


Introduction
Paediatric patients with advanced heart failure require mechanical circulatory support while awaiting transplantation or recovery, when conservative therapy fails. For children up to 30 kg, the Berlin Heart EXCOR® Paediatric, a paracorporeal, pneumatically driven, pulsatile ventricular assist device (VAD), is the most widely used system.
Over 1700 children worldwide have received support with this device, with significantly improved survival rates. Reference Griffiths, Profsky and Mokshagundam1,Reference Rohde, Van and Veen2 Comorbidities such as thromboembolic events have declined due to strict anticoagulation protocols. Reference Griffiths, Profsky and Mokshagundam1,Reference Rohde, Van and Veen2 Neurologic outcomes remain a key concern: studies report clinically significant rates of stroke and other neurologic events, often occurring early in the course of mechanical circulatory support. These findings highlight the need to balance effective anticoagulation with bleeding risk and develop better methods for early and reliable thrombus detection. Reference Jordan, Ichord and Reinhartz3
The EXCOR® Active driving unit, introduced in 2020 for use with the Berlin Heart EXCOR® Paediatric ventricular assist device, extends the mobility of the previously stationary IKUS driving unit. It features in-line flow sensing, prioritised audio-visual alarms, and a 12-hour battery life. 4 The E-Motion Study demonstrated significant improvements in patient mobility and family quality of life with this device. Reference Miera, Sandica and Haas5,Reference Conway, Pidborochynski and Ly6 However, its use remains legally restricted to hospitals. Consequently, children supported by EXCOR® Active often experience prolonged hospitalisation, placing considerable strain on patients and their families. At Deutsches Herzzentrum der Charité, Germany, the Excor Active driving unit has been in use since February 2020. Since then, 49 children have been treated and three software updates became necessary. The children typically stay in the pediatric intensive care unit for three to six days before transfer to intermediate care, where mobilisation is intensified. Early mobilisation follows strict safety protocols, and standard operation procedures regulate responses to pump complications such as thrombus formation. Parents receive tailored ventricular assist device training from engineers, and mobilisation on campus is encouraged, as soon as the medical situation allows.
Drawing upon our extensive clinical experience and the potential of the new BH-EA to facilitate home discharge, we posed the following research questions:
-
a. What are the most significant challenges encountered in the inpatient setting for children with BH-EA?
-
b. What are the most crucial considerations on an individual and cohort level prior to discharging children with a BH-EA?
We conducted semi-structured interviews with healthcare professionals and caregivers of children with BH-EA to explore patient safety, daily care, hospital environment, and requirements for discharge. The aim was to gather diverse perspectives on the challenges of caring for children with BH-EA and to include caregivers’ insights into the lived experience of managing a hospitalised child supported by this device.
Methods
Study design
Between November 2024 and February 2025, we conducted a qualitative study with 25 professionals and caregivers caring for children supported by BH-EA at the Department of Paediatric Cardiology, Deutsches Herzzentrum der Charité, Berlin. Semi-structured interviews explored key aspects of patient safety and daily care, hospital challenges, and requirements for safe home transition with EXCOR Active.
Participants
Participants were selected using purposive sampling to include individuals with different professional backgrounds, roles, and levels of experience (physicians with specialisations in, e.g., paediatric cardiology or intensive care medicine, nursing, social work, psychology, engineering, child education, and religion). Reference Palinkas, Horwitz, Green, Wisdom, Duan and Hoagwood7 Additionally, caregivers of children hospitalised with BH-EA at our centre during the data collection period were recruited through convenience sampling on a voluntary basis.
Data collection
The research team developed a semi-structured interview guide covering two domains: (1) hospital environmental factors, safety, caregiving, and (2) requirements for home transition, including remote patient monitoring (see Supplementary Guideline S1). After pilot testing and refinement, a single researcher conducted all face-to-face interviews for consistency. Interviews were audio-recorded, transcribed, and ranged from 15 to 100 minutes in duration.
Data analysis
The interviews were evaluated using reflexive thematic analysis according to Braun and Clarke. Reference Braun, Clarke, Braun and Clarke8,Reference Byrne9 The analysis began with familiarisation through repeated transcript readings and analytical notes. Between April and July 2025, inductive coding was performed using MAXQDA software (version 24). To ensure consistency and minimise bias, the first interview was double-coded by another researcher, and discrepancies were discussed. Codes were clustered into main- and subthemes, which were reviewed against all transcripts. Two interdisciplinary meetings refined interpretation and validated findings using Braun and Clarke’s checklist for good thematic analysis. Reference Braun, Clarke, Braun and Clarke8
Data presentation
We followed the standards for reporting qualitative research Reference Brien, Harris, Beckman, Reed and Cook10 and provided the Consolidated Criteria for Reporting Qualitative Research Checklist in the Supplementary Checklist S2. Reference Tong, Sainsbury and Craig11
Main- and subthemes were clearly presented, analysed semantically, and summarised. Quotes were used to illustrate the content. Selected quotes, translated from German to English, illustrate the findings.
