


Introduction
Reducing stigma and discrimination of people with mental health conditions remains a central priority in global mental health policy (World Health Organization, 2022). Stigma is associated with substantial adverse consequences, including reluctance to seek professional help due to concerns about acquiring a ‘spoiled identity’ (Goffman, Reference Goffman1963) and anticipated social rejection and discrimination (Clement et al., Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko, Bezborodovs, Morgan, Rüsch, Brown and Thornicroft2015; Schnyder et al., Reference Schnyder, Panczak, Groth and Schultze-Lutter2017). Discrimination also contributes to difficulties finding or retaining employment, seeking education opportunities, and securing stable housing (Reavley et al., Reference Reavley, Jorm and Morgan2017, Reference Reavley, Ross, McNaught, Green and Morgan2026; Thornicroft et al., Reference Thornicroft, Sunkel, Alikhon Aliev, Baker, Brohan, El Chammay, Davies, Demissie, Duncan, Fekadu, Gronholm, Guerrero, Gurung, Habtamu, Hanlon, Heim, Henderson, Hijazi, Hoffman, Hosny, Huang, Kline, Kohrt, Lempp, Li, London, Ma, Mak, Makhmud, Maulik, Milenova, Morales Cano, Ouali, Parry, Rangaswamy, Rüsch, Sabri, Sartorius, Schulze, Stuart, Taylor Salisbury, Vera San Juan, Votruba and Winkler2022). In response, a range of evidence-based strategies have been implemented internationally, including social contact interventions, legislative reform, and initiatives targeting media representations of people with mental health conditions (Thornicroft et al., Reference Thornicroft, Sunkel, Alikhon Aliev, Baker, Brohan, El Chammay, Davies, Demissie, Duncan, Fekadu, Gronholm, Guerrero, Gurung, Habtamu, Hanlon, Heim, Henderson, Hijazi, Hoffman, Hosny, Huang, Kline, Kohrt, Lempp, Li, London, Ma, Mak, Makhmud, Maulik, Milenova, Morales Cano, Ouali, Parry, Rangaswamy, Rüsch, Sabri, Sartorius, Schulze, Stuart, Taylor Salisbury, Vera San Juan, Votruba and Winkler2022; World Health Organization, 2024). Despite these efforts, it remains unclear whether population-level attitudes towards people with mental health conditions are improving over time. Monitoring change in stigma is essential to evaluate the impact of stigma reduction initiatives and to identify priority areas for further action. Population-based surveys that randomly sample members of the public provide the most robust method for assessing community attitudes (Carina and Michael Reference Carina and Michael2018).
Several countries have examined change in stigmatising attitudes using large, representative samples and vignettes describing a person with depression or schizophrenia (Angermeyer et al., Reference Angermeyer, Grausgruber, Hackl, Moosbrugger and Prandner2021; Pescosolido et al., Reference Pescosolido, Halpern-Manners, Luo and Perry2021; Schomerus et al., Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022). These population-based studies have focused on unwillingness to interact with people with mental health conditions, known as desire for social distance, and perceptions of dangerousness or fearful reactions. Collectively they paint a mixed picture. In the USA, reductions in desire for social distance towards depression were observed between 2006 and 2018, whereas social distance towards schizophrenia and perceptions of dangerousness showed little change over this period (Pescosolido et al., Reference Pescosolido, Halpern-Manners, Luo and Perry2021). In Germany, surveys conducted in 2011 and 2020 showed little change in desire for social distance for either schizophrenia or depression (set against increases for schizophrenia that occurred between 1990 and 2001) (Schomerus et al., Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022). Furthermore, no changes in emotional reactions, such as fear and uneasiness, were observed for either vignette. In contrast, surveys conducted in Austria in 1998 and 2018 showed reduced desire for social distance towards schizophrenia but an increase in perceived dangerousness over time (Angermeyer et al., Reference Angermeyer, Grausgruber, Hackl, Moosbrugger and Prandner2021). These inconsistent findings suggest that trends in stigma may be context-specific and cannot be assumed to generalise across countries.
In Australia, changes in stigmatising attitudes were examined between 2003 and 2011 with two large representative surveys using the same vignettes and outcome measures (Reavley and Jorm, Reference Reavley and Jorm2012). There were mixed findings for changes in attitudes towards people with depression and early schizophrenia. Similar to the findings from Austria, there were some reductions in desire for social distance for schizophrenia and depression, but increases in beliefs about dangerousness and unpredictability in people with these conditions. In addition, there were reductions in beliefs that schizophrenia was a sign of personal weakness and not a real medical illness. Another large survey of Australian adults conducted in 2021 observed higher desire for social distance for depression and schizophrenia than the 2011 survey (Behavioural Economics Team of the Australian Government [BETA], 2022). However, differences in vignette wording and the inability to statistically control for changes in population demographics limited comparability across survey years.
