


In the US, disability civil rights laws, in particular the Americans with Disabilities Act 1 and the Rehabilitation Act, 2 require medical centers that are publicly owned, provide services to the public, or are federally funded to ensure that people with disabilities are not discriminated against with respect to access to their services, programs, and/or benefits. This non-discrimination requirement includes a right to reasonable accommodations, if requested. Yet people with disabilities, particularly those with mental illness, are routinely excluded from participation in clinical research, which is generally subject to US disability civil rights laws for the reasons noted above, i.e., funding, site of performance, and public service. A recent analysis of trials, for example, showed exclusion of people with psychiatric disability in 68 percent of clinical trials.Reference Plosky 3 That analysis reported that only a minority of studies included any justification for exclusion, the most frequent of which referred to concerns about participant safety or the interpretation of study results.Reference Plosky 3 Of course, other reasons such as medical contraindications (e.g., drug-drug interactions), concerns about participant reliability or ability to consent, and discrimination may exist, but not be documented. Exclusion occurs both in research about mental illness, for example, excluding more symptomatic patients from clinical trials of psychiatric treatments, as well as in clinical research more broadly, including both observational and investigational studies. Beyond contravening legal requirements, such exclusion compromises the scientific quality and generalizability of research, violates ethical principles of equitable participant selection 4 and equitable research access for underrepresented groups, 5 and deprives people with mental illness of potential benefits from clinical research. Clearly, there is an ethical, legal, and scientific imperative to improve access to clinical research for people with mental illness. This is particularly compelling when the condition under study is the treatment of a mental health condition or a condition that might be related to mental health, but the importance of equitable access is not limited to such research.
To this end, this article explores the use of supported decision-making as a means for including people with mental illness in both mental health- and non-mental health-related clinical research. Reluctance to include people with mental illness in clinical research may arise from concerns about capacity to consent, which are often based on a lack of familiarity with the capacity of people with mental illness and its dynamic nature. Although mental illness can impact decision-making capacity in select situations, broad and routine exclusion of people with mental illness without offering individualized assessments of decision-making capacity, including necessary accommodations, is a form of discrimination. Supported decision-making provides a means to enhance capacity to consent and directly addresses a common reason for clinical research exclusion of people with mental illness.
Supported decision-making is a strategy that allows people to select trusted others to help them understand, make, and communicate decisions. Following the model of the United Nations Convention on the Rights of Persons with Disabilities,Reference Res 6 supported decision-making has been directed to enabling individuals with reduced decision-making capacity to continue to make decisions on their own. In some US states, support arrangements have formal legal recognition. However, even without formal legal recognition, informal support arrangements comprise good clinical practice for many patients, enabling people to make and communicate decisions about their care. Specifically, it is commonplace, recommended, and backed by evidence that bringing a companion, such as a family member or friend, to medical visits improves patient understanding, communication, and outcomes.Reference Wolff and Roter 7
Given the utility of support arrangements in clinical care, it is important to consider how they may also function as accommodations for participation in clinical research.Reference Bierer 8 Supported decision-making may aid individuals with reduced decision-making capacity to participate in clinical research by involving supporters who assist them in understanding, making, and expressing their informed choices about research participation. By enhancing these required elements of capacity, supported decision-making thereby strengthens the capacity of individuals with reduced decision-making capacity and may permit them to make their own autonomous decisions about research participation. In contrast to surrogate decision-making, where decisions are made by someone else on behalf of the individual, supported decision-making allows the participant to remain the ultimate decision-maker.Reference Kohn, Dinerstein and Wright 9 Supporters may assist in various ways, such as simplifying complex information, helping with communication between the participant and the research team, and providing reminders about how or when to do something required of the trial, among other ways. This support can enhance the participant’s understanding of and communication about the study and permit the participant to demonstrate the necessary elements of decision-making capacity and to provide voluntary informed consent, utilizing their own autonomous capacity to consent to research participation. In the event a participant is unable to demonstrate capacity to consent even with support, then surrogate consent, if approved for a research protocol, would be required.
Much prior work on supported decision-making has focused predominantly on adults with intellectual and developmental disabilities. However, cognitive disabilities that start in early life and are relatively stable present different opportunities and challenges for supported decision-making than other kinds of medical conditions. This article considers mental illness as a central case, with the recognition that similar observations may apply to other conditions with intermittent or variable decision-making capacity such as neurological disorders (e.g., relapsing/remitting multiple sclerosis, traumatic brain injury, and encephalitis), severe hypothyroidism or nutritional deficiencies, or extreme pain, among others. Conditions that cause intermittent communication disabilities, despite intact cognitive capacity, would raise similar considerations for the use of supported decision-making. Progressive neurological conditions, such as Alzheimer’s, Parkinson’s, and Huntington’s diseases, also raise separate considerations for supported decision-making, as they cause cognition to worsen progressively and predictively over time.Reference Largent, Peterson and Karlawish 10 These situations also are distinct from short-term reversible conditions, such as acute intoxication or delirium, that cause a temporary lack of decision-making capacity, as well as scenarios in which people fully lack any meaningful way to participate in decision-making, such as people in a coma or without a functional communications system, or research in which consent has been waived, where supported decision-making does not have a role.
