

Introduction
Coronavirus disease 2019 (COVID-19) quickly emerged in late 2019 and was quickly designated a global pandemic (Chen et al., Reference Chen, Zhou, Dong, Qu, Gong, Han, Qiu, Wang, Liu, Wei, Xia, Yu, Zhang and Zhang2020; Stein et al., Reference Stein, Ramelli, Grazioli, Chung, Singh, Yinda, Winkler, Sun, Dickey, Ylaya, Ko, Platt, Burbelo, Quezado, Pittaluga, Purcell, Munster, Belinky, Ramos-Benitez, Boritz, Lach, Herr, Rabin, Saharia, Madathil, Tabatabai, Soherwardi, McCurdy, Peterson, Cohen, de Wit, Vannella, Hewitt, Kleiner and Chertow2022). As an acute global emergency, COVID-19 is very contagious (Tan et al., Reference Tan, Kwan, Rodríguez-Barraquer, Singer, Park, Lewnard, Sears and Lo2023) and leads to multisystem symptoms, which can even be life threatening for some patients (Parotto et al., Reference Parotto, Gyöngyösi, Howe, Myatra, Ranzani, Shankar-Hari and Herridge2023; Wiersinga et al., Reference Wiersinga, Rhodes, Cheng, Peacock and Prescott2020), with more than 770 million cases globally over the past 3 years (Marks and Gulick, Reference Marks and Gulick2023; World Health Organization, 2023). The latest Global Burden of Disease Study 2021 estimates that COVID-19 is the leading cause of disability-adjusted life-years globally (GBD 2021 Diseases and Injuries Collaborators, 2024), with 15.9 million excess deaths from 2020 to 2021(GBD 2021 Demographics Collaborators, 2024). In May 2023, the World Health Organization (WHO) announced that COVID-19 ‘no longer constitutes a public health emergency of international concern’, considering that it has not been an unusual or unexpected event (Harris, Reference Harris2023). However, COVID-19 has been and will continue evolving to influence global health through long symptoms, new mutations, and frequent recurrence, which necessitates the attention of global health (El-Shabasy et al., Reference El-Shabasy, Nayel, Taher, Abdelmonem, Shoueir and Kenawy2022; Yisimayi et al., Reference Yisimayi, Song, Wang, Jian, Yu, Chen, Xu, Yang, Niu, Xiao, Wang, Zhao, Sun, An, Zhang, Wang, Wang, Yu, Lv, Gu, Shao, Jin, Shen, Xie, Wang and Cao2024).
During the COVID-19 pandemic, multiple stress factors, such as worries about exposure and infection, social isolation and physical inactivity, and unavailable psychosocial support, could exacerbate psychological distress (Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021) and impact mental health, such as anxiety, depression, sleep problems, post-traumatic stress disorder (PTSD) and other symptoms (Alimoradi et al., Reference Alimoradi, Broström, Tsang, Griffiths, Haghayegh, Ohayon, Lin and Pakpour2021; Cénat et al., Reference Cénat, Blais-Rochette, Kokou-Kpolou, Noorishad, Mukunzi, McIntee, Dalexis, Goulet and Labelle2021; Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022). This implication has been of global concern, as growing evidence has revealed an increased mental health burden (COVID-19 Mental Disorders Collaborators, 2021; Kola et al., Reference Kola, Kohrt, Hanlon, Naslund, Sikander, Balaji, Benjet, Cheung, Eaton, Gonsalves, Hailemariam, Luitel, Machado, Misganaw, Omigbodun, Roberts, Salisbury, Shidhaye, Sunkel, Ugo, van Rensburg, Gureje, Pathare, Saxena, Thornicroft and Patel2021; Prime et al., Reference Prime, Wade and Browne2020). However, major gaps and concerns remain regarding the shifts in mental health impacts and associated factors during different pandemic periods, and limited information is available on post-acute mental health symptoms (Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022; Pirkis et al., Reference Pirkis, John, Shin, DelPozo-Banos, Arya, Analuisa-Aguilar, Appleby, Arensman, Bantjes, Baran, Bertolote, Borges, Brečić, Caine, Castelpietra, Chang, Colchester, Crompton, Curkovic, Deisenhammer, Du, Dwyer, Erlangsen, Faust, Fortune, Garrett, George, Gerstner, Gilissen, Gould, Hawton, Kanter, Kapur, Khan, Kirtley, Knipe, Kolves, Leske, Marahatta, Mittendorfer-Rutz, Neznanov, Niederkrotenthaler, Nielsen, Nordentoft, Oberlerchner, O’Connor, Pearson, Phillips, Platt, Plener, Psota, Qin, Radeloff, Rados, Reif, Reif-Leonhard, Rozanov, Schlang, Schneider, Semenova, Sinyor, Townsend, Ueda, Vijayakumar, Webb, Weerasinghe, Zalsman, Gunnell and Spittal2021; Raina et al., Reference Raina, Wolfson, Griffith, Kirkland, McMillan, Basta, Joshi, Oz, Sohel, Maimon and Thompson2021). Additionally, the results from many studies have shown substantial heterogeneity among their study populations and times (Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020; Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022) and have limited methodological quality due to small sample sizes and convenience sampling, as well as unclear representativeness and generalizability(Cénat et al., Reference Cénat, Blais-Rochette, Kokou-Kpolou, Noorishad, Mukunzi, McIntee, Dalexis, Goulet and Labelle2021; Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022). To more reliably estimate shifts in mental health impacts and to identify factors associated with symptoms at different pandemic stages, we conducted this large-sample multicentre study with a repeated cross-sectional design at 3 representative stages (stable, recurrence, and end-of-emergency) in the general Chinese population with our previous experience during the initial COVID-19 wave (Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020) and return-to-work period (Wang et al., Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020). This study can also provide timely references for the post-COVID-19 era and future potential pandemics and recurrence, helping in more appropriately mediating health policies and identifying and protecting individuals at risk and promoting long-term resilience; thus, providing important information for policy makers, practicing clinicians, researchers and other stakeholders (Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022).
Materials and methods
Study design and sampling process
This repeated cross-sectional study was conducted through 3 surveys from 2021 to 2023. The ethics committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University approved this study. All participants provided online or oral informed consent. This study followed the 1964 Helsinki Declaration and its later amendments and reports according to the Statement of Reporting of Observational studies in Epidemiology (STROBE; von Elm et al., Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke2014). The surveys were anonymous, and the confidentiality of the data was ensured.
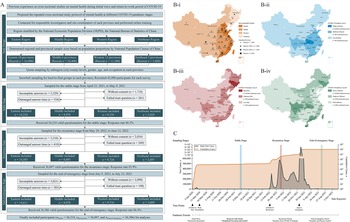
The study procedure is shown in Fig. 1. Based on our previous experience during the COVID-19 epidemic (Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020), we proposed the current study protocol and applied a region-stratified population-based quota combined with a snowball sampling strategy to recruit a representative national sample, which was previously established when random sampling was inappropriate during the epidemic (Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020). First, we contacted the investigators and site coordinators of all 31 provinces of mainland China and performed unified online training. According to the National Economic Population Division (NEPD) of the National Bureau of Statistics (NBS; National Bureau of Statistics of People’s Republic of China, 2011), these provinces were stratified into four socio-geographic regions: eastern, middle, western and northeast. Second, the required sample sizes of each region and affiliated provinces were determined based on the population proportions of the National Population Census (NPC) 2020 (Office of the Leading Group of the State Council for the Seventh National Population Census, 2020). Third, we calculated the required quotas to recruit individuals with representative characteristics by further stratifying the proportions of subregions (at the city/county level), genders, ages and occupations for each sampling province. After that, investigators were required to invite individuals with these specific characteristics. The invitations were sent online, by telephone, via posters or person to person. When an individual agreed for participation and was verified to have required characteristics, he/she was marked as ‘recruited’ and sent with surveys. Snowball sampling was used as a supplement for some hard-to-find groups (e.g., elderly individuals) when necessary, which encouraged participants to introduce others with the required characteristics to the investigators. A nominal payment (lucky draw) was set as a recruitment incentive for all participants. Finally, the same procedure was repeated triply at the stable (25 April 2021 to 9 May 2021), recurrence (29 May 2022 to 12 June 2022) and end-of-emergency (9 July 2023 to 23 July 2023) COVID-19 pandemic stages. Participants could participate in one or more different surveys but were allowed to answer only once for the same survey.
Flow diagram showing the study procedure (A), sketch map showing the region divisions (B), and timeline showing the COVID-19 stages (C). COVID-19, coronavirus disease 2019; NEPD, National Economic Population Division. Region division was classified based on socio-geographical characteristics or the influence of COVID-19 on regional features and infection risk at different pandemic stages, refers to Supplementary Table 1 for detailed regional division for provinces; socio-geographic region was stratified based on NEPD, the National Bureau of Statistics for the normal period; COVID-19 pandemic area I was stratified according to cumulative confirmed cases between January 2020 and March 2020 (initial wave, 2020) and data from the National Health Commission, China; COVID-19 pandemic area II was stratified according to cumulative confirmed cases between March 2022 and May 2022 (recurrence, 2022) and data from the National Health Commission, China; and COVID-19 pandemic area III was stratified according to cumulative confirmed cases between January 2020 and December 2022 (end-of-emergency, 2023).
