


Introduction
Cognitive behavioural therapy (CBT) is a well-established and evidence-based psychological treatment that is widely recommended as an adaptable and effective intervention across a range of mental health conditions (MHCs), with a substantial and solid body of evidence (Fordham et al., Reference Fordham, Sugavanam, Edwards, Stallard, Howard, Nair, Copsey, Lee, Howick, Hemming and Lamb2021; Kazantzis et al., Reference Kazantzis, Luong, Usatoff, Impala, Yew and Hofmann2018). Although CBT has proven its effectiveness for various MHCs both globally (Avsar and Sevim, Reference Avsar and Sevim2022; Falahat et al., Reference Falahat, Baradarn Eftekhari, Dejman, Forouzan, Mahmoodi, Padyab and Tavassoli2022; Hiltunen et al., Reference Hiltunen, Kocys and Perrin-Wallqvist2013; Oud et al., Reference Oud, De Winter, Vermeulen-Smit, Bodden, Nauta, Stone and Stikkelbroek2019; Salartash et al., Reference Salartash, Yekta and Zabihi2022; Sanabria-Mazo et al., Reference Sanabria-Mazo, Colomer-Carbonell, Fernández-Vázquez, Noboa-Rocamora, Cardona-Ros, McCracken, Montes-Pérez, Castaño-Asins, Edo, Borràs, Sanz, Feliu-Soler and Luciano2023), as well as in South Africa (Mhlungu, Reference Mhlungu2018; Nozizwe, Reference Nozizwe2024), it remains under-utilised in practice in South Africa (Young, Reference Young2009). Research on CBT interventions has demonstrated improved clinical outcomes for patients (Cuijpers et al., Reference Cuijpers, Harrer, Miguel, Ciharova, Papola, Basic, Botella, Cristea, de Ponti, Donker, Driessen, Franco, Gómez-Gómez, Hamblen, Jiménez-Orenga, Karyotaki, Keshen, Linardon, Motrico, Matbouriahi and Furukawa2025). Furthermore, CBT is identified as a flexible therapeutic modality in terms of number of sessions required and transferability across settings (Falahat et al., Reference Falahat, Baradarn Eftekhari, Dejman, Forouzan, Mahmoodi, Padyab and Tavassoli2022). In addition to the clinical effectiveness of CBT, research has demonstrated the broader applicability of CBT principles in early intervention and prevention programmes (Birur et al., Reference Birur, Moore and Davis2017; Caldwell et al., Reference Caldwell, Davies, Thorn, Palmer, Caro, Hetrick, Gunnell, Anwer, López-López, French, Kidger, Dawson, Churchill, Thomas, Campbell and Welton2021).
CBT development in South Africa
In their 2013 call-to-action paper, Pillay et al. (Reference Pillay, Ahmed and Bawa2013) called for a fundamental reorientation of clinical psychology training in South Africa towards equity, cultural relevance, and community responsiveness. The authors advocated aligning the curricula with primary healthcare principles and indigenous epistemologies to address systemic inequities in mental health provision. Despite lauding CBT as an adaptable intervention and applicable to diverse contexts, CBT remained under-utilised in South Africa (Edwards et al., Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012). At the time, research indicated only 20% of clinical psychologists had received training in CBT and only 6% used CBT as their primary therapeutic approach and could be identified as CBT practitioners (Möller and van Tonder, 1999 in Edwards et al., Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012). Möller and van Tonder (Reference Moller and van Tonder1999), Young (Reference Young2009) and Edwards et al. (Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012) all made the same call – to grow CBT in South Africa and advocate for more training opportunities (Edwards et al., Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012; Young, Reference Young2009) as well as a national society to promote broader implementation of CBT (Edwards et al., Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012). However, psychodynamic approaches dominated in postgraduate training programmes (Edwards et al., Reference Edwards, Rossouw, Drake, Young, Naeem and Kingdon2012), despite evidence of the efficacy, adaptability, and suitably of CBT for a culturally diverse and under-resourced healthcare system like in South Africa (Young, Reference Young2009). In 2019, the CBT association of South Africa (CBTASA) was finally established, aimed at promoting CBT in SA and broader Africa for mental health care (CBTASA, n.d.). The association has a growing membership and is affiliated to the European Association of Behavioral and Cognitive Therapies (EABCT). In 2024, CBTASA hosted an inaugural CBT congress, the first in Africa. While the establishment of CBTASA is a promising step to promote the use of CBT in South Africa, it does not guarantee its uptake among trainees and practising professionals. As such, research is needed to understand CBT training experiences in South Africa and how these shape perceptions of confidence and competence and decisions about future use.
Clinical psychology training in South Africa
The training of clinical psychologists in South Africa includes one to two years at a Higher Education institution (known as Masters year 1 or M1 for short), followed by a 12-month internship at a healthcare facility linked to the National Department of Health (M2), and a 12-month community service placement (Pillay et al., Reference Pillay, Ahmed and Bawa2013). Community service placements are facilitated between the National Department of Health and the National Department of Correctional Services. During this training period, students provide psychological services to patients and are required to be proficient in various therapeutic modalities (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022). In South Africa, the structure and content of the Master of Clinical Psychology programme varies across universities. While the training programmes vary, there are specific guidelines provided by the Health Professions Council of South Africa (HPCSA) that each programme that must adhere to, such as including training on psychological interventions (Health Professions Council of South Africa, 2024). However, the guidelines allow universities autonomy to decide which intervention modalities they offer. Psychodynamic psychotherapy and CBT are two of the most common modalities included in training programmes across South African universities. Historically, staff involved in clinical psychology training programmes have expressed scepticism toward evidence-based practice and instead opted to offer a range of modalities during training to ensure critical engagement in the discipline, and to ensure consideration for cultural and linguistic diversity in South Africa (Kagee and Lund, Reference Kagee and Lund2012). In their study exploring psychology training directors’ views on the extent to which evidence-based practice is emphasised in clinical and counselling psychology training in South Africa, Kagee and Lund (Reference Kagee and Lund2012) recommended developing standardised accreditation criteria for all training programmes. To date, no such standardised accreditation criteria are available.