Reducing stigma and discrimination remains a priority in Australian mental health policy. The draft national stigma and discrimination reduction strategy advocates for regular population monitoring of stigmatising attitudes (National Mental Health Commission, 2023). However, there has been no recent examination of change in stigma using directly comparable methodology to the 2011 survey. The present study addresses this gap by analysing data from the 2024-2025 National Survey of Stigma and Discrimination, which surveyed a large representative sample of Australian adults using the same vignettes and outcome measures as the 2011 survey. We aimed to examine change over the preceding 13-year period in stigmatising attitudes and willingness to interact, adjusting for participant demographics between survey years. Given the mixed findings internationally, we did not have specific hypotheses about how stigma may have changed over time in the population.
Methods
2011 sample
The 2011 survey methods have been previously described (Reavley and Jorm, Reference Reavley and Jorm2011). The Social Research Centre in Melbourne, Victoria, recruited participants by random-digit dialling of both landlines and mobile phones. Data were collected using computer-assisted telephone interviews with 6019 Australians aged 15 or older. Interviews were conducted between January and May 2011, and the response rate was 44.0%. The study received ethics approval from the Centre for Youth Mental Health Human Ethics Advisory Group (#1035140).
2024 sample
The 2024 survey was collected as part of the 2024-2025 National Survey of Stigma and Discrimination (Reavley et al., Reference Reavley, Ross, McNaught, Green and Morgan2026). The Social Research Centre again recruited participants, this time using their ‘Life in Australia’ probability-based online panel (Kaczmirek et al., Reference Kaczmirek, Phillips, Pennay and Neiger2019). Members are recruited to the panel via random digit dialling or address-based sampling, allowing for known probability of selection and more accurate and less variable results than non-probability samples or opt-in online panels. The Life in Australia panel was chosen in preference to a sample collected via random-digit dialling because this is increasingly cost-prohibitive, given the very low response rates obtained when contacting Australians by phone. A stratified random sample was drawn from Life in Australia panellists on strata defined by age, gender, highest level of education and speaking a language other than English at home. Data were collected over a 2-week period in November and December 2024. Surveys were completed by 6032 Australian adults and the response rate was 63.7%. The study received ethics approval from the University of Melbourne Human Research Ethics Committee (#29098).
Measures
Each study collected several measures related to stigma, experiences of discrimination, and mental health literacy. The measures that were shared in each study are described below.
Vignette
Both studies used two vignettes describing a person with depression or early schizophrenia. Other vignettes were also included at each timepoint but were not the same so have not been included here. The depression and early schizophrenia vignettes describe a person early in the onset of the condition who has not yet sought treatment and are shown in Table 1. The vignette gender was matched to that of the participant and was described as John or Jenny in 2011 and Sam in 2024. Participants were randomly assigned to one vignette.
Vignettes

a Male version shown. Vignette gender (pronouns) was matched to participant gender.
Personal stigmatising attitudes
Stigmatising attitudes were assessed with the Personal Stigma Scale (Griffiths et al., Reference Griffiths, Christensen, Jorm, Evans and Groves2004), which includes nine items answered in response to the person described in the vignette. The items are: (1) People with a problem like Sam’s could snap out of it if they wanted; (2) A problem like Sam’s is a sign of personal weakness; (3) Sam’s problem is not a real medical illness; (4) People with a problem like Sam’s are dangerous; (5) It is best to avoid people with a problem like Sam’s so that you don’t develop this problem; (6) People with a problem like Sam’s are unpredictable; (7) If I had a problem like Sam’s I would not tell anyone; (8) I would not employ someone if I knew they had a problem like Sam’s; (9) I would not vote for a politician if I knew they had suffered a problem like Sam’s. Responses are made on a 5-point Likert scale: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree. To analyse change over time, responses were dichotomised into agree or strongly agree (4 or 5) versus strongly disagree, disagree, or neither agree nor disagree (1 to 3).
Social distance
The Social Distance Scale (Link et al., Reference Link, Phelan, Bresnahan, Stueve and Pescosolido1999) was used to assess willingness to interact with the person described in the vignette. The scale includes five items assessing willingness to (1) move next door to Sam; (2) spend an evening socialising with Sam; (3) make friends with Sam; (4) work closely with Sam on a job; (5) have Sam marry into their family. Each item was rated on a 4-point scale: 1 = Definitely willing, 2 = Probably willing, 3 = Probably unwilling, 4 = Definitely unwilling. To analyse change over time, responses were dichotomised into probably or definitely unwilling (3 or 4) versus probably or definitely willing (1 or 2).