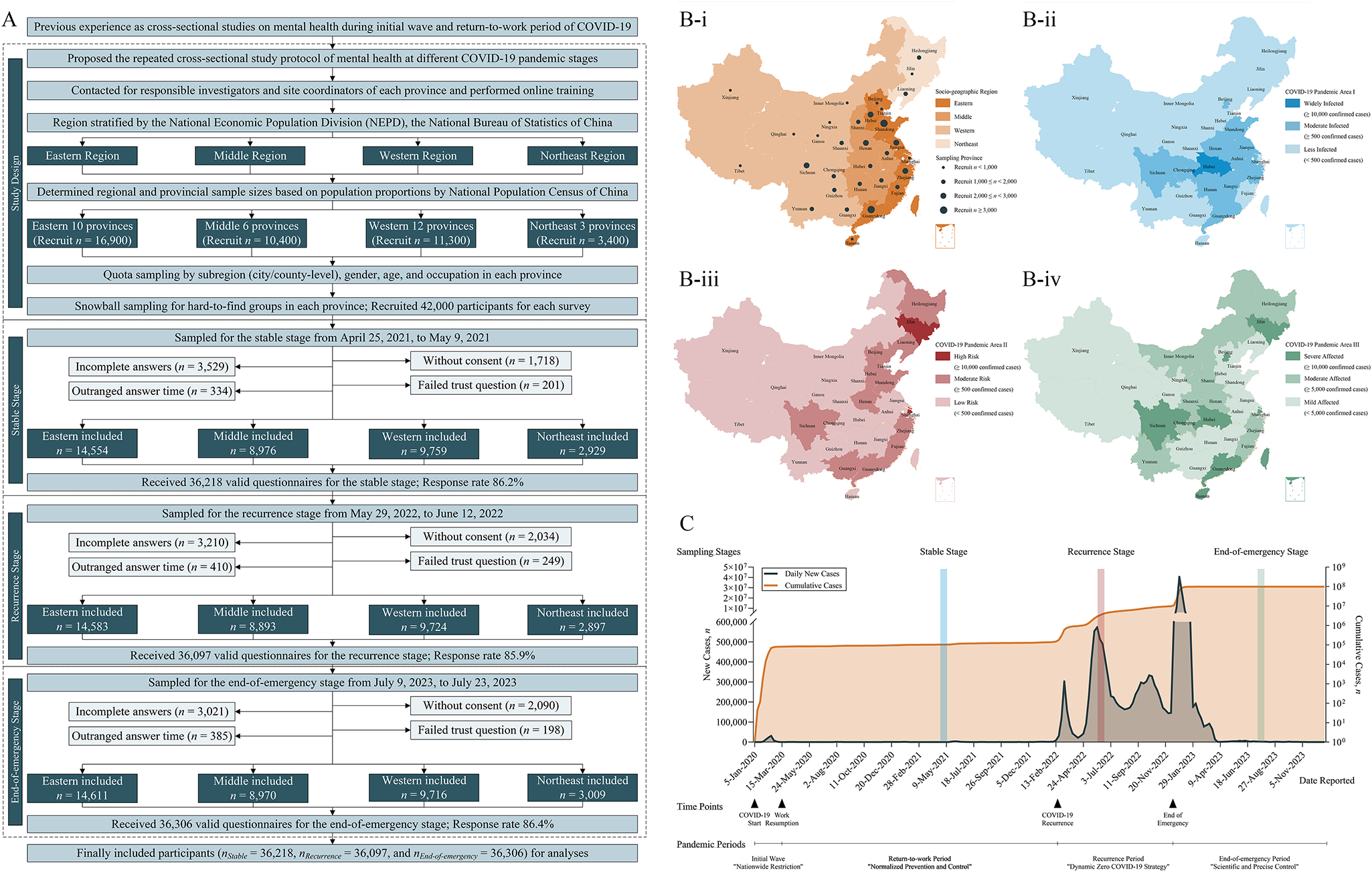
Pandemic periods classification, key time points and health policies were collected from epidemic reports by the National Health Commission of China (NHC; www.nhc.gov.cn). Specifically, from late 2019 to March 2020, China experienced initial epidemic wave and applied ‘nationwide restriction’ policy. This initial wave was basically controlled from February 2020 and the ‘normalized prevention and control’ during this stable stage. However, the epidemic recurrent from March 2022, during which the ‘dynamic zero’ policy were applied. In December 2022, the Chinese government declared the end of the emergency of the COVID-19 epidemic and announced the ‘scientific and precise control’ (Fig. 1).
Additionally, the NHC database and the WHO dashboard (World Health Organization, 2023) were queried to stratify the infection risks of these provinces during different pandemic periods in exploring its potential influences on mental health at different pandemic stages. Pandemic area I (initial wave) was stratified according to cumulative confirmed cases between January 2020 and March 2020 in capturing regional characteristics of the initial waves; pandemic area II (recurrence) was stratified according to cumulative confirmed cases between March 2022 and May 2022 to classified risks of the first COVID-19 recurrence waves; and pandemic area III (end-of-emergency, summary of the pandemic) was stratified according to cumulative confirmed cases between January 2020 and December 2022 in summarizing the entire pandemic situation until the end of emergency. The detailed regional divisions are shown in Supplementary Table 1.
Study population
This study assessed the mental health of the general population. Considering ethical issues and measurement scales, only adults (≥18 years) were included. The target sample size for recruitment was calculated in PASS software version 2021 (NCSS LLC) for multiple (3) comparisons of proportions (Chow et al., Reference Chow, Shao and Wang2008), in which the statistical power was set to 90.0% and the overall α = 0.05 (Bonferroni adjusted α = 0.0167). Based on previous studies (Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020), the proportion of mental health symptoms was estimated to be 15%, and the acceptable margin of differences was set to 1%. When the dropout rate was set to 20%, the dropout-inflated enrolment sample size was 41,864 for each stage. Considering the convenience of calculating the required quotas, we increased the sample size to 42,000 for each survey stage.
For these participants, 5,782 (1,718 without consent, 3,529 with incomplete answers, 201 with failed trust questions and 334 with outrange answer times), 5,903 (2,034 without consent, 3,210 with incomplete answers, 249 with failed trust questions and 410 with outrange answer times) and 5,694 (2,090 without consent, 3,021 with incomplete answers, 198 with failed trust questions and 385 with outrange answer times) invalid questionnaires were excluded for the stable, recurrence, and end-of-emergency stages, respectively. The events per variable (EPV) for the final eligible participants also met the requirements for logistic regression (all EPVs ≥ 10) (Chow et al., Reference Chow, Shao and Wang2008) in identifying factors associated with symptoms (Table 1).
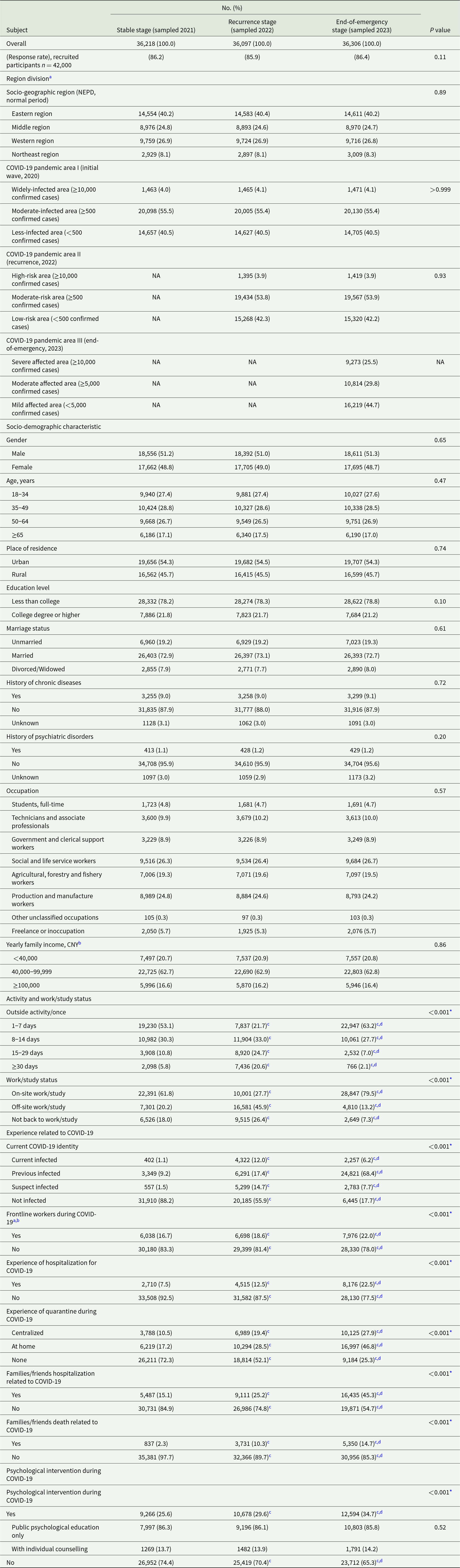
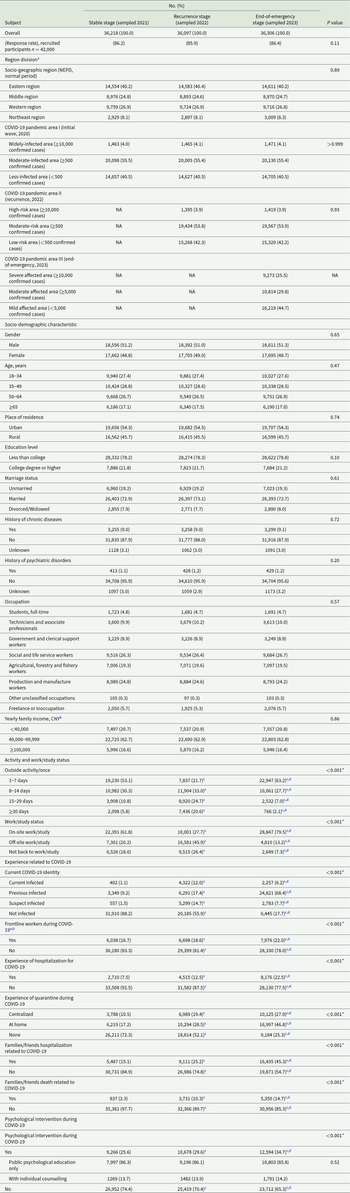
Socio-demographic characteristics, activity and work/study status, relevant experiences, and psychological interventions of all included participants at different COVID-19 pandemic stages (n Stable = 36,218, n Recurrence = 36,097 and n End-of-emergency = 36,306)
COVID-19, coronavirus disease 2019; NEPD, National Economic Population Division, by the National Bureau of Statistics, China; NA, not applicable.