CBT training structure in South Africa
In South Africa, training in CBT forms part of clinical psychology programmes (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022). As such, there is limited exposure to CBT during undergraduate and honours programmes where only brief theoretical engagement is offered. Students selected for the clinical psychology programmes are typically trained in CBT during their M1 year at most Higher Education institutions in SA. However, as mentioned, the training varies across institutions with some institutions providing fewer training hours (for example 19 versus 70 hours) (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022). At Stellenbosch University (SU), students are trained in both psychodynamic psychotherapy and CBT. Student clinical psychologists receive approximately 70 hours of CBT training which includes a combination of seminars, student presentations, individual and group supervision, as well as self-study components. These 70 hours thus cover CBT theory and the practical application of CBT techniques. Of these 70 hours, 20 hours are dedicated to group supervision for clinical cases and student clinical psychologists each have access to individual clinical supervision for input on case work throughout the year. Students are typically required to assess patients’ suitability for therapy after the initial clinical assessment. They are also expected to determine the modality to be used (CBT or Psychodynamic Psychotherapy) depending on the assessment findings and diagnosis. Use of CBT with patients varies among the students as this depends on the psychological presentation of the patient and the modality selected for psychotherapy. On average, students at SU deliver CBT to one of their five to six patients they treat during their M1 year. Patients can expect to receive between 12 and 20+ sessions of CBT. Some of the key adaptations clinical students need to make when using CBT include explaining therapeutic concepts, adapting language to South African English, and working flexibly to accommodate patients’ circumstances (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022). Environmental factors and structural barriers (such as transport difficulties and financial constraints) often disrupt attendance and continuity of care (Burger and Christian, Reference Burger and Christian2020). Additional adaptations are sometimes required when working with trauma for example (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022) where trauma is a continuous experience (Kaminer et al., Reference Kaminer, Eagle and Crawford-Browne2018).
Evaluating competence in CBT training
Competence in CBT may be defined and assessed in various ways (Newman, Reference Newman2010). Despite the diverse definitions and assessments there are core aspects of competence in CBT that cut across different training programmes and include a sound theoretical knowledge, an ability to conceptualise using the CBT model, and skilful use of CBT intervention techniques (Muse et al., Reference Muse, Kennerley and McManus2022; Bergvall et al., Reference Bergvall, Ghaderi, Andersson, Lundgren, Andersson and Bohman2023; Beutler et al.,Reference Beutler, Crago, Arizmendi, Garfield and Bergin1986; Padesky, Reference Padesky and Salkovskis1996; Shaw and Dobson, Reference Shaw and Dobson1988).
In the context of MA Clinical Psychology professional training programmes like ours, competence has not been objectively measured using a rating scale. Instead, competence is typically assessed through submitted assignments that are graded by training staff who are experts in CBT and in group and individual supervision.
Objectively, competence in CBT is often measured using the Cognitive Therapy Rating Scale-Revised (CTRS-R) (Beck Institute for Cognitive Behaviour Therapy, 2022; Blackburn et al., Reference Blackburn, James, Milne, Reichelt, Garland, Baker, Standart and Claydon2001) which is a revised version of the original rating scale developed by Young and Beck (Reference Young and Beck1980). This rating scale is based on an adapted version of the Dreyfus five-stage model of skills acquisition (Dreyfus and Dreyfus, Reference Dreyfus and Dreyfus1980). The Dreyfus model is a learning progression framework for skill acquisition and explains how skills are learned across five stages from the novice to the expert. While various objective rating measures of CBT competence exist, these measures do not adequately capture perceived self-competence, which entails students’ own perceptions and beliefs in their ability to deliver CBT competently (Muse and McManus, Reference Muse and McManus2013; Rapley and Loades, Reference Rapley and Loades2019). Andersen et al. (Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022) have argued that CBT is well positioned to address the mental health treatment gap in SA. However, CBT can only be effective if therapists are competent and confident in their abilities. Therefore, part of the call from Andersen et al. (Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022) included calling on universities to ensure appropriate training of student psychologists and calling on the HPCSA to provide oversight and ensure adequate CBT competencies, a call that aligns with ethical practice guidelines as set out by the HPCSA (Health Professions Council of South Africa, 2017). Self-competence can be used as a marker for readiness (Andersen et al., Reference Andersen, Rossouw, Kagee, Kazantzis, Hofmann and Higgins2022; Hendricks et al., Reference Hendricks, Cartwright and Cowden2021); however, existing literature has demonstrated that discrepancies often exist between supervisor and trainee ratings (Caron et al., Reference Caron, Muggeo, Souer, Pella and Ginsburg2020; Gonsalvez et al., Reference Gonsalvez, Riebel, Nolan, Pohlman and Bartik2023). For example, in their study on supervisor versus self-assessment of trainee competence, Gonsalvez et al. (Reference Gonsalvez, Riebel, Nolan, Pohlman and Bartik2023) found that trainees under-estimated their competence significantly, early on in their training. In contrast, Caron et al. (Reference Caron, Muggeo, Souer, Pella and Ginsburg2020) found an over-estimation of self-rated competence among trainees. There is limited research in SA on self-perceived competence in CBT; however, international findings consistently highlight discrepancies in the assessment of competence (De Wit et al., Reference De Wit, Goldstein, Saurman, Rodriguez and Vickers2024). Understanding student clinical psychologists’ self-competence in CBT delivery may provide important insights into trainee readiness, as well as the barriers and facilitators associated with adopting CBT as a treatment modality in clinical practice.
