

Introduction
A recent comparative work-psychology-based study of UK health professionals’ fitness to practise revealed two important results. (Reference Searle, Rice, McConnell and Dawson1) First, despite differences in the relative numbers of registrants, there were striking similarities between the misconducts of doctors, nurses, and allied health professionals. Second, despite divergence in registrant numbers, one type of malpractice – sexual misconduct – emerges more frequently from male doctors relative to other professionals. Indeed, no cases were found among women doctors, nor amongst midwives. Findings confirm earlier studies with incidents being more frequent in specialties including obstetrics and gynaecology, psychiatry and family medicine. In this chapter I draw on social cognitive theory (Reference Bandura2; Reference Bandura3) to consider three inter-related factors (behavioural, person, and the environment) and then review research evidence of how they contribute to the creation and sustainment of sexual violence for this profession. Through this approach, distinct personal, social and environmental influences are identified that would enable better detection, amelioration and prevention of sexual misconduct in medicine. I start by arguing that this form of misconduct is distinct, especially in the health context and specifically this profession. I use the term ‘sexual misconduct’ to underline behaviours that are at odds with what is expected of professionals, and I deliberately use the terms ‘targets’ and ‘perpetrators’ to discuss these incidents, thereby aiming to shift attention away from victimhood and its notions of passivity and helplessness. I note that there is as yet no satisfactory term to refer to those who are on the receiving end of these actions.
Sexual Misconduct Matters to Some Professions More Than Others
Research into counterproductive work behaviours (e.g. Reference Robinson and Bennett4–Reference Spector, Fox, Penney, Bruursema, Goh and Kessler5) has distinguished different forms of transgression. Critically, taxonomies separate interpersonally focused deviance from that which is directed at the organization, for example sexual harassment versus expenses fraud. The former is a far more severe transgression, because it violates social norms. (Reference Robinson and Bennett4) Sexual misconduct can be considered one of the most transgressive, interpersonally directed forms of counterproductive work behaviour due to its explicit, immoral, sexually aggressive content. (e.g. Reference Bowes-Sperry, Tata, Luthar, Sagie, Stashevsky and Koslowsky6–Reference Pina and Gannon10) It endures as one of the most pervasive forms of interpersonal violence against women. (Reference Fitzgerald11)
Sexual misconduct by a professional is a significant concern – in health and social care it can be a violation not only of professional standards but also of significant organizational requirements, endangering patients and service-users, with consequences for the wellbeing of other employees. (Reference Searle and Rice12) As I outline, sexualized contexts can be a symptom of a stressful workplace, with such relationships a means to access resources. They create distinct workplace dynamics between staff members that blur important boundaries between work and personal lives. More widely, such behaviours can damage public trust in employing institutions and regulators.
Until recently, sexual misconduct incidents have been viewed in isolation. However, following prolific sexual abuse cases, including those connected to the Catholic Church and to the UK’s prolific serial abuser Jimmy Savile, who used his status to access people in hospitals and the BBC, more insidious concerns have arisen: these abuses occurred in a health context, and show the exploitation of organizational weaknesses by perpetrators for their own nefarious ends. (Reference Bandura13) Further, the wilful obscuring of events by institutions betrays those who have been targeted. (Reference Heffernan14) The #MeToo movement has galvanized targets to come forward and share their experiences. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) The scale of these reports renders obsolete the simple scapegoating of individuals; instead, it raises more pressing and uncomfortable questions about complex social environments and their roles in enabling and facilitating such incidents. Extending the perspective from a straightforward perpetrator–target dyad clarifies the adverse consequences for witnesses and others. (Reference Cesario16) Instead, it draws attention to the various social networks and complex environments that are critical in the creation, perpetuation, and even exacerbation of sexual violence by virtue of developing, sharing, accepting, and acquiescing to deviant values, norms, and behavioural models. (Reference Bandura13)