Mental illness poses challenges for the inclusion of participants in clinical research due to its effects on decision-making capacity. Mental illness can be dynamic and vary widely in nature (e.g., diagnosis, symptom severity, functional impairment) and duration (e.g., short-term, episodic, intermittent, progressive, permanent). A key feature of mental illness is that variation or reduction in decision-making capacity may be anticipated over the course of a longitudinal research study. Although decision-making capacity may manifest differently in different types of mental illness, distinctions among different types of mental illness are not particularly helpful in evaluating decision-making capacity. Decision-making capacity must be assessed on an individualized basis and cannot be determined categorically based on a diagnosis alone. For example, some people with schizophrenia retain decision-making capacity, while some with depression do not. The common thread is that mental illnesses may influence cognitive ability in variable and fluctuating ways, which can lead to intermittent decision-making capacity or capacity that varies in degree from having to lacking capacity at different times due to episodic symptoms. To determine how that impacts a particular person with mental illness, regardless of the specific diagnosis, an individualized assessment of decision-making capacity by an appropriately trained and credentialed clincian is required. Moreover, that capacity assessment may need to be repeated as the illness and symptoms evolve. Historical bright lines about decision-making capacity in mental illness, such as the idea that people with psychosis as a category cannot make their own decisions, are not scientifically supported.
Although a full discussion of the clinical assessment of capacity is beyond the scope of this article, it is worth noting that decision-making capacity is determined at a point in time: it is an individual’s ability to make, comprehend, and communicate an informed decision about a specific question at a specific time. Decision-making capacity changes over time and varies with the decision being made; more complex decisions typically require higher levels of capacity. 11 In clinical research, more complex or more risky trials may, as a matter of fact, require more cognitive ability to understand or appreciate. Enrollment in more complex or high-risk trials ethically requires a higher standard of capacity, especially where the benefits for the participant are limited, for example, in phase I cancer clinical trials.
Determining the amount or sufficiency of capacity required for different decisions is made even more complex by the typically subjective and binary nature of capacity assessments in clinical research, which most often involve a physician or clinical investigator doing a one-on-one clinical interview with a potential participant prior to enrollment and using their clinical judgment to decide if the participant can consent to study participation. As governed by the Common Rule in the United States, 12 clinical research requires a binary “yes” or “no” answer to whether a participant has capacity and can consent to research participation. This binary decision is problematic and does not reflect the reality that decision-making impairment is a complex clinical phenomenon that is context- and time-dependent and occurs along a continuum of ability with wide grey areas. The variable threshold for sufficient capacity, the lack of standardization of the criteria for assessment, and the binary adjudication of capacity are reasons to be critical of capacity determinations in clinical research.
Further, it is essential to note that refusing research enrollment — or refusing the assistance of a supporter — is never, in and of itself, an indicator of decision-making incapacity. It is the capacity to decide, rather than the decision itself, that should be evaluated as part of a decision-making capacity assessment. Disagreement with a clinician’s or investigator’s recommendation is not alone a basis for saying that a participant is irrational or lacks decision-making capacity. The decision about research enrollment or support must be voluntary and must reflect a person’s will and preference, but it cannot be judged according to what researchers or others would consider to be a good choice. Capacity assessments are necessary any time there is a question about a person’s understanding or ability to make decisions — not just when a participant disagrees — to be certain that the choice represents their will, values, and an informed understanding and appreciation of the decision being made.
This article explores considerations for the use of supported decision-making in clinical research for people with intermittent cognitive impairment related to mental illness, which may impact decision-making capacity to varying degrees at different times. These include challenges in the selection of a supporter, what to do at points in the trial if needed support becomes unavailable, when to reassess decision-making capacity, what to do when a person in a more symptomatic phase changes their mind about support or trial participation, and how to determine if supported decision-making has become surrogate decision-making in practice. Further, the article addresses how the continuum of risk (from survey research to interventional trials of investigational products), burden, and benefit of the clinical trial impact these considerations and the need for other relevant protections through the life cycle of trial participation. Recommendations for research teams, institutions, and institutional review boards (IRBs) are provided (Table 1).