The role of supervision and reflective practices in CBT training
Existing literature on assessing CBT competence suggests that self-competence may be enhanced through self-reflection (Gale and Shröder, Reference Gale and Schröder2014; Newman, Reference Newman2010). At SU, CBT training is focused on providing the theoretical foundation of CBT, the application of theory, and group supervision for both case discussions and role-plays to practise techniques. CBT training is predominantly delivered in a didactic style, and while both individual and group supervision spaces theoretically provide opportunities for self-reflection, students often perceive these spaces primarily as forums for case management input rather than reflective practice. However, supervision is an integral part of training as the supervisory relationship contributes to the development of supervisee competence and confidence in therapeutic skills. A strong supervisory relationship, one that is characterised by empathy, collaboration and facilitates constructive feedback, can serve as a safe base for supervisees to self-reflect, engage with feedback and enhance their clinical skills (Watkins and Milne, Reference Watkins and Milne2014). More specifically, CBT supervision often mirrors the structure of therapy sessions and creates room to promote self-reflection and critical thinking (Beck Institute for Cognitive Behaviour Therapy, 2022; Sudak et al., Reference Sudak, Codd III, Ludgate, Sokol, Fox, Reiser and Milne2015). Using Socratic dialogue helps supervisees challenge their own assumptions, enhancing clinical decision-making (Haarhoff and Thwaites, Reference Haarhoff and Thwaites2016). Supervisors can thus scaffold experiential learning through CBT techniques such as modelling, role-play and guided discovery (Murr et al., Reference Murr, Nicklas and Harper2020).
Self-perception of CBT competence is an evolving process for trainees, and useful for gauging implementation of CBT. It is shaped by several factors but also personal experiences and preferences (Maruniakova and Rihacek, Reference Maruniakova and Rihacek2018). Additional factors shaping self-perception are learning opportunities, supervision and feedback, increased confidence, and self-practice and self-reflection (Bennett-Levy and Beedie, Reference Bennett-Levy and Beedie2006; Chigwedere et al., Reference Chigwedere, Bennett-Levy, Fitzmaurice and Donohoe2021; Jenkins et al., Reference Jenkins, Waddington, Thomas and Hare2018; Maruniakova and Rihacek, Reference Maruniakova and Rihacek2018). In their randomised controlled trial, Pace et al. (Reference Pace, Song, Suvak, Shields, Monson and Wiltsey Stirman2021) found that while therapist self-efficacy increased over time with experience, it did not predict treatment fidelity, but therapists with low initial self-efficacy benefited significantly from consultation, leading to better patient outcomes. Self-reflection is also a well-known teaching and learning tool to enhance teaching and learning outcomes (Hickson, Reference Hickson2011; Ryan, Reference Ryan2013). Self-reflection, a practice involving observation and interpretation of your own thoughts and actions, allows students to reflect on and evaluate their own practice of CBT (Bennett-Levy et al., Reference Bennett-Levy, Turner, Beaty, Smith, Paterson and Farmer2001). Structured self-reflection and self-experience are essential in CBT training, enhancing therapists’ empathy, confidence, and competence while supporting ethical practice and preventing burnout (Prasko et al., Reference Prasko, Ociskova, Abeltina, Krone, Kantor, Vanek, Slepecky, Minarikova, Mozny, Piliarova and Bite2023).
Concluding summary
Although CBT is a flexible and adaptable therapeutic approach, there is limited empirical research examining how CBT competence is developed and assessed across training programmes within the South African context. International literature suggests that variability in training exposure, supervision and competency evaluation is common. Similar challenges may exist in South Africa, where no national CBT-specific competency framework currently guides training. Against this backdrop, our guiding research question in this study was: how do student clinical psychologists perceive their competence in delivering CBT at the end of their M1 training year, and how do their training experiences shape these perceptions?
Research aim and objectives
The primary aim of this study was to explore how student clinical psychologists perceive their competence in delivering CBT at the end of their first year (M1) of professional training, and how their training experiences may shape these perceptions.
Our objectives were threefold: (1) to explore how student clinical psychologists understand and develop perceived competence in CBT during their first year of training; (2) to identify the factors that shape their perceptions of self-competence in CBT; and (3) to explore how perceived competence influences their intentions to use CBT in future clinical practice.
Method
Research design
To achieve the aim of this study, a qualitative exploratory design was used. The qualitative design provides an opportunity to gain in-depth insights into student clinical psychologists’ perceived self-competence in delivering CBT while also providing a rich narrative of their subjective experiences of their M1 training (Gough and Lyons, Reference Gough and Lyons2016; Moser and Korstjens, Reference Moser and Korstjens2017). Consistent with the constructivist paradigm, understanding students’ perceived self-competence requires attention to the contextual factors that may shape these perceptions, including teaching and assessment methods, experiences of the modality and the broader socio-cultural context (Moser and Korstjens, Reference Moser and Korstjens2017).
Recruitment
We used purposive sampling to recruit student clinical psychologists from the clinical psychology masters programme at SU. R.v.d.P., a psychology doctoral candidate experienced in qualitative research, joined the study as a research assistant to conduct the qualitative interviews with support and guidance from B.C. The decision to appoint R.v.d.P. was to have someone who is experienced in qualitative research but not directly involved in the programme, so as to support participation and minimise power dynamics, given that M.S.Footnote 1 is the convenor of the programme. R.v.d.P. met with the trainee students to invite them to participate in the study. During their meeting, R.v.d.P. presented the aims and objectives of the study and students were invited to participate. Initially six of the eight students expressed interest in participating by emailing R.v.d.P., but ultimately only five students took part in the interview.
Data collection
Data were collected by means of semi-structured interviews. Initially, a second data source was included. Students were given the option of writing a reflexive essay on their two submitted assignments, a written case-conceptualisation, and a written case report accompanied by a video recording of one session with a client. The purpose of the reflexive essay was to collect data on students’ perceived self-competence in delivering CBT. The instruction for the reflection was as follows: (a) reflect on the reason(s) for selecting the submitted session; (b) reflect on their ability to use CBT as demonstrated in the video submission; (c) reflect on their ability to conceptualise and formulate a treatment plan using CBT as demonstrated in the submitted assignments; and finally (d) reflect on areas for improvement regarding their ability to deliver CBT, conceptualise a case, and formulate a treatment plan. All participants opted out of the reflection essay, presumably due to the demands of the clinical programme at the time, and chose to participate in the interview only. The interview schedule was developed based on the literature, as well as the aims and objectives of this study. Five interviews were conducted with an average duration of 56 minutes (range 45–65 minutes). Participants were asked about their perceived self-competence in delivering CBT; any discrepancies between training-related CBT competence assessments and their own perceived self-competence in CBT delivery; the extent to which their perceived self-competence in CBT influences their decision to use CBT in practice; and to identify factors (barriers and facilitators) that may influence self-competence in CBT amongst student clinical psychologists. Given that students opted out of the reflection activity mentioned earlier, we included the following reflexive questions as part of the interview. Firstly, they were asked to reflect on their video assessment submissions as evidence for their demonstrated competence in CBT, by answering (1) what was your reason for selecting this session?; (2) so, what does this tell you about your ability to use CBT in sessions with clients?; and (3) what do you need to improve CBT delivery in future? Secondly, they were asked to reflect on their case report submission. This submission is the main assessment in the CBT course. Students were asked: (1) what was your reason for selecting this case to write up?; (2) what does this tell you about your ability to conceptualise and formulate a treatment plan using CBT?; and (3) what do you need to improve your ability to conceptualise and formulate a treatment plan using CBT? To establish rigour, R.v.d.P. used member checking throughout the interviews by asking clarifying questions to ensure that the interviewer was correctly understanding what the participant was saying (Shenton, Reference Shenton2004).