Sociodemographics
The following sociodemographic information was collected in both surveys: age (18–34, 35–64, 65+), gender (male, female, non-binary/other), country of birth (Australia or English-speaking country, non-English speaking country), highest level of education completed (Bachelor degree or above, below bachelor level), language spoken at home (English only, language other than English). The sociodemographic characteristics of the samples at each time point are provided in Supplementary Table 1.
Statistical analysis
As the 2011 survey included participants aged 15–17, these were dropped from the analyses for comparability with the 2024 sample. This left 1967 in the 2011 sample (993 depression vignette; 974 early schizophrenia vignette) and 1984 in the 2024 sample (1008 depression vignette; 976 early schizophrenia vignette). Data per time point were presented with per cent frequencies and 99% confidence intervals, using sample weights to adjust for the probability of being selected and to satisfy population benchmarks for key sociodemographic characteristics.
To examine change over time, weighted logistic regression models were used with survey year as the predictor. These models controlled for sociodemographic variables (age, gender, level of education, country of birth and language spoken at home) as population levels of these variables may have changed between survey years. Given the large sample sizes and number of analyses, results were considered significant at p < .01. All analyses were performed using Stata SE 18.
Results
Weighted responses to the personal stigmatising attitudes questions in 2011 and 2024 are given in Table 2. As shown in the column combining agree or strongly agree responses, there was a general shift towards less agreement with most stigmatising attitudes for both depression and early schizophrenia. Notably, however, increases were often in those neither agreeing or disagreeing rather than in those disagreeing or strongly disagreeing. Four attitudes were endorsed by less than 10% of the sample in 2024 for both conditions: that people could snap out of the problem if they wanted, the problem is a sign of personal weakness, the problem is not a real medical illness, and it is best to avoid people so that you don’t develop this problem. Attitudes about unpredictability had the highest agreement across both vignettes.
Personal stigmatising attitudes in 2011 and 2024
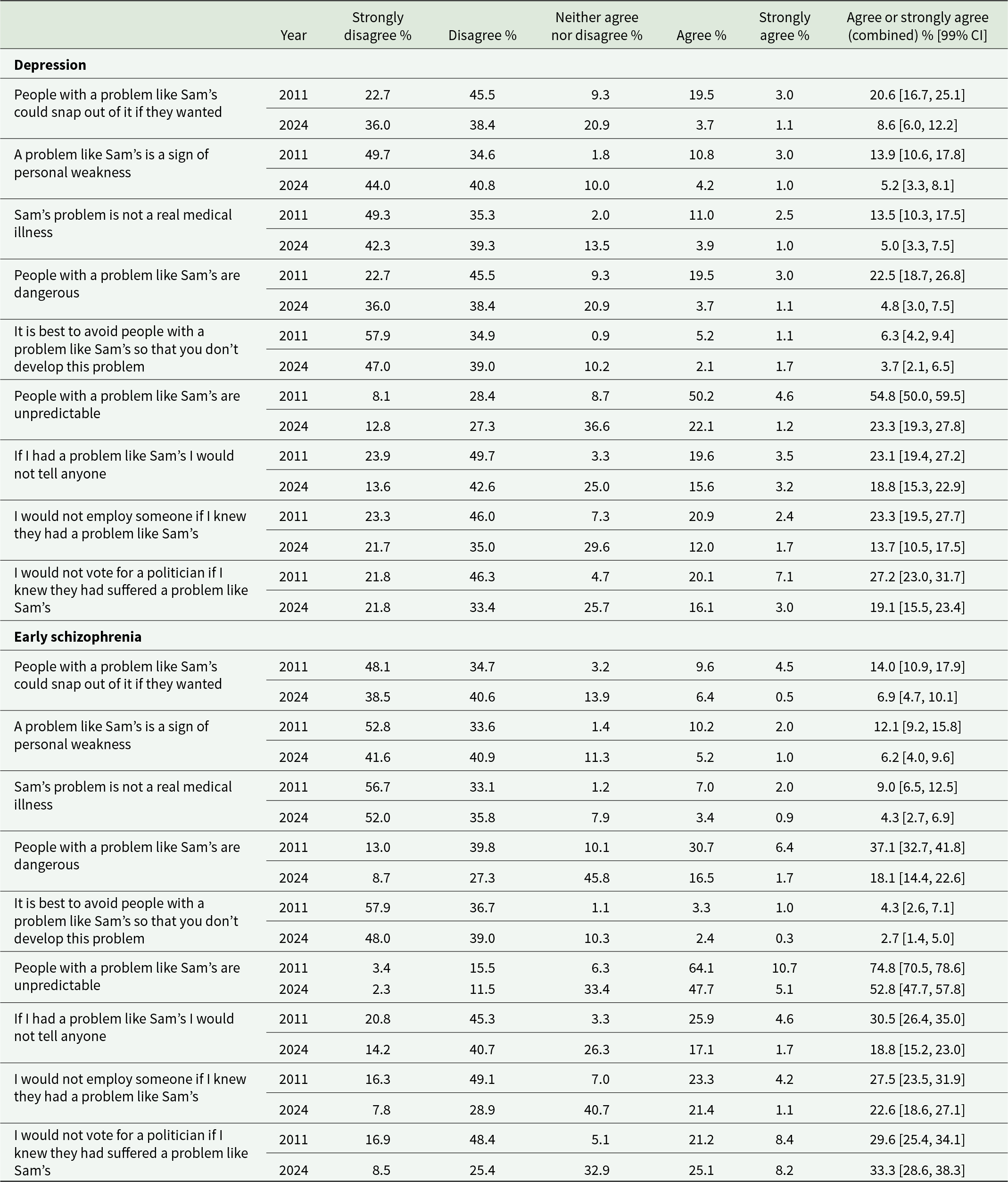
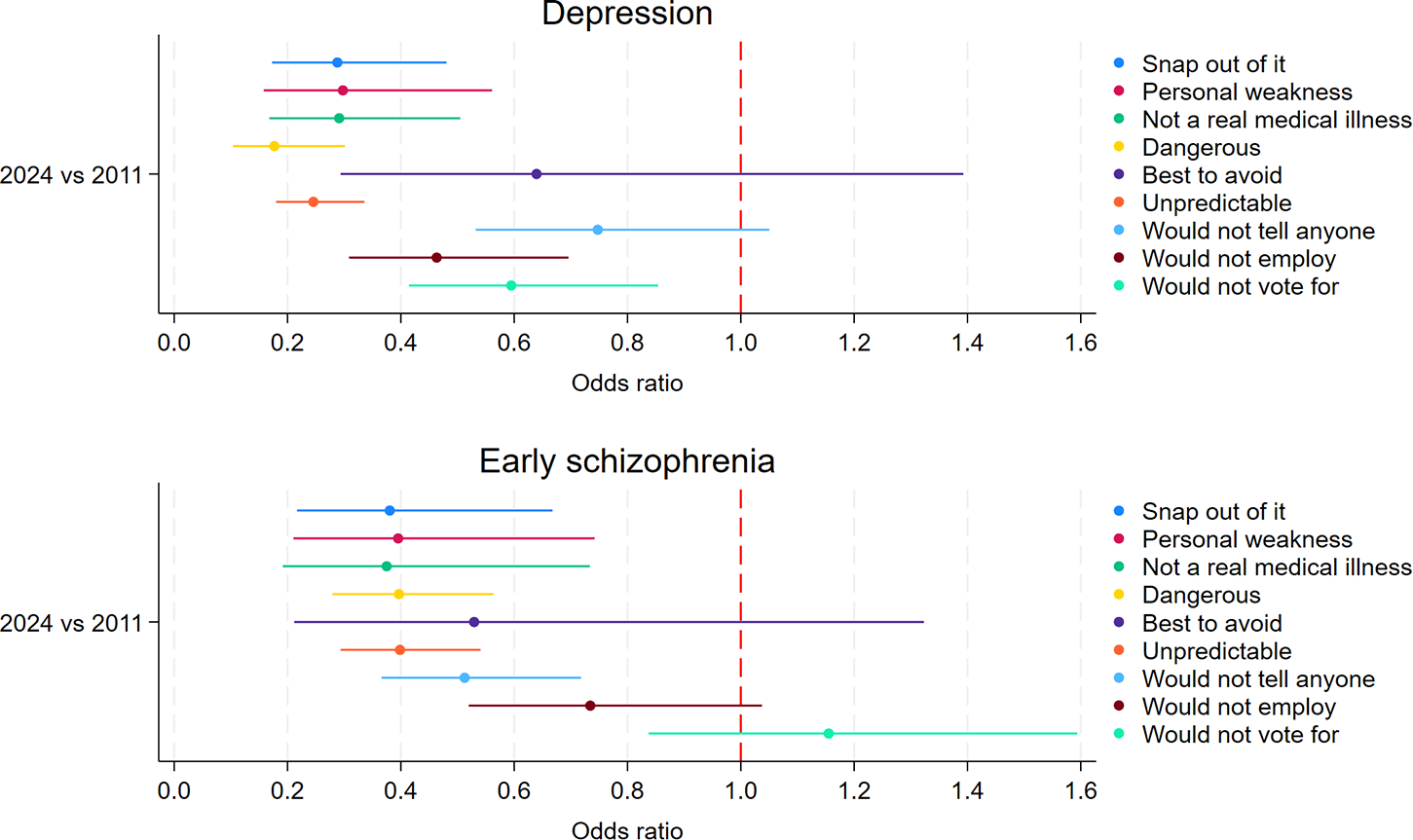
Figure 1 shows the change in agreement with each stigmatising attitude from 2011 to 2024, controlling for age, gender, education level, country of birth, and language spoken at home. For depression, there was a statistically significant reduction in 2024 in the odds of agreeing with all stigmatising attitudes except for ‘It is best to avoid people with a problem like Sam’s so that you don’t develop this problem’ (which had low endorsement in 2011) and ‘If I had a problem like Sam’s I would not tell anyone’. Findings were similar for schizophrenia, with significant reductions in agreement with six of the nine stigmatising attitudes and no significant increases.
