Vanishing twin syndrome (VTS) is a type of miscarriage when one or more fetuses in a pregnancy of multiples (i.e., twins, triplets, and higher-order multiples) fail to develop or are lost, typically in the first trimester (Zamani & Parekh, Reference Zamani and Parekh2021). According to Quenby et al. (Reference Quenby, Gallos, Dhillon-Smith, Podesek, Stephenson, Fisher, Brosens, Brewin, Ramhorst, Lucas, McCoy, Anderson, Daher, Regan, Al-Memar, Bourne, MacIntyre, Rai, Christiansen, Sugiura-Ogasawara and Coomarasamy2021), ‘Miscarriage is generally defined as the loss of a pregnancy before viability [outside of the womb]’ (para. 1). However, VTS may occur as late as the third trimester, though it is much rarer (Zamani & Parekh, Reference Zamani and Parekh2021). Recent estimates suggest VTS occurs in more than 50% of naturally conceived triplet pregnancies, more than 40% of naturally conceived twin pregnancies and at least 30% of pregnancies conceived with fertility assistance, but accurately determining the prevalence in natural pregnancies is a challenge due to a lack of close and early monitoring from conception, which more often occurs in pregnancies conceived with fertility assistance (Zamani & Parekh, Reference Zamani and Parekh2021). The potential outcomes of VTS are influenced by several factors, including chorionicity and amnionicity — key characteristics of multiple pregnancies (Zamani & Parekh, Reference Zamani and Parekh2021). Chorionicity refers to the number of placentas present in a multiple pregnancy, while amnionicity describes whether the fetuses share an amniotic sac (Miller, Reference Miller2021). These factors can significantly impact the risks associated with VTS, including complications such as twin-to-twin transfusion syndrome (TTTS) in monochorionic pregnancies (Miller, Reference Miller2021).
This variation in circumstances leads to different biological outcomes, including complete resorption of the deceased fetus by the maternal body or the surviving twin, the formation of a blighted ovum, or compression and calcification of fetal tissue into what is known as fetus papyraceous (Zamani & Parekh, Reference Zamani and Parekh2021). Although these are the primary biological processes associated with VTS, clinical outcomes can vary significantly, affecting both the surviving fetus and the mother. Risks to the surviving twin can include preterm birth, low birth weight, spina bifida, chimerism, psychological disorders, epigenetic alterations, and other fetal malformations (Császár & Bókkon, Reference Császár and Bókkon2019; Fjeldstad et al., Reference Fjeldstad, Johnsen and Staff2020; van Dongen et al., Reference van Dongen, Gordon, Odintsova, McRae, Robinson, Hall, Boomsma and Martin2021), while maternal complications may include vaginal bleeding, cramping, placental abnormalities, and emotional distress (Evron et al., Reference Evron, Sheiner, Friger, Sergienko and Harlev2015; Highet et al., Reference Highet, McCarthy and Lally2022; Song et al., Reference Song, Larsson, Fang, Almqvist, Pedersen, Magnusson and Valdimarsdóttir2020; Weitzner et al., Reference Weitzner, Barrett, Murphy, Kingdom, Aviram, Mei-Dan, Hiersch, Greg, Van Mieghem, Abbasi, Fox, Rebarber, Berghella and Melamed2023). Furthermore, aside from the biologically complex aspects of this type of miscarriage, confusion for providers and patients may be compounded by the use of ambiguous terminology to denote and discuss the syndrome. For example, while ‘vanishing twin syndrome’ is the most commonly used, it implies relevance only to twins, leading to misunderstandings in the literature (Batsry & Yinon, Reference Batsry and Yinon2022). Other terms used include ‘vanishing twins syndrome’ (plural), which may imply the vanishment of more than one twin (Sun et al., Reference Sun, Jiang and Chen2017). As previously indicated, full vanishment of the deceased fetus(es) does not always occur, thus any form of ‘vanishing twin syndrome’ may be misleading, especially in diagnostics and medical imaging.