Data analysis
The interviews were transcribed verbatim by R.v.d.P. and analysed by R.v.d.P. and B.C. using the six-step process of reflexive thematic analysis (RTA) (Braun et al., Reference Braun, Clarke, Hayfield, Terry and Liamputtong2019). A hybrid inductive-deductive approach to coding was conducted by R.v.d.P. and B.C. with the assistance of ATLAS.ti software. An inductive approach to the coding meant codes were generated from the data with no pre-existing coding framework being used. However, we were guided by our aim and objectives and so a hybrid inductive-deductive approach best describes our data coding approach, aligning with RTA. From the codes, themes and sub-themes were constructed and reviewed by R.v.d.P. and B.C. to ensure they accurately reflected the data and addressed the aims and objectives of the study. The themes constructed are presented below with verbatim quotes to illustrate each theme and enhance the credibility of the findings. Pseudonyms have been used to protect participants’ privacy.
Results
Five out of eight invited student clinical psychologists completing their M1 training took part in the study. In order to protect confidentiality, and given the small cohort size, detailed demographic or identifying information about participants is not reported.
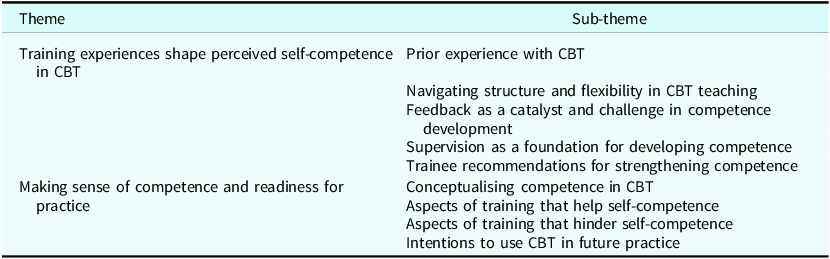
As can be seen from Table 1, we identified two over-arching themes and nine sub-themes that captured participants’ experiences of CBT training in their M1 year, and their understanding and perceptions of their self-competence in CBT and the factors that influenced their self-competence. Only edited if words were exactly alike like this.
Themes and sub-themes

Theme 1: Training experiences shape perceived self-competence in CBT
Participants’ self-competence perceptions were influenced by several factors. Participants reported on (1) CBT training they had received thus far, (2) teaching style and content, and (3) feedback delivery. Furthermore, they provided recommendations towards developing self- competency.
1.1. Prior experience with CBT
All participants stated that their M1 training year was the first time that they had received formal training and practised CBT, either through role-playing or in a therapeutic session with clients. Participants explained that they had a relatively good understanding of what CBT entailed, theoretically. One participant had broadly applied principles of CBT in their previous capacity as counsellors. D2 said:
It was my first formal, sort of intensive training. But when I was doing lay counselling at lifeline, there was often CBT worksheets that would be used, you know, through therapist aid, and that. And [I] obviously learned about the theory very broadly in undergrad and honours, but not, yeah, definitely my first time, actually sitting with it.
Another participant (D4) said:
Like, umm, I’ve been introduced to theory. It was, it was very new. I stressed quite a bit if I’m going to get this right. And I was quite confused also initially. Oh my God this. So yeah, like I said, it was very new. I felt confused. I felt a bit like this is just something really foreign. So yeah, which was quite anxiety provoking also because we had to do, like I did CBT with my very first client and yeah.
1.2. Navigating structure and flexibility in CBT teaching
Participants reported on the teaching style and content of the CBT training in their M1 year. Participants noted a difference in teaching style between the two lecturers and how this difference impacted on their perceptions of CBT and their own competence in delivering CBT.
One participant (D6) said:
I think for me initially, the way it was taught, was that there’s these steps. You know, like someone comes in and you do a mood check, but like when you do a mood check, you say you’re doing a mood check, but in practice that’s not how it necessarily has to come through you know. You can literally, when someone sits, you can just say, hi, how are you? You know, that’s a mood check. So, I think the rigidity just, just in terms of these steps man, it made, the way it was taught, especially the first half, was the steps that you have to do and it has to look this way and you know, but in reality I found that it’s more flexible, but the rigidity puts people off in my opinion.
Participants reported that they had experienced both a rigid and flexible teaching style, which created some confusion around best practice for use with clients in a real-world setting. For example, one participant (D2) explained that the experience of learning CBT and then applying it in practice felt quite unnatural and said:
I mean, if you’re sitting in therapy. It didn’t feel, I don’t know, it just didn’t come naturally to sit and do a worksheet, you know, a thought record. Something like the, the downward arrow technique sometimes, I often felt a bit silly doing it. It felt like, how do I explain it? It felt like, something that I had to actively concentrate on and bring it in and it didn’t always feel like it would naturally flow into, OK, this is a good time to do a thought record.
For this participant and others, the rigidity and inflexibility of CBT felt unnatural and to some extent inappropriate for use with their clients. Instead, these participants explained that a more psychodynamic approach would often be preferred as this approach allows for more rapport building with the client and exploration of the client’s past, which seemed necessary and appropriate to them. Despite the discrepancy in their experience of the teaching styles, participants remarked that overall, the way in which the content was presented was helpful and they especially enjoyed the role-playing. Participants stated that the role-playing, and the practice this afforded them with using CBT skills, supported their perceptions of self- competence.
