance was a p-value below .05.
Ethical Aspects
The participants were maternity and child health clinic staff and not clients. No ethical review was sought for the study. The study did not interfere with the participants’ physical integrity, present strong stimuli, or cause mental harm or a safety threat beyond the limits of normal everyday life to the participants or their loved ones. Before the study, the university’s Data Protection Officer was consulted, and the study followed the regulations set by the Data Protection Act (DAP; 1050/2018) and the EU General Data Protection Regulation (GDPR; 679/2016) on the processing of personal data. The study did not deviate from the principle of informed consent (Finnish National Board on Research Integrity [TENK], 2023). The research information sessions organized in connection with the staff meetings of the working units also covered the study’s privacy notice and the processing of personal data. These were also available at the beginning of the questionnaire in a bulletin to the study participants. Participants were given the opportunity to ask questions about the study before making a voluntary decision to participate. Before collecting the data, a member of the Finnish Advisory Board on Research Integrity was consulted regarding research and data collection around the indigenous population.
The processing of personal data was based on scientific research carried out in the public interest. The personal data processed, which was minimized, were data related to age, gender, education, area of work, job title and work experience. Ethical justification is provided by the limited research data related to the research topic, the need to develop family nursing at maternity and child health clinics, and the need to support multiple-birth families. The research results can be utilized extensively in the future (Finnish National Board on Research Integrity, 2023) If the questionnaire lacked the participant’s informed consent, the responses were not used. If participants wanted to ask for more information, the form included the contact information of the researchers. The questionnaire response and the participant could not be linked. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees and with the Helsinki Declaration (World Medical Association, 2024).
Results
Knowledge of Multiple Parenthood, Pregnancy and Childbirth
Midwives and public health nurses had the most knowledge about multiple-birth parenthood, pregnancy and childbirth, for which the median sum variables (Mdn) were 4.1 and the interquartile range (IQR) was 3.86-4.44. Midwives/nurses had knowledge of multiple pregnancies, the parent–child interaction related to multiple-birth families, challenges and concerns related to multiple-birth parenthood, and expectations regarding parental support (Table 3).
Knowledge of multiple-birth families among midwives and nurses (n = 92). Medians, interquartile ranges and p values of the summary variable groups. A median (Mdn) of less than 4 indicates a lack of knowledge

Table 3 Long description
.
However, examination of correlations between sum variables revealed a modest correlation between multiple pregnancy knowledge and the expectation of parental support (r = .343) and knowledge related to caring for children and understanding its demands (r = .376). When examining participants’ knowledge of the association of aspects of zygosity (monozygosity and dizygosity) with multiple-birth pregnancy monitoring and childbirth, 54% somewhat agreed or strongly agreed, but 25% did not know. Altogether, 69% of the participants somewhat agreed or strongly agreed on the association of multiple pregnancy with the risk of premature birth, while 24% did not know. Moreover, 74% of participants were completely sure of monozygotic twins being of the same sex and 88% of dizygotic twins being of the same or a different sex.
Knowledge of Midwives/Public Health Nurses Concerning Multiple-Birth Family Interaction
Midwives and nurses had the least knowledge of parent–child interaction in a multiple-birth family, with a median sum variable (Mdn) of 3.8 and an interquartile range (IQR) of 3.64-4.08. Participants’ multiple-birth family knowledge was clearly limited, related to early interaction and attachment between a parent and more than one child of the same age, as well as a parent’s different preference for their children (Mdn 3.44, IQR 3.23-3.70). In addition, knowledge was lacking on growing and developing as twins, such as the importance of child individualization (Mdn 3.9, IQR 3.60-4.30), the relationship between twins (Mdn 3.75, IQR 3.50-4.13) and support for the child’s speech development (Mdn 3.25, IQR 2.75-3.50). Knowledge was also limited on the comparison between children (Mdn 3.5, IQR 3.25-4.00) and its effects on the children’s growth and development. In these sum variables, the median (Mdn) was less than 4, indicating a lack of knowledge (Table 3).
