


Competitive advantage
Mental health research in the UK differs from that in most other countries in that a substantial proportion of the academics involved are clinically qualified. The rationale for this model is that researchers with psychiatric experience will be more aware of research issues that are a clinical priority, and ideally placed to translate new findings into better mental healthcare. The main research funding bodies in the UK (Wellcome Trust, Medical Research Council, National Institute for Health and Care Research (NIHR)) support clinical research fellowships that are specifically designed for junior and senior clinical academics. In addition, there is a national training scheme for clinical academics, the NIHR Integrated Academic Training (IAT) programme, comprising Academic Clinical Fellow (ACF) posts at the start of psychiatric training, and Clinical Lecturer posts at the Specialist Trainee level. ACF posts allocate 25% of the postholder’s time to research (with the remainder being clinical), whereas for Clinical Lecturer posts, the research:clinical split is 50:50. Finally, there is parity of pay between clinical academics and clinicians, which ensures that academic psychiatrists are paid at the same rate as their National Health Service (NHS) colleagues.
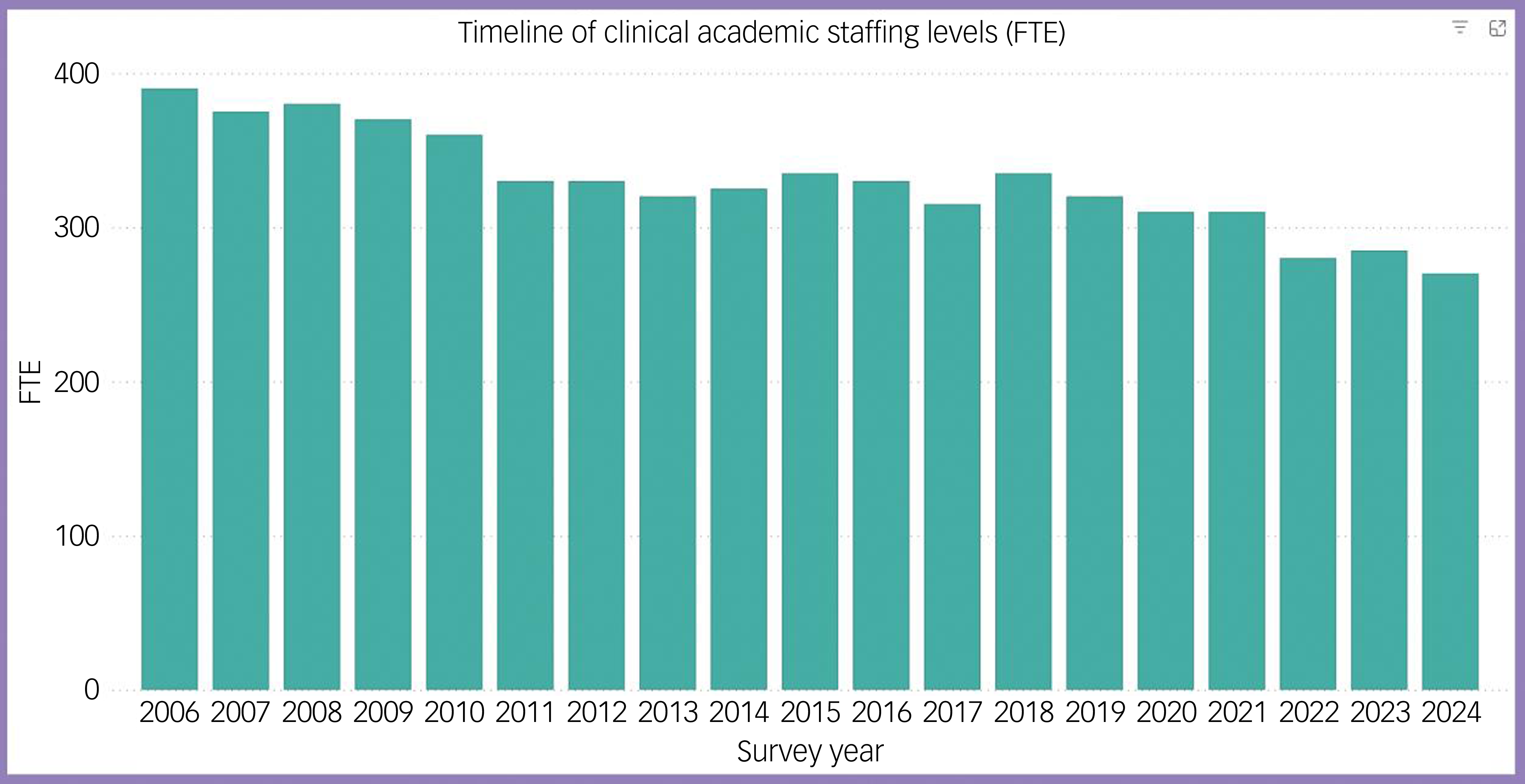
This strategic support for clinical academics has allowed the UK to punch well above its research weight internationally: it has the highest average number of citations per paper worldwide, and is second only to the USA in total number of publications. Reference Zhang, Chen, Gao, Yang, Zhen and Li1 Over the past two decades, academic psychiatrists in the UK have been critical to the clinical translation of advances in mental health research, such as the development and implementation of early detection and intervention services, the identification of candidate biomarkers for more personalised care and the development of new classes of treatment. Reference Coutts, Koutsouleris and McGuire2 However, over the same period, the total number of clinical academic psychiatrists in the UK has progressively declined. In 2006, this corresponded to a total of 390 full-time equivalent roles, but it had fallen to 270 in 2024, a reduction of 31% (Fig. 1). In contrast, in most other medical specialties, the number over the same period has remained relatively stable. 3
Total number of all academic psychiatrists (Professors, Readers, Senior Lecturers, Lecturers and Clinical Researchers) in the UK (full-time equivalents (FTEs)), 2006–2024. Chart generated using data from the Medical Schools Council. 3