VTS may be classified under the broader umbrella of pregnancy loss, but it is distinct from traditional miscarriage. While spontaneous miscarriage involves the complete expulsion or spontaneous abortion of fetal tissue, VTS often involves partial retention of fetal remnants. The classification of VTS as a form of pregnancy loss is subject to variation in medical terminology and provider communication, which may contribute to discrepancies in how patients are informed about their diagnosis. Furthermore, providers’ perspectives on fetal viability, personal biases, and institutional policies may shape the way VTS diagnoses are communicated to patients (Brann et al., Reference Brann, Bute and Scott2020; Hayton, Reference Hayton2010). Additionally, ethical and legal debates over the classification of fetal remains as medical waste versus human remains add complexity to the discussion, influencing how information is presented to patients and whether they are offered options for memorialization (Middlemiss, Reference Middlemiss2021; Nahidi et al., Reference Nahidi, Awad, Mills, Lewis and Woolard2021).
Although research on VTS remains limited, existing studies suggest that communication surrounding perinatal loss can significantly impact parental coping and psychological outcomes (Batsry & Yinon, Reference Batsry and Yinon2022; Richards et al., Reference Richards, Graham, Embleton, Campbell and Rankin2015). Most available research has focused on the biological and obstetric implications of VTS, while little attention has been given to how patients comprehend their diagnosis and the quality of provider communication. This gap in research contributes to inconsistencies in patient management, including how patients are counseled and supported after experiencing VTS (Rankin et al., Reference Rankin, Hayes and Embleton2021). Additionally, terminological ambiguities — such as whether VTS should be classified as twin loss, pregnancy loss, or a variant of miscarriage — exacerbate patient confusion and lead to variability in healthcare provider responses (Batsry & Yinon, Reference Batsry and Yinon2022). Richards et al. (Reference Richards, Graham, Embleton, Campbell and Rankin2015) found that mothers who experienced perinatal loss of a co-twin reported a lack of emotional support from healthcare providers, highlighting the need for clearer communication and improved psychological care. Without standard protocols, patients may receive inadequate information and support, which may hinder their patient experience and ability to process the loss, make informed decisions, and be equipped to care for their surviving child(ren) postpartum (Rankin et al., Reference Rankin, Hayes and Embleton2021).
Establishing guidelines for VTS management remains a challenge due to the complexity of care coordination among obstetricians, maternal-fetal medicine specialists, and mental health professionals (Weitzner et al., Reference Weitzner, Barrett, Murphy, Kingdom, Aviram, Mei-Dan, Hiersch, Greg, Van Mieghem, Abbasi, Fox, Rebarber, Berghella and Melamed2023). Although guidelines exist for managing multiple pregnancies, including recommendations from the National Institute for Health and Care Excellence (NICE) in the UK, these guidelines do not specifically address VTS (National Institute for Health and Care Excellence, 2013). This absence of specific protocols can result in patients receiving varying levels of information and support depending on their healthcare provider and location. NICE guidelines suggest that chorionicity and amnionicity should be recorded between 11w2d and 14w1d, but given that VTS can occur as early as 6 weeks, some patients may receive incomplete or delayed information regarding their pregnancy status (Khalil et al., Reference Khalil, Giallongo, Bhide, Papageorghiou and Thilaganathan2020). Thus, future guidelines should account for the risks associated with early loss in multiple pregnancies and consider suggesting earlier and closer monitoring.
To the extent of the knowledge of the authors, this study is among the first to analyze the lived experiences of individuals diagnosed with VTS, with a particular focus on patient-provider communication. Common themes in patient-provider discussions, diagnostic experiences, and information gaps provide insights into how patient care, and potentially patient outcomes, may be improved. Additionally, the findings may inform potential strategies for standardizing VTS-related communication in clinical practice, enhancing provider education and training, and ensuring that patients receive comprehensive, accurate, and empathetic information about their diagnosis.