Data on early interaction showed that participants fully agreed (99%) on the importance of early interaction for each child’s growth and development. Participants fully agreed (75%) and somewhat agreed (22%) on the contribution of foetal movement monitoring and hearing heart sounds to early interaction. However, the results showed dispersion, especially in the difficulty of forming early interactions in the multiple-birth family; only 14% strongly agreed, 40% partly agreed, 25% did not agree or disagreed, 18% partially disagreed and 3% strongly disagreed. In contrast, 95% of participants agreed or partially agreed that the separation after birth of twins caused the disruption of early interaction. Altogether, 83% of the participants pointed out that one child may feel closer to a parent than the other. However, none of the participants fully agreed with the parent’s different preference for a child based on the child’s gender, while 26% partially agreed, 32% agreed or disagreed, and 42% disagreed. On the parent’s preference for a more liked child because of its ease of care, 51% responded in the same direction and 49% in a different direction. The results indicate that the participants were uncertain about information related to multiple-birth families.
Knowledge of Midwives/Nurses Concerning the Relationship Between and Care of Children of the Same Age
Midwives and nurses had the second highest amount of knowledge concerning the relationship between and care of children of the same age, with a Mdn of 3.8 and an IQR of 3.62-4.12. The participants knew about the challenges and concerns faced by multiple-birth parents, the expectation of parental support, caring for children and understanding the demands of caregiving. However, little was known about the relationship between twins (Mdn 3.75, IQR 3.50-4.13) (Table 3).
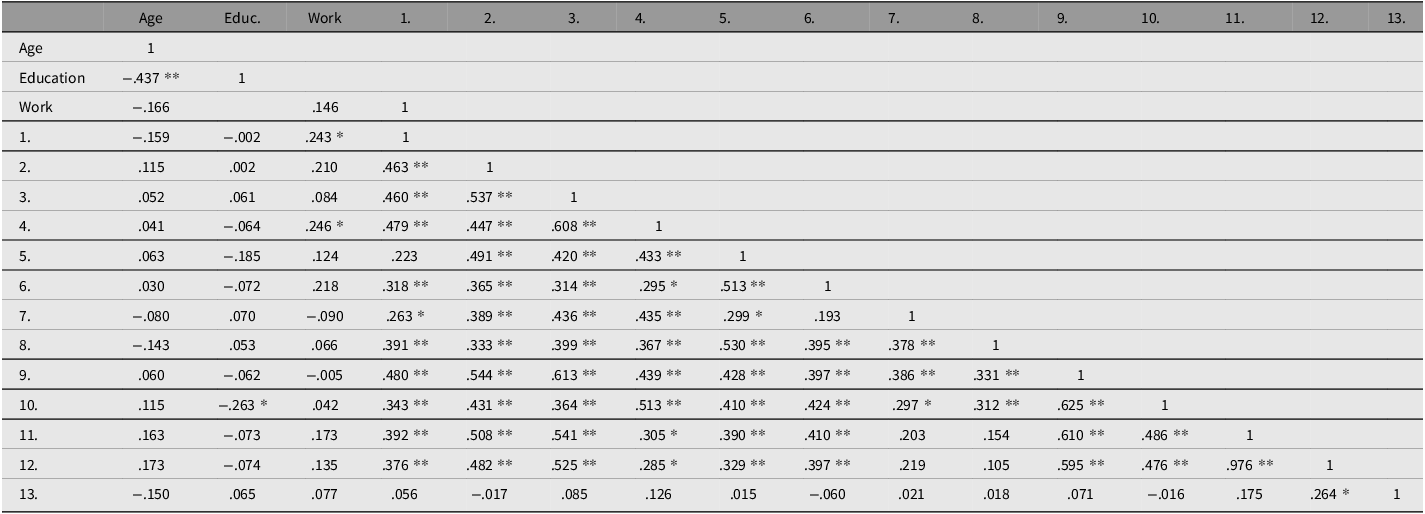
Examination of the correlations revealed that if participants had knowledge concerning the expectation of parental support, they also had fairly good knowledge about parent–child attachment (r = .431), the importance of child individualization (r = .513), the relationship between twins (r = .410), and the parent’s different preferences for the children (r = .424). In contrast, the level of knowledge was lower concerning early interaction (r = .364), comparison between the children (r = .312) and the children’s speech development (r = .297) (Table 4).