Agreement with stigmatising attitudes in 2024 versus 2011, controlling for sociodemographics, with 99% confidence intervals.

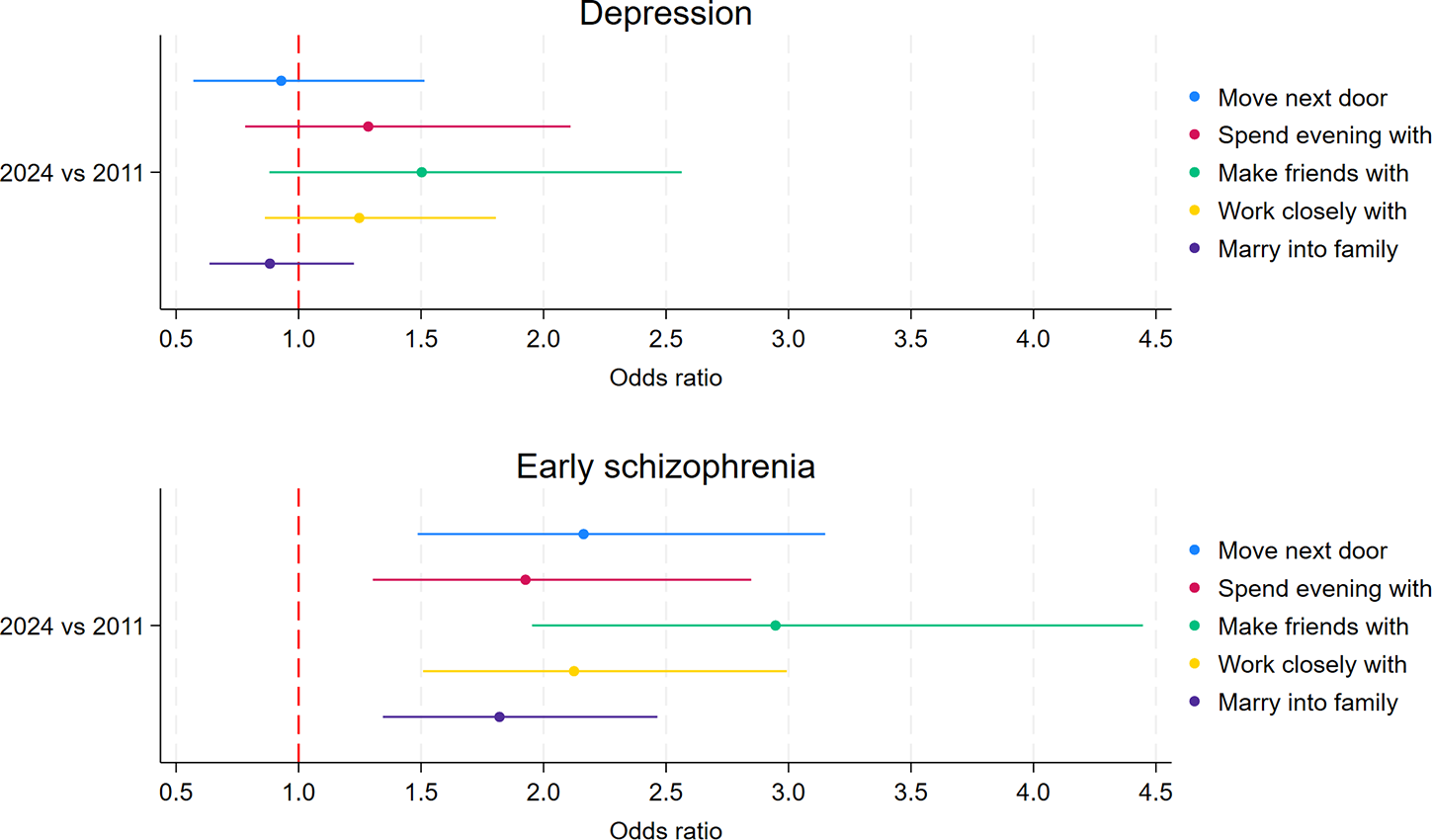
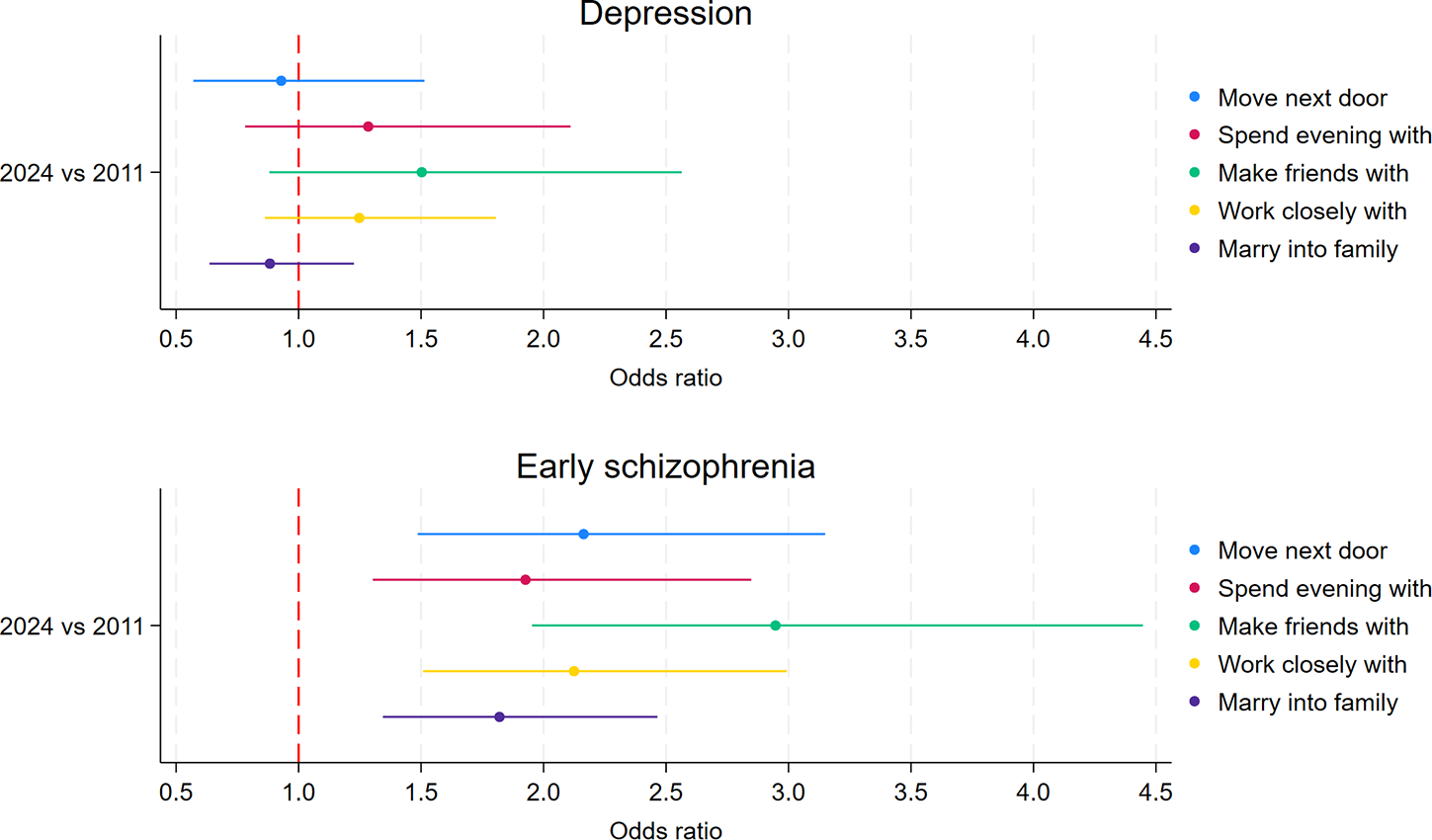
Table 3 presents the weighted responses to items on the Social Distance Scale, describing willingness to interact with the person in the vignette. For depression, the proportion of the sample who were probably or definitely unwilling showed little differences between 2011 and 2024, with the greatest unwillingness for the person marrying into the family. Logistic regression models (shown in Fig. 2) confirmed that there were no significant reductions in unwillingness to interact over time. In contrast, for schizophrenia, desire for social distance had increased significantly over time, with approximately double the odds of being unwilling to interact in each situation in 2024 compared to 2011. Supplementary analyses tested the interaction between survey year and vignette to explore whether the change over time was significantly greater for schizophrenia compared to depression. These analyses were statistically significant (p < .01) for unwillingness to move next door (p = .002) and marry into the family (p < .001) but not for spend an evening with (p = .081), make friends with (p = .033) or work closely with (p = .015).