Materials and Methods
A global, online survey was developed and analyzed using Qualtrics. The survey contained 11 questions, including quantitative demographic questions, open-ended qualitative questions, and one sliding-scale rating question. All questions were optional. Participants completed the questionnaire once and did not have follow-up participation. A total of 153 individuals participated in the study (N = 153), but some participants opted to not answer every question. The study targeted individuals who had experienced or believed they had experienced VTS. To ensure clarity, eligibility criteria were refined as follows:
-
Individuals who were formally diagnosed with VTS prior to the study.
-
Individuals who suspected they had previously experienced VTS without receiving a formal diagnosis (e.g., in cases of patients born prior to mainstream use of ultrasound).
-
Individuals who had experienced the loss of a co-twin during pregnancy.
All individuals were eligible to participate, provided they met one of the above criteria and were over the age of 18. The survey was open to participants for 3 months, from February 27, 2024 to April 27, 2024.
A combination of snowball sampling, voluntary response sampling, and convenience sampling was used. The researchers distributed the survey within various VTS and twin loss parent and survivor support groups, as well as through bereavement and research organizations and social media platforms. Participants were recruited from various VTS and twin-loss support communities, as well as through bereavement and research organizations. Organizations that participated in sharing the survey included Multiples of America (i.e., the National Organization of Mothers of Twins Clubs), the International Council for Multiple Birth Organizations, Return to Zero H.O.P.E., the Pregnancy Loss and Infant Death Alliance, and Twins Trust. Several organizations publicly shared the survey on their websites and social media, while others distributed it privately among members. Social media platforms used for recruitment included LinkedIn, Facebook, Instagram, and X.
To assess participants’ experiences and sentiment regarding VTS, the survey included the following measures:
-
Demographics: Primary country of residence while pregnant with VTS, month and year of VTS diagnosis.
-
Experience with VTS: Whether they had received a formal diagnosis, suspected they had experienced VTS without a diagnosis, and timing of the loss.
-
Sentiment and perceived support: Participants rated their experiences with healthcare providers using a sliding scale (0−10) to measure satisfaction and emotional support received. Additionally, Qualtrics AI was used to perform sentiment analysis on some open-ended reflection questions. Sentiment analysis results were manually reviewed by the research team.
-
Open-ended reflections: Participants were asked to describe their diagnosis experience, communication with healthcare providers, and what information they wished had been provided.
Qualtrics’ Stats iQ and Crosstabs iQ tools were used to analyze quantitative data, and qualitative responses were thematically double-coded to identify recurring themes in patient experiences.
Institutional approval for this study was granted by the Institutional Review Board at the Massachusetts College of Pharmacy and Health Sciences on May 2, 2024 (reference number IRB-2022-2023-123). The study was classified as exempt, as no private health information was collected. All participants provided informed, written consent virtually via the study survey before participation. Participants did not receive any financial or material compensation for their participation in the study.
Results
Among the 153 total responses received, more than 60% originated from the United States, with additional responses from Europe, Australia, New Zealand, Central America, and the Middle East, as depicted in Figure 1. The analysis aimed to assess the quality of provider communication and the level of information patients received during their VTS diagnosis.
Number of responses per country of residence while pregnant with VTS (N = 153).

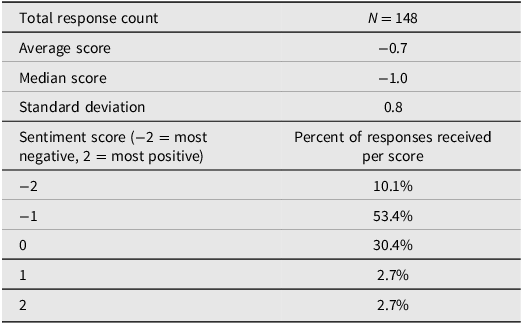
Participants who received formal diagnoses reported predominantly negative sentiment toward provider communication, with an average sentiment score of −0.7 on a scale from −2 (most negative) to 2 (most positive); 53.4% of responses were rated at −1, indicating a largely negative perception of how risks and symptoms were communicated by healthcare providers (Table 1). Five responses were omitted from the analysis as they did not contain sufficient data for inclusion. A sentiment score of −0.7 suggests that while some participants had neutral or slightly positive experiences, the majority found their provider communication inadequate or distressing. The standard deviation of 0.8 indicates considerable variation in how providers conveyed information across different patient experiences.