Multiple-birth family knowledge among midwives and nurses and Pearson correlation coefficients at statistically significant levels

Table 4 Long description
The table presents Pearson correlation coefficients among midwives and nurses, focusing on various aspects of multiple-birth family knowledge. It has 13 rows and 13 columns, including headers for Age, Education, Work, and numbered columns 1 through 13. Each cell contains correlation coefficients, with some marked with asterisks indicating statistical significance. Row 1 lists Age, Education, and Work. Rows 2 through 13 provide correlation values for different variables. Notable values include strong correlations such as .537 and .608, and weaker correlations like .002 and -.263. The table highlights significant relationships between different knowledge areas among participants.
Note: 1. Knowledge of multiple-birth pregnancy; 2. Bonding between mother and child; 3. Early interaction; 4. Individualization; 5. The intertwin relationship; 6. Parental favouritism a child/children; 7. Factors affecting twins’ speech; 8. Comparing the children with each other; 9. Challenges and concerns around parenting; 10. Support expected by parents; 11. Caring for children and understanding caregiving; 12. Caring, understanding and breastfeeding; 13. Breastfeeding.
**Statistically significant at the .01 level (two-tailed); *Statistically significant at the .05 level (two-tailed).
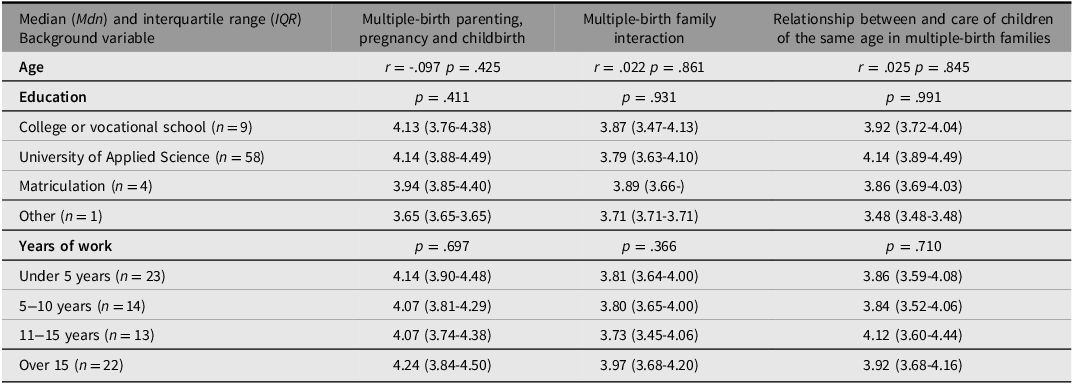
Impact of the Background Characteristics of the Participants
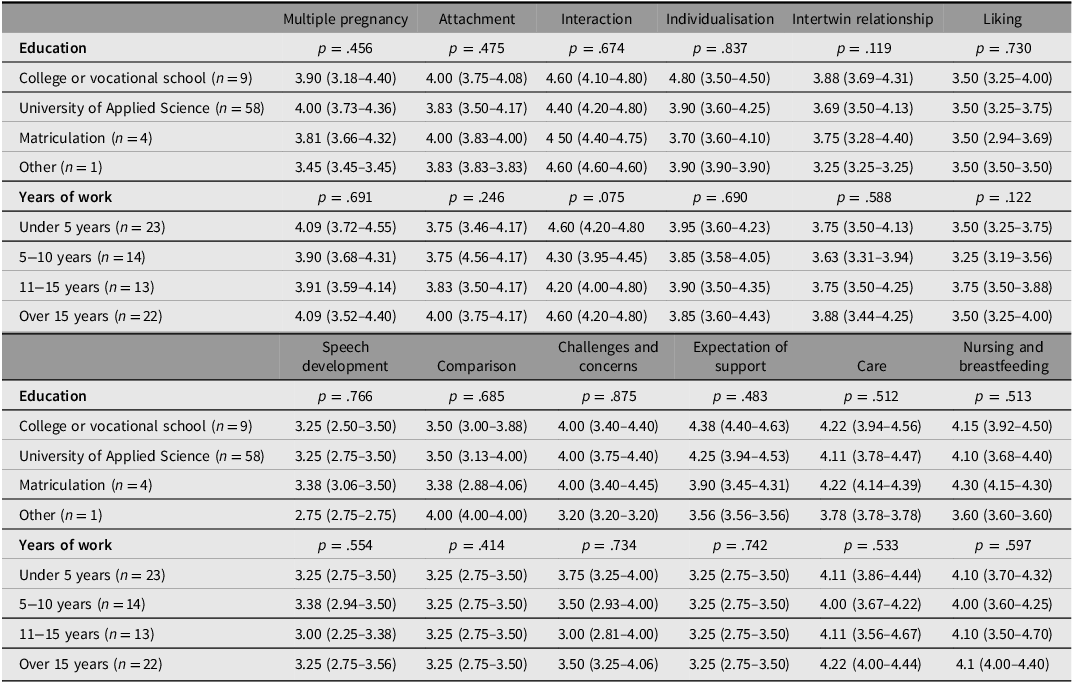
The background information on the participants, presented in Table 2, indicated that their age, educational level, and work experience had no statistically significant association with their multiple-birth family knowledge (at the 5% significance level). However, the effect of the area of work was that midwives and public health nurses who worked in maternity and child health clinics (n = 53) knew statistically significantly (p = .020) more about multiple pregnancies than those who worked only in child health clinics (n = 16) (Table 5).