a Region division was classified based on different socio-geographical characteristics or COVID-19 influences in reflecting regional features and infection risks at different pandemic stages, refers to eTable 1 for detailed region division for provinces; Socio-geographic region was stratified based on NEPD, the National Bureau of Statistics, China, for normal period; COVID-19 pandemic area I was stratified according to cumulative confirmed cases between January 2020 to March 2020 (initial wave, 2020), data from the National Health Commission, China; COVID-19 pandemic area II was stratified according to cumulative confirmed cases between March 2022 to May 2022 (recurrence, 2022), data from the National Health Commission, China; COVID-19 pandemic area III was stratified according to cumulative confirmed cases between January 2020 to December 2022 (end-of-emergency, 2023).
bAs of September 2nd, 2024, 1 CNY = 0.139 USD, the stratification could be regarded as ‘low-income family’, ‘moderate-income family’ and ‘high-income family’ based on standard of the National Bureau of Statistics, China.
a,b,Frontline workers indicate individuals who directly participated in the control of COVID-19, serving with the potential for direct or indirect exposure to COVID-19 patients or infectious materials. *P < 0.01 (Pearson’s χ2 test).
c(Bonferroni) adjusted P < 0.05 comparing with the Stable stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction).
d(Bonferroni) adjusted P < 0.05 comparing with the Recurrence stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction).
Measurements and covariates
The same questionnaire design was applied for the 3 surveys. Participants preferred to answer online via WJX links (Ranxing LLC) with an IP address restriction to prevent repeated answers from the same person in the survey. For those who could not finish the online survey, telephone interviews read by investigators were provided with the same content. Additionally, participants were asked to answer only one type of survey to avoid duplication. A guiding webpage or oral introduction of the informed consent was provided prior to the survey. The participants were informed about their free decision to participate or not participate, provided informed consent or not, and could terminate the survey at any time.
The self-designed survey consisted of 4 sections and required approximately 15 minutes to complete. The first section collected socio-demographic information, including sex, age (division according to previous epidemiological studies [Huang et al., Reference Huang, Wang, Wang, Liu, Yu, Yan, Yu, Kou, Xu, Lu, Wang, He, Xu, He, Li, Guo, Tian, Xu, Xu, Ma, Wang, Wang, Yan, Wang, Xiao, Zhou, Li, Tan, Zhang, Ma, Li, Ding, Geng, Jia, Shi, Wang, Zhang, Du, Du and Wu2019; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020] for comparisons), place of residence (urban vs rural), education level, marital status, history of chronic disease and psychiatric disorders, occupation (classified by the NPC 2020), and yearly family income. The second section asked pandemic-related questions about current activity (outside activity frequency) and work/study status (on-site, off-site or not), experience related to COVID-19 (current identity, frontline workers or not, experience of hospitalization and quarantine, and hospitalization and death of family/friends), and psychological interventions during COVID-19 (with or without; and public psychological education only, i.e., provided by governments, societies, communities and others, which was delivered once or scattered times without specialized guiding, or with individual counselling, i.e., provided by professional psychologists with systematic terms and individualized treatments).
The third section included 4 standardized screening scales, including the Generalized Anxiety Disorder-7 scale (GAD-7, scores from 0-21, Cronbach’s α coefficient = 0.93)(Zhang et al., Reference Zhang, Wang, Zeng, Zhao, Zhang, Zhai, Meng, Wang and Liu2021), Patient Health Questionnaire-9 (PHQ-9, scores from 0-27, Cronbach’s α coefficient = 0.90)(Wang et al., Reference Wang, Bian, Zhao, Li, Wang, Du, Zhang, Zhou and Zhao2014; Zhang et al., Reference Zhang, Liang, Chen, Zhang, Zhang, Weng, Yang, Zhang, Shen and Zhang2013), Impact of Events Scale-Revised (IES-R, scores from 0-88, Cronbach’s α coefficient = 0.95)(Creamer et al., Reference Creamer, Bell and Failla2003; Wu and Chan, Reference Wu and Chan2003), and Insomnia Severity Index (ISI, scores from 0-28, Cronbach’s α coefficient = 0.91)(Chung et al., Reference Chung, Kan and Yeung2011; Thorndike et al., Reference Thorndike, Ritterband, Saylor, Magee, Gonder-Frederick and Morin2011), which measured anxiety, depression, PTSD, and insomnia symptoms, respectively. These scales are all validated Chinese versions and have been widely used in previous epidemiological investigations (Chen et al., Reference Chen, Feng, Liu, Wu, Li, Zhang, Yang and Zhang2023; Lai et al., Reference Lai, Ma, Wang, Cai, Hu, Wei, Wu, Du, Chen, Li, Tan, Kang, Yao, Huang, Wang, Wang, Liu and Hu2020; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020). Higher scores on these scales indicate more severe symptoms. In the present study, the cut-off scores for detecting symptoms were ≥10, ≥10, ≥33 and ≥15, and scores ≥15, ≥15, ≥37 and ≥22 indicated severe symptoms for the GAD-7, PHQ-9, IES-R and ISI, respectively. These cut-off values were determined according to Chinese norms and previous studies of the Chinese population (Chen et al., Reference Chen, Feng, Liu, Wu, Li, Zhang, Yang and Zhang2023; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020), which has been widely recognized and further reviewed by a consensus of neuropsychologists.
For the fourth section, two trust test questions were designed: ‘I answered truthfully (yes or no)’ and ‘What is ten plus ten?’ Surveys without consent, with incomplete answers, with a failure of any trust question, or with an outrange of time (i.e., <1 min or >2 hours) were regarded as invalid questionnaires.
Statistical analysis
Categorical variables are reported as numbers and percentages. The prevalence of symptoms was calculated, and 95% confidence intervals (CIs) were determined by exact binomial methods. Pearson’s x 2 test was used to compare categorical variables. For pairwise comparisons of multiple groups, post hoc z-tests were applied after adjusting by Bonferroni correction. Considering the incomplete answers were missing randomly and variables in regression analysis, all analyses were based on complete data (Graham, Reference Graham2009).
Logistic regression was used to explore potential factors (such as region divisions, socio-demographic characteristics, activity and work/study status, experience related to COVID-19, and psychological interventions) associated with symptoms. All factors with significance in the univariable unadjusted logistic analyses, which might convey important information, were then entered into multivariable logistic regression (backward) to adjust for confounding effects of other variables in the model. The contrast was used as an indicator of the subgroup with the lowest prevalence to explore potential risk factors. The adjusted odds ratios (aORs), 95% CIs and P values of the risk factors are provided. Additionally, multicollinearity diagnostics tested by variance inflation factors were verified with < 10 in the final model, suggesting the independence of these factors.
In this study, all the statistical tests were two-sided, and the significance level was set at α = 0.05. All analyses were performed in SPSS software version 27 (IBM Crop) and R software version 4 (R Foundation), and the figures were drawn using GraphPad Prism version 10 (GraphPad Software LLC).
Results
Socio-demographic characteristics
Data from a total of 36,218, 36,097, and 36,306 participants were included in the final analysis at the stable, recurrence and end-of-emergency stages, respectively, with a response rate comparable to 85.9–86.4%. Generally, 93.9–95.0% and 5.0–6.1% of the participants were recruited from quota and snowball sampling; and 87.6–89.0% and 11.0–12.1% of them were surveyed online or through telephone, respectively. Participants recruited from quota or snowball sampling, as well as surveyed online or through telephone were compared with nonsignificant difference in characteristics or outcomes, confirming their equivalence (all P > 0.05). Baseline characteristics of the included participants (subregions, genders, ages and occupations) were compared with the designed quotas and the NPC 2020, and no significant difference was revealed (all P > 0.05), suggesting that the included participants had sufficient representativeness of the general population and inconsequential influences of the missing data.
No significant difference was found in the distribution of regional populations among these 3 surveys, and their socio-demographic characteristics were comparable (Table 1), indicating good comparability. Among these participants at each survey stage, 18,392–18,611 (51.0–51.3%) participants were reported as male, aged 18–87 years (IQR 32–58, the same for 3 surveys), and 19,656–19,707 (54.3–54.5%) participants were urban residents. Most participants had an educational level less than college (28,274–28,622 [78.2–78.8%]) and were married (26,393–26,403 [72.7–73.1%]). A significant difference was found in pandemic-related variables. Increased participants have previously infected (3,349 [9.2%] vs 6,291 [17.4%] vs 24,821 [68.4%]), served as frontline workers (6,038 [16.7%] vs 6,698 [18.6%] vs 7,976 [22.0%]), experienced hospitalization (2,710 [7.5%] vs 4,515 [12.5%] vs 8,176 [22.5%]), quarantine (centralized, 3,788 [10.5%] vs 6,989 [19.4%] vs 10,125 [27.9%]), and at home, 6,219 [17.2%] vs 10,294 [28.5%] vs 16,997 [46.8%]), and had family/friends’ hospitalization (5,487 [15.1%] vs 9,111 [25.2%] vs 16,435 [45.3%]) and death (837 [2.3%] vs 3,731 [10.3%] vs 5,350 [14.7%]) related to COVID-19 from the stable stage to recurrence and end-of-emergency stages.
