


Background
The Fontan operation completes single ventricle palliation and has been shown to have excellent perioperative and long-term outcomes. Reference Tweddell, Nersesian and Mussatto1,Reference Rogers, Glatz and Ravishankar2 However, there is a subset of patients who reach superior cavopulmonary anastomosis, or stage 2 palliation, but do not advance to Fontan. As patients progress through staged palliation, changing haemodynamics and other medical conditions can prevent completion of Fontan. The attrition of patients between stage 2 and Fontan, or failure to complete Fontan, has been described in other literature as approximately 8–13% over different centres and eras. Reference Lawrence, Ittenbach and Hunt3,Reference Stack, Schluger and Roberts4,Reference Carlo, Carberry and Heinle5 Risk factors for mortality throughout single ventricle palliation have been described, Reference Cnota, Allen and Colan6,Reference Rochelson, Richmond, LaPar, Torres and Anderson7,Reference Alsaied, Bokma and Engel8 but there has been less literature regarding the risk of non-Fontan candidacy and the pathways of those who cannot complete single ventricle palliation. Reference Zheng, Lee and dUdekem9 Patients on the single ventricle pathway are a heterogeneous group with variability in anatomic diagnosis with single left versus right ventricle, differences in additional surgery needed initially in infancy, and even differences in provider practices leading to variable timing of pre-Fontan testing. Reference Wallace, Jaggers and Li10,Reference Loomba, Frommelt, Anderson, Flores and Tweddell11,Reference Pace Napoleone, Oppido, Angeli, Giardini, Resciniti and Gargiulo12 Non-Fontan candidacy can be a source of emotional stress on the patient, family, and providers. Given the uncertainty of Fontan attrition and lack of literature into pathways after non-Fontan candidacy, we sought to describe the incidence of completion at our institution, investigate the reasons for non-Fontan candidacy, and describe pathways after non-candidacy was determined.
Methods
This is a retrospective single-centre study including patients who underwent single ventricle palliation between January 1st, 2010, and December 31st, 2020. Our institutional surgical database was queried, and patients who completed superior cavopulmonary anastomosis were included for analysis. Clinical data were extracted from the medical records. The typical age of Fontan was defined as ranging from 2 to 4 years old based on the majority institutional practice. Patients who completed or were referred for Fontan by 4 years old were included in the Fontan group. Referral for Fontan required all pre-Fontan testing (cardiac catheterisation and transthoracic echocardiogram) had been reviewed at the institutional combined Cardiology and Cardiothoracic Surgery conference and were determined to be a candidate for Fontan. Patients who underwent 1.5 or 2 ventricle repair or were lost to follow-up between superior cavopulmonary anastomosis and typical age of Fontan were excluded from analysis. Any patient with late pre-Fontan testing was excluded from the analysis, including death prior to pre-Fontan testing, Kawashima, or late referral for provider practice preference. This was done in an effort to compare patients with similar management strategies. Baseline demographics were obtained from the medical record, and notes were reviewed to determine the main reason for non-Fontan candidacy or reason for delay of pre-Fontan testing. Cardiac catheterisation reports were reviewed for haemodynamic data. Echocardiograms were reviewed pre- and post-stage 2 and Fontan to obtain the degree of atrioventricular valve regurgitation and a qualitative functional assessment. This study was approved by the Children’s Healthcare of Atlanta Institutional Review Board (IRB #00000210), and informed consent was waived.
Statistical analysis
Statistical analysis was completed in IBM SPSS version 29.0.2.0 (Armonk, NY). Continuous data were analysed with the paired t-test or Mann-Whitney U test, and categorical data were analysed with the Pearson chi-square test. Odds ratios were calculated for specific variables of interest. A p-value of <0.05 was considered significant. Kaplan-Meier survival curves were generated to compare Fontan candidates to non-Fontan candidates.