Association of background factors of midwives and nurses with knowledge of multiple-birth families (n = 90). Medians, interquartile ranges and p values of summary variables. A median (Mdn) of less than 4 indicates a lack of knowledge

Table 5 Long description
A table comparing background factors of midwives and nurses with knowledge of multiple-birth families. The table has 11 rows and 4 columns. The columns are labeled as follows: Background variable, Multiple-birth parenting, pregnancy and childbirth, Multiple-birth family interaction, and Relationship between and care of children of the same age in multiple-birth families. The rows are labeled with different background variables such as Age, Education, and Years of work. Each row provides median (Mdn) and interquartile range (IQR) values for the variables. The table includes specific data points for different educational levels and years of work, along with p-values indicating statistical significance.
Discussion
Review of Results
This cross-sectional study investigated the multiple-birth family knowledge of midwives and public health nurses working in maternity and child health clinics. The results demonstrated that the respondents had most knowledge about multiple-birth parenting, pregnancy and childbirth and least knowledge about multiple-birth family interaction. No connection was found between the respondents’ age, level of education and work experience and their multiple-birth family knowledge.
Based on our results, we conclude that there were gaps in the participants’ knowledge regarding the monitoring and delivery of multiple pregnancies, information on twin types, and the risks of premature birth. The nursing work at the maternity clinic supports the preparation for parenthood, which in the case of multiple-birth families should be started well in advance due to the risks related to pregnancy. Our results showed that the respondents were aware of the need for multiple-birth family support but need more information on where the support expected by parents should be targeted, information on caring for children, and a comprehensive understanding of the situation of multiple-birth families. Multiple-birth families are families whose guidance and support of the children’s growth and development require different information compared to other families with children. However, the need for different types of support may not be recognized. Growth into multiple-birth parenthood begins with the knowledge that more than one child is expected in the family and the formation of an attachment relationship with the fetus and fetuses during pregnancy. Pregnancy means preparing for parenthood and caring for multiples but also preparing for the many everyday challenges (Heinonen, Reference Heinonen2015a, Reference Heinonen2015b, Reference Heinonen2015c; Reference Heinonen2022; Heinonen et al., Reference Heinonen, Häggman-Laitila and Moilanen2016). The monitoring and delivery of multiple pregnancies is planned individually. The more the fetuses have in common, the greater the risks, which should be considered starting from pregnancy monitoring (Kaprio, Reference Kaprio, Kumpula, Kaprio, Lavikainen and Moilanen2020). Almost 40% of twins are born prematurely, with a pregnancy duration of less than 37+0 weeks or up to 258 days. About 40% of twins weigh less than 2500 grams and 9% weigh less than 1500 grams (Tiitinen, Reference Tiitinen2023), and 42.9% of twins and 100% of triplets required neonatal intensive care/supervision after birth. Correspondingly, for one newborn, treatment was needed by 12.6% (THL, 2023). The risk of premature birth in multiple-birth pregnancies is considerable. Parents also often face the challenges of premature babies (Tiitinen, Reference Tiitinen2023). Respondents also had uncertainty about monozygosity (genetically identical) and dizygosity in relation to the child’s gender. The results show that education should highlight special knowledge related to multiple births, but also basic information. Previous research indicates that challenges in forming maternal interaction may also begin as early as pregnancy (Damato, Reference Damato2004a; Reference Damato2004b). According to Gowling et al. (Reference Gowling, McKenzie-McHarg, Gordon and Harrison2021), mothers of twins described their worry and guilt, but also shame, about atypical attachment when there is more than one fetus. Receiving information and discussing the attachment relationship, in addition to support, reinforces the normalization of the situation during pregnancy.