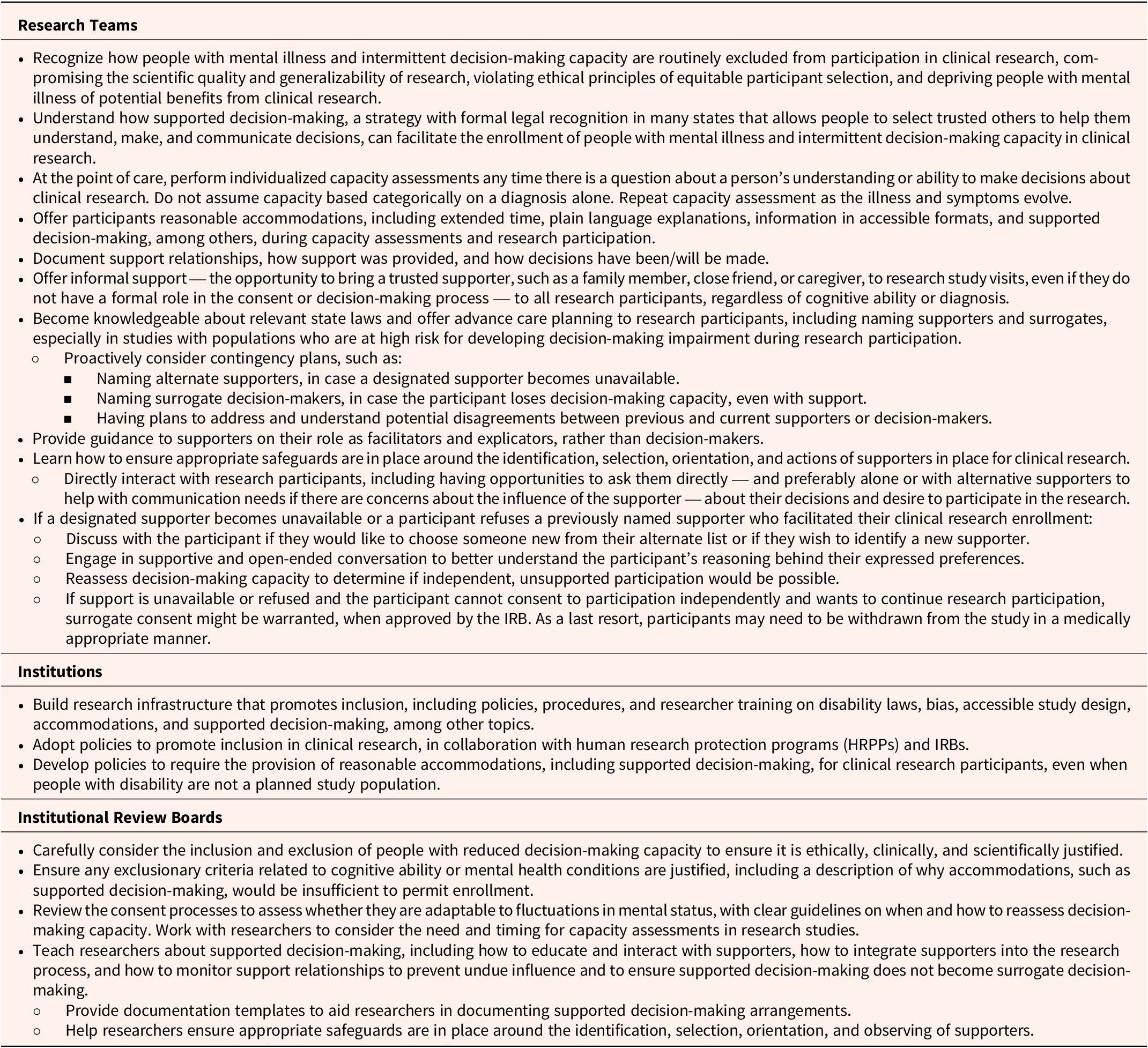
Recommendations for Research Teams, Institutions, and Institutional Review Boards (IRBs)

Table 1: Long description
The table is divided into three main horizontal sections, each anchored by a bolded stakeholder group heading. At the top, Research Teams are listed with nine primary bullet points, including recognizing exclusion of people with mental illness, understanding supported decision-making, performing individualized capacity assessments, offering reasonable accommodations, documenting support relationships, offering informal support, learning relevant laws and advance care planning, providing guidance to supporters, and ensuring safeguards for supporters. Several bullets contain nested sub-bullets, such as contingency planning for alternate supporters and addressing disagreements. The middle section, Institutions, contains three bullet points: building inclusive research infrastructure, adopting policies for inclusion in collaboration with H R P Ps and I R Bs, and developing policies for reasonable accommodations including supported decision-making. The bottom section, Institutional Review Boards, lists four main recommendations: careful consideration of inclusion and exclusion criteria, justification for exclusionary criteria, reviewing adaptable consent processes, and teaching researchers about supported decision-making. This section includes sub-bullets on providing documentation templates and ensuring safeguards for supporters. All recommendations are presented in a top-to-bottom sequence within each group.
Challenges with Selecting and Retaining a Supporter for Clinical Research
Supporters are usually trusted individuals chosen by the person seeking support to assist them in making informed decisions, among other types of support.Reference Hyseni 13 These supporters may include family members, close friends, caregivers, or other individuals who ideally have an established, meaningful relationship with the participant and an understanding of their values, communication style, and preferences.
The selection of a supporter is a highly individualized process and must be fully voluntary on the part of the person being supported. This ensures that the supporter is someone whom the person trusts to respect their autonomy and choice rather than to impose the supporter’s own preferences. Ideally, the supporter’s role is collaborative and aimed at enhancing the person’s ability to engage in the decision-making process without undermining their independence. Some people may prefer to select different supporters for different decisions, for example for health care decisions or for financial matters.Reference Peterson, Karlawish and Largent 14 This may also include low-risk versus high-risk healthcare decisions or routine clinical care versus investigational clinical research. Ensuring that individuals can freely choose their supporters — and change them if needed — is critical to the implementation of supported decision-making.