In the context of the medical profession, this misconduct can be regarded as far more significant and therefore likely to have more important consequences for targets. First, doctors are exhorted on entering the profession (e.g. the Hippocratic Oath) to behave with humanity and compassion. It is also enshrined in codes of conduct (17). Sexual misconduct inflicts harm on others, (Reference O’Leary-Kelly and Bowes-Sperry18) and therefore stands in direct opposition to the expected behaviour of a professional. Second, the role of physician elevates the individual’s social status, (Reference Bandura13) making that person a powerful authority figure in most societies. As it is non-consensual, sexual misconduct is a far more profound violation of trust, argued to be akin in form and impact to a parent’s abuse of a child. (Reference Galletly19) Finally, through perceptions about the training they have received, doctors have elevated presumptive trust: patients and the public assume those in this role are trustworthy. (Reference Kramer20) Indeed, prior idealized notions of professions have helped obscure their misconduct, making others reluctant to believe the claims of targets. (Reference Clements, Dawson and das Nair21)
Given the high status of perpetrators, and the trust that is placed in them, their targets’ initial responses and capacity to raise concerns are likely to challenge the status quo. A typical response to sexual assault is shame (Reference Bhuptani, Messman-Moore, O’Donohue and Schewe22) Targets also experience short-term freezing and withdrawal coping responses, which can be misinterpreted by perpetrators as acquiescence, thus prolonging the abuse. (Reference Fitzgerald, Drasgow, Hulin, Gelfand and Magley23) Targets’ responses can further compound their sense of shame (Reference Smirles24) and feeling that they are somehow responsible, with recent #MeToo cases exposing the fallacy of enduring rape myths regarding targets’ silence. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) Yet these erroneous views persist, and are accepted more by men, (Reference Diehl, Rees and Bohner25) especially those with similar sexual aggressive behaviours. (Reference Diehl, Glaser and Bohner26) Where the target is a trainee, silence arises from fear of significant detrimental career consequences if they complain. (Reference Stone, Phillips and Douglas27) Indeed, a common tactic of perpetrators is to discredit the target with powerful others to whom the target has less access. (Reference Scott and Martin28) Therefore, a high-status perpetrator, such as a male physician, can benefit from the significant skew to their power relative to their target. We will now consider the three co-related factors of social cognitive theory. (Reference Bandura2)
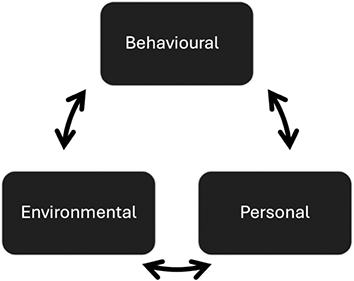
Key co-determinants of transgressive behaviours.

Behavioural Factors
Sexual misconduct includes ‘unwelcome sexual advances, requests for sexual favours, and other verbal or physical conduct of a sexual nature’. When directed at co-workers it ‘unreasonably interferes with an individual’s work performance, or creates an intimidating, hostile, or offensive work environment’. (Reference Pina, Gannon and Saunders29) Further, as such misconduct includes non-consensual and coercive behaviour, it can be covert, with perpetrators deliberately secretive in their actions, leading to diverging accounts between the parties and no means of independent verification. (Reference McDonald30) The opacity of these events and the lack of independent verification can make those informed be reluctant to take further action. (Reference Bandura13)
Sexual misconduct can be separated, distinguishing aggressive from sexualised actions, (Reference Larsen, Nye and Fitzgerald31) with the former more typical in gender harassment (i.e. unwanted conduct related to an individual’s sex or the sex of another person, rather than unwanted conduct of a sexual nature), (Reference Larsen, Nye and Fitzgerald31; Reference O’Leary-Kelly, M, Bowes-Sperry, Bates and Lean8) and is often associated with rejection. (Reference Stockdale, Gruber and Morgan32) Critically, sexual misconduct is a goal-directed behaviour, often occurring concurrently with other forms of interpersonal violence. (Reference O’Leary-Kelly, Paetzold and Griffin33) Extant research suggests three drivers for this response. First, it is a means of dissipating negative affective responses that arise from prior adverse experiences, which perpetuates a cycle of aggression. (Reference Berkowitz34) Adverse experiences are common in the medical profession, with negative emotions elicited from caring for patients, or working in resource-constrained and time-pressed contexts. (Reference Kumar35)
The second driver is retributive, responding to perceived injustices by punishing those deemed responsible. (Reference O’Leary-Kelly, Paetzold and Griffin33) Prior study shows both men and women punish women for being ‘uppity’, meaning they deviated from feminine ideals towards more masculine characteristics including assertiveness, independence, and dominance. (Reference Berdahl36) Similar agression is also shown towards men who deviate from traditional masculine stereotypes. Retaliation against women is more marked in previously male-dominated professions, where they are considered as taking ‘men’s jobs’. (Reference Willness, Steel and Lee37) Such behaviours are deployed to maintain unequal and female-hostile social workplace hierarchies (Reference Page and Pina9; Reference McDonald30; Reference Berdahl38).