Sentiment analysis of participant recollection of how provider(s) offered information any potential risks or symptoms associated with VTS

When participants rated the amount of information they received during their VTS diagnosis on a scale of 0−10 (10 being the most informative, 0 being the least), the average score was 3.0, reflecting widespread dissatisfaction with the level of information provided. A standard deviation of 2.6 suggests significant variability in the quality of information among participants. These findings indicate that while some patients may have received detailed explanations, most found the information lacking or unclear.
Chorionicity Awareness
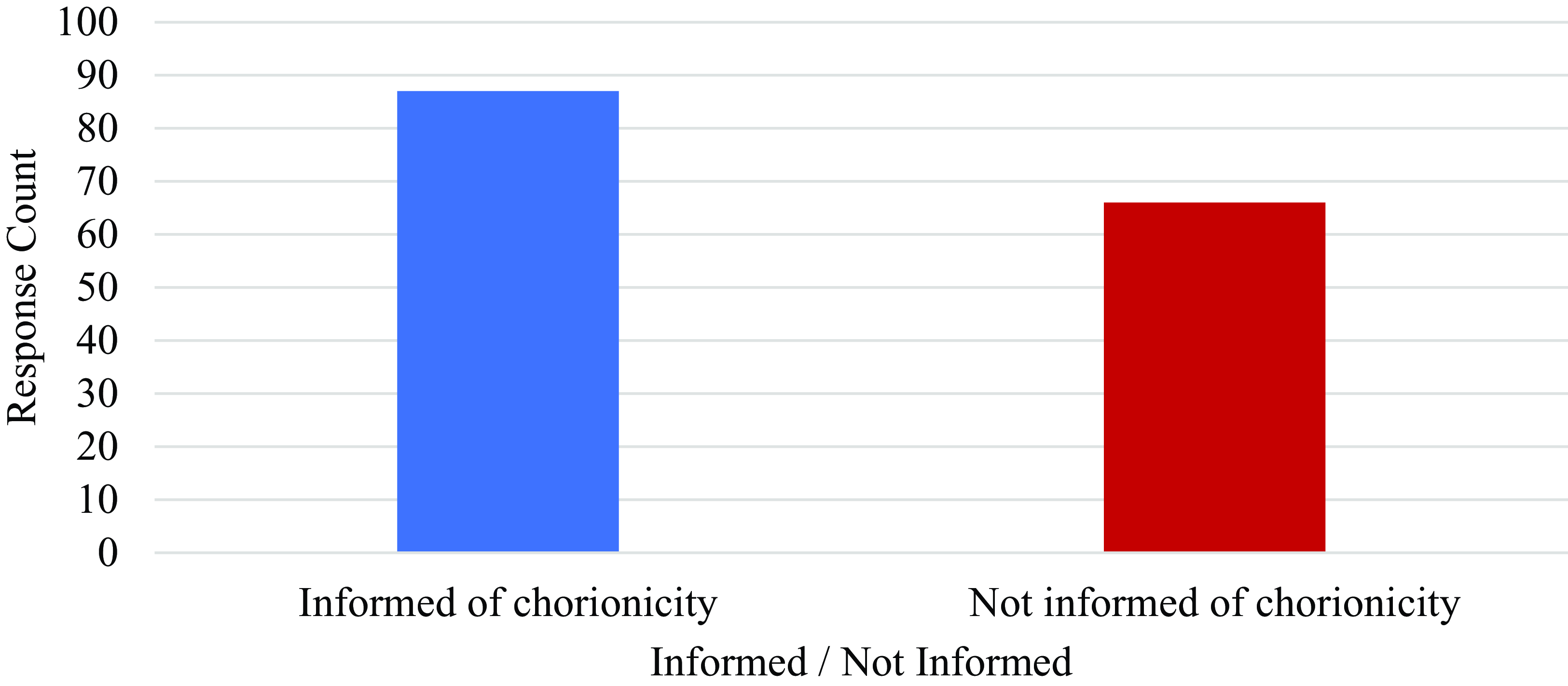
When asked whether they were informed about chorionicity during their VTS pregnancy, 43% of respondents reported that they were not informed, as illustrated in Figure 2. This lack of disclosure may be due to the timing of VTS diagnosis — if the loss occurred early in pregnancy (before 11−14 weeks gestation), chorionicity might not have been assessed. The lack of disclosure may also be due to the corresponding lack of provider requirements to disclose chorionicity even in cases of blighted ova. However, given its clinical significance in cases where loss occurs as early as 6−8 weeks gestation, improving provider communication about chorionicity of any deceased multiples or blighted ova is necessary to ensure that patients receive comprehensive information about their pregnancies so they can make the most informed decisions for themselves and the surviving child(ren). Australia had an equal amount of ‘yes’ (informed) and ‘no’ (not informed) responses, while just under half of the responses from the United States were marked ‘no’ (not informed), as noted in Figure 3. Just over 40% of responses from countries comprising the United Kingdom also marked ‘no’ (not informed). Responses received from Canada and New Zealand indicate providers in these nations are rated highest in informing VTS patients of chorionicity based on self-reported patient experiences.
Number of respondents informed of multiple chorionicity during VTS diagnosis (N = 153).

Percent of responses by nation that were informed of the chorionicity of their multiples during their VTS diagnosis.

Desired Information and Support