Results
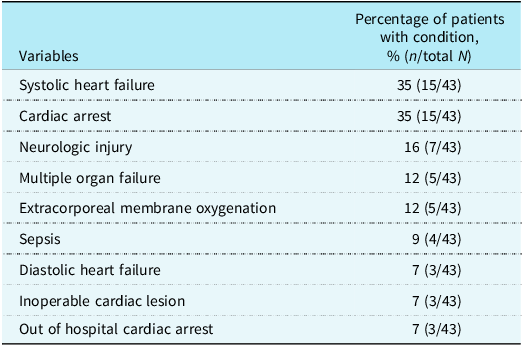
A total of 552 patients who reached superior cavopulmonary anastomosis between 2010 and 2020 were reviewed. After exclusion criteria were applied, the total number of eligible and included patients was 427. The number of excluded patients and reasons for exclusion are provided in Figure 1. Three hundred ninety-six (396) out of 427 included patients (93%) underwent the Fontan procedure or were referred for Fontan before the age of 4 years old (Figure 1). The mean age at the time of Fontan was 4.5 years old. Thirty-one (7%) patients were deemed non-Fontan candidates. Baseline demographics and a breakdown of data between Fontan and non-Fontan candidates are reported in Table 1. In further investigation of the excluded patients, delayed referral (n = 20) was due to practice variation or family preference in all but 3 patients who had medical reasons delaying pre-Fontan testing, those reasons being poor weight gain, multiple infections delaying the pre-Fontan catheterisation, and a stage with a shunt to the left pulmonary artery due to hypoplasia, respectively. The main practice