Our results indicate that information is needed about attachment, the parent’s preference for the child, the individualization of the child, the importance of comparing children with each other, and information related to speech development. The results demonstrate that although midwives and nurses had knowledge of multiple-birth family interaction, there were gaps in the information: for example, only 14% of the respondents recognized the challenges of early interaction and attachment to several children at the same time. Although they had knowledge about general interaction, it is difficult to apply this to a multiple-birth family situation. This result is in line with previous research on the lack of knowledge among professionals and the need for multiple-birth family information (Heinonen, Reference Heinonen2013, Reference Heinonen2017; Turville et al., Reference Turville, Alamad, Denton, Cook and Harvey2021). After the birth of multiples, parents may have challenges in interaction and forming an attachment (Bryan, Reference Bryan2003; Moilanen, Reference Moilanen and Alkio2007; Moilanen & Pennanen, Reference Moilanen and Pennanen1997), as one-on-one time with one child is scarce and mainly in care situations (Robin et al., Reference Robin, Josse and Tourette1988). In multiple-birth families, interaction in care situations is at least three-way (triad) (Moilanen et al., Reference Moilanen, Kunelius, Tirkkonen, McKinsey Grittenden, Grittenden, McKinsey and Claussen2003; Robin et al., Reference Robin, Josse and Tourette1988) and the presence of another child makes it difficult to form an interactive relationship (Manninen, Reference Manninen, Niemelä, Siltala and Tamminen2003; Trias, Reference Trias2006). Maternal unresponsiveness has shown to be exclusively linked to being the parent of twins and the twin parenthood has a significant effect on maternal mental health and on the quality of mother-infant interaction (Crugnola et al., Reference Crugnola, Ierardi, Prino, Brustia, Cena and Rolle2020). Parental guidance requires information on how to balance the situation and give individual attention to the child.
According to the results, midwives and nurses need to strengthen their knowledge of the relationship between twins, especially the importance of child individualization, reducing mutual comparisons, and supporting speech development. There is also a lack of knowledge concerning a parent’s different preference for multiples and unequal attachment. In all these groups of sum variables, the median was less than 4, indicating a lack of knowledge. The findings of Ionio et al. (Reference Ionio, Mascheroni, Lista, Colombo, Ciuffo, Landoni, Daniele and Gattis2022) showed that mothers interacting with 3-month-old monozygotic twins paid less attention to their children’s needs and displayed less positivity and warmth in caregiving situations than mothers of children of different ages. Parents may prefer twins in different ways (Moilanen & Pennanen, Reference Moilanen and Pennanen1997; Trias, Reference Trias2006), such as mothers preferring a weaker and smaller or a larger and more sociable child (Piontelli, Reference Piontelli2002) or perceiving the firstborn child as easy to care for, healthy and less demanding than the second child (Hay & O’Brien, Reference Hay and O’Brien1984). Public health nurses at the maternity clinic have also observed a parent’s different attitudes and favoritism in relation to the other child (Heinonen, Reference Heinonen2013). Equal and balanced attachment of both parents to both children is important for the development of a healthy personality. A prerequisite for a child’s healthy psychological development is that he or she can first form a sufficiently secure attachment relationship with his or her parent and then with the twin sibling (Manninen, Reference Manninen, Niemelä, Siltala and Tamminen2003). Trias (Reference Trias2006) found that excessive dependence and a close relationship between twins have effects on the children’s wellbeing, somatic symptoms and experiences of melancholy and depression, and that very strong leadership or submissiveness is reflected in the emotional life of twins (Trias, Reference Trias2006; Trias et al., Reference Trias, Ebeling, Penninkilampi-Kerola and Moilanen2010). In order to guide parents, midwives/nurses need multiple-birth family knowledge about early interaction and attachment. Deep knowledge and early intervention are also needed for issues that may be difficult for a parent to raise (e.g., preference). Challenges related to multiple-birth family interaction should already be discussed with parents during pregnancy. In order to support the child’s growth and development, multiple-birth family competence must be strengthened due to the special characteristics of twin relationships.