The list below presents a ranking of the types of information and resources that participants expressed desire to have during their VTS experience, beginning with the most common:
-
1. Support groups or peer connections
-
2. Mental health resources (grief counseling, emotional support)
-
3. Genetic testing information
-
4. Long-term effects on the surviving twin
-
5. Chorionicity and risks to surviving twin
-
6. General VTS information (causes, why it happens, statistics)
-
7. Written materials to reference later
-
8. Medical follow-up recommendations
-
9. Provider sensitivity and acknowledgment of loss.
Some redundancy was identified in the data used to produce the list above. These data were consolidated to avoid duplication.
The following five responses are direct quotes gathered from participants in response to the following survey prompt: Describe how your provider(s) informed you of your vanishing twin syndrome diagnosis and the fetal loss(es) that occurred or is currently occurring within your body.
They told me at my 7.2 ultrasound that the heart of the second baby was too slow and he was a little behind for his size, so I would be losing him. They booked me another ultrasound 10 days later and his little heart had stopped.
I went in for an ultrasound at 5 weeks pregnant due to bleeding. I was told I was having a di/di twin pregnancy. Both sacs appeared to have implanted ‘perfectly’. Two weeks later I was on vacation and experienced bright red bleeding. I went to the emergency room and was told there was only one baby and there were no longer any signs of a twin pregnancy. Because it was a different hospital, they did not diagnose me with VTS because they did not have confirmation that my pregnancy had originally been a twin pregnancy. When I returned to my own doctor’s office the next week, I received the VTS diagnosis.
OBGYN told me it was a ‘piece of junk’. ER doctor told me I was pregnant with twins but only one had a heartbeat, paperwork showed the chorionicity.
Went to the ER for bleeding early [in] pregnancy thinking I was only pregnant with one baby and miscarrying, ultrasound showed 2 sacs/yolk sacs. I was informed through numerous test results and ultrasound notes.
I was simply shown my living child and the second gestational sac. I had experienced a prior anembryonic pregnancy, prior twin stillbirth, and prior twin live birth, so my provider just acknowledged that the second sac had been a second embryo, but it was not developing.