variation was a desire to delay Fontan until a decrease in oxygen saturations, in order to delay the non-cardiac complications of Fontan palliation. There were 43 patients who died prior to pre-Fontan testing with a median age at death of 8.5 months. Table 2 shows the morbidities present in these patients.
Flow diagram detailing the included patients and reasons for non-Fontan candidacy.

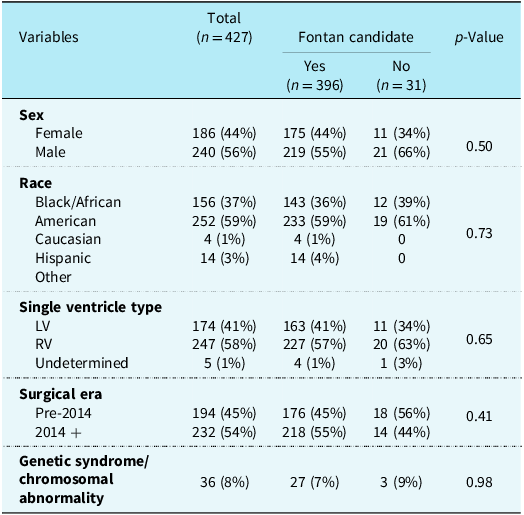
Demographics and patient characteristics of overall cohort stratified by Fontan candidacy

Results depicted in n (percentile), median (interquartile range/IQR).
LV = left ventricle; RV = right ventricle.
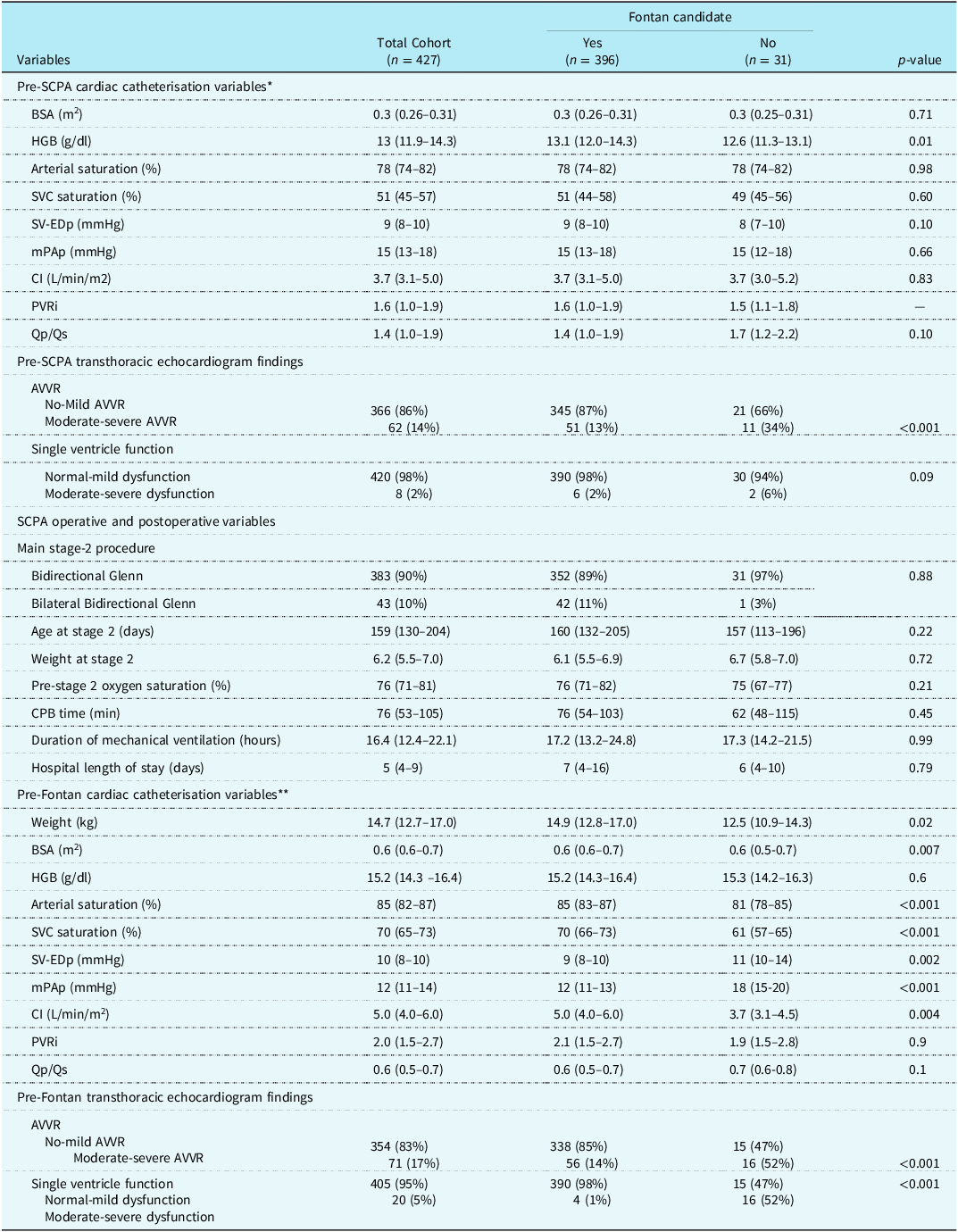
Pre-SCPA and pre-Fontan cardiac catheterisation and echocardiographic variables stratified by Fontan candidacy

BSA = body surface area; HGB = .haemoglobin; SVC = superior vena cava; SV-EDp = single ventricle end-diastolic pressure; mPAP = mean pulmonary artery pressure; CI = cardiac index; PVRi = indexed pulmonary vascular resistance; Qp = pulmonary blood flow; Qs = systemic blood flow; AVVR = atrioventricular valve regurgitation; CPB = cardiopulmonary bypass.