Results
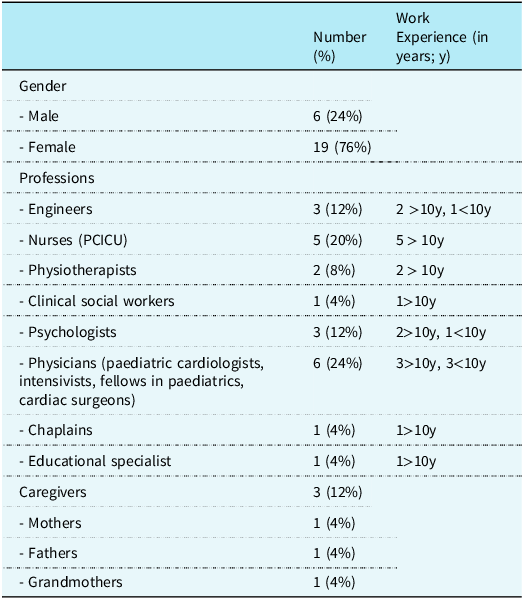
We interviewed 22 professionals from nine disciplines and three caregivers from two families of hospitalised infants supported by BH ventricular assist device at the time of interview (Table 1).
Interview participant characteristics

PCICU = Pediatric cardiac intensive care unit.
Reflexive thematic analysis identified three main themes: “alarms” (technical considerations, emergencies), “hospital stay” (routines, emotions, wishes, space, care), and “requirements for home discharge of paediatric VAD patients.” This paper focuses on “alarms” and “home discharge requirements,” while “hospital stay” will be reported separately.
Alarms
The theme Alarms, based solely on professional input, included five subthemes (Figure 1): (1) types and characteristics of alarms, (2) views on alarm management, (3) alarm fatigue, and wishes and expectations regarding alarm management in inpatient (4), and outpatient (5) settings.
Figure 1 shows the theme “Alarms,” which emerged during interviews with clinicians. It can be divided into five further subthemes.

Types of alarms
A prominent finding was that the most common BH-EA alarms—specifically “pressure loss” or “flow too low”—usually result from low circulating volume or a kinked cannula, mainly occurring during movement or at night. Participants also noted that the second most common alarm is the flow sensor alarm, typically caused by the flow sensor overheating. Several professionals indicated that “driving unit alarms occur rarely,” especially with the new EXCOR® Active driving unit.
One participant explained that alarm limits cannot be set below certain minimum thresholds, which means that patients with small pump sizes may experience more frequent alarm sounds. Another professional stated that the alarm signals are programmed differently to help staff and caregivers to distinguish between high- and low-priority alarms.
Management of alarms
Professionals emphasised that every alarm must be investigated until its cause has been identified and that meaningful interpretation requires a comprehensive analysis, including inspection of the pump-membrane, vital signs, and assessing the child’s overall condition. In a clinical context, this process can be completed swiftly. However, one participant pointed out that it becomes more challenging when an expert is momentarily unable to see the child in the hospital:
The bigger problem is when, for example, there are these low-flow alarms, really finding out what the cause is when you’re not standing next to the patient yourself and, for example, have ECG monitoring and can observe the pump function in parallel.
Furthermore, it was noted that only a few alarms require immediate complex intervention (e.g., drive fault alarms), while others often do not require immediate action and can be resolved through simple measures, such as adjusting the bed cover (e.g., flow sensor alarms). Nevertheless, one participant emphasised the importance of parental vigilance, noting that while most caregivers judge situations well, this ability varies among families.
Alarm fatigue and learned behaviour
Interviewed professionals noted that certain alarms, especially those occurring frequently and not requiring immediate action, are perceived as annoying and are disregarded in practice.
So you have to tolerate these flow alarms to a certain extent; there’s no other option.
We don’t need to take immediate action on this flow sensor issue, because the flow sensor itself only provides a control value and does not interfere with the function of the drive. So it’s really just annoying.
One professional observed that frequent alarms teach families to silence them immediately, behaviour another professional identified as a potential safety risk.
I think that’s a bit of a danger, though, that you just keep silencing the alarm again and again and again and again. Because you think, well, nothing happened the last 200 times.