Self-presentation is the final motivation, supporting the perpetrator’s desired social image (the ‘big man’), (Reference O’Leary-Kelly, Paetzold and Griffin33) protecting or enhancing a sex-based status. (Reference Berdahl38) This can include more instrumental personal sexual gratification. (Reference Pina, Gannon and Saunders29)
Research shows discernible differences in perpetrators’ various goal choices, highlighting the severity, type, duration, and frequency of incidents and their targets. (Reference Lucero, Allen and Middleton39) For example, some perpetrators focus on a few targets for more persistent abuse, while opportunists are characterized by their wider range of targets and incidents. In contrast, ‘harassers’ denotes repetitive and stable behaviours, which can escalate in severity, becoming more prolific; critically, in these cases sanctions are less effective. (Reference Lucero, Allen and Middleton39)
A study has examined health professionals’ misconduct and identified strong predictive and recidivist patterns to the sexual misconduct behaviour of doctors. (Reference Spittal, Bismark and Studdert40) The research highlights an important and perplexing failure of prior sanctions. Social cognitive theory has also identified four mechanisms that individuals use to allow them to morally disengage from their transgressive activities and still maintain a positive self-image. (Reference Bandura41) Indeed, working in a morally praiseworthy profession can leave doctors more vulnerable to other cognitive distortions, including moral licensing, (Reference Klotz and Bolino42) where these good deeds can provide a moral credit to off-set against their immoral actions. (Reference Griep, Germeys and Kraak43) As a result, medical doctors may be more vulnerable than other professions from falling prey to such perverse cognitions. Research on sexual perpetrators has identified particular use of moral disengagement strategies, including blaming targets for their own deviance, especially amongst those with traditional sex-role beliefs (Reference Jensen and Gutek44) and sexist attitudes. (Reference De Judicibus and McCabe45) Recent study of sexual misconduct that included medical doctors showed greater incidence of these tactics when compared to other health professionals – notably, denying that any incident had occurred or injury had been caused, and implying a dehumanized target was responsible. (Reference Berdahl, Raver and Zedeck46) Further, those in the profession were less likely to try and displace responsibility onto others, probably in recognition of their more senior work roles.
Critically, engaging in this behaviour affects environments, which in turn alters perpetrators’ behaviour. (Reference Bandura13) Prior study has identified important personal and organizational influences regarding these behaviours. (Reference Fitzgerald, Drasgow, Hulin, Gelfand and Magley23)
Personal Factors
Interpersonal factors are important in determining how individuals perceive their environments, and how they behave. (Reference Bandura13) They include biological and intrapsychic influences, such as competencies, belief systems, self-conceptions, emotional states, goals, attitudes, and values.
An important recurring demographic for sexual misconduct is gender, it largely, but not exclusively, being committed by men, typically those with sexist attitudes (Reference Berdahl, Raver and Zedeck46). Disbelief from professionals about female perpetrators, however, contributes to exacerbating its adverse consequences for targets. (Reference Clements, Dawson and das Nair21) Studies show both men and women can target those they perceive as transgressing traditional gendered roles. Targets include senior ‘uppity’ women, and men in previously female-dominated occupations. (Reference Berdahl36, Reference Berdahl38, Reference Kabat-Farr and Cortina47) However, the consequences of sexual misconduct have been argued to be less severe for male targets. (Reference Waldo, Berdahl and Fitzgerald49) Such relative arguments are always problematic as such events have long-lasting impacts. Similar target demographics were found in a recent UK study of health professionals’ sexual misconduct, revealing offending medical doctors to be exclusively male, and more frequent targeting of vulnerable women, critically younger and lower seniority, and also those with mental-health concerns. (Reference Berdahl, Raver and Zedeck47) These targets are in line with Scott and Martin’s (Reference Scott and Martin28) arguments about cynical targeting of naïve and unreliable witnesses.