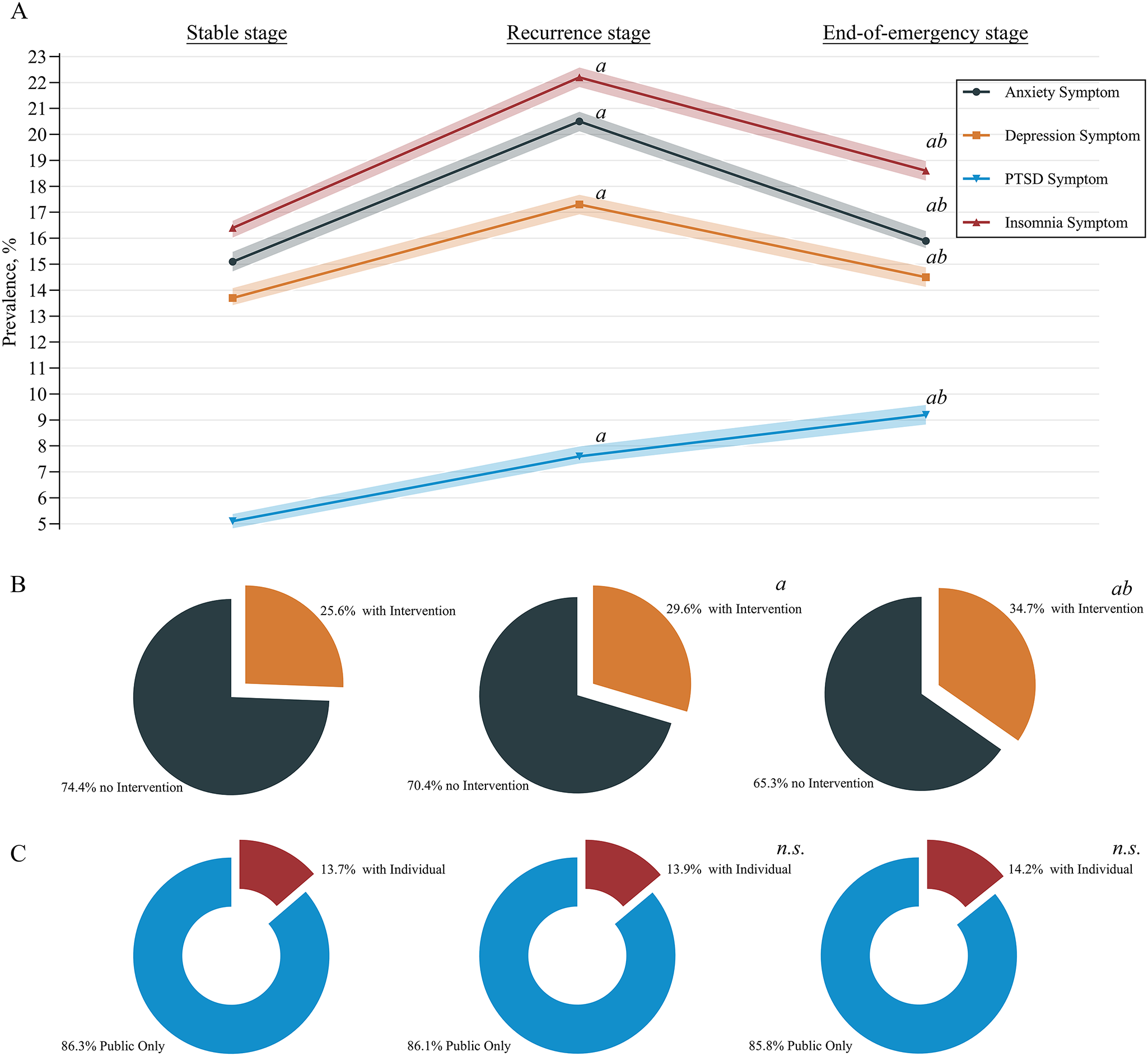
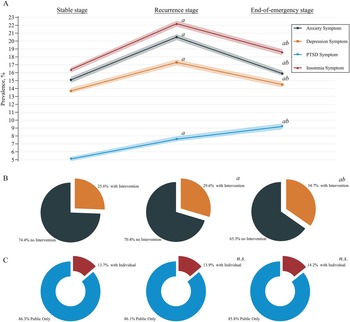
In addition, although a significant increase was observed in participants who accepted psychological intervention (9,266 [25.6%] vs 10,678 [29.6%] vs 12,594 [34.7%]), the proportions of individual counselling did not significantly change for these 3 stages (13.7% [1269] vs 13.9% [1482] vs 14.2% [1,791]) (Fig. 2).
Line chart showing trends in the prevalence of mental health symptoms (A) and sector chart showing the proportions of participants who received psychological intervention (B) and the distribution of intervention types (C; public psychological education only or with individual counselling) during the COVID-19 pandemic. COVID-19, coronavirus disease 2019; PTSD, post-traumatic stress disorder; n.S., Not significant. A(Bonferroni) adjusted P < 0.05 compared with the stable stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction); b(Bonferroni) adjusted P < 0.05 compared with the recurrence stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction).
Prevalence of mental health symptoms at different pandemic stages
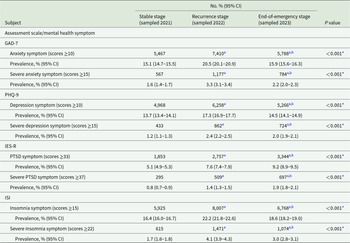
The prevalence of mental health symptoms at different pandemic stages is shown in Table 2 and Fig. 2. The prevalence of anxiety symptoms increased from 15.1% (95% CI, 14.7–15.5%) at the stable stage to 20.5% (20.1–20.9%) at the recurrence stage and decreased to 15.9% (15.6–16.3%) at the end-of-emergency stage. Similar trends were also revealed in the prevalences of depression (13.7% [13.4–14.1%] vs 17.3% [16.9–17.7%] vs 14.5% [14.1–14.9%]) and insomnia (16.4% [16.0–16.7%] vs 22.2% [21.8–22.6%] vs 18.6% [18.2–19.0%]) symptoms. In addition, severe symptoms were observed as anxiety in 1.6% (1.4–1.7%), 3.3% (3.1–3.4%), and 2.2% (2.0–2.3%) of participants; depression in 1.2% (1.1–1.3%), 2.4% (2.2–2.5%), and 2.0% (1.9–2.1%) of participants; and insomnia in 1.7% (1.6–1.8%), 4.1% (3.9–4.3%) and 3.0% (2.8–3.1%) of participants at the stable, recurrence and end-of-emergency stages, respectively, similar to the aforementioned trends. Although symptoms and severe symptoms decreased from the recurrence stage to the end-of-emergency stage, their prevalence was still greater than that at the stable stage. However, the prevalence of PTSD symptoms continuously increased from 5.1% (4.9–5.3%) at the stable stage to 7.6% (7.4–7.9%) at the recurrence stage and reached 9.2% (8.9–9.5%) at the end-of-emergency stage. Severe PTSD symptoms increased from 0.8% (0.7–0.9%) to 1.4% (1.3–1.5%) to 1.9% (1.8–2.1%).