Wishes and expectations regarding alarm management in hospitalised children
One participant expressed a wish for shared alarm management between physicians and technicians, along with automatic data transfer from the device to the digital patient file, and standardised alarm procedures with clear notification chains.
Wishes and expectations regarding alarm management in outpatients
Furthermore, professionals noted that caregivers must feel confident in interpreting alarms and knowing when and how to seek assistance. Clear emergency contact pathways and home telemetry could reduce miscommunication.
And I think what’s really important is that parents (…) also recognize when they need support.
Requirements for home discharge of paediatric ventricular assist device patients
Interviews identified four subthemes for home discharge criteria: (1) necessity of an emergency hotline and immediate support options, (2) requirements for remote patient monitoring and lack of thrombus prediction tools, (3) training needs for the broader healthcare system, (4) training for families and support networks.
Emergency hotline for caregivers
Professionals emphasised the need for a 24/7 emergency hotline for caregivers of patients with BH-EA at home. Participants expressed various ideas about what an emergency hotline could entail. Some proposed two different hotlines: one for emergencies (112) and another for non-urgent concerns handled by the paediatric cardiology team at the hospital.
I think it would be important to have a hotline where parents could reach the doctor on call in the intensive care unit at any time if there were any concerns, meaning, around the clock.
Another interviewee suggested separate hospital lines: one for asking technical questions directed to the device expert/engineer, and another for medical questions addressed to the medical staff.
And then they can call the hotline, which is located here at the hospital. So they call the cardiac technicians and get advice on what to do. Whether they can ignore the alarm, whether they should call the emergency medical team. Or whether they should go to the clinic, to the outpatient clinic.
In addition to advising parents on appropriate action, some professionals suggested that the on-duty doctor should act as a coordinator and contact the emergency medical services if necessary. If alerted by an emergency call, the emergency medical service or telephone dispatcher should also call the clinic’s team of experts for guidance on how to proceed in uncertain situations. One professional suggested storing patient telephone numbers with specific codes to flag medical risks.
It was also noted that caregivers need thorough training to know when to call each hotline.
What kind of warning signs should I look out for, what signals should I pay attention to, and when should alarm bells start ringing in my head, telling me to dial my emergency number? This is something that requires very sensitive training.
Remote patient monitoring
Remote patient monitoring should allow the device to transmit data directly to the clinic and trigger a noticeable alarm. This would enable the paediatric cardiology team to initiate contact with the families at home.
One participant stressed that only high-priority alarms should be forwarded and highlighted that implementing this system could be challenging.
Yes, in the case of such high-priority alarms, an active notification should of course be sent to the clinic or the device coordinator. This may be a little difficult to implement in such a way that it works reliably.
One participant said that excluding thromboembolic events is complex and noted a knowledge gap regarding the significance of certain complications. This is important to consider when discharging patients with BH-EA, since thromboembolic complications within the first year of life are one of the greatest risk factors for this patient population.
So, especially when children are young, in their first year of life, they have this thromboembolic complication as the main risk factor. So we have to address this in our remote patient monitoring. And that’s what matters.
Training of the broader healthcare system
Many participants recognised the need for appropriate emergency training in paediatric life support across the healthcare system. However, it remained unclear who constitutes this system. The following parties were mentioned: police, physicians from ambulatory care settings, nursing staff, fire brigade, and emergency medical services.
But that also involves a huge amount of effort, logistical effort. That means the fire department, 112, which also involve a lot of people. And they have to be trained.
Training of caregivers and support network
Many statements were made by professionals and one caregiver regarding the requirements for families with children on BH–EA in a home setting related to emergency training. Figure 2 illustrates the complexity of what respondents believe caregivers should know and be able to implement in practice. When developing caregiver training, both their needs and skills must be assessed individually and repeatedly. Participants suggested that caregivers should not only be listened to attentively before discharge, but also evaluated to determine whether discharge is the appropriate course of action for them.
Figure 2 shows the requirements that clinicians and caregivers of children with support from a BH-EA had in mind. It can be divided into four different areas, with the area of caregiver training having a particularly large number of subthemes.

And then the parents’ needs must be clearly understood and addressed in advance. How much do they want to take on, how much do they dare to do, how much support do they need?
One professional said that the caregivers’ sense of security when managing the device is crucial, by ensuring they know how to respond to various situations, so they do not live in constant fear.
Otherwise, I think it’s really about security when using the device and what to do if this or that happens, who to call, etc. So, I think the most important thing is to have an emergency plan so that you don’t have to live in constant fear.
It was frequently mentioned that caregivers should be provided with an emergency plan, outlining recommendations for various potential scenarios. This plan should include a feedback loop to inform caregivers whether their actions were effective and what further steps should be taken.