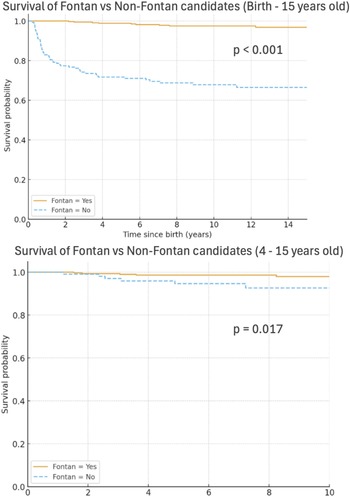
Reasons for non-Fontan candidacy are detailed in Figure 1 and divided into cardiac (n = 26), respiratory (n = 3), and other reasons (n = 2). A majority of patients who were not candidates for cardiac reasons had systolic or diastolic ventricular dysfunction as the primary reason for non-candidacy (n = 15), with fewer having atrioventricular valve regurgitation or stenosis (n = 8) or pulmonary vein stenosis (n = 3) (Figure 1). Those with atrioventricular valve regurgitation who were deemed non-candidates had either concurrent ventricular dysfunction or a prior attempt at surgical repair of the valve, and repeat valve intervention was not thought to be beneficial. Respiratory aetiologies included pneumonectomy and obstructive sleep apnoea. One patient had a right pneumonectomy and left pulmonary vein stenosis prior to superior cavopulmonary anastomosis and another had a pneumonectomy due to severe unilateral pulmonary vein stenosis after superior cavopulmonary anastomosis. The patients with other reasons for non-candidacy included one patient who was tracheostomy dependent, non-ambulatory, and had abnormal right lung vasculature, and another patient who had complete occlusion of the Kawashima that was not able to be resolved medically or surgically. No patient was deemed a non-Fontan candidate after superior cavopulmonary anastomosis for a genetic syndrome or neurologic issue. The outcomes from each group are detailed in Figure 1. Most patients with cardiac reasons for non-Fontan candidacy went on to transplant (n = 17), but others have had a Fontan at another centre (n = 2), died (n = 3), or remain alive with superior cavopulmonary anastomosis (n = 4). Those with respiratory and the other reasons for non-Fontan candidacy are alive with superior cavopulmonary anastomosis at the time of the study. There were 2 non-Fontan candidates at our centre who went on to undergo Fontan at another centre. The reasons for non-Fontan candidacy in these 2 patients were atrioventricular valve regurgitation (although our centre had planned to do an atrioventricular valve repair before the Fontan, whereas the other centre did both simultaneously) and pulmonary vein stenosis, respectively. Of the patients who were non-Fontan candidates, 17 went on to heart transplant, 2 underwent Fontan at another centre, and 9 are alive with superior cavopulmonary anastomosis. Only 3 non-Fontan candidates have died, all 3 of whom had a transplant or were listed for transplant at the time of death. The mean age of patients who are alive with superior cavopulmonary anastomosis at the time of the study is 11 years old. Survival of Fontan vs non-Fontan candidates is shown in Figure 2. Patients who were non-Fontan candidates had a much higher probability of death overall with a p-value of <0.001. The survival curve from age 4 to 14 is also shown with a statistically significant difference in Fontan and non-Fontan candidates with a p-value of 0.017.
Kaplan-Meier curves demonstrating the survival of Fontan candidates to non-Fontan candidates from birth to 15 years old (top) and from 4 to 15 years old (bottom). Fontan candidates - yellow; Non-Fontan candidates - blue.

Pre-stage 2 haemodynamic and echocardiographic data are displayed in the top portion of Table 3, showing that the only significant variable differing between Fontan and non-Fontan candidates pre-superior cavopulmonary anastomosis was the degree of atrioventricular valve regurgitation, with the non-Fontan group having a higher incidence of moderate or severe atrioventricular valve regurgitation. Odds ratio demonstrates that there are higher odds (3.5) of patients with atrioventricular valve regurgitation pre-stage 2 being non-Fontan candidates eventually, whereas odds ratio does not support that depressed function pre-stage 2 is predictive of non-Fontan candidacy. Otherwise, the haemodynamic data were similar between the two groups.
Comorbidities and causes of death in patients who died prior to pre-Fontan testing

Results are depicted as % (n/Total N); Total N = 43.
Pre-Fontan haemodynamics and echocardiographic data are displayed in the lower portion of Table 3. The non-Fontan candidates were smaller at the time of pre-Fontan catheterisation. They had significantly lower arterial and venous oxygen saturations, higher ventricular end-diastolic pressure, higher mean pulmonary artery pressures, and lower cardiac index. The QpQs and indexed pulmonary vascular resistance were not significantly different between the two groups. On echocardiogram, the non-Fontan patients have a higher incidence of moderate or greater atrioventricular valve regurgitation and moderate or greater ventricular dysfunction, which is also supported by odds ratios displayed in the table.