For individuals with mental illness, identifying a trusted supporter can be a difficult process. Severe and chronic mental illness typically impacts relationships, sometimes leading to social isolation, strained family dynamics, or loss of long-term friendships, potentially reducing the pool of close trusted contacts who could be potential supporters. The symptomatic phases of other disorders can give rise to similar challenges. Some conditions, such as bipolar disorder, schizophrenia, or severe depression, may involve psychosis, paranoia, or fluctuations in mood, making it harder during symptomatic phases to accurately perceive someone else’s intentions or to be able to put trust in another person. Similarly, some personality disorders limit the ability to have consistent trusting relationships. People with mental illness may also experience stigma or fear of judgment by others, making them hesitant to reach out to potential supporters. In some cases, individuals may have a history of trauma or mistreatment (which is more common among people with mental illness than the general population), 15 further complicating the process of selecting someone they trust to be a supporter.
When possible, advance planning may mitigate some difficulties with selecting trusted supporters. Clinicians and researchers could anticipate and discuss the potential roles for supporters and the applicability of already existing support arrangements during less symptomatic phases or at times prior to when support is needed. When no personal connections are available, trained professionals or advocates may step in as supporters, although there may be legal limits on the formalization of these arrangements in some states. In such cases, it will be important to ensure that these supporters are impartial, continue to work with the individual as the decision-maker, and do not step into the role of surrogate unless otherwise authorized and necessary. Ongoing work to address the potential role of trained professionals or advocates is needed.
What Happens If Difficulties Arise with the Support Arrangement During Trial Participation?
In addition to the challenges with selecting and relying on a supporter, it is possible that support arrangements may break down during trial participation. Here, too, anticipation and contingency planning are important. As symptoms fluctuate, participants may mistrust or reject support that they had previously welcomed. Supporters may become uncomfortable with their roles. Or supporters may become unavailable during trial participation for any number of reasons, including their own medical or mental conditions. When a supporter becomes unavailable during a clinical trial, just as when difficulties arise within the support arrangement, research teams should first determine if independent, unsupported participation would be possible. If not, consideration could be given to whether alternative support arrangements are possible. In the absence of capacity with or without support, surrogate decision-making might be warranted for some studies and would be legally permissible when approved by an IRB. 16 As a last resort, participants may need to be withdrawn from the study in a manner that is medically appropriate, e.g., safely tapering off medications and arranging necessary follow-up care.
Alternate supporters may be named and arranged in advance, to prevent any potential interruptions. When this has not occurred, the first step is to engage with the participant to determine whether they wish to identify a new supporter and, if so, to assist them in selecting someone they trust. This process should respect the participant’s preferences and timelines, as choosing a new supporter can be a significant and fraught decision. If the participant does not have another supporter, the research team should explore the possibility of identifying and providing a supporter to the participant. Importantly, researchers cannot impose a replacement supporter without the participant’s consent, as this would undermine the intent of supported decision-making.
If the participant chooses not to identify or accept a replacement supporter, the research team should work to provide additional accommodations that may serve the same function of enabling the participant to make and express their own choices about research participation, such as providing additional communication aids, giving more time to make decisions, and providing information in different and more accessible formats, although these measures should also have already been offered from the start. These measures are all intended to help increase decision-making capacity, which is required to provide informed consent and is usually necessary to participate in clinical research. By proactively addressing these scenarios through preestablished processes, research teams can foster continuity, prevent unnecessary withdrawal, uphold the participant’s inclusion in research, and promote the participant’s well-being and autonomy.
Moreover, supporters who remain available may be uncertain about their responsibilities or feel unprepared to assist with decisions related to clinical research. Supporters themselves may need help in understanding how to provide support, especially in responding to fluctuating symptoms and attitudes on the part of those for whom they are providing support. In such situations, attempts to educate the supporter and to work with them are essential. It is the responsibility of the research team to provide information to supporters in a way they can understand, just like the requirement for any informed consent process. Researchers will need guidance and training on how to educate and interact with supporters to include them in research participation most effectively.
Supported Decision-Making and Fluctuating Decision-Making Capacity
A defining characteristic of many mental illnesses is fluctuation in symptoms, where individuals may experience periods of stability interspersed with phases of heightened symptoms or distress. Bipolar disorder is a good example. During times of euthymia, a person with bipolar disorder may be asymptomatic and typically retain full cognitive ability and decision-making capacity. During an acute manic episode, however, the same person may have racing thoughts, grandiosity, and delusions that impact cognitive functioning and may not be able to understand or appreciate their condition sufficiently to make medical decisions for themselves. Over the course of this continuum of symptoms, this person will likely benefit from or require assistance in making medical decisions that might include supporters or even substituted decision-makers. In a multi-year longitudinal clinical research study, a person with bipolar disorder may go through many different mood states and related shifts in decision-making ability during research participation. As a result, the applicability and utility of supported decision-making would also fluctuate over time.
During periods of stability, an individual may be fully capable of understanding and making decisions independently, requiring little to no support. However, during symptomatic phases — such as episodes of severe anxiety, depression, mania, psychosis, or disorganized thinking — the same individual may experience worsening decision-making capacity and may benefit from supported decision-making to enable them to retain the capacity to consent. The intermittent and dynamic nature of mental illness makes the need for supported decision-making more variable compared to relatively static conditions like intellectual and developmental disabilities. More or less support, and different types of support, may be needed as symptoms change. As a result, supported decision-making arrangements must be flexible and anticipate that individuals may want to activate, disengage, or change support as their situations change.