Prevalence of mental health symptoms of all included participants at different COVID-19 pandemic stages (n Stable = 36,218, n Recurrence = 36,097, and n End-of-emergency = 36,306)
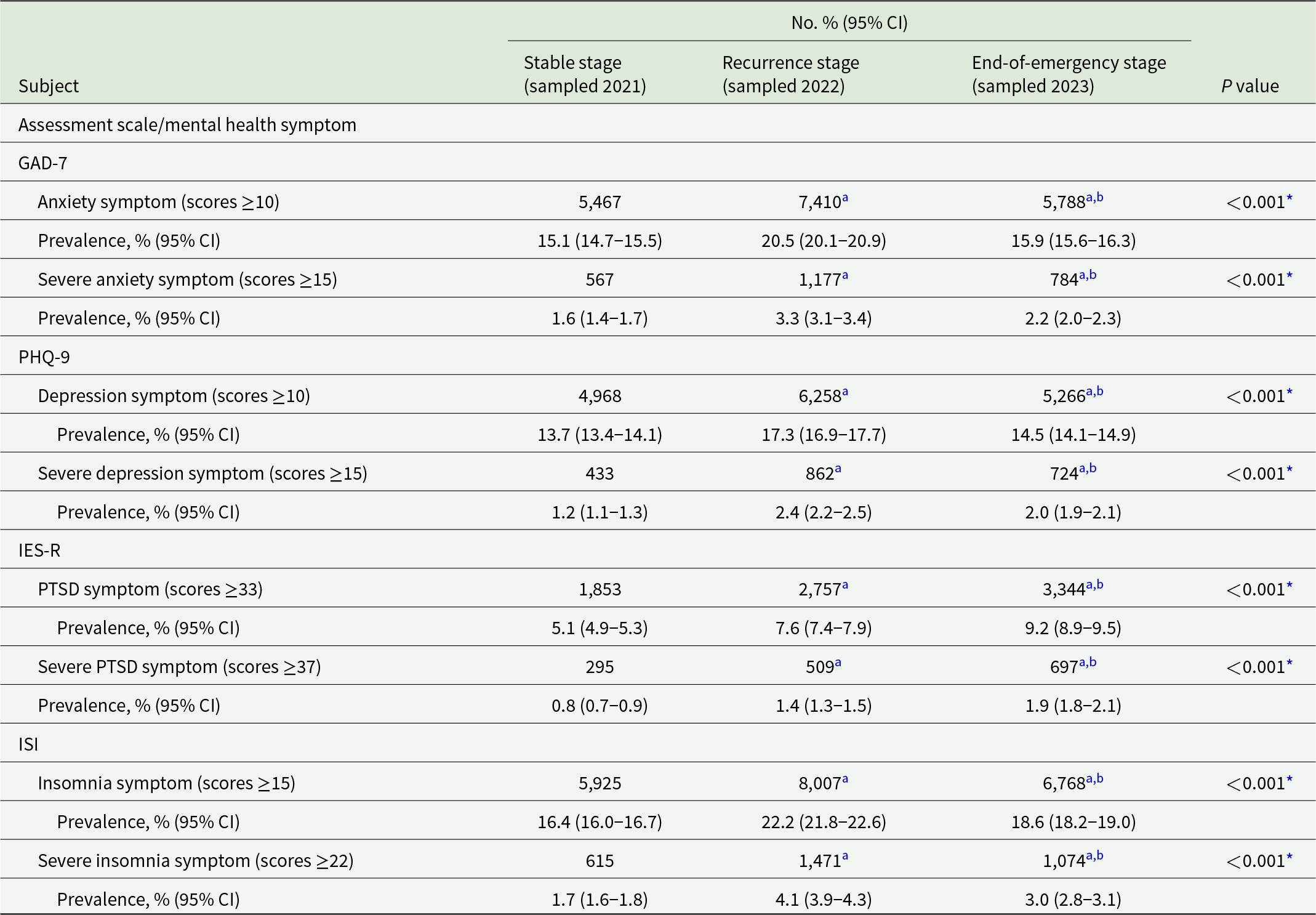
COVID-19, coronavirus disease 2019; GAD-7, Generalized Anxiety Disorder-7 scale; PHQ-9, Patient Health Questionnaire-9; IES-R, Impact of Events Scale-Revised; PTSD, post-traumatic stress disorder; ISI, Insomnia Severity Index; CI, confidence interval. *P < 0.01 (Pearson’s χ2 test).
a (Bonferroni) adjusted P < 0.05 comparing with the Stable stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction).
b(Bonferroni) adjusted P < 0.05 comparing with the Recurrence stage (post hoc z-test for pairwise comparisons, adjusted by Bonferroni correction).
Factors associated with mental health symptoms
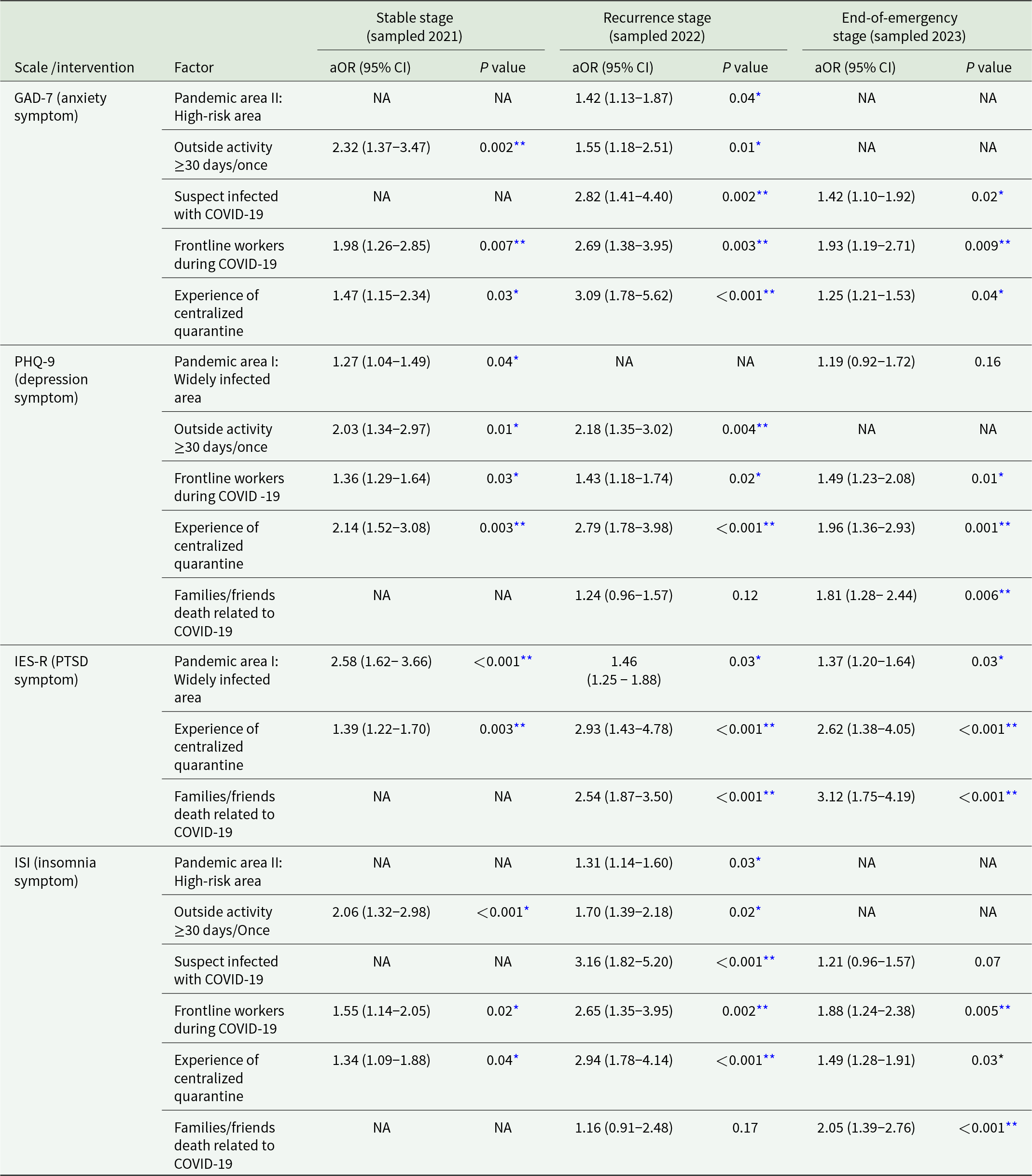
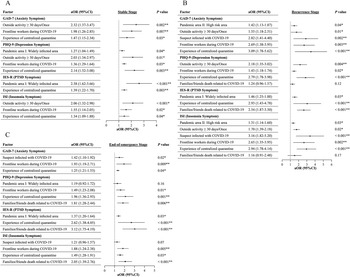
Unadjusted univariable logistic regressions are presented in Supplementary Tables 2-5. After controlling for confounders, multivariable analyses (Table 3 and Fig. 3) revealed that residents of widely infected areas in the initial wave (i.e., Hubei) had a greater risk of symptoms of depression (aOR, 1.27 [95% CI, 1.04–1.49]) and PSTD (aOR, 2.58 [1.62–3.66]) at the stable stage and PTSD at the recurrence stage (aOR, 1.46 [1.25–1.88]) and the end-of-emergency stage (aOR, 1.37 [1.20–1.64]). Living in high-risk areas in the recurrence wave (i.e., Shanghai and Jilin) was associated with a greater risk of symptoms of anxiety (aOR, 1.42 [1.13–1.87]) and insomnia (aOR, 1.31 [1.14–1.60]) at the recurrence stage. Having engaged in outside activities once in ≥30 days had increased odds of having symptoms of anxiety (aOR, 2.32 [1.37–3.47]), depression (aOR, 2.03 [1.34-2.97]) and insomnia (aOR, 2.06 [1.32–2.98]) at the stable stage and anxiety (aOR, 1.55 [1.18–2.51]), depression (aOR, 2.18 [1.35–3.02]) and insomnia (aOR, 1.70 [1.39–2.18]) at the recurrence stage. Participants with suspected infection demonstrated a greater risk of symptoms of anxiety (aOR, 2.82 [1.41–4.40]) and insomnia (aOR, 3.16 [1.82-5.20]) at the recurrence stage and anxiety (aOR, 1.42 [1.10–1.92]) at the end-of-emergency stage. Serving as COVID-19 frontline workers was a common risk factor for symptoms of anxiety (aOR, 1.98 [1.26–2.85]), depression (aOR, 1.36 [1.29–1.64]) and insomnia (aOR, 1.55 [1.14–2.05]) at the stable stage; anxiety (aOR, 2.69 [1.38–3.95]), depression (aOR, 1.43 [1.18–1.74]) and insomnia (aOR, 2.65 [1.35–3.95]) at the recurrence stage; and anxiety (aOR, 1.93 [1.19–2.71]), depression (aOR, 1.49 [1.23–2.08]), and insomnia (aOR, 1.88 [1.24–2.38]) at the end-of-emergency stage. In addition, individuals who experienced centralized quarantine had an elevated risk of symptoms of anxiety (aOR, 1.47 [1.15–2.34]), depression (aOR, 2.14 [1.52–3.08]), PTSD (aOR, 1.39 [1.22–1.70]) and insomnia (aOR, 1.34 [1.09–1.88]) at the stable stage; anxiety (aOR, 3.09 [1.78–5.62]), depression (aOR, 2.79 [1.78–3.98]), PTSD (aOR, 2.93 [1.43–4.78]) and insomnia (aOR, 2.94 [1.78–4.14]) at the recurrence stage; and anxiety (aOR, 1.25 [1.21–1.53]), depression (aOR, 1.96 [1.36–2.93]), PTSD (aOR, 2.62 [1.38–4.05]) and insomnia (aOR, 1.49 [1.28–1.91]) at the end-of-emergency stage. Family/friends’ deaths were also associated with a greater risk of symptoms of PTSD (aOR, 2.54 [1.87–3.50]) at the recurrence stage and depression (aOR, 1.81 [1.28–2.44]), PTSD (aOR, 3.12 [1.75–4.19]) and insomnia (aOR, 2.05 [1.39–2.76]) at the end-of-emergency stage.