Additionally, participants deemed paediatric life support training to be important, with differing opinions on whether it should be mandatory or offered at the request of the caregiver.
But at least: Resuscitation-training, that’s also quite important for understanding how they can react.
So, proper CPR training for parents: definitely something you can do if they want it.
One family member stressed the importance of caregivers knowing what they can do in an emergency if their partner is absent. This individual also highlighted the necessity for caregivers to be trained in clinical observation of their child, enabling them to recognise warning signs early and to provide first aid.
Because even if you have telemonitoring at home, you might say, okay, if my child’s lips turn blue, that might be a sign of something. Even if the device might show something good for a moment, you still say, okay, I’ll keep an eye on that.
Another participant noted:
So, the clinical perspective—actually, we need to train them for the clinical perspective—that they have a close bond with their child and can see when the child is a little different.
Beyond immediate emergency management, many skills usually performed by nursing staff or cardiac technicians in the hospital must be mastered by caregivers in the case of outpatient care. These include INR management, medication management, checking the ventricular assist device system for thrombi or damage, and retrospectively evaluating the performance of the device.
One professional noted that thrombus formation is difficult to predict and is often associated with uncertainty, even in an inpatient setting, underscoring the need for assessment by an interdisciplinary team.
But we are also sometimes unsure and think, okay, is this necessary? And then, as a nurse, when I say, okay, I’m not so sure, no matter how much experience I have here, I bring in one of the doctors. Sometimes doctors themselves bring in a surgeon or a device team to see what it is and how to proceed.
Professionals stated that the families’ social networks should be prepared for emergencies. They suggested that training should be recorded as videos or podcasts to be made available to both caregivers and their network.
Several professionals voiced ideas on structure and content of caregiver training. The training could be delivered by representatives from the ventricular assist device system, the cardiology team, and the nursing team. It should be multidisciplinary, follow a standardised structure, document acquired knowledge, and consist of several short sessions over a number of days, or one longer session on a designated training day.
In addition to the diverse requirements for caregiver training, one participant mentioned the need for emotional support throughout the entire period outside the hospital.
… so that you still provide them with emotional support and prepare them again and again for emergencies, should they arise.
Discussion
We conducted semi-structured interviews with the multidisciplinary inpatient team and caregivers of children supported by BH-EA to characterise needs, priorities, and challenges in hospital care and requirements for home discharge.
Evidence for discharging children on BH-EA remains limited to small, off-label single-centre reports. Reference Rottermann, Dittrich and Dewald12
Clear criteria for discharge readiness would have to be developed and verified. Reference Elias, Tunuguntla and Smyth13 Home use lacks legal approval in many countries. Moreover, in many organ allocation systems, such as Eurotransplant, in-hospital status grants higher priority for transplantation making home discharge potentially disadvantageous, as organ waiting times might become longer without an in-hospital status. This contributes to caregiver concern about home discharge. Reference Crowe, Simpson, Reinhardt and Rankin14 In the UK, stable outpatients with intracorporal continuous-flow devices are reclassified from the urgent to the routine transplant list.
Alarms
Participants reported considerable challenges in alarm management. Alarms occur frequently, often requiring clinical interpretation, while many are non-actionable, leading to alarm fatigue among staff and families. Clear responsibility, automatic data transfer, and improved alarm systems are needed. Patient management would benefit from automatic transfer of device data into the electronic health record. To our knowledge, our study is the first to present a detailed user experience of alarm management. Frequent false alarms increase the risk for alarm fatigue, a finding that is also supported by Drew et al. In this prospective adult ICU study, 89 % of annotated alarms were false positive. Reference Drew, Harris and Zègre-Hemsey15 In an interview study of adult ventricular assist device patients, 56 % criticised alarm noises, and 25 % could not distinguish alarm types by sound. Reference Geidl, Zrunek and Deckert16
Similarly, among caregivers of children with type 1 diabetes, 25 % reported alarm fatigue and 40 % expressed fear of insulin pump alarms. Reference Kaylor and Morrow17
Overall, our findings indicate that caregivers and healthcare professionals of children with BH-EA are at risk of alarm fatigue, posing a significant patient safety concern. From our perspective, these risks must be carefully addressed before discharge on ventricular assist device support can be considered a broadly applicable option. This may ultimately include a critical review and, where appropriate, modification of certain alarm settings, but only within a controlled clinical and research framework and in close collaboration with the manufacturer, clinicians, and safety experts.