Discussion
Fontan attrition, or failure to complete Fontan after superior cavopulmonary anastomosis, has been reported to be approximately 8–13% at other institutions in different single-centre studies. Reference Lawrence, Ittenbach and Hunt3,Reference Stack, Schluger and Roberts4,Reference Carlo, Carberry and Heinle5 Of the 427 included patients who underwent stage 2 palliation at our institution, 31 patients (7%) were not Fontan candidates. The largest reason for non-Fontan candidacy was cardiac reasons (26/31, 84%), including atrioventricular valve regurgitation and ventricular dysfunction, with a smaller subset of patients having respiratory (3/31, 10%) or other reasons (2/31, 6.5%). The only significant finding on pre-stage 2 echocardiogram and cardiac catheterisation data was an increased incidence of moderate or severe atrioventricular valve regurgitation and moderate or severe ventricular dysfunction in the non-Fontan group. As expected, those who were not Fontan candidates did have significant differences in Fontan cardiac catheterisation data with increased ventricular end-diastolic pressure, pulmonary artery pressure, and decreased cardiac index. Unfortunately, other than the echocardiographic findings mentioned, there was no significant finding prior to stage 2 that could help determine the likelihood of candidacy at pre-Fontan testing. However, despite not being candidates for Fontan, a significant number of patients went on to transplant or have survived with superior cavopulmonary anastomosis physiology at the time of the study. Interestingly, although many of the patients who died prior to pre-Fontan testing had systolic or diastolic dysfunction, it was not the majority of patients, further demonstrating the lack of ability to predict non-Fontan candidacy at the time of superior cavopulmonary anastomosis.
In prior single-centre studies, the absolute attrition rates reported may vary based on the exclusion criteria applied to that study. In a 30-year report by Lawrence et al., there is an attrition rate of 8.3% when excluding patients who died prior to hospital discharge after superior cavopulmonary anastomosis, were awaiting Fontan and deemed a candidate at their institution at the time of the study, were lost to follow-up, or underwent two-ventricle repair. Reference Lawrence, Ittenbach and Hunt3 With the inherent variability in mind, our study excluded similar patients to the study published by Lawrence et al. Some literature has shown that there is a considerable increased risk of attrition attributable to medical complexity or need for procedures and additional surgeries between the superior cavopulmonary anastomosis and Fontan. Reference Ravishankar, Gerstenberger and Sleeper13 Surrogates for complexity in these studies included length of stay at the time of stage 2, longer cardiopulmonary bypass times at stage 2, and additional surgery needs such as atrioventricular valve repair at the time of superior cavopulmonary anastomosis. A study by Stack et al. demonstrated that with combined atrioventricular valve regurgitation and ventricular dysfunction, there is 20 times higher odds of Fontan attrition. Reference Stack, Schluger and Roberts4 Similarly, we found a significant difference in incidence of atrioventricular valve regurgitation between the Fontan and non-Fontan groups, both on pre-stage 2 and pre-Fontan testing. We did not find other differences between the Fontan and non-Fontan candidate groups from the standpoint of the aforementioned surrogates for medical complexity.
Cardiac reasons for non-Fontan candidacy in our group included atrioventricular valve regurgitation, ventricular dysfunction, and pulmonary vein stenosis. Interestingly, there were not haemodynamic factors pre-stage 2 that were associated with ultimate non-Fontan candidacy, possibly due to the patients with significant differences not undergoing superior cavopulmonary anastomosis and thus being excluded from this analysis. Pulmonary vein stenosis and total anomalous pulmonary venous connections have historically difficult outcomes in single ventricle patients. A study from Geoffrion et al. investigating single ventricle with total anomalous pulmonary venous connection patients from 1984 to 2021 showed 54% survival to 10 years old in the era from 2008 to 2021 that has not significantly improved from the era from 1993 to 2007. Reference Geoffrion, Aronowitz and Mangeot14 Another study from Sugano et al. showed 5-year survival at 58% and freedom from re-stenosis at 54%, with some patients going on to Fontan completion. Reference Sugano, Murata and Ide15 Three patients in our cohort were non-Fontan candidates due to pulmonary vein stenosis, and one did go on to get a Fontan at another centre. This patient population has a high risk for failure of single ventricle palliation, but based on the literature, each patient must be weighed on a case-by-case basis with the knowledge that re-stenosis of pulmonary veins may lead to non-Fontan candidacy. Although the number of patients with pulmonary vein stenosis is small in our study, the two who did not have Fontan are alive, as is the patient who went to another centre for Fontan.