Factors associated with mental health at stable (A), recurrence (B) and end-of-emergency (C) COVID-19 pandemic stages. COVID-19, coronavirus disease 2019; GAD-7, Generalized Anxiety Disorder-7 scale; PHQ-9, Patient Health Questionnaire-9; IES-R, Impact of Events Scale-Revised; PTSD, post-traumatic stress disorder; ISI, Insomnia Severity Index; CI, confidence interval. The factors with significance in the univariable analyses (refer to Supplementary Tables 2–5) were then entered into the multivariable logistic regression in a backward fashion to adjust for confounding effects of other factors included in the model. The contrast was set as an indicator determined by the group with the lowest prevalence (proportions) of anxiety, depression, PTSD, and insomnia symptoms to identify potential risk factors for mental health symptoms. The multicollinearity diagnostics showed that variables that were included in the multivariable analyses did not have significant multicollinearity (all variance inflation factors, VIF < 10). *P < 0.05 (multivariable logistic regression); **P < 0.01 (multivariable logistic regression).

Multivariable logistic regression in identifying independent influential factors of psychological symptoms and interventions of all included participants at different pandemic stages (n Stable = 36,218, n Recurrence = 36,097 and n End-of-emergency = 36,306)
The factors with significance in the univariable analyses (refer to Supplementary Table 2–5) were then entered into the multivariable logistic regression in a backward fashion to adjust for confounding effects of other factors included in the model. The contrast was set as an indicator determined by the group with lowest prevalences (proportions) of anxiety symptoms, depression symptoms, insomnia symptoms and psychological interventions to identify risk factors. The multicollinearity diagnostics showed variables that were included in the multivariable analyses did not have significant multicollinearity (all variance inflation factors, VIF < 10). COVID-19, coronavirus disease 2019; GAD-7, Generalized Anxiety Disorder-7 scale; PHQ-9, Patient Health Questionnaire-9; IES-R, Impact of Events Scale-Revised; ISI, Insomnia Severity Index; PTSD, post-traumatic stress disorder; NA, not applicable.
* P < 0.05 (multivariable logistic regression); **P < 0.01 (multivariable logistic regression).
Discussion
Up to date, this is the largest nationwide repeated cross-sectional study on mental health symptoms and associated factors at different COVID-19 pandemic periods for general population, of which dataset can have important contributions to the global scientific community. In total, 36,218, 36,097 and 36,306 participants with sufficient national representativeness were enrolled at 3 crucial stages: stable, recurrence and end of emergency, respectively. The prevalence of anxiety, depression and insomnia symptoms exhibited a similar trend, increasing from 13.7–16.4% at the stable stage to 17.3–22.2% at the recurrence stage. Although the prevalence decreased to 14.5–18.6% at the end-of-emergency stage, it was still higher than that at the stable stage. The prevalence of PTSD symptoms continuously increased from 5.1% at the stable stage to 7.6% and 9.2% at the recurrence and end-of-emergency stages, respectively. Several factors were also associated with a greater risk of mental symptoms, including centralized quarantine, frontline workers, and initial wave widely infected area at all 3 stages; lack of outside activity at the stable and recurrence stages; high-risk areas at the recurrence stage; and suspected infection and family/friends’ deaths at the recurrence and end-of-emergency stages. These findings could more reliably inform public health policies and population-specific strategies and could be an important reference for future potential pandemics and recurrence (Aknin et al., Reference Aknin, Andretti, Goldszmidt, Helliwell, Petherick, De Neve, Dunn, Fancourt, Goldberg, Jones, Karadag, Karam, Layard, Saxena, Thornton, Whillans and Zaki2022).
Estimates of mental health status are closely related to the measurement scales and their cut-off thresholds (Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022; Salari et al., Reference Salari, Hosseinian-Far, Jalali, Vaisi-Raygani, Rasoulpoor, Mohammadi, Rasoulpoor and Khaledi-Paveh2020; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020). In the present study, we applied the cut-offs that optimally prompt probable clinical diagnoses of anxiety, depression, PTSD and insomnia as scores above moderate symptoms (the best cut-off for a probable diagnosis) to avoid overestimation (mild preclinical symptoms) or underestimation (severe symptoms) (Chung et al., Reference Chung, Kan and Yeung2011; Creamer et al., Reference Creamer, Bell and Failla2003; Thorndike et al., Reference Thorndike, Ritterband, Saylor, Magee, Gonder-Frederick and Morin2011; Wang et al., Reference Wang, Bian, Zhao, Li, Wang, Du, Zhang, Zhou and Zhao2014; Wu and Chan, Reference Wu and Chan2003; Zhang et al., Reference Zhang, Liang, Chen, Zhang, Zhang, Weng, Yang, Zhang, Shen and Zhang2013, Reference Zhang, Wang, Zeng, Zhao, Zhang, Zhai, Meng, Wang and Liu2021). In addition, this stratification also improved the compatibility of the current findings with those of pre-COVID-19 studies on mental disorders (Huang et al., Reference Huang, Wang, Wang, Liu, Yu, Yan, Yu, Kou, Xu, Lu, Wang, He, Xu, He, Li, Guo, Tian, Xu, Xu, Ma, Wang, Wang, Yan, Wang, Xiao, Zhou, Li, Tan, Zhang, Ma, Li, Ding, Geng, Jia, Shi, Wang, Zhang, Du, Du and Wu2019; Lu et al., Reference Lu, Xu, Huang, Li, Ma, Xu, Yin, Xu, Ma, Wang, Huang, Yan, Wang, Xiao, Zhou, Li, Zhang, Chen, Zhang, Yan, Ding, Yu, Kou, Shen, Jiang, Wang, Sun, Xu, He, Guo, Jiang, Li, Pan, Wu, Li, Jia, Shi, Shen and Zhang2021), other COVID-19 studies (Chen et al., Reference Chen, Feng, Liu, Wu, Li, Zhang, Yang and Zhang2023; Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022; Salari et al., Reference Salari, Hosseinian-Far, Jalali, Vaisi-Raygani, Rasoulpoor, Mohammadi, Rasoulpoor and Khaledi-Paveh2020; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020), and our previous estimates(Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020). However, it should also be noted that the current samples are all from Chinese populations, and the scales and cut-off values are based on Chinese norms. Although theoretically, the severity classification standards represented by these cut-off values are consistent with those of international samples, further research is needed to validate their international applicability and comparability. Generally, compared with the pre-COVID-19 prevalence of mental disorders (3.6–5.0% for anxiety, depression and other disorders; and 15.0% for insomnia) in the general population in China (Cao et al., Reference Cao, Wang, Zhong, Zhang, Ungvari, Ng, Li, Chiu, Lok, Lu, Jia and Xiang2017; Huang et al., Reference Huang, Wang, Wang, Liu, Yu, Yan, Yu, Kou, Xu, Lu, Wang, He, Xu, He, Li, Guo, Tian, Xu, Xu, Ma, Wang, Wang, Yan, Wang, Xiao, Zhou, Li, Tan, Zhang, Ma, Li, Ding, Geng, Jia, Shi, Wang, Zhang, Du, Du and Wu2019; Kola et al., Reference Kola, Kohrt, Hanlon, Naslund, Sikander, Balaji, Benjet, Cheung, Eaton, Gonsalves, Hailemariam, Luitel, Machado, Misganaw, Omigbodun, Roberts, Salisbury, Shidhaye, Sunkel, Ugo, van Rensburg, Gureje, Pathare, Saxena, Thornicroft and Patel2021), there is a clear indication of an upward burden of mental health problems across different pandemic periods, even after the end of emergency.
