


Introduction
Social anxiety disorder (SAD), which involves fear of situations where one may be scrutinized (American Psychiatric Association, Reference American Psychiatric Association2013), is common (Baxter, Patton, Scott, Degenhardt, & Whiteford, Reference Baxter, Patton, Scott, Degenhardt and Whiteford2013; Kessler, Chiu, Demler, & Walters, Reference Kessler, Chiu, Demler and Walters2005; Wittchen et al., Reference Wittchen, Jacobi, Rehm, Gustavsson, Svensson, Jönsson and Steinhausen2011) and impairing (Aderka et al., Reference Aderka, Hofmann, Nickerson, Hermesh, Gilboa-Schechtman and Marom2012; Stein et al., Reference Stein, Lim, Roest, de Jonge, Aguilar-Gaxiola, Al-Hamzawi and Williams2017). Serotonin reuptake inhibitors (SSRIs) pharmacotherapy is an efficacious first-line treatment for SAD (Curtiss, Andrews, Davis, Smits, & Hofmann, Reference Curtiss, Andrews, Davis, Smits and Hofmann2017; Davis, Smits, & Hofmann, Reference Davis, Smits and Hofmann2014; Mayo-Wilson et al., Reference Mayo-Wilson, Mavranezouli, Kew, Clark, Ades