This fluctuation in capacity also raises questions about when and how to reassess decision-making capacity during different stages of trial participation to best align with the participant’s evolving needs and preferences for research participation. Assessing decision-making capacity during a longitudinal clinical trial is an important and often poorly considered process. Research teams must consider how frequently and under what circumstances formal and informal reassessments of capacity should occur. For example, reassessment may be necessary at key study milestones, such as whenever re-consent is required for a protocol amendment, during follow-up study visits involving investigational drug or device administration, if study staff observe noticeable changes in a participant’s behavior or communications, and at the end of a study if the option for continued access to the intervention is offered.
Judgments about capacity reassessment must balance competing factors. On the one hand, reassessment of capacity provides an added safeguard to research participants by ensuring voluntary, informed participation. On the other hand, overly frequent or unnecessary capacity assessments can undermine a participant’s autonomy, be perceived as threats to dignity by making discriminatory assumptions via repeatedly questioning a participant’s decision-making capacity because of their diagnosis, and create an inappropriate obstacle to research participation. Reassessment plans must consider the risks and benefits of the study, characteristics of the study population, requirements of study participation, availability of new evidence, study changes, and the form taken by original consent to participation (e.g., supported decision-making or surrogate decision-making), among other factors. At the time of study design, researchers and sponsors, in consultation with their IRBs, should anticipate the need and timing for capacity assessments and should write this into the research protocol. At the same time, researchers should be aware that reassessment of capacity may be needed at any time in the moment of care when questions about mental status or decision-making arise. Finally, it is important to note that assessments of decision-making capacity themselves must always anticipate and include the provision of reasonable accommodations, including extended time, plain language explanations, and the presence of a supporter, among others.Reference Wright 17
In the context of fluctuating conditions like mental illnesses, research protocols should also clearly address plans for what happens next based on the results of decision-making capacity reassessments. Participants may need more or less support for ongoing trial participation. There will be times when the symptoms of mental illness may be too severe for supported decision-making to be sufficient to enable an individual to meet the demands of a consent process. In those cases, a switch to surrogate decision-making may be necessary, if it has been approved as an option by the IRB. If the switch is not a possibility, the participant may need to be withdrawn from the study in an appropriate manner. In other cases, a participant who has improved cognitive functioning may benefit from the opportunity to ensure their preferences have not changed from those expressed with the help of a supporter, to re-consent without the supporter, or to autonomously re-consent with or without a supporter if previous decisions had been made by a surrogate. By being proactive and implementing clear and consistent capacity assessment and consenting processes, research teams can safely and thoughtfully include individuals with mental illness in clinical research.
An important reminder in reassessing capacity is that the level of capacity required to enroll in a clinical research study is often higher than the level of capacity required to select a supporter or nominate a surrogate decision-maker. It is possible to envision a scenario where the participant cannot independently consent to study participation but still maintains the cognitive ability to consent with support. Participants may also select surrogates to consent for them through devices such as health care powers of attorney, even when they lack capacity to consent on their own. Depending on state laws, powers of attorney may also include consent to participation in research. What is necessary for appointment of a power of attorney is that the participant understand who they are selecting and what kinds of decisions the person will be able to make. To be sure, selection of a clearly unreasonable supporter or surrogate (such as an imaginary character, an unfamiliar figure, or the perpetrator of substantiated prior abuse) should warrant inquiry into whether the participant has even the comparably lower level of capacity needed. These complexities also highlight the need to consider the possibility that someone selected as a supporter, or who may try to volunteer to serve as a supporter, may not be appropriate to the role. In general, research teams should ensure that appropriate safeguards are in place around the identification, selection, and orientation of a supporter. Some safeguards could include having discussions with the participant alone about the choice of the supporter, gaining an understanding of and respecting the dynamics of pre-existing support relationships, monitoring supporter involvement to ensure it is in the best interests of the participant, and having parameters for independent assessment and potential rejection of supported decision-making arrangements when it is clear the supporter is substituting their own preferences, abusing their role, and/or harming the participant.
A particularly difficult set of questions arises around what to do if a participant appears to refuse support but is deemed not to have the capacity to make the decision to refuse. Should the support agreement at the time of trial enrollment be considered binding, on the analogy to a Ulysses contract which cannot be revoked in a time of incapacity? Is there a role for research advance directives to include discussion about the use of supporters in situations of diminished capacity, and if so, would those directives be binding? In Ulysses contracts, a past decision made by a competent individual is used to predetermine or override a future decision at a time when that person no longer has decision-making capacity. It has been argued that Ulysses contracts can be ethically justified in healthcare when they are used to uphold decisions that someone would have wanted when they had decision-making capacity, thereby protecting their autonomy and personal interests.Reference Spellecy 18 Similarly, some states do have legally binding advance directives for mental health treatment. 19 For example, during a time of stability and intact decision-making capacity, a person with bipolar disorder may agree in advance to specific treatments or preferences in care, like hospitalization or medications, for future manic episodes during which they might lack decision-making capacity and/or might refuse medical recommendations. As elaborated in the next section of this article, however, clinical research is different than medical treatment, especially non-therapeutic research with little or no prospect for direct benefit. Because of this, supported decision-making arrangements in clinical research should generally not be binding, and there should be a relatively low threshold of capacity required for a participant to refuse support and/or to refuse to participate in clinical research.