Unwillingness to interact in 2024 versus 2011, controlling for sociodemographics, with 99% confidence intervals.
Social distance in 2011 and 2024

Discussion
This study aimed to examine changes in stigmatising attitudes towards adults with depression or schizophrenia in the Australian population between 2011 and 2024. Overall, findings present a mixed picture. There were significant reductions in most stigmatising attitudes towards people with depression or schizophrenia, but no change in willingness to interact with a person with depression, and an increase in unwillingness to interact with a person with schizophrenia.
The size of the reduction in stigmatising attitudes is notable, particularly for beliefs about dangerousness and unpredictability, which had increased between 2003 and 2011 (Reavley and Jorm, Reference Reavley and Jorm2012). This is in contrast to other countries, where beliefs about dangerousness have not changed in recent years (Pescosolido et al., Reference Pescosolido, Halpern-Manners, Luo and Perry2021; Schomerus et al., Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022) or have increased over time (Angermeyer et al., Reference Angermeyer, Grausgruber, Hackl, Moosbrugger and Prandner2021). There may be many reasons for this change, but one potential influence could be improved media reporting of violent incidents involving a person with mental illness. Australia has a robust system of supports to improve media reporting of mental illness, including specific guidance on reporting of complex mental illness in the context of violence and crime and active connection of lived experience stories with media (Ross et al., Reference Ross, Morgan, Wake, Jorm and Reavley2020, Reference Ross, Morgan and Reavley2024; Everymind, 2022). Australia also has a range of anti-stigma initiatives that may have played a role, including education/contact interventions and awareness campaigns, though few have been rigorously evaluated to understand their effectiveness (Morgan et al., Reference Morgan, Wright and Reavley2021). Nevertheless, although beliefs about dangerousness are now only endorsed by a minority, unpredictability is still endorsed by a sizeable proportion of the population, particularly for schizophrenia. Endorsement of beliefs that a person with depression or schizophrenia is weak rather than sick have continued their downward trend and the vast majority of Australians no longer share these beliefs. This mirrors findings observed in other countries where causal beliefs about weakness or bad character are uncommon (Pescosolido et al., Reference Pescosolido, Medina, Martin and Long2013). Future assessment of stigma should consider shifting away from beliefs about personal weakness towards other stigmatising attitudes that are important, such as beliefs about competency or being able to recover and live a meaningful life.
Despite these positive changes, it is surprising and troubling to observe the lack of change or even deterioration in willingness to interact with a person with depression or schizophrenia. The previous evaluation of change from 2003 to 2011 observed decreases in desire for social distance (Reavley and Jorm, Reference Reavley and Jorm2012). The increase in unwillingness since 2011 is sizeable for schizophrenia and the proportions unwilling in 2024 are even higher than those in 2003 (e.g. 12.0% were unwilling to make friends in 2003 versus 26.9% in 2024). This increase contrasts with the lack of change or decrease in desire for social distance observed in population studies in other countries over similar time periods (Angermeyer et al., Reference Angermeyer, Grausgruber, Hackl, Moosbrugger and Prandner2021; Pescosolido et al., Reference Pescosolido, Halpern-Manners, Luo and Perry2021; Schomerus et al., Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022). However, the increase does align with higher rates of discrimination related to mental health reported in 2024 compared with 2014 in Australia (Reavley et al., Reference Reavley, Ross, McNaught, Green and Morgan2026). Despite this, the different survey administration mode is a possible explanation for the differences, which was face-to-face in 2003, telephone in 2011 and online survey in 2024. Surveys containing sensitive questions may have less social desirability bias when self-administered rather than in response to an interviewer (Tourangeau and Yan, Reference Tourangeau and Yan2007). Accordingly, participants may have been more willing to admit stigmatising responses to the 2024 online survey, although this does not explain why we also observed a decrease in stigmatising responses to the Personal Stigma Scale. Nor does it explain the increase in desire for social distance for schizophrenia relative to depression, which suggests the change represents a true time trend and is not an artefact of survey mode, given the same survey methodology was used for both conditions at each timepoint.