During the COVID-19 outbreak, an overall 11.0–31.9% prevalence of mental health symptoms was reported (Chen et al., Reference Chen, Feng, Liu, Wu, Li, Zhang, Yang and Zhang2023; Ettman et al., Reference Ettman, Abdalla, Cohen, Sampson, Vivier and Galea2020; Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022; Salari et al., Reference Salari, Hosseinian-Far, Jalali, Vaisi-Raygani, Rasoulpoor, Mohammadi, Rasoulpoor and Khaledi-Paveh2020; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020). A great number of national and regional governments have applied drastic outside activity restrictions and strict interpersonal isolation, while panic (Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020; Xiong et al., Reference Xiong, Lipsitz, Nasri, Lui, Gill, Phan, Chen-Li, Iacobucci, Ho, Majeed and McIntyre2020), quarantine (Jin et al., Reference Jin, Sun, Zheng and An2021; Kelly, Reference Kelly2021), hospitalization (Patel et al., Reference Patel, Robertson, Kwong, Griffith, Willan, Green, Di Gessa, Huggins, McElroy, Thompson, Maddock, Niedzwiedz, Henderson, Richards, Steptoe, Ploubidis, Moltrecht, Booth, Fitzsimons, Silverwood, Patalay, Porteous and Katikireddi2022), physical distancing (Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020) and policy stringency (Aknin et al., Reference Aknin, Andretti, Goldszmidt, Helliwell, Petherick, De Neve, Dunn, Fancourt, Goldberg, Jones, Karadag, Karam, Layard, Saxena, Thornton, Whillans and Zaki2022) have contributed to serious psychiatric epidemics co-occurring with COVID-19(Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020). After the initial waves of the pandemic, changes in mental health symptoms varied substantially across studies (Patel et al., Reference Patel, Robertson, Kwong, Griffith, Willan, Green, Di Gessa, Huggins, McElroy, Thompson, Maddock, Niedzwiedz, Henderson, Richards, Steptoe, Ploubidis, Moltrecht, Booth, Fitzsimons, Silverwood, Patalay, Porteous and Katikireddi2022; Salanti et al., Reference Salanti, Peter, Tonia, Holloway, White, Darwish, Low, Egger, Haas, Fazel, Kessler, Herrman, Kieling, De Quervain, Vigod, Patel, Li, Cuijpers, Cipriani, Furukawa, Leucht, Sambo, Onishi, Sato, Rodolico, Oliveira Solis, Antoniou, Kapfhammer, Ceraso, O’Mahony, Lasserre, Ipekci, Concerto, Zangani, Igwesi-Chidobe, Diehm, Demir, Wang, Ostinelli, Sahker, Beraldi, Erzin, Nelson, Elkis, Imai, Wu, Kamitsis, Filis, Michopoulos, Bighelli, Hong, Ballesteros, Smith, Yoshida, Omae, Trivella, Tada, Reinhard, Ostacher, Müller, Jaramillo, Ferentinos, Toyomoto, Cortese, Kishimoto, Covarrubias-Castillo, Siafis, Thompson, Karageorgiou, Chiocchia, Zhu and Honda2022). For the Chinese government, work resumption and the ‘normalized prevention and control’ policy were announced in February 2020. A slight increase in the prevalence of anxiety, depression, and insomnia symptoms was observed at 14.9–18.3% (versus 11.0–13.3% with a similar design for the initial wave) at the beginning of work resumption (Wang et al., Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020), and a lower prevalence of symptoms (10.8–16.4%) was reported in later surveys and this study (Tan et al., Reference Tan, Hao, McIntyre, Jiang, Jiang, Zhang, Zhao, Zou, Hu, Luo, Zhang, Lai, Ho, Tran, Ho and Tam2020), as the pandemic was gradually controlled with vaccines(Fiolet et al., Reference Fiolet, Kherabi, MacDonald, Ghosn and Peiffer-Smadja2022; Polack et al., Reference Polack, Thomas, Kitchin, Absalon, Gurtman, Lockhart, Perez, Pérez Marc, Moreira, Zerbini, Bailey, Swanson, Roychoudhury, Koury, Li, Kalina, Cooper, Frenck, Hammitt, Türeci, Nell, Schaefer, Ünal, Tresnan, Mather, Dormitzer, Şahin, Jansen and Gruber2020). A time series analysis of electronic healthcare records also suggested reductions in primary care-recorded self-harm following the onset of the pandemic (Pirkis et al., Reference Pirkis, John, Shin, DelPozo-Banos, Arya, Analuisa-Aguilar, Appleby, Arensman, Bantjes, Baran, Bertolote, Borges, Brečić, Caine, Castelpietra, Chang, Colchester, Crompton, Curkovic, Deisenhammer, Du, Dwyer, Erlangsen, Faust, Fortune, Garrett, George, Gerstner, Gilissen, Gould, Hawton, Kanter, Kapur, Khan, Kirtley, Knipe, Kolves, Leske, Marahatta, Mittendorfer-Rutz, Neznanov, Niederkrotenthaler, Nielsen, Nordentoft, Oberlerchner, O’Connor, Pearson, Phillips, Platt, Plener, Psota, Qin, Radeloff, Rados, Reif, Reif-Leonhard, Rozanov, Schlang, Schneider, Semenova, Sinyor, Townsend, Ueda, Vijayakumar, Webb, Weerasinghe, Zalsman, Gunnell and Spittal2021). The present study captured a crucial pandemic recurrence period when new virus mutations occurred and caused recurrent infections(El-Shabasy et al., Reference El-Shabasy, Nayel, Taher, Abdelmonem, Shoueir and Kenawy2022; Yisimayi et al., Reference Yisimayi, Song, Wang, Jian, Yu, Chen, Xu, Yang, Niu, Xiao, Wang, Zhao, Sun, An, Zhang, Wang, Wang, Yu, Lv, Gu, Shao, Jin, Shen, Xie, Wang and Cao2024), during which the Chinese government announced the ‘dynamic zero’ policy (Bai et al., Reference Bai, Sha, Cheung, Su, Jackson and Xiang2022), a strategy similar to the test-trace-quarantine strategy but still widely restricted cross-regional activities(Kerr et al., Reference Kerr, Mistry, Stuart, Rosenfeld, Hart, Núñez, Cohen, Selvaraj, Abeysuriya, Jastrzębski, George, Hagedorn, Panovska-Griffiths, Fagalde, Duchin, Famulare and Klein2021). There was a significant increase in mental health symptoms (17.3–22.2%) at the recurrence stage, suggesting the synchronous nature of the mental health crisis. In December 2022, the Chinese national government announced the end-of-emergency of the pandemic and abolished restrictions. Our survey at 6 months after this time point suggested that mental health symptoms decreased but remained in 14.5–18.6% of the population, suggesting potential time lag effects and post-acute symptoms (Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022). Experience from other epidemics, such as severe acute respiratory syndrome (SARS), suggested long-term mental health consequences, which could last for more than 3 years (Liu et al., Reference Liu, Kakade, Fuller, Fan, Fan, Kong, Guan and Wu2012; Wu et al., Reference Wu, Fang, Guan, Fan, Kong, Yao, Liu, Fuller, Susser, Lu and Hoven2009). The impacts of chronic mental health necessitate the attention of the global health community and require future studies. The continuous increase in PTSD symptoms is noteworthy. During the recurrence and end-of-emergency periods, the rapid spread of the virus and insufficient medical resources have led to more individuals experiencing quarantine and deaths from family/friends, which could result in traumatic experiences and cause PTSD symptoms (Cao et al., Reference Cao, Wang, Fang, Liu, Bi, Luo, Grace and Olff2022; Cénat et al., Reference Cénat, Blais-Rochette, Kokou-Kpolou, Noorishad, Mukunzi, McIntee, Dalexis, Goulet and Labelle2021; Chamaa et al., Reference Chamaa, Bahmad, Darwish, Kobeissi, Hoballah, Nassif, Ghandour, Saliba, Lawand and Abou-Kheir2021; Chen et al., Reference Chen, Feng, Liu, Wu, Li, Zhang, Yang and Zhang2023; Dubey et al., Reference Dubey, Biswas, Ghosh, Chatterjee, Dubey, Chatterjee, Lahiri and Lavie2020; Jafri et al., Reference Jafri, Zaheer, Fatima, Saleem and Sohail2022), requiring timely preventive and treatment measures. Together, our findings systematically traced the temporalities of the mental health impacts of different COVID-19 pandemic periods and highlighted the increases in mental health symptoms when the pandemic recurred and symptoms remained even after the end of the emergency, especially PTSD symptoms.
Centralized quarantine, frontline workers, and initial wave widely infected area were persistent risk factors for mental health symptoms at all 3 stages. Under centralized quarantine, people might experience multiple pressures, such as infection concerns and interpersonal isolation(Jin et al., Reference Jin, Sun, Zheng and An2021; Kelly, Reference Kelly2021; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020). An epidemiological study of the general population in China during the COVID-19 outbreak also revealed that quarantine was associated with depression, anxiety, insomnia, and acute stress symptoms(Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020), while the current study further confirmed the long-term existence of this risk factor. They also reported that home quarantine contributed to poor mental health (Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020), which was not observed in this study. We assume that this discrepancy is related to expanded knowledge of the virus after the initial waves and more easily accessed psychosocial support at home (Parotto et al., Reference Parotto, Gyöngyösi, Howe, Myatra, Ranzani, Shankar-Hari and Herridge2023). In addition, this study, together with previous studies, suggested long-lasting negative effects, such as PTSD symptoms, requiring sufficient management (Brooks et al., Reference Brooks, Webster, Smith, Woodland, Wessely, Greenberg and Rubin2020; Dubey et al., Reference Dubey, Biswas, Ghosh, Chatterjee, Dubey, Chatterjee, Lahiri and Lavie2020). Frontline workers also reported sustained symptoms of anxiety, depression and insomnia, which was also suggested in studies during the outbreak (Dubey et al., Reference Dubey, Biswas, Ghosh, Chatterjee, Dubey, Chatterjee, Lahiri and Lavie2020; Lai et al., Reference Lai, Ma, Wang, Cai, Hu, Wei, Wu, Du, Chen, Li, Tan, Kang, Yao, Huang, Wang, Wang, Liu and Hu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021). Frontline workers experienced greater occupational exposure risks, increased work overtime and nightshifts, and more frequently witnessed suffering and death of infected patients, requiring particular attention to their mental health and fostering a resilient work environment (Berkhout et al., Reference Berkhout, Sheehan and Abbey2021; Labrague, Reference Labrague2021; Lai et al., Reference Lai, Ma, Wang, Cai, Hu, Wei, Wu, Du, Chen, Li, Tan, Kang, Yao, Huang, Wang, Wang, Liu and Hu2020). Another prominent finding was that residents of the initially wide infected area (i.e., Hubei) had a persistently greater risk of PTSD symptoms. Populations in Hubei (including Wuhan city), which experienced early transmission of COVID-19 in China, experienced the most worries and uncertainty about the pandemic and the initial strict outside activity restrictions and had the highest rates of infection and deaths during the outbreak (Huang et al., Reference Huang, Wang, Li, Ren, Zhao, Hu, Zhang, Fan, Xu, Gu, Cheng, Yu, Xia, Wei, Wu, Xie, Yin, Li, Liu, Xiao, Gao, Guo, Xie, Wang, Jiang, Gao, Jin, Wang and Cao2020; Zhu et al., Reference Zhu, Zhang, Wang, Li, Yang, Song, Zhao, Huang, Shi, Lu, Niu, Zhan, Ma, Wang, Xu, Wu, Gao and Tan2020). In addition to many studies during the initial waves reporting a high risk of psychological distress in Hubei (Lai et al., Reference Lai, Ma, Wang, Cai, Hu, Wei, Wu, Du, Chen, Li, Tan, Kang, Yao, Huang, Wang, Wang, Liu and Hu2020; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021), this study also revealed post-acute symptoms even after the end of emergency, indicating that persistent symptoms are still challenging for residents in this area.