In our study, patients deemed non-candidates for respiratory reasons all survived with superior cavopulmonary anastomosis at the time of this study with an average age of 11 years old. There are considerable haemodynamic changes that can result from respiratory conditions, which may lead to failed Fontan physiology despite favourable haemodynamics with the superior cavopulmonary anastomosis at the time of pre-Fontan testing, but there are not outcomes specifically for patients with pre-existing respiratory conditions undergoing Fontan, likely due to small sample sizes.
Although there are patients who were deemed non-Fontan candidates at both our centre and when presented to other centres for second opinions, some of these patients remain alive with superior cavopulmonary anastomosis at the time of the study. This begs the question: would there have been an opportunity to complete Fontan palliation at some point, or would the patient have had a worse outcome if proceeding with Fontan with their physiology? Is the option of having superior cavopulmonary anastomosis as the last stage of palliation an acceptable alternative and destination? This cannot be known from this type of study but would be an interesting avenue for future research. This study also adds to the literature by demonstrating that non-candidacy for Fontan may lead to other avenues, as there may be many years that a patient can live with their superior cavopulmonary anastomosis physiology, giving a later opportunity for Fontan completion or transplantation if haemodynamics or medical conditions become more favourable. This is supported by a recent study by Miyake et al. following 36 patients with superior cavopulmonary anastomosis without progression to Fontan. The 20-year survival was approximately 50% in their group, with 40-year survival being approximately 40%. Reference Miyake, Sakamoto, Kondo, Iwakura, Doi and Tamura16 Knowledge of this type of data may help in counselling families and patients who are non-Fontan candidates.
Limitations of this study include those limitations common to all retrospective studies. In addition, the exclusion criteria pose a challenge due to variability in exclusion criteria amongst similar studies, leading to difficulty comparing the attrition rates. We attempted to exclude similar groups of patients as other studies. Excluding patients deceased prior to Fontan evaluation may be excluding a subset of patients who would have been non-Fontan candidates due to failed superior cavopulmonary anastomosis physiology, but the main reason for this was to determine non-candidacy in survivors of superior cavopulmonary anastomosis. Additionally, not finding differences in pre-stage 2 catheterisation data may be due to the exclusion of those who did not undergo superior cavopulmonary anastomosis or died between stage 2 and Fontan testing. Unfortunately, there was not pre-Fontan cardiac catheterisation data for every non-Fontan candidate for a variety of reasons, including family preference to avoid invasive testing when the patient was unlikely to be a candidate based on echocardiographic findings. Given the small number of patients who are non-Fontan candidates and the heterogeneity of the group, we are unable to adequately complete a multivariate analysis to compare risk factors or predictors for non-Fontan candidates. Finally, non-Fontan candidacy is determined by provider consensus rather than protocol, which introduces inherent variability in candidacy criteria. Due to the changes in staff at the institution in any given year, this is not something that can be standardised in a retrospective study.
Conclusions
We describe reasons for non-Fontan candidacy and the outcomes of patients who do not undergo Fontan at our institution with an overall attrition rate of 7%. Those who are non-Fontan candidates have a higher incidence of moderate or severe atrioventricular valve regurgitation or ventricular dysfunction. Prior to Fontan, cardiac catheterisation data demonstrates lower cardiac index, higher mean pulmonary artery pressures, and higher ventricular end-diastolic pressure. Earlier in single ventricle palliation, prior to the stage 2 operation, it remains difficult to predict those who will not be candidates for Fontan, but the outcomes of non-Fontan candidates can be considered when counselling patients who are not candidates.
Competing interests
All authors have no financial relationships or competing interests to disclose.


 Open access
Open access