Research on the nexus of behaviour and personal factors reveals important differences in the interpretation of social interactions, with men more likely to misconstrue women’s behaviour as being ‘more than simply friendly’, regardless of the women’s status or responses. (Reference Johnson, Stockdale and Saal50) Further personal determinants of perpetrators include their sexual attraction to targets, as well as particular personality traits, notably their strong need for control and power. A study shows that men with low levels of agreeableness and high hostile sexism can use sexual violence as retaliation for perceived earlier interactional organizational injustices. (Reference Krings and Facchin51) Similar reactions were found in men with low subjective power and influence who were promoted, exploiting their new status to rectify prior injustices, especially by targeting female co-workers who had thwarted their earlier sexual advances. (Reference O’Donohue, Downs and Yeater52; Reference Williams, Gruenfeld and Guillory53) These retaliatory reactions show the role of prior situational triggers for some men.
Environmental Factors
Environments are important in motivating and regulating transgressive behaviours, (Reference Bandura13) positioning individuals as meshed in socially situated causal structures, rather than as autonomous moral agents.
Critically, sexual misconduct is sustained by being culturally embedded, as shown by pervasive sexist attitudes and beliefs across most societies, (Reference Russell and Oswald55) and their maintenance within institutions. (Reference Fitzgerald11) As a result, targets are predominantly women, particularly those with lower socioeconomic and hierarchical status in a workplace. Women’s economic precarity and lower status can exacerbate their vulnerability to become targets, in that their economic dependence on their jobs reduces their capacity to complain, or to be believed in the face of higher status males (Reference O’Leary-Kelly, M, Bowes-Sperry, Bates and Lean8; Reference McDonald30; Reference Easteal and Judd56).
Bandura (Reference Bandura13) distinguishes three ways in which individuals impact environments. First, in imposed environments, individuals have limited control over the physical and psycho-cultural aspects that impinge on and constrain them. Goffman (Reference Goffman54) has noted how these institutional forces also affect patients and service users. Individuals can vary their understanding of, and responses to, such constraints. Second, selected environments offer individuals far greater latitude, including choice of profession, that offers more fine-grained means to shape working environments, select departments and even shifts, or to access a variety of contexts through locum working. Might this be a factor in explaining why there are different distributions of these behaviours across distinct specialties? The selection of an environment offers professionals greater opportunities and levels of oversight. Finally, as perpetrators gain power they have further means to more nefariously shape places, creating environments, in order to advance their misconduct. Over time, these deliberate behaviours alter the local workplace climate and wider cultures to facilitate their malfeasance. These climates quickly form, with facilities where employees live-in further insulating them from alternative views. Through micro-social-engineering, important and facilitatory social networks can be forged to support evolving deviant activity patterns. The permissive norms that develop are integral to facilitating sexual harassment climates, (Reference Pina and Gannon10) and the resultant environments are central to enabling those with chronic predispositions to harass to act on their proclivities. (Reference Page and Pina57)
Extant study shows more sexual misconduct occurs in workplaces without a corrective influence of professionalism, with limited employee knowledge of complaint procedures, and where there are pervasive sexist attitudes. (Reference O’Hare and O’Donohue58) In workplaces where there is a sex-based hierarchy, sexist attitudes can become entrenched. (Reference Willness, Steel and Lee37) Cultures with high levels of competition and gendered power relations, and where informal networks are significant, can facilitate sexual misconduct. (Reference Hennekam and Bennett59) Reporting of concerns often involves contacting human resources, who have less power and status in health care organization, making it difficult to challenge senior clinicians with high status (e.g. surgeons).