1.3. Feedback as a catalyst and challenge in competence development
Participants recounted their experiences of the way in which the feedback they received during their training was delivered to them. Again, participants drew attention to the difference in feedback provided by the two lecturers on the module. As can be seen from the first quote, the feedback was tied to perceptions of self-competence. However, the discrepancy in feedback received created doubt about competence. The participant (D6) said:
OK, so every time we get CBT we get feedback, like feedback from all the lecturers. And the general consensus was that, so from the one lecturer it was like, OK, I’m, you know, competent and adequate with CBT. And then the other lecturer, well my supervisor was, yes, I’m adequate, but my case conceptualisation … So I need to work more on that. So she picked that up already mid-year. With CBT that I have to work on. And then the, so that’s the feedback I got and then the report from the assignments.
Participants reported wanting more detailed and consistent feedback, and suggested feedback earlier on in the training year instead of at the end of their training. Participants also reported that clear feedback about specific areas for development in the application of CBT helped them understand what to improve on in future. Participant D2 stated:
In terms of the CBT assignment feedback, I think I could have used a little bit more to be honest. Although I don’t know what more I could want, ’cause it was sort of just, if they were worried, they would tell you what the worries were and if they weren’t [worried], then there wasn’t really much, you know … so that was all fine. Well I just felt relieved if I did OK, that is.
1.4. Supervision as a foundation for developing competence
Participants recounted positive experiences of their CBT group supervision, which is facilitated by two experienced CBT practitioners at the institution. Students also receive individual clinical supervision. However, individual supervisors practise from different therapeutic modalities. Therefore, experiences of additional CBT supervision differed:
You know, those supervision sessions. I feel like I’m, I’m not sure if that forms part of the CBT module. CBT supervision with XXX and XXX. That is, I feel like that is Gold hey. Because you are taking what you are doing in your sessions and you’re taking it back to, I feel like these two experts, and they are just able to guide you and the they are able to not give you a, give you an answer, but to work with you through what you are, or work with you in terms of your thinking and in terms of what you think you need to do and I think that is really gold. [D5]
One participant shared her experience of CBT supervision (both group and individual). This participant recounted a positive experience as her supervisor for both group and individual CBT supervision had expertise in using CBT in practice. The supervision she received contributed to her self-competence perception and enjoyment of the modality:
I think so. I think it impacts my willingness. Because, well then, the question is why do I enjoy it? I think that’s the thing, because I think I enjoy it because I have enough experience of it and I think because of my supervision again, the CBT supervisor, I became more comfortable with it very quickly and you know, I sort of used it in sessions with clients and I saw how useful and helpful it is most of the time. So, I think that’s why I enjoy it and that’s why I think I’m very open to it. [D6]
1.5. Trainee recommendations for strengthening competence
Participants stated several suggestions for improvement to the CBT training. Participants reported that addressing the misperceptions of CBT as a rigid modality would be helpful if done earlier in the module. Furthermore, they recommended more opportunities to demonstrate their skills in case conceptualisations:
And I think that’s the essence to start off CBT like that, not to start off, start it off on a rigid note because I think that really sets the tone for how people perceive it. So I would recommend more flexibility from the beginning, more practical examples of how it manifests, even though there’s these steps. And then more like I said, the case conceptualisation maybe doing like a mock case conceptualisation of a client, even if it’s a psychodynamic client, very early in the training to give people more confidence as well. [D6]
This participant went on to say:
And like I would actually recommend, this is obviously a side note, but I would recommend, in the training, in the beginning of the year. I know we got like a slide with like points of how a case conceptualisation looks like. But I would actually encourage the lectures to maybe, in that training, let us do, let the students do, like formulate or conceptualise someone and bring it to class and actually discuss it. Does that makes sense? Instead of leaving it for an assignment or the, it’s very like delayed, and it also then, I think it helps expose students very early to case conceptualisation.
Two participants stated that they struggled using CBT with clients with personality related challenges and would like to see the training address this specifically. For example:
There was one client I had that I struggled with a lot with CBT. They had avoidant personality trait. And I think that experience of really trying, I felt like I had to work so hard in session. And it was really, really difficult, just very, very difficult, like pulling teeth trying to get somewhere with that. And yeah, maybe then something on CBT with personality disorders could be helpful. We did cover it, but I think the expectation was that we wouldn’t be seeing that many people with personality disorders this year. And I think everyone was surprised to see how many people with personality disorders actually came and presented at the clinic, and then maybe that would have been helpful. But it’s not at all, you know a train smash. I was able to speak to one of the CBT supervisors and get their advice on a book about personality and CBT. It wasn’t at all a train smash, but that could be helpful. [D2]
Theme 2: Making sense of competence and readiness for practice
Perceived self-competence was informed by participants’ ideas of what constitutes a competent CBT therapist. Furthermore, participants reported aspects of the training that facilitated and hindered self-competence, as well as factors that influenced their decisions to use CBT in practice.
2.1. Conceptualising competence in CBT
Following the discussion of their CBT training experience, participants reported their understanding of competence and what a competent CBT therapist looks like. Related to competence, participants described it as having a complete understanding of a certain set of skills and the degree to which one can practise those skills adequately and effectively. As one participant said:
So, when you say competence, what comes up for me is that there’s some kind of a rubric, maybe of the dimensions of the practice. So, there’s different aspects of a practice and so, then I want to assess myself against maybe someone who’s experienced in it and say, am I able to practise this across all these dimensions in a way that’s going to be effective.
Participants also spoke about their definition of self-competence in CBT:
I think that’s somebody who, once again has a very good understanding of the theory, as a base to understand their client, you know, you know, formulate their client, really use those concepts to understand why they are the way they are or why they’re struggling with what they are struggling with. And then to use that framework, work from that framework using evidence-based techniques to be able to, you know, help them help themselves, I suppose. So, for me that’s CBT helping someone get the skills to help themselves. I suppose competence can also be, is it working? Are you being helped? But for me that’s more outcome than actually being competent, I suppose. [D2]
2.2. Aspects of training that help self-competence
Participants recounted various aspects of their training that facilitated a sense of self- competence in CBT. An example of this is the practical application of CBT with a client during the training and on which their assessments (case conceptualisation and video submission) were based. In addition, one participant stated that the knowledge acquired about the structure of CBT provided them with a good basis from which to continue learning. This participant (D6) said:
But I think specifically with CBT you’re going to have to be very mindful of like having the techniques at the back of your head in session, and have that sort of that toolbox, and knowing when to bring it up in session with a client and for that specific client. Does that make sense? So, it’s obviously just being a therapist in general, the core you know, competencies. But I think specifically with CBT, you have to really understand having the toolbox but understand like core beliefs, understand the downward arrow technique. Understand how to use these techniques in session. But like in a, in a relaxing way, you know.