As people change their minds about support arrangements, it is essential to respond in a way that both respects their autonomy to the highest degree possible but also ensures their safety. One important safeguard is the requirement for reassessment of capacity at times of shifts between decision-making models. For example, consider a research participant who is assessed and has been found to lack capacity to consent independently for a study and then subsequently names a supporter and requests supported decision-making. The participant would need a reassessment of capacity with their supporter to determine if they are able to meet the demands of the consent process with the help of the supporter. In this scenario, to permit consent via supported decision-making, the clinician assessing capacity must pay careful attention to who is making decisions, i.e., to ensure it is the participant and not the supporter, and should document what changed between the capacity assessments, such as how the participant was able to understand or communicate better with the help of the supporter and how this now enabled the participant to meet the threshold for having capacity to consent.
If that participant then later refuses support and wants to continue in the research, reassessment of capacity would again be required to determine if the participant can consent independently or if surrogate consent or study withdrawal may be an appropriate course of action. Research teams must carefully discern whether the decision to refuse support reflects a stable, values-concordant, informed choice or is a temporary response to a symptomatic condition. Researchers are encouraged to engage in open-ended conversation to better understand a participant’s reasoning behind their expressed preferences. If the participant is opting out of using a supporter, the research team can explore whether other accommodations, such as additional time, alternative simplified language, the addition of imagery, or scheduling flexibility, may allow them to retain decision-making capacity without the use of a supporter. If the participant declines a supporter, is unable to make decisions on their own, and is willing to have a surrogate make decisions on their behalf, a shift to surrogate decision-making may be possible when surrogate consent has been approved by the IRB. Researchers should consider whether this option should be built into the study protocol at the time of initial submission to the IRB. In cases where a participant wishes to withdraw from the trial, even when their capacity is impaired, their decision should be respected unless there are exceptional circumstances, such as immediate safety risks to abrupt study cessation (e.g., acute medication withdrawal effects). Respecting dissent, even if capacity to consent is impaired, protects participant safety, for example, by avoiding physical risks of having to restrain or force study procedures onto a participant, and upholds a participant’s fundamental dignity, personhood, and bodily autonomy, even in the face of cognitive impairment. If the participant wishes to continue in the trial but refuses support or support is unavailable, the participant does not have the capacity to consent without support, and surrogate consent has not or cannot be authorized, the participant should be withdrawn from the research in a manner that is medically appropriate.
Because of these shifting scenarios, clinical research enrolling people with mental illness and intermittent decision-making capacity using supported decision-making may need to anticipate the possibility of increased frequency of withdrawals. Research protocols should include plans for study withdrawal in a manner that is safe and does not compromise the research participant. Enrollment numbers and plans for statistical analysis may need to account for this possibility. Although there is no evidence to date that a population enrolled with the provisions of supported decision-making does indeed have more withdrawals, this will need to be studied as the practice of incorporating supported decision-making into clinical research becomes more widely adopted. Regardless, the overall benefits of inclusion for scientific quality and generalizability of research, as well as being the right legal and ethical approach, outweigh this potential risk of increased study withdrawals, and the risk can be mitigated by appropriate trial planning and preparation.
Finally, consideration should be given to what happens after a participant’s mental status returns to a baseline, i.e., after the symptomatic phase improves, if they have previously withdrawn from the study. Will participants be given the option to reenroll in the research or to re-consent on their own, with or without the same or different supporters? Some clinical researchers may want to plan for such temporary pauses in research participation and to develop processes for how participants will be able to stop and later rejoin the study.
When enrolling participants with mental illness and intermittent decision-making capacity, research protocols should include clear plans for addressing these scenarios, with a goal of offering inclusion in research, respecting the autonomy of people with mental illness, and protecting them during their most vulnerable moments. Research protocols should describe and justify inclusion and exclusion criteria, plans for capacity assessment, and consent models used (e.g., independent, supported, or surrogate decision-making). Beyond the protocol, however, the accountability for ensuring participants understand and freely consent to research and are not excluded merely for convenience rests at the point of care with the medical and research teams.
Impact of Continuum of Risk and Benefit on Supported Decision-Making
Decisions to participate in clinical trials, particularly those with limited potential for direct therapeutic benefit, differ significantly from decisions to undergo clinical treatment. In clinical care, the primary goal is to benefit the patient. Patients typically make decisions based on expectations of improvements in their health, management of their symptoms, or prevention of disease. In contrast, while participation in research may sometimes offer direct benefits, the primary goal is typically the creation of generalizable knowledge and the advancement of science. These goals are often confused, with research participants deciding to enroll in research with limited potential for direct therapeutic benefit in the hope that it will benefit them, a phenomenon known as the therapeutic misconception.Reference Applebaum, Roth and Lidz 20 For some individuals with impaired decision-making capacity, understanding the differences between clinical care and research and the associated potential risks and benefits, which can be obscured by therapeutic misconception, can be especially challenging, and it requires special attention during capacity assessment and consenting processes. Similarly, when using supported decision-making, it is essential to ensure a supporter understands these distinctions.