Stress and anxiety associated with home care may impair caregiving performance and increase error risk, Reference Petruik, Mack, Conway, Buchholz and Manen18 potentially leading to emotional exhaustion and mental health complications for the caregivers. Furthermore, many healthcare professionals stated that detecting thrombi is already very complex in the inpatient setting and depends on interdisciplinary judgement, making outpatient management of young patients with BH-EA particularly challenging. Reference Rohde, Van and Veen2,Reference Adderley, Pidborochynski and Buchholz19 Future studies should advance sensor technology for monitoring flow patterns and clot formation to reduce neurological events.
Requirements for Home Discharge
At home, safety management depends on well-trained caregivers, a responsive healthcare network, and reliable 24/7 expert access via emergency hotlines.
Interviews highlighted the need for comprehensive parental training in medication and coagulation management, recognition of clinical changes, and emergency care, including paediatric basic life support. This would necessitate, among other things, a protocol, particularly in the area of outpatient coagulation management, whose safety should be verified in further prospective studies.
Some competencies can be taught by outpatient nursing staff. This raises several questions, such as: How can a comprehensive training for parents be provided, by whom, and how often? How can the assessment of caregiver knowledge and skills with regards to the medical situation and device management be assessed? How can the training be tailored to meet the individual needs and abilities of the caregivers?
Duffy et al. developed a comprehensive strategy for managing children treated with the HeartMate3TM LVAD, including a standardised training programme combining lectures and hands-on sessions. Reference Duffy, Nandi, Hodge, Deitemyer and Simsic20 The programme imparts knowledge regarding medication, LVAD system and power supply, dressing changes, troubleshooting, alarm response, and paediatric life support conducted by the American Heart Association. Safety measures include checklists, manuals, and a 24/7 physician hotline. The training is community-based, conducted by a multidisciplinary ventricular assist device team, and assessed via the teach-back method. Families complete unsupervised on- and off-campus trips before discharge and receive regular outpatient follow-up with LVAD log review. However, as only one patient has been successfully discharged so far, there is currently no data on the effectiveness of this training yet. Reference Duffy, Nandi, Hodge, Deitemyer and Simsic20
Conway et al. present a standardised ventricular assist device outpatient training programme but stress that no family can be fully prepared for the demands of home care, underscoring the necessity for continuous psychological support. Reference Conway, Vanderpluym, Jeewa, Sinnadurai, Schubert and Conway21
A qualitative study by Crowe et al. with 25 families with children with ventricular assist devices revealed strong parental concerns about their child’s discharge, with many reporting stress and anxiety linked to increased responsibility. Reference Crowe, Simpson, Reinhardt and Rankin14
Such stress may impair caregivers´ mental and physical health and performance, reinforcing the need for sustained psychological support, including regular consultations with a psychologist to mitigate emotional burden and avoid parental guilt in the case of complications. Reference Saimaldaher and Wazqar22
Conclusion
The study presents three primary conclusions:
-
1. The current BH–EA alarm system is conceptualised for in-hospital care and lacks reliable safety mechanisms for non-professionals in home settings, particularly during medical emergencies such as thrombosis.
-
2. Safe discharge requires extensive training for both caregivers and healthcare networks. However, standardised procedures and adequate resources are lacking. Establishing an integrated outpatient care programme is essential for safety, appropriate outcome assessment, and the prevention of adverse events.
-
3. Both professionals and caregivers expressed strong scepticism towards home discharge, citing numerous reasons for their concerns.
Until organ allocation systems are adjusted to avoid disadvantages in organ waiting times after home discharge, and until a safe discharge of infants with BH–EA is possible, efforts should focus on expanding patient and family freedom within the safety net of the hospital campus, such as by developing dedicated living spaces outside the ward itself—thereby addressing many key family needs while maintaining immediate access to expert care. Active family involvement in care enhances emotional well-being and quality of life during BH–EA support. Caregivers should contribute to the development of discharge management protocols. Establishing cross-regional multidisciplinary teams is crucial to create standardised procedures forming the basis of a structured discharge programme in the future. Reference Crowe, Simpson, Reinhardt and Rankin14
Limitations
Given the small sample of families of patients with BH–EA and despite reflexivity measures, the research team’s professional composition may have influenced data collection and interpretation, so findings may not fully capture all perspectives or be generalisable. A number of queries, including those pertaining to the discharge readiness criteria and the optimal time for patient release, remain unanswered due to their absence from the interview questions.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113018.
Acknowledgements
We thank all interviewees for their time and contribution to this study.
Financial support
This work was supported by the Federal Ministry of Research, Technology, and Space of the Federal Republic of Germany (grant number 16KISK212, 6G Health).
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation (“Good Clinical Practice”) and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the ethics committee of the Charité—Universitätsmedizin Berlin (EA2/229/24).





 Open access
Open access