Other participants reported witnessing positive outcomes from the psychotherapeutic sessions with their clients contributing to the self-competence perception. For many of the participants, despite negative feedback they received from their lecturers on their approach to CBT, their interactions with clients and seeing visible improvements enhanced their self-competence.
One participant (D4) said:
Yeah, I’ve seen like a, like there’s been a massive growth in the patient there’s been the anxiety scales, the Beck, the the BI, the BAI. Yeah, the Beck Anxiety Inventory that I’ve administered, there’s been a massive drop from the start of the patient’s journey with me. And this patient has been able to be their own therapist between sessions, and I think. Yeah. The low mark and all. Like the evaluation of me doing CBT that was just, me feeling, that has made me feel really incompetent, but when I, wrote up the case study and when I reflected on all the work that I’ve done with this patient and how she has grown, then it makes me feel somewhat that maybe I can do this.
One of the participants reported that having a supervisor who regularly used CBT in practice had a direct influence on her self-competence. She stated that this supervisor’s experience of delivering CBT in practice facilitated a supervision space that helped challenge the idea that CBT is rigid and inflexible. This encouraged her to engage with the principles of CBT in client sessions even when she was using only basic CBT techniques.
Other aspects that built self-competence included role-plays, client suitability for CBT, and engaging in self-evaluation and self-reflection. In terms of self-reflection specifically, participants shared mixed responses. Some participants found the constant self-reflection exhausting, and others found it helpful to reflect as it facilitated an understanding about their CBT competency. Participants recommended self-reflection to form part of the module more formally in the future:
It’s nice talking to you. And it’s nice to reflect like this, genuinely. Because, yes, I do, I think we all get a little bit sick of reflecting about ourselves. Yeah, and being asked to do so. But what has been helpful about this is, it’s kind of looking at my experience with CBT as a journey, and it’s still going so, that’s really helpful. Because it’s made me think about, I think a little bit beyond my immediate, sort of reaction or indifference to CBT. [D2]
Another participant said:
Umm, I never thought of that before. But, I guess it does. For me, let me talk about me. When I sit and I reflect, I can usually decipher what is happening for me and I think then I can get a clearer picture, of what’s happening. And then I guess to some degree because I have a clearer picture. It would, I won’t, I can’t say like my competence in it in that specific whatever. The more clearer the information becomes for me of what’s happening for me, I think I can understand what is happening better. For me, then maybe it affects my perception of what is happening. Does that make sense? [D6]
2.3. Aspects of training that hinder self-competence
In addition to the aspects that promoted self-competence, participants also spoke about aspects of training that hindered self-competence. One participant reported their perceptions of self-competence were influenced by their passion for CBT. This participant believed that if they enjoyed CBT more, they would perhaps feel more competent in using CBT. The participant said:
Yeah, that’s a good question. I think, maybe because I’m not very passionate about CBT, that I didn’t, there’s, there isn’t that sort of drive to, there’s no excitement to do it. And then that, I think lack of excitement is also related, like you say, to a lack of confidence in it. I think maybe if I was a little bit more confident. A little bit more excitement, but when I’m, when I say I’m, I’m OK. I think I’m average at CBT. And I think that’s also related to my, yeah, like my sort of neutral feeling towards it. [D2]
Participants also spoke about how the feedback they received on their use of CBT impacted their self-competence. One participant said:
The low mark and all. Like the evaluation of me doing CBT that was just, me feeling, that has made me feel really incompetent, but when I wrote up the case study and when I reflected on all the work that I’ve done with this patient and how she has grown, then it makes me feel somewhat that maybe I can do this. [D4]
For another participant, while overall she felt confident and competent to deliver CBT, she recounted that getting to a core belief was challenging and that she needed more guidance and training on what to do when she gets to this point.
Yes, I personally you know when they get to the core belief. I don’t know what to do. Like I know [xxx] speaks about reframing. But [xxx], I don’t know hey, like when I get there like, I was like, what am I gonna do now? Like, so usually I, there are … that’s why I think it’s important to spend time with your client. So you are, you already. So, so yeah, I think it’s when you get to the core belief and challenging the core belief. And I know theoretically it’s about reframing those experiences, but it feels very difficult to do. You know what I mean? So yeah, I don’t know if you want me to give you an example, but it’s yeah. [D6]
2.4. Intentions for future CBT use
Participants reported various reasons that would facilitate their decision to use CBT in the future. Participants stated that they would be motivated to use CBT if their internship sites used this modality, and they could receive more guidance and training in it. One participant said:
Yeah, I do think I’ll be using it going forward. Umm I hope to build my competence and my confidence in using it. I will be using it, particularly because of the settings we’ll be in where, I do like that CBT, for example includes psychoeducation. And I think that will be very useful. Also, with a time limit, you don’t know how long you’re gonna see patients for in the hospital and in that sense, I feel quite confident in delivering and helping with practical, you know, sort of step by step practical stuff that I can maybe help improve somebody else. And I also know that in the hospital, well with the hospital where I’m going, let’s say with the hospital where I’m in the ward with psychosis. And I think that there will be room for that, a lot of room for that. So I will definitely be using it. [D2]
Participants also reported that their enjoyment of the modality motivated them to use CBT. This enjoyment came from their experience with CBT, witnessing client improvement, and receiving adequate supervision:
I think so. I think it impacts my willingness. Because, well then the question is why do I enjoy it? I think that’s the thing, because I think I enjoy it because I have enough experience of it and I think because of my supervision again, the CBT supervisor, I became more comfortable with it very quickly and you know, I sort of used it in sessions with clients and I saw how useful and helpful it is most of the time. So, I think that’s why I enjoy it and that’s why I think I’m very open to it. [D6]
Discussion
Perceived self-competence in CBT delivery
This study explored student clinical psychologists’ perceptions of self-competence in delivering CBT. Findings indicate that perceived competence is shaped by multiple factors, including training structure, teaching styles, supervision quality, and feedback. Initial exposure to CBT during the M1 year often elicited confusion and anxiety, particularly among students with no prior formal CBT training. While some participants found the structured nature of CBT rigid and unnatural, others appreciated its clarity and systematic approach. Practical components such as role-playing and structured supervision were consistently reported to enhance self-efficacy. Supportive supervision and positive client outcomes further contributed to increased self-competence, whereas rigid training formats and challenging client presentations sometimes undermined confidence. These findings align with previous research suggesting that self-perceived competence evolves over time and is influenced by experiential learning and supervisory support (Bennett-Levy and Beedie, Reference Bennett-Levy and Beedie2006; Jenkins et al., Reference Jenkins, Waddington, Thomas and Hare2018; Rakovshik & McManus, Reference Rakovshik and McManus2013). Structured training and continued supervision have also been shown to support the retention of competence post-training (Liness et al., Reference Liness, Beale, Lea, Byrne, Hirsch and Clark2018).