In this study, the participant’s awareness of the expectation of parental support was linked to knowledge of caring for children and its demands. This finding is in line with previous research on the need for support and assistance in childcare (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013; Leonard, Reference Leonard2000), breastfeeding (Cinar et al., Reference Cinar, Alvur, Kose and Nemut2013; Jonsdottir et al., Reference Jonsdottir, Flacking and Jonsdottir2022), putting children to sleep (Heinonen, Reference Heinonen2013; Heinonen et al., Reference Heinonen, Häggman-Laitila and Moilanen2016), and supporting individuality (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013; Robin et al., Reference Robin, Corroyer and Casati1996; Robin et al., Reference Robin, Josse and Tourette1988). Staying up at night affects parents’ coping and causes stress and exhaustion (Heinonen, Reference Heinonen2013). Due to the lack of time, there is also concern about the lack of attention paid to other children in the family (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013). Turnville et al. (Reference Turville, Alamad, Denton, Cook and Harvey2021) found that nurses and parents alike need information especially on caring for multiple children. It is significant that the needs of the former are related to multiple-birth family information and partly closely to the information needed and expected by parents (Heinonen, Reference Heinonen2013).
The results indicate shortcomings in the multiple-birth family knowledge of midwives and public health nurses working in maternity and child health clinics. A participant’s better knowledge of the expectation of multiple-birth parental support was associated with greater knowledge of attachment, individualization, the twin relationship, and a parent’s preference for the child. The weakest knowledge concerning the expectation of parental support was also associated with poor knowledge of children’s speech development. Although midwives and public health nurses are aware of the expectations and need for parental support, their multiple-birth family knowledge is lacking. Diverse training and continuing education on early interaction and attachment have been available for social and health care professionals, which increases knowledge of the subject. However, there is a strong impression that the information available is not always sufficient and/or applicable to multiple-birth families. Previous studies have shown that social and healthcare professionals face challenges in understanding and supporting multiple-birth families and have highlighted the need for training (Harvey et al., Reference Harvey, Athi and Denny2014; Heinonen, Reference Heinonen2013, Reference Heinonen2017; Turville et al., Reference Turville, Alamad, Denton, Cook and Harvey2021). The lack of multiple-birth family knowledge and training among care workers contributes to the unmet care needs of families with multiples (Heinonen, Reference Heinonen2013; Heinonen et al., Reference Heinonen, Häggman-Laitila and Moilanen2016; Jonsdottir et al., Reference Jonsdottir, Flacking and Jonsdottir2022; Turnville et al., Reference Turville, Alamad, Denton, Cook and Harvey2021) Social and healthcare professionals have observed multiple-birth families to be families with different individual needs compared to those with children of different ages (Heinonen, Reference Heinonen2013, Reference Heinonen2017). In order to be able to take into account and support the individual needs of multiple-birth families from the beginning of pregnancy, midwives and public health nurses working at maternity and child health clinics must have a broad understanding and competence regarding the information and support needs of multiple-birth families.
Reliability
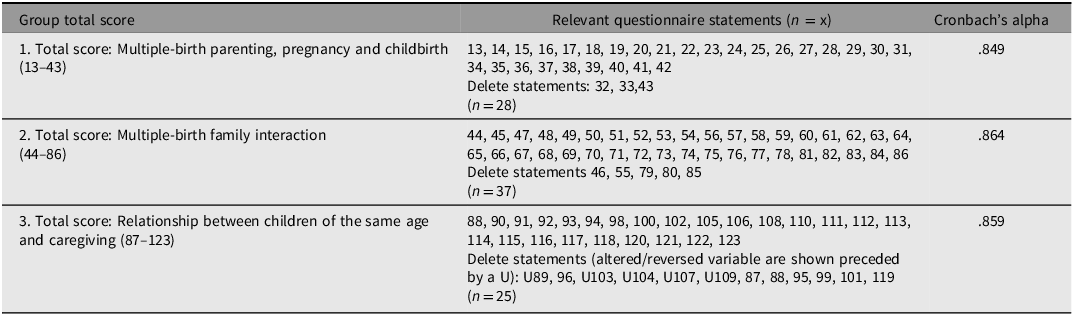
The Joanna Briggs collaboration evaluation criteria for a cross-sectional study are utilized in the consideration of reliability (Hoitotyön tutkimussäätiö [Hotus], 2026). Multidisciplinary knowledge and research, as well as related expertise, were utilised in the preparation of the questionnaire. The questionnaire was developed in several stages. Feedback was given by experts, and the feedback focused on the content, the clarity and quantity of questions and statements, as well as the use of time. A separate Content Validity Index measurement was not used, but the expert group was multidisciplinary from a subject perspective. The indicator developed for the study indicates good reliability (over 80%). The reliability of the questionnaire sections was studied with Cronbach’s alpha (α) and detailed results are given in Tables 6 and 7 for all topic areas.