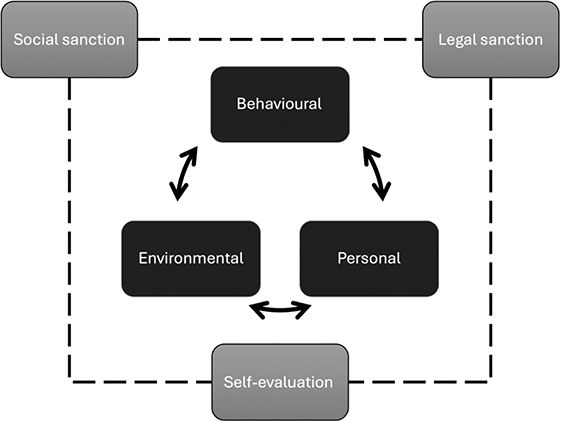
Aside from facilitating misconduct, environments can also be important in inhibiting transgressive behaviours (Reference Bandura13) (see figure 10.2). First, individuals are crucial to self-regulation, restraining actions that violate their own standards of behaviour – even if these activities are unlikely to be noticed by others. Inhibition stems from moral values, motivating individuals to avoid the resultant guilt, remorse, and self-criticism that would arise from a transgressive act. However, working in a profession of ‘good deeds’ can provide moral credits that can off-set immorality. (Reference Griep, Germeys and Kraak43) Self-control is a finite resource which can be eroded by ongoing efforts. (Reference Baumeister, Bratslavsky, Muraven and Tice60) Research indicates higher instances of impulsive sexual behaviour by those with low self-control of overall traits, and where recent events have depleted the strength of their self-control, diminishing their capacity to stifle sexual thoughts and resist temptation. (Reference Gailliot and Baumeister61)
Co-determinants and sanctions that inhibit transgressive behaviours.
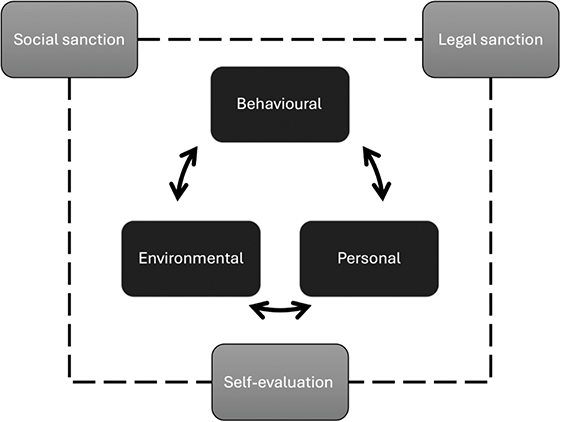
Individuals’ self-regulatory capability can be undermined by environmental factors, critically by stress associated with either their roles or managing uncertainty. (Reference Fox, Spector and Miles62) However, studies reveal men’s capacity to inhibit transgressive tendencies is more affected by stress than women’s ability to do likewise. (Reference Spector and Zhou63) This capacity is also affected by emotions, with a nurse-based study of less serious deviant conduct showing how anger- or anxiety-inducing events caused a temporary moral disengagement. (Reference Fida, Paciello, Tramontano, Fontaine, Barbaranelli and Farnese64) The study found such events ‘compromise’ workers’ capacity to be aware of others, and their adverse responses diminished their means to self-sanction. Strikingly, one response to stressful workplaces can be to seek protection from a more senior person, which proliferates more sexualized climates. (Reference Berdahl and Aquino65) In these workplaces, boundaries between individuals can become confused, making them less safe places for patients as well. A second and distinct source of inhibition is formal regulator sanctions, (Reference Bandura13) externally imposed by regulation of health professions and national legislation. Workplaces also have their own specific formal policies and practices.
Notably, in the context of this form of misconduct, inhibitory capability appears eroded. First, despite being illegal within most societies, sexual violence is growing at least in part due to low reporting and conviction levels. (Reference Fitzgerald11) Second, detailed comparative study of UK health professionals’ sexual misconduct shows doctors are less likely to be permanently suspended, even where there are repeated incidents. (Reference Berdahl, Raver and Zedeck47) This may lead some within this profession to perceive that serious sanctions are less likely. Reducing the fear of perceived sanction reduces their effectiveness, and may be a factor contributing to the recidivism found for sexual misconduct. (Reference Spittal, Bismark and Studdert40) Finally, different professions working in the same contexts are regulated applying different standards and sanctions to their actions, with serious case reviews raising concerns about the divergence of processes and resultant sanctions. (Reference Hodson66; Reference Peng and Zeng67) However, sanction ambiguity for sexual perpetrators can lead them to downplay the risk to them of sanctions, using a variety of moral disengagement mechanisms to distance themselves from their actions. (Reference Berdahl, Raver and Zedeck47) Bandura (Reference Bandura13) contends that ambiguity, coupled with a lack of societal engagement in tackling this form of interpersonal violence, reduced the inhibitory impact of sanctions.