Some stage-specific risk factors were also identified. A lack of outside activity was identified as a risk factor for anxiety, depression and insomnia symptoms during the previous outbreak and return-to-work periods of COVID-19 (Creese et al., Reference Creese, Khan, Henley, O’Dwyer, Corbett, Vasconcelos Da Silva, Mills, Wright, Testad, Aarsland and Ballard2021; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021; Zhang et al., Reference Zhang, Wang, Ding, Meng, Hu, Liu, Zeng, Guan and Wang2020), while current findings suggest that engaging in outside activity once in ≥ 30 days also increases the risk of anxiety, depression and insomnia symptoms at the stable and recurrence stages. As restrictions and isolation controls were abolished after the end of the emergency, the frequency of outside activities was quickly restored, and it no longer served as risk factors. At the recurrence stage, living in a high-risk area was also associated with increased odds of anxiety and insomnia symptoms, suggesting the rationality of mediating mental health policy when a pandemic occurs. With growing populations and their families or friends having experienced the infection, participants with suspected infections and who experienced family/friends’ deaths were at a greater risk of symptoms at the recurrence and end-of-emergency stages. These negative experiences and events were also found to have impacts on mental health during the outbreak (Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020, Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021), inspiring us to protect vulnerable individuals in a timely manner(Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022). These identified risk factors could contribute to the delivery of effective targeted interventions for those at risk for mental health symptoms(Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020; Wang et al., Reference Wang, Zhang, Ding, Meng, Hu, Liu, Zeng and Wang2020). In addition, demographic factors such as sex and age were also previously reported but with substantial heterogeneity and controversial results (Lai et al., Reference Lai, Ma, Wang, Cai, Hu, Wei, Wu, Du, Chen, Li, Tan, Kang, Yao, Huang, Wang, Wang, Liu and Hu2020; Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022; Shi et al., Reference Shi, Lu, Que, Huang, Liu, Ran, Gong, Yuan, Yan, Sun, Shi, Bao and Lu2020), while the findings of the current study were not significant. This variation might be related to the sample, location and culture, and future controlled studies are needed.
Finally, although a significant increase in the proportion of patients receiving psychological intervention was observed, only limited of them have received individual counselling, which were still not enough to cover potential mental health burdens (Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020; Kola et al., Reference Kola, Kohrt, Hanlon, Naslund, Sikander, Balaji, Benjet, Cheung, Eaton, Gonsalves, Hailemariam, Luitel, Machado, Misganaw, Omigbodun, Roberts, Salisbury, Shidhaye, Sunkel, Ugo, van Rensburg, Gureje, Pathare, Saxena, Thornicroft and Patel2021; Salari et al., Reference Salari, Hosseinian-Far, Jalali, Vaisi-Raygani, Rasoulpoor, Mohammadi, Rasoulpoor and Khaledi-Paveh2020). Public psychological education has its advantages as providing some knowledge in relieving psychological distress and promoting those with potential symptoms to pursue professional interventions. But for people who have already developed mental health symptoms, especially severe symptoms, public education is not enough, while individual counselling provided by professional psychologists with systematic terms and individualized treatments could be more effectively (Hossain et al., Reference Hossain, Tasnim, Sultana, Faizah, Mazumder, Zou, McKyer, Ahmed and Ma2020; Labrague, Reference Labrague2021; Wang et al., Reference Wang, Zhang, Guan, Ding, Meng, Hu, Liu, Zeng and Wang2021). While pandemic during an infectious could be a non-negligible barrier for face-to-face psychological interventions, an important lesson was the growing evidence of remotely computerized or videoconferencing delivered interventions during COVID-19, which guides more safety measures (Bryant et al., Reference Bryant, Dawson, Keyan, Azevedo, Yadav, Tran, Rawson and Harvey2022; Liu et al., Reference Liu, Qiao, Xu, Zhao, Yang, Wen, Li, Nie, Dong, Tang, Jiang, Wang, Zhao and Xu2021). However, their efficacy, stability, acceptability and applicability still need future comparisons with traditional well developed measures. To better address changes in the mental health burdens of society, psychosocial crisis prevention and multipronged intervention models should be urgently developed at the level of individualization by the government, healthcare providers, and other stakeholders in preparation for future potential pandemics and recurrences (Dubey et al., Reference Dubey, Biswas, Ghosh, Chatterjee, Dubey, Chatterjee, Lahiri and Lavie2020; Dzinamarira et al., Reference Dzinamarira, Iradukunda, Saramba, Gashema, Moyo, Mangezi and Musuka2024). Furthermore, considering potential post-acute and long-term symptoms, prolonged evidence-based interventions should be applied to address mental health and unfavourable socio-environmental factors for at-risk populations (Ettman et al., Reference Ettman, Abdalla, Cohen, Sampson, Vivier and Galea2020; Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022).
Our study has some limitations. First, because of pandemic restrictions, random sampling was unavailable, which might introduce selection bias. Second, due to the nature of cross-sectional surveys, the present study did not follow the same group due to sensitivity concerns. Additionally, the participants in the current study were surveyed only 6 months after the end of emergency. A longitudinal cohort study with longer follow-ups would be better for exploring changes in and long-term effects of mental health symptoms. Third, comparisons of the current findings with those of other studies could reveal heterogeneity in sample and methodology (especially for the assessment scales used and their cut-offs), and findings from the current study still need to be verified in other countries/regions and international collaboration, which could be a future research direction. Finally, the measurement of mental health symptoms was based on self-reported screening tools, which cannot represent clinical diagnoses.
Conclusions
The prevalence of anxiety, depression, and insomnia symptoms increased from 13.7–16.4% at the stable stage of the COVID-19 pandemic to 17.3–22.2% at the recurrence stage. Although the prevalence decreased to 14.5–18.6% at the end-of-emergency stage, it was still higher than that at the stable stage. The prevalence of PTSD symptoms continuously increased from 5.1% at the stable stage to 7.6% and 9.2% at the recurrence and end-of-emergency stages, respectively. Several key factors and their variations were identified at different pandemic stages. Centralized quarantine, frontline workers and initial wave-widely infected areas had a persistent increase in the risk of symptoms, while stage-specific risk factors included a lack of outside activity, high-risk recurrence areas, suspected infections and family/friend deaths, suggesting potential differences in at-risk populations. Current individual counselling still does not cover those potentially experienced mental health symptoms enough.
List of abbreviations
- GAD-7
Generalized Anxiety Disorder-7 Scale
- PHQ-9
Patient Health Questionnaire-9
- ISI
Insomnia Severity Index
- COVID-19
coronavirus disease 2019
- aORs
adjusted odds ratios
- PTSD
post-traumatic stress disorder.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796025100243.
Financial support
This study was supported by the National Natural Science Foundation of China (81830033 and 81971070) and the National Key Research and Development Program of China (2022YFC2405100 and 2016YFC0105900). The funders played no role in the design and conduct of the study; the collection, management, analysis and interpretation of the data; the writing, review or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests
The authors declare that they have no competing interests.
Ethical standards
The ethics committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University approved this study. All participants have provided informed consent for this study by clicking an ‘agree to the consent’ button before they began the online survey or by offering oral consent before a telephone review of the survey. This study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments and was reported following the STROBE Statement for cross-sectional studies. Consent for publication was not applicable.
Availability of data and materials
The data that support the findings of this study are included in the article/supplementary material. More information is available on request from the corresponding authors upon reasonable request.
Acknowledgements
We would like to gratitude all the participants, volunteers, investigators and site coordinators for their constructive participation and generous assistance. Dr. Shu Wang served as senior collaborator of the Global Burden of Disease (GBD) Collaborator Network, which is supported by the Institute for Health Metrics and Evaluation (IHME), the University of Washington.
Author contributions
SW designed the study, collected the data, analysed the data, illustrated figures, drafted the manuscript and revised the manuscript. YZ, WD, YM, HH, YG, XZ and ZL collected the data, analysed the data and revised the manuscript. MW and JZ designed and supervised the study, collected the data, analysed the data, and revised the manuscript. All the authors read and approved the final manuscript.
Minzhong Wang and Shu Wang can also be contacted for correspondence email: wmzwlq@163.com and email: WangShu.cn@Outlook.com.




 Open access
Open access