Group total score, relevant questionnaire statements and Cronbach’s alpha

Table 6 Long description
The table presents data on group total scores, relevant questionnaire statements, and Cronbach's alpha values. It has three rows and three columns. The columns are labeled 'Group total score', 'Relevant questionnaire statements (n = x)', and 'Cronbach's alpha'. The rows detail different aspects of the questionnaire: 1. Total score: Multiple-birth parenting, pregnancy and childbirth (13-43), 2. Total score: Multiple-birth family interaction (44-86), and 3. Total score: Relationship between children of the same age and caregiving (87-123). Each row lists specific questionnaire statements and the corresponding Cronbach's alpha value. For example, the first row includes statements 13 to 42 with a Cronbach's alpha of 0.849, the second row includes statements 44 to 86 with a Cronbach's alpha of 0.864, and the third row includes statements 88 to 123 with a Cronbach's alpha of 0.859. Some statements are marked for deletion.
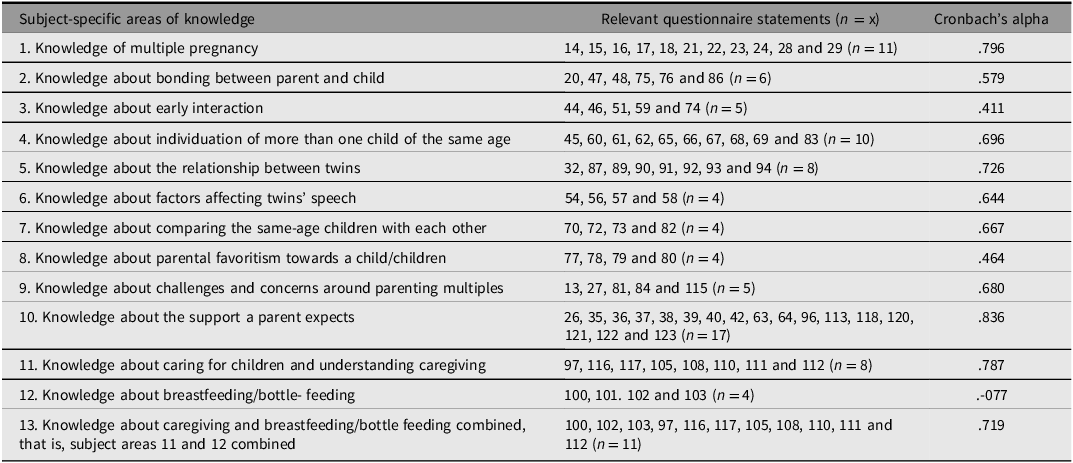
Subject-specific areas of knowledge, relevant questionnaire statements and Cronbach’s Alpha

Table 7 Long description
The table has three columns: Subject-specific areas of knowledge, Relevant questionnaire statements (n = x), and Cronbach's alpha. It contains 13 rows, each detailing a specific area of knowledge, the relevant questionnaire statements, and the corresponding Cronbach's alpha value. Row 1: Knowledge of multiple pregnancy, 14, 15, 16, 17, 18, 21, 22, 23, 24, 28 and 29 (n = 11), 796. Row 2: Knowledge about bonding between parent and child, 20, 47, 48, 75, 76 and 86 (n = 6), 579. Row 3: Knowledge about early interaction, 44, 46, 51, 59 and 74 (n = 5), 411. Row 4: Knowledge about individuation of more than one child of the same age, 45, 60, 61, 62, 65, 66, 67, 68, 69 and 83 (n = 10), 696. Row 5: Knowledge about the relationship between twins, 32, 87, 89, 90, 91, 92, 93 and 94 (n = 8), 726. Row 6: Knowledge about factors affecting twins' speech, 54, 56, 57 and 58 (n = 4), 644. Row 7: Knowledge about comparing the same-age children with each other, 70, 72, 73 and 82 (n = 4), 667. Row 8: Knowledge about parental favoritism towards a child/children, 77, 78, 79 and 80 (n = 4), 464. Row 9: Knowledge about challenges and concerns around parenting multiples, 13, 27, 81, 84 and 115 (n = 5), 680. Row 10: Knowledge about the support a parent expects, 26, 35, 36, 37, 38, 39, 40, 42, 63, 64, 96, 113, 118, 120, 121, 122 and 123 (n = 17), 836. Row 11: Knowledge about caring for children and understanding caregiving, 97, 116, 117, 105, 108, 110, 111 and 112 (n = 8), 787. Row 12: Knowledge about breastfeeding/bottle-feeding, 100, 101, 102 and 103 (n = 4), -077. Row 13: Knowledge about caregiving and breastfeeding/bottle feeding combined, that is, subject areas 11 and 12 combined, 100, 102, 103, 97, 116, 117, 105, 108, 110, 111 and 112 (n = 11), 719.