Finally, social sanction is also fear-based. (Reference Bandura13) However, perpetrators can choose workplaces with enabling, rather than inhibiting, social networks. (Reference Bandura13) Prior study of sexual misconduct reveals how social sanctions can be subtly undermined, through pervasive sexist work attitudes, the erosion of professionalism, and curtailing knowledge of the complaint procedures. (Reference O’Hare and O’Donohue58) Male perpetrators of sexual violence often garner sympathy rather than censorship. (Reference Bagenal and Baxter68) The cultural embedding of sexist attitudes within societies restricts the impact of social sanctions. Further, research shows the efficacy of social norms varies; critically for this profession, fear of being socially ostracized is more acute for those with lower self-efficacy, (Reference Peng and Zeng69) and sanctions are rarely directed at those with high job performance. (Reference Quade, Greenbaum and Petrenko70) Therefore, elites who are delivering are not impacted, especially those regarded as doing important work. (Reference Bagenal and Baxter68) More lenient standards are also applied to those who are regarded as being otherwise morally praiseworthy, rather than understanding that these positive actions provide the psychological means for them to appease their immorality. (Reference Griep, Germeys and Kraak43)
Through the more insidious efforts of perpetrators to select and create environments, social objections can be undermined. For example, the fostering of uncertainty about what constitutes sexual misconduct can make bystanders reluctant to intervene. (Reference Bennett, Banyard and Garnhart71) Although they might feel some responsibility to support and protect vulnerable others, (Reference Hershcovis, Neville, Reich, Christie, Cortina and Shan72) their lack of confidence about formal reporting procedures (Reference Hershcovis, Parker and Reich73) and cynicism about their organization’s tackling of sexual harassment, along with unethical local climates, combine to suppress reporting. (Reference Cheung, Goldberg, King and Magley74) In contrast, training that helps to establish clear boundaries between acceptable and deviant conduct can make bystanders more certain about how to act. (Reference Searle, Rice, McConnell and Dawson1; Reference Lee, Hanson and Cheung75)
By selecting and micro-social-engineering choices about where and with whom to take breaks or extra-curricular activities, important divergent group norms are formed, (Reference Pina and Gannon10) and perpetrators can strategically diminish the level of social sanctions they might receive. (Reference Scott and Martin28) Yet research shows how incidents reported by colleagues are among those receiving the highest sanctions. (Reference Spittal, Studdert, Paterson and Bismark75)
Leaders are critical as powerful role models to others, with their actions enhancing others’ agency to respond to and challenge incivility. (Reference Hershcovis, Neville, Reich, Christie, Cortina and Shan72) Medical doctors are often stalwarts of their communities, especially if they are more conservative rural locations, leaving individuals reluctant to raise suspicions. (Reference Spittal, Bismark and Studdert40; Reference Spittal, Bismark and Studdert76) However, leaders can also undermine social sanctions through the use of moral disengagement to reframe and diminish others’ transgressions. (Reference Dang, Umphress and Mitchell78) Indeed, in stressful workplaces sexualized environments often emerge, with senior staff (majority male) exploiting the ‘protection’ they offer lower-level employers though the use of favours and rewards. (Reference Berdahl and Aquino65) Through establishing more sexualized climates, awareness and concerns about apparently consensual sexual behaviour of co-workers become blurred, making colleagues reluctant to intervene or challenge. (Reference Aquino, Sheppard, Watkins, O’Reilly and Smith79) A further, innocuous veneer can be added to these antics by using humour to deflect attention away from the deleterious work and wellbeing consequences of sexual misconduct; (Reference Berdahl and Aquino65) in addition, others’ moral disengagement is facilitated by removing the actions’ moral dimensions in order to reconstruct them as benign. (Reference Page, Pina and Giner-Sorolla80) Or doing so through moral credits that allows perpetrators to be positioned as morally praiseworthy. (Reference Griep, Germeys and Kraak43) Norms inform ethical behavioural choices and comprise both macro (national culture) and micro (peer) influences. (Reference Westerman, Beekun, Stedham and Yamamura81) They extend to include norms that tacitly support, facilitating misconduct by their silence. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) Paradoxically, instead of reducing local workplace deviance, fear of social sanctions is used against those who are not involved. (Reference Jahanzeb and Fatima82) In these ways perpetrators mould contexts that facilitate their proclivities, encouraging others to think they can do likewise, and further stifling the voices of those with concerns. (Reference Hershcovis, Vranjes, Berdahl and Cortina15)