At the same time, the level of risk and potential benefit to a particular research study are important factors in determining the level of capacity required for enrollment and the use of supported decision-making. As described above, the higher the risk or burden of participation, the higher the level of capacity required to enroll in research.Reference SACHRP, Buchanan and Brock 21 As such, it may be that a person would require a supporter to meet the demands of the consent process and to enroll in a riskier study, while they may be able to enroll without support in a less risky study. For example, a participant might require support to enroll in an investigational drug study but be able to consent without support to a low-risk survey study. Similarly, a participant might require support to enroll in an invasive investigational device study, for example a deep brain stimulation trial, but be able to consent without support to a lower-risk drug study. If two studies have equivalent risks but one has known direct therapeutic benefit and the other does not, the risk-benefit ratios differ; the level of capacity needed to enroll, therefore, and the potential need of a supporter, may also vary between the two studies.
Identifying Whether Supported Decision-Making Has Shifted to Surrogate Decision-Making
Determining whether supported decision-making has unintentionally shifted into surrogate decision-making requires careful observation of the participant decision-making process. The key distinction between supported decision-making and surrogate decision-making lies in who retains ultimate decision-making authority and how this authority is exercised in practice. Supported decision-making allows the participant to make their own autonomous decisions with support, while surrogate decision-making removes autonomy and places the final decision with the surrogate.
It is important to maintain the distinction between the two forms of decision-making and to identify when supported decision-making may have unintentionally shifted to surrogate decision-making. Signs that supported decision-making may be drifting into or have transitioned into surrogate decision-making include instances where the supporter dominates conversations, answers questions on behalf of the participant without their input, or dismisses the participant’s expressed preferences. This shift can also occur subtly if supporters frame options in a biased way that limits the participant’s perceived choices or overly influences the participant’s understanding of the research. To prevent this, research teams should directly interact with research participants, including having opportunities to ask them directly — and preferably alone or with alternative supporters to help with communication needs if there are concerns about the influence of the supporter — about their decisions and desire to participate in the research. Additionally, supporters should receive clear guidance on their role as facilitators and explicators, rather than decision-makers, and should be reminded that their purpose is to enhance the participant’s ability to make and express decisions rather than to make decisions for them. Education for researchers on how to interact with supporters and what to look out for is also important. Documentation of the support relationship, how support was provided, and how decisions were made can offer another important safeguard to ensure supported decision-making does not inadvertently shift into surrogate decision-making. Outside of supported decision-making arrangements, this is not dissimilar from good clinical practice or any other research enrollment, in which clinicians and researchers must ensure a patient or participant makes their own voluntary decisions, with input from but without inappropriate influence by others.
As described above, in other situations when a research participant’s capacity has diminished and they can no longer make autonomous decisions even with support, an alternative may be for supported decision-making to be replaced by surrogate decision-making, if permitted by law and allowed in the research protocol. In those situations, the supporter may be the same person or a different person from the surrogate. In particular, the participant may have prospectively named the same or different person to be a supporter and surrogate, such as by a healthcare proxy. In the absence of a named guardian or surrogate, in states where there is a state default surrogate statute, the supporter, by the nature of their relationship with the research participant, might have surrogate authority by default — or alternatively, that authority might default to an alternate party. These scenarios will vary depending on state laws and on whether state surrogate decision-maker statutes permit consent to participation in research. (Some state surrogate statutes include enrollment in research, while others do not.Reference Wright, Ariel Cascio and Racine 22 When this does not exist, it is common practice to apply the surrogate laws for medical care to clinical research, especially as the decisions made within the context of a clinical research study are often medical ones.) Nonetheless, it is easy to see how these transitions between decision-makers can be complicated and could lead to challenging situations in which decision-making authority could shift between parties and/or lead to disagreements between previous and current supporters or decision-makers. The best approach is to consider the need for supporters or surrogates in advance and to address these issues in research protocols and during the initial discussions about participation in the research. Researchers are advised to be knowledgeable about their state laws and to offer advanced care planning to research participants, especially in studies with populations who are at high risk for developing decision-making impairment during research participation.
How Do Decentralized Clinical Trials Impact Supported Decision-Making?
The conduct of clinical trials, particularly those that are virtual, decentralized, and/or reliant on technology, presents unique challenges for the practical implementation of supported decision-making. Virtual and decentralized trials often remove in-person interactions, which may make it more difficult for researchers to observe subtle cues of participant understanding or decision-making capacity. While this challenge applies to consent for all decentralized trials, it is particularly important when enrolling participants who are known to have intermittent decision-making capacity. Technology has the potential to hamper or, alternatively, improve the use of supported decision-making. On the one hand, it may limit opportunities for supports to effectively assist participants, for example, if a trial relies on online portals or video calls without built-in accommodations, or if technological limitations, such as limited internet access, unfamiliarity with digital platforms, or inability to conference in multiple parties, prevent the supporter from being present with the participant. On the other hand, technology may facilitate communication and understanding, for example, by deploying text-to-speech programs, and may enhance the effectiveness of supported decision-making. In designing decentralized trials, research teams should intentionally include procedures that facilitate communication and engagement, such as using accessible technology, ensuring the technological ability for designated supporters to join virtual meetings, and making available consent forms and study materials in multiple formats (e.g., large print, audio, and simplified language).