The divergence of temporal trends on each measure of stigma warrants discussion. Stigma is conceptualised as comprising cognitive, affective, and behavioural components that are interconnected (Corrigan and Watson, Reference Corrigan and Watson2002). For instance, believing the stereotype that people with schizophrenia are dangerous may lead to a fear response and a desire to avoid them. This is why anti-stigma efforts focus on correcting misconceptions to reduce discriminatory behaviours through both education and contact with people with mental health conditions. Logically then, reductions in stigmatising beliefs would be expected to correspond to reductions in discrimination, operationalised here as unwillingness to interact. Angermeyer et al. (Reference Angermeyer, Grausgruber, Hackl, Moosbrugger and Prandner2021) in their recent population survey in Austria also observed this diverging trend and suggested that there must be other factors that are driving the desire for social distance. Our study found personal stigmatising attitudes and desire for social distance were correlated (rs .40 to .66), but there may be other unmeasured variables that correlate with willingness to interact with a person with depression or schizophrenia. Schomerus et al. (Reference Schomerus, Kummetat, Angermeyer and Link2024) have shown that there is a strong relationship between desire for social distance and beliefs about the relatability of people with mental health conditions and whether there is continuity between ‘us’ and ‘them’, particularly for schizophrenia. They propose that promoting messages that simultaneously focus on relatability and the continuum between ‘us’ and ‘them’ would have stigma reduction effects. Nevertheless, there is a need for careful development and testing of intervention messaging to avoid inadvertently widening the gap in stigmatising attitudes towards people with depression and schizophrenia (Reavley, Reference Reavley2026). Qualitative research exploring reasons behind unwillingness to interact would be helpful to understand the presence of other stigmatising beliefs or contributing factors, such as the belief it would be emotionally taxing or burdensome.
Another factor to consider may be the different response options of the two scales – one allowing for a neutral ‘neither’ response (Personal Stigma Scale) and one with four options without a neutral midpoint (Social Distance Scale). Link’s adapted Social Distance Scale (1999) forces respondents to choose a stigmatising or non-stigmatising response and is an approach thought to reduce social desirability bias in sensitive topics. As shown in the results, there appeared to be an increase in the proportion of ‘neither’ responses to the Personal Stigma Scale, sometimes at the expense of ‘disagree’ or ‘strongly disagree’ (e.g. dangerous beliefs in the schizophrenia vignette). This may reflect a more nuanced understanding of mental health conditions, where participants may understand that their attitudes depend upon the particular individual and set of circumstances, rather than relying on stereotypes that apply equally regardless of the situation. Participants deprived of a neutral ‘it depends’ option may have selected the unwilling response options for the Social Distance Scale. If so, this would suggest it may be preferable to add a neutral response option to the Social Distance Scale to reduce measurement error.
As has been noted by others, vignettes are imperfect tools to measure stigmatising attitudes but have advantages over using a diagnostic label (Link et al., Reference Link, Yang, Phelan and Collins2004). To enable comparison over time, our vignettes remained the same as those used in Australian surveys of mental health literacy begun in the 1990s (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997). Those surveys sought to understand the role of mental health literacy in stigma and intended help-seeking, and therefore the vignettes described a person with symptoms before they had sought any treatment. It is important to note that attitudes may be different towards vignettes that describe a person living well in the community who had undergone treatment for depression or schizophrenia in the past (McGinty et al., Reference McGinty, Goldman, Pescosolido and Barry2015). Furthermore, while monitoring stigmatising attitudes over time can provide insight into structural stigma (which reflects prevailing societal norms), it is critical to measure experiences of discrimination to fully understand stigma’s impact on the lives of people with mental health conditions (Reavley et al., Reference Reavley, Ross, McNaught, Green and Morgan2026).
This study has several strengths, including two large, nationally representative samples of Australian adults. Vignettes and survey measures were consistent between time periods, allowing for accurate comparison over time. Analyses also controlled for change in population demographics, which are known to be associated with stigmatising attitudes (Yap et al., Reference Yap, Mackinnon, Reavley and Jorm2014). As noted above, limitations to consider include the different survey administration mode and the use of vignettes, which may not accurately reflect attitudes to real-life situations.
In conclusion, the data show mixed findings regarding change in stigma in the Australian population. Despite many stigmatising beliefs diminishing over time, this has not translated into greater willingness to interact with people with depression or schizophrenia. Key action is needed on understanding the barriers to interacting with people with mental health conditions and reducing perceptions of unpredictability, particularly for schizophrenia, which remains more highly stigmatised.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100602.
Availability of data and materials
Data are available on reasonable request.
Acknowledgements
We would like to thank SANE’s Lived Experience Advisory Committee for providing input into the survey questions.
Author contributions
NR and AM led the survey design. AM conducted the statistical analysis and wrote the first draft of the manuscript. All authors contributed to the research design, drafting of the manuscript, and approved the final manuscript.
Financial support
The 2024-2025 National Survey of Stigma and Discrimination was funded by SANE Australia. AR receives funding from NHMRC (Investigator Grant #2025181), AM from Mental Health First Aid International and Veski and NR from SANE.
Competing interests
Rachel Green and Gayle McNaught are employees of SANE, Australia. Anna Ross and Nicola Reavley receive some salary support from SANE, Australia.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000.





 Open access
Open access