Examining specific evidence regarding sexual harassment in a health context confirms that despite the establishment of oaths and professionals’ ethical training, these workplaces continue to report incidents of misconduct. (Reference Locke and Hicks83–Reference Nielsen, Kjær, Aldrich, Madsen, Friborg, Rugulies and Folker85) Further, study of medical specialties indicates some critical professions with raised levels of misconduct, specifically family medicine, obstetrics/gynaecology, and psychiatry. (Reference Sansone and Sansone86) Similar professions were indicated in a UK study, pointing to workplace hotspots, including: hospitals; GP surgeries and other private consulting spaces; and those with vulnerable service-users such as care homes, mental-health providers, and institutions for young people. (Reference Searle, Rice, McConnell and Dawson1) Further attention is required to understand why it is more pervasive in particular professions, whether this attracts distinct types of individuals, and the working context. Research profiling risks has identified elevation among doctors working in rural workplaces. (Reference Spittal, Bismark and Studdert76) Co-workers in these locations might have more pervasive traditional sexist attitudes, (Reference Berdahl38) combined with greater reverence for doctors that provides perpetrators with secluded consulting rooms, unchallenged opportunities to undertake intimate examinations, and access to vulnerable patients in communities that can be shamed into silence.
There is a more pervasive cultural embedding of sexual misconduct, with females working in health targeted not only by male professionals, (Reference Berdahl, Raver and Zedeck47) but also by patients. (Reference Phillips and Schneider87; Reference Gabay and Shafran Tikva88) The consequences of these harmful experiences can be exacerbated by line managers who fail to recognize and treat the incidents as serious staff assaults, adding further stress, which can culminate in professionals’ decisions to quit. Responses, including keeping a list of perpetrators who should not be sent female trainees, actively contribute to a culture of abuse, with 91% of women doctors in a recent survey reporting experiencing sexism, yet only 48% feeling it could be reported. (Reference Bagenal and Baxter68)
A study that has matched sexual misconduct events in health care to their wider workplace climate reveals these environments are likely to erode self-regulation resources, through pervasive incivility and violence. (Reference Searle, Rice, McConnell and Dawson1) There are clear associations between these incidents and workplaces with long working hours (self-regulation), high levels of interpersonal violence from both staff and service-users, and poor quality of communication between staff and management. In contrast, workplaces with lower incidents of misconduct had taken steps to clarify boundaries and procedures through high levels of diversity and inclusion training.
There is growing evidence of the relevance of a socio-cognitive framing of professionals’ misconduct, with an Australian comparative health professions study creating predictive risk scores by combining personal details (sex, age), behaviours (number of prior complaints and cause for complaint), and selected environment (profession and specialty). (Reference Spittal, Bismark and Studdert40) Critically, it showed risk profiles for doctors and dentists were highly predictive, identifying troubling repeating behavioural patterns, including for sexual misconduct. These suggest areas where sanctions might be less effective. However, a meta-analytic criminal justice study of sexual harassers highlights that those at greatest risk are the least likely to complete treatment programmes. (Reference Olver, Stockdale and Wormith89) In synthesizing these studies, important personal and environmental facets are revealed which could be used to both screen out individuals from some or all medical careers, and to enhance efforts upstream to identify potential hotspots and ensure all staff are clear about sexual misconduct behaviours and how to report their concerns. While this patently remains a widespread societal issue, #MeToo scandals have raised awareness of the social and institutional factors that are implicit in these incidents. This chapter argues this misconduct is both conceptually and empirically more likely to be undertaken by male doctors. Given the marked recidivist trajectories for this transgressive behaviour, rather than reduced sanctions, educators, regulators and employers should establish higher standards to protect their female workforce and patients, especially in delivering family medicine, as well as mental and female health services. Greater attention should be paid to how workplaces may deplete individuals’ capability to self-regulate, recognising that the content of the work, the associated emotions, and working in resource-depleted organisations can adversely affect individuals’ behaviours. Since social and workplace factors can transform proclivities into misconduct, we need a multi-strand approach to seriously tackle these incidents.

 Open access
Open access