Interestingly, participants noted discrepancies between formal assessments of CBT competence and their own self-perceptions. Several reported initially over-estimating their abilities, only to later experience a mismatch between feedback received and their subjective experience of CBT delivery. This led to feelings of inadequacy and uncertainty. These findings are consistent with prior studies indicating that trainees may either over-estimate (Mathieson et al., Reference Mathieson, Barnfield and Beaumont2009) or under-estimate (Beale et al., Reference Beale, Liness and Hirsch2020) their competence compared with expert ratings. Jenkins et al. (Reference Jenkins, Waddington, Thomas and Hare2018) further suggest that such discrepancies may stem from the complex internal processes involved in developing a theoretical orientation and professional identity within CBT. Emotional states and learning experiences also play a role in shaping self-competence perceptions (Jenkins, Reference Jenkins2017).
Factors shaping perceived self-competence in CBT
Several factors were identified as shaping perceived self-competence. The structure and delivery of CBT training played a pivotal role; rigid formats were associated with reduced confidence, while flexible, principle-based approaches enhanced perceived competence. Feedback from lecturers and supervisors was another key factor, with consistent and constructive feedback contributing positively to self-perceptions. Positive client outcomes also reinforced feelings of competence. The expertise of supervisors was particularly valued, as experienced supervisors were able to contextualise CBT delivery and provide realistic guidance. These findings are supported by Jenkins (Reference Jenkins2017), who emphasises the importance of regular feedback, and Prasko et al. (Reference Prasko, Mozny, Novotny, Slepecky and Vyskocilova2012), highlighting the role of trainer expertise in effective CBT training. Practical components of the course, including role-playing, modelling, and experiential learning, were unanimously viewed as integral to competence development. This is consistent with existing literature underscoring the value of experiential methods in CBT training (Jenkins et al., Reference Jenkins, Waddington, Thomas and Hare2018; Murr et al., Reference Murr, Nicklas and Harper2020; Rakovshik & McManus, Reference Rakovshik and McManus2013).
Influence of perceived competence on CBT use in practice
The study found that perceived self-competence played an important role in students’ willingness to use CBT in future clinical practice. Those with more extensive experience, positive training encounters, and adequate supervision expressed greater confidence and openness to applying CBT professionally. Notably, visible client improvement and supportive supervision were key motivators for continued CBT use. These findings reinforce the importance of supervision in fostering competence and confidence (Guindon et al., Reference Guindon, Myhr and Renaud2022; Jenkins et al., Reference Jenkins, Waddington, Thomas and Hare2018; Murr et al., Reference Murr, Nicklas and Harper2020; Rakovshik et al., Reference Rakovshik, McManus, Vazquez-Montes, Muse and Ougrin2016; Rakovshik & McManus, Reference Rakovshik and McManus2013). Self-reflection also emerged as a critical factor, with participants identifying it as a mechanism for challenging negative assumptions about CBT and enhancing self-insight. This aligns with previous research that self-reflection is essential for developing CBT skills and professional growth (Bennett-Levy and Beedie, Reference Bennett-Levy and Beedie2006; Gale and Shröder, Reference Gale and Schröder2014). Prasko et al. (Reference Prasko, Mozny, Novotny, Slepecky and Vyskocilova2012) similarly highlight the role of reflective practice in improving understanding of CBT methods and promoting personal development.
Additional insights
A notable finding was the perception of CBT as rigid and protocol-driven, particularly among students exposed to highly structured teaching methods. This perception appeared to influence their clinical interactions, with some students opting to switch to a different therapeutic modality, hindering implementation of CBT. This finding is consistent with Ball and Corrie’s (Reference Ball and Corrie2024) study exploring dual modality training where they found that students transitioning from psychodynamic approaches to CBT, perceived CBT as a hindrance to their developing therapeutic skills. The current findings also highlighted student concern around rapport building in a perceived rigid therapeutic space. It would be helpful to explore this further however, as students in this training programme are provided with dual modality training concurrently.
On the other hand, some would prioritise adherence to procedural steps over therapeutic flexibility. Dessert et al. (Reference Dessert, Lynch, McMillon, Terrill and MacNeil2023) caution against this misconception, noting that manualised CBT treatments are designed to be adaptable to individual client needs. CBT, when correctly understood, is inherently client-centred and responsive to diverse presentations. These insights suggest that training programmes should emphasise the principles underpinning CBT rather than rigid protocols and incorporate reflective supervision and experiential learning to support the development of flexible, competent practitioners. Furthermore, training programmes should highlight that CBT can provide benefits like increased flexibility in thinking even when basic techniques are used in isolation (Clark and Egan, Reference Clark and Egan2015). Braun et al. (Reference Braun, Strunk, Sasso and Cooper2015) demonstrated session-by-session depressive symptom reduction with early use of Socratic dialogue, a foundational CBT technique.