The indicator as part of the questionnaire should be further developed and tested. The study recruited participants who worked in nursing at maternity and child health clinics and who had experience of working with multiple-birth families. The number of participants in the research presentation sessions is based on information provided by supervisors. Reliability is increased by the representativeness of the sample and reasonably good response rate. Data were collected in different parts of Finland to obtain a broader overall picture. The validity was confirmed by asking the same question at two different points on the form (Polit & Beck, Reference Polit and Beck2022). Reliability could also have been increased by repeated measurement or more detailed interviews. During the data collection, participants were reminded once and the response time was extended by one week, which did not significantly increase the number of responses. The survey took place during the COVID-19 pandemic, which may have affected the response activity. The expertise of a biostatistician was utilized in the selection of statistical analyses. When interpreting the answers, it is good to consider the acquiescence bias. If respondents are not quite sure in their response whether they agree, they are more likely to choose to agree or what is socially acceptable (Pasek & Krosnick, Reference Pasek, Krosnick and Leighley2010).
Based on the research results, information is needed on multiple-birth parenthood and preparation for it, support for multiple-birth families and challenges faced by the families already from the beginning of pregnancy, interaction and attachment between the parents and child(ren), the mutual relationship between multiple-birth children, the special characteristics of supporting the growth and development of multiple-birth children, and caring for multiple-birth children.
Conclusions and Further Research
Social and health workers play a key role in supporting and informing multiple-birth families. The knowledge and skills of midwives/health nurses working in maternity and child health clinics in the field of multiple-birth families need to be strengthened through training and continuing education. Midwives/nurses have general knowledge, but it is difficult to apply it to the multiple-birth family situation. There are clear gaps in knowledge about multiple-birth families. Education and training should be developed, and further training provided to increase this knowledge.
Counseling services for multiple-birth families and other families with special needs should be developed, drawing on multidisciplinary expertise, to better meet the needs of the families. Development cooperation should be multidisciplinary, involving actors from different organizations (universities, universities of applied sciences, nursing organizations).
The evidence-based nature of care for multiple-birth families should be strengthened. Multidisciplinary cooperation is needed in research on multiple-birth families and in the development of the skills of social and health professionals. There is a need for further research on the specific knowledge required by multiple-birth families in different care settings. Research is also needed on education and training in social and health care and its effectiveness.
What is New in This Article?
A multiple-birth family must be treated from pregnancy onwards as a family with special needs. Specific information is needed about expecting, giving birth to, and parenting more than one child of the same age, early interaction and attachment, supporting the growth and development of multiples, and their interrelationship and care. Training should be given to midwives and nurses working in maternity and child health clinics to strengthen their knowledge of multiple-birth families.
Acknowledgments
We would like to thank all those who participated in the study. We also thank knowledge specialists Tuija Korhonen ja Katri Larmo, biostatistician Hanna Granroth-Wilding and Ville Kinnula and language help university lecturer Roy Siddall.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.
Ethics
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees and with the Helsinki Declaration. All relevant ethical guidelines have been followed during research process.
Responsibilities
Research design: KH, JK, KV-J. Data collection: KH, JK, KV-J. Data analysis: KH, JK. Writing of the manuscript: KH, JK, KV-J. Commenting on the manuscript: KH, JK, TR, KV-J. Approval of the manuscript: KH, JK, TR, KV-J.

 Open access
Open access