The research team should evaluate the feasibility and safety of remote and technology-based interactions with participant and supporter and whether additional accommodations are required to facilitate study enrollment and participation. Decentralized trials may require flexibility to include supporters who assist participants in different locations or time zones. Providing technical training for both participants and supporters and integrating user-friendly platforms can help mitigate these issues. Importantly, researchers must also consider privacy and data security, as supported decision-making typically includes sharing protected health information with the supporter. By addressing these logistical and technological considerations, decentralized clinical trials can effectively implement supported decision-making.
What Is the Role of Institutional Review Boards (IRBs)?
Institutional review boards play an essential role in ensuring the inclusion and protection of people with intermittent decision-making capacity, including those with mental illness, in clinical research. To fulfill this responsibility, IRBs must strike a balance between protection and inclusion, ensuring safeguards are in place to respect the autonomy of participants and to protect participants from potential harms, but also not to place unnecessary or discriminatory obstacles to their inclusion.Reference Friesen 23
During research protocol review, IRBs should carefully consider the inclusion and exclusion of people with decision-making impairment to ensure it is ethically, clinically, and scientifically justified.Reference Strauss, White and Bierer 24 Any exclusionary criteria related to cognitive ability or mental health conditions must be justified, including a description of why accommodations, such as supported decision-making, would be insufficient to permit enrollment. As described above, for clinical research anticipating the enrollment of people with intermittent decision-making capacity, IRBs should work with researchers to consider the need and timing for capacity assessments as part of the protocol review.
For studies intending to enroll participants with disability impacting decision-making capacity and anticipating the use of supported decision-making, IRBs should also evaluate how the use of supporters is described, with particular attention to how support will be managed during periods of fluctuating mental status. IRBs should ensure that consent processes are adaptable to fluctuations in mental status, with clear guidelines on when and how to reassess decision-making capacity without unnecessarily burdening participants or undermining their autonomy. On a case-by-case basis, IRBs have the regulatory responsibility for determining whether to approve surrogate decision-making in situations when capacity diminishes to the point where supported decision-making is no longer sufficient.
Beyond protocol-specific review, IRBs, working in collaboration with their human research protection programs and institutions, should adopt policies to promote inclusion in clinical research. Institutions should have policies requiring the provision of reasonable accommodations, including supported decision-making, for research participants, even when people with disability are not a planned study population. Institutions must develop a research infrastructure that promotes inclusion, including policies, procedures, and training on disability laws, bias, accessible study design, 25 accommodations, and supported decision-making, among other topics.
Toward that end, IRBs typically have a role in shaping institutional policy and contributing to researcher education. IRBs should be involved in helping to educate the research community about supported decision-making, including how to integrate supporters into the research process and how to monitor support relationships to prevent undue influence and to ensure supported decision-making does not become surrogate decision-making. By focusing on these considerations for protocol review, policy, and education, IRBs can play their part in improving the inclusion of people with mental illness and intermittent decision-making capacity in clinical research while ensuring their autonomy as well as their safety.
Conclusion
This article explores the special considerations for the use of supported decision-making in clinical research for people with intermittent decision-making capacity, as illustrated by the example of people with mental illness. In recent years, the clinical trial community has traditionally taken a dichotomous approach to this population, often excluding them inappropriately, for convenience, or based on diagnosis alone, in part due to a lack of familiarity with the capabilities of people with mental illness or to outright discrimination. Instead, a dimensional approach must be endorsed to include people with mental illness and intermittent decision-making capacity in research, with the requirement for an individualized capacity assessment with a supporter before deciding whether a participant is ineligible. Although certainly not required of all people with mental illness (as many mental illnesses do not impact decision-making capacity), when decision-making capacity is in question and may lead to research exclusion, supported decision-making should be offered as a reasonable accommodation prior to capacity assessment and throughout the entirety of research participation. This will further the aims of ethically sound research participation for individuals who may otherwise be excluded from research when decision-making ability is uncertain or impaired. Updated guidance to facilitate organizational development and implementation of comprehensive supported decision-making policies is imperative to ensure the ethical inclusion of this population in clinical research.
Incorporating supported decision-making into clinical research for people with mental illness and addressing the many possible nuances that might arise are likely to require education, changes in practice, and resources. This added burden risks even greater exclusion due to resource limitations or convenience. As such, it will be important for the field to wrestle with what accommodations are reasonable to require and whether the inclusion of people with mental illness in clinical research is impacted. Notably, some measures can be taken with minimal resource requirements. For example, informal support — the opportunity to bring a family member, close friend, or caregiver to research study visits, even if they do not have a formal role in the consent or decision-making process — should always be offered to research participants, regardless of cognitive ability or diagnosis, just as it is a part of good clinical practice.
Disclosures
There was no funding for this article. DHS receives consulting income as an external member of the Takeda Ethics Advisory Council.

 Open access
Open access