Overall, the responses above reflect the diverse ways in which healthcare providers convey the diagnosis of vanishing twin syndrome, from direct communication to instances of confusion due to conflicting information. Additionally, the responses illustrate the complex network of care that is demanded by obstetrics and gynecology, especially when there is a reduction in pregnancies of multiples.
Discussion
Key Findings and Implications
This study highlights significant communication challenges between providers and patients diagnosed with VTS. Findings indicate that many patients felt uninformed or unsupported, with low sentiment scores reflecting dissatisfaction with provider communication. The lack of discussion regarding chorionicity suggests a need for standardized guidelines to ensure that key aspects of multiple pregnancies are consistently addressed during patient consultations. The results underscore the importance of improving healthcare provider education on VTS, ensuring that patients receive comprehensive and accurate information. Future research should explore tailored interventions aimed at enhancing patient-provider communication and developing evidence-based protocols for managing VTS pregnancies.
Limitations and Future Directions
This study relied on self-reported data, which may introduce recall bias. Additionally, the recruitment strategy primarily targeted support groups, potentially leading to sampling bias, as participants who had extreme experiences (both negative and positive) may have been more likely to respond. While responses were received from multiple countries, country-specific comparisons were omitted due to sample size limitations. Some nations were represented by only one or two participants, making it inappropriate to draw conclusions about national differences. Instead, the study focuses on broader trends in patient-provider communication across all respondents. Responses gained throughout this research do not include individuals who do not have access to online surveys. Additionally, the study’s cross-sectional design limits the ability to establish causal relationships between variables. Relationships between variables are also inhibited in some cases as medical education/training, laws, and regulations can vary by nation, state/province, and individual institutions (e.g., disposal/memorialization of fetal remains).
Moreover, most of the responses gathered were from individuals who experienced VTS between 1995 and the present. Older populations born before the routine use of ultrasound may have had undiagnosed cases of VTS, with some only identified postpartum through findings such as fetus papyraceous. However, due to the limited availability of diagnostic technology at the time, these cases were less likely to be formally recorded or recognized. While fewer individuals from this era are represented in the data, it is essential to acknowledge their experiences, consider how advancements in medical imaging have influenced the detection and understanding of VTS, and recognize the potential limitations these technological shifts may introduce in interpreting historical trends. Moreover, future studies should include a more diverse sample, including individuals of wider age ranges and those who may not be active in VTS-related support communities, to ensure a more representative analysis of patient experiences.
Conclusion
This study reveals critical gaps in the way VTS diagnoses are communicated to patients, emphasizing the need for standardized provider education and clearer patient information. Addressing these issues could improve patient experiences by ensuring that those diagnosed with VTS and other types of miscarriage/death of multiples receive the support and guidance necessary to navigate their pregnancy and post-diagnosis care effectively.
Acknowledgments
Multiples of America (National Organization of Mothers of Twins Cubs Inc.), Pam Edelman and Kimberly Ozark; Dr Marc A. Nascarella, Massachusetts College of Pharmacy and Health Sciences; International Council of Multiple Birth Organisations (ICOMBO) and Dr Carloyn Lister; Dr Anthony Lacina and Helen Ewing, Massachusetts College of Pharmacy and Health Sciences; Dr Kiley Hanish, Return to Zero H.O.P.E.; Pregnancy Loss and Infant Death Alliance (PLIDA); Twins Trust; Dr Jeff Craig, Murdoch Children’s Institute; Dr Wolfgang Rumpf, University of Maryland Global Campus; The Columbus Mothers of Twins Club; Alvaro Danilo Silva, Silva Music Studios; Alison Jacobson, First Candle; Zane Welker, Phosphorix Ltd.
Authorship
During the preparation of this work the authors used ChatGPT 3.5 in order to reduce the word count of the original manuscript. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Competing interests
None.
Funding
No funding was obtained for this research.