One factor that may have contributed to this decline is a reduction in number of people being trained as academic psychiatrists. Medical students typically find the theory of psychiatry interesting, but clinical practice is not as clearly based on the mechanisms underlying health disorders, as in other branches of medicine. Reference Craddock, Antebi, Attenburrow, Bailey, Carson and Cowen4 Students with a strong academic potential may therefore be more attracted to careers in other disciplines. Although some medical schools have made intercalated degrees mandatory, the overall number of students taking a basic science degree may be decreasing, 5 which could reduce the likelihood of them pursuing a clinical academic career. The introduction of preference informed allocation has prevented students with an interest in research from choosing specialised foundation programmes that offer academic opportunities, and prevented foundation schools from selecting applicants with the potential for a clinical academic career. Reference Barratt, Sharp, Dhillo and Pugh6
Although the IAT programme is a great asset, the number of ACF and Academic Clinical Lecturer (ACL) posts it supports is limited, resulting in some trainees with strong research potential being unable to join the clinical academic pathway. If they then enter the clinical pathway, they will usually have little opportunity for research experience. Although they can take up a research post outside a clinical training scheme, time spent in these posts is unlikely to be accredited as part of their training. Academically inclined trainees may thus feel that if they are unable to join IAT, a clinical academic career is no longer possible.
Despite the IAT pathway being designed for trainees with an interest in research, a recent survey found that only about half of ACFs and ACLs were confident that they would pursue a clinical academic career on completion of training. Reference Oakley, West and Jones7 They expressed concerns about the competing demands of clinical and research work, and the quality of the academic training and supervision. In addition, there is a paucity of funding available for trainees to complete a PhD, and most trainees are unable to pay the fees themselves.
Before the UK left the European Union (Brexit), substantial numbers of talented trainee psychiatrists moved to the UK, attracted by a clinical academic infrastructure that is largely absent from the rest of Europe. Post-Brexit, psychiatrists from the European Union require a visa to work in the UK, their training is no longer recognised as equivalent and the number of psychiatrists moving to the UK has dwindled.
Ideally, when trainees complete clinical academic training, they would be able to apply for a senior academic psychiatry post. However, the number of Senior Lecturer, Reader and Professor posts has also declined, with a 35% reduction in since 2006. The extent to which the loss of these posts reflects reductions in university or NHS funding, or both, is unclear. However, the need to address this issue was highlighted 5 years ago in a Royal College of Psychiatrists report, which called for a 50% increase in senior academic psychiatry positions. 8 National coordination of the funding for these posts, and incentives for local universities or NHS Trusts to support them, would be helpful.
In a some psychiatric subspecialities, the decline in the clinical academic workforce has now reached a critical level. For instance, in many UK centres, there are no opportunities for aspiring clinical academics who want to specialise in addictions, intellectual disability or forensic psychiatry.
Reversing the decline
A first step in addressing the decline in academic psychiatry numbers would be to substantially increase the number of ACF and ACL posts that are funded nationally. In addition, it would be sensible to match the distribution of these posts to the capacity of sites to provide high-quality academic training, and the likely number of strong clinical academic applicants. At a local level, if the number of good applicants exceeds the number of nationally funded posts, additional positions can be created, as long as the academic component can be funded by the university rather than NIHR, and there is a local training number available for the applicant.
Once they have started training in academic psychiatry, it is critical that as many trainees as possible progress along the clinical academic career pathway. This can be facilitated by ensuring that they have access to a wide range of research experiences, and that there is a high standard of academic supervision and support. In addition, some regions have introduced bespoke leadership programmes to prepare academic psychiatry trainees for the later transition to senior roles.
Some psychiatric trainees want to join the clinical academic pathway, but are unable to find a post. Others develop an academic interest after starting on a clinical training programme. At a national level, it would be useful to establish a system that facilitates the subsequent migration of such trainees to the academic pathway, so that the possibility of an academic psychiatry career is not precluded by starting on the clinical pathway. At a local level, research posts can be included as part of a clinical training scheme, so that trainees can gain meaningful academic experience without having to leave the programme. These can be supported by the local university if Deanery funding is not available. Over the past two decades, it has become increasingly difficult for consultant psychiatrists in the NHS to engage in academic activity. Reference Critchley, Tracy, Malhi, Alexander, Baldwin and Cavanagh9 However, some mental health Trusts have been open to modifying consultant job plans so that these include protected academic sessions. This can allow consultants with an academic interest to make a significant contribution to research or teaching. It can also make the posts more attractive, facilitating recruitment of good-quality applicants.
Clinical academics play a key role in all areas of medicine, but are especially important in psychiatry, where there is a particular need for new types of assessment and treatment. Academic psychiatrists are the researchers who are best placed to drive translational research. However, if their numbers continue to decline, it will be harder to deliver improvements in mental healthcare.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Author contributions
P.M., K.S. and B.R.L. contributed to conception of the article, its drafting and critical review, and final approval of the version to be published. They agree to be accountable for all aspects of its content.
Funding
This editorial received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
P.M. and B.R.L. are members of the British Journal of Psychiatry Editorial Board, but played no role in the review process for this article. K.S. has no competing interests to declare.

eLetters
No eLetters have been published for this article.