Lastly, the findings suggest that students’ own interest and enjoyment of CBT as a modality played a role in motivation to build competence and consequently, their decision to use CBT. One of the key practice points of Roscoe and Wilbraham’s (Reference Roscoe and Wilbraham2024) study titled ‘When it goes well, it works fantastically: motivations to train and their impact on the practice of CBT’, is that motivational factors are implicated in engagement and delivery of CBT.
Implications for CBT training
Students’ reports of perceived self-competence and the factors that influence competency and decisions to utilise CBT in practice can enhance training programmes by identifying areas for improvement. CBT instructors can utilise this information to plan training components and increase activities that build perceived self-competency. An example is including self-reflexive exercises that can focus and address therapists’ negative beliefs about competency. Furthermore, incorporating students’ self-reflections contributes to the development of indigenous knowledge and supports the decolonisation project.
In response to the findings of this study, several enhancements were implemented within the training programme to strengthen pedagogical and experiential learning outcomes. First, additional workshop topics were introduced to deepen theoretical and practical understanding of CBT, including the therapeutic relationship, collaborative empiricism, Socratic dialogue, guided discovery, and an introductory module on cognitive therapy for personality disorders. Second, a benchmark for client exposure was established, requiring students to deliver CBT to a minimum of two clients over at least six sessions each, thereby reinforcing experiential learning and skill consolidation. Third, the Cognitive Therapy Rating Scale-Revised (CTRS-R) was integrated into the programme to provide structured, objective feedback on students’ therapeutic competence, as assessed by two independent supervisors. Finally, Socratic dialogue was explicitly employed within supervision sessions and case discussions to foster reflective practice and to model the technique’s application in clinical contexts, consistent with evidence supporting its role in enhancing metacognitive awareness and therapeutic skill development (Haarhoff and Thwaites, Reference Haarhoff and Thwaites2016; Murr et al., Reference Murr, Nicklas and Harper2020; Sudak et al., Reference Sudak, Codd III, Ludgate, Sokol, Fox, Reiser and Milne2015). Self-reflection forms part of the clinical psychology training programme, whereby students are expected to reflect on all interactions with clients. However, this practice has yet to be incorporated within the CBT training. M.S. continues to think about more adaptations to the training, such as more role-play opportunities and perhaps developing resources for the course, such as training videos.
Conclusion
Participants’ experiences of their CBT training varied and was largely related to the difference in teaching style across the lectures and perceptions of how the theory should be applied in practice – rigidity versus flexibility. Self-competence in CBT is tied to CBT teaching style, supervision, delivery of feedback and client outcomes. Self-reflection plays a role in self-competence and that opportunities for self-reflection (both formal and informal) need to be incorporated into the teaching of CBT.
Limitations
The study included only one cohort of students at one institution. It would be helpful to know what the experience of students are in the broader Western Cape and South Africa. In addition, students came into the masters programme from various undergraduate and honours programmes and had different training and exposure to CBT prior to this training. This difference may have influenced the students’ perceptions of their self-competence. Lastly, the qualitative approach and small sample size could also be considered a limitation; however, the study’s aim was to provide insights into student experiences and not draw any statistical conclusions.
Data availability statement
The data that support the findings of this study are available from the corresponding author (M.S.) upon reasonable request.
Acknowledgements
Microsoft Copilot (V2.20260305.37.0) was used to source relevant literature during the revision process between August 2025 and March 2026. Copilot was used to suggest literature for specific topics or concepts being discussed and how they were relevant. The literature suggested was then manually sourced and verified. ChatGPT (OpenAI, GPT-5.3) was used to assist with minor language editing and improving clarity of sentences during the most recent revision stage, mostly in the background section of the paper. The authors confirm that none of the tools was used to analyse data or interpret any of the findings. The authors declare that they are entirely responsible for the scientific content of the paper and that the paper adheres to the journal’s policy. We would like to thank all of our participants for their contributions to this study.
Author contributions
Mariam Salie: Conceptualization (lead), Data curation (equal), Formal analysis (supporting), Funding acquisition (equal), Investigation (equal), Methodology (lead), Project administration (lead), Resources (lead), Software (equal), Supervision (equal), Validation (equal), Visualization (equal), Writing - original draft (equal), Writing - review & editing (equal); Bronwynè Coetzee: Conceptualization (supporting), Data curation (equal), Formal analysis (equal), Funding acquisition (equal), Investigation (equal), Methodology (supporting), Project administration (supporting), Resources (supporting), Software (equal), Supervision (equal), Validation (equal), Visualization (equal), Writing - original draft (equal), Writing - review & editing (equal); Ryan van der Poll: Data curation (equal), Formal analysis (equal), Investigation (equal), Software (equal), Supervision (equal), Validation (equal), Visualization (equal), Writing - original draft (equal), Writing - review & editing (equal).
Financial support
The authors received funding from Stellenbosch University: FIRLT (Fund for Innovation and Research into Learning and Teaching).
Competing interests
The authors declare none.
Ethical standards
Ethical clearance for this study was received from the Research Ethics Committee (Social, Behavioural and Education Research, ref. 26112). Permission from the Division for Information Governance was also applied for and received (ref. IG-3613). All participants provided written informed consent, and all data have been de-identified and stored on a secure, password protected drive. Microsoft Copilot, V1.25102.233.0, an AI tool, was used in the following ways: (a) sourcing relevant literature (this information was verified before use), and (b) grammar and style editing (Discussion). ChatGPT was used to assist with minor language editing.
Key practice points
-
(1) Trainees found CBT training valuable but initially confusing, with early rigidity in teaching styles contributing to anxiety and uncertainty about competence.Trainees described greater self-competence when teaching and supervision were experienced as flexible and responsive, rather than narrowly focused on rigid, step-based instruction. Trainees valued experienced CBT-trained supervisors as crucial for developing confidence and perceived competence.
-
(2) Consistent, detailed feedback and opportunities for experiential learning (e.g. role-plays, early case conceptualisations) were perceived by trainees as key to support self-competence and motivation for future use.
-
(3) Trainees’ experience of positive client outcomes enhanced their perceived self-competence in CBT delivery.

 Open access
Open access
Comments
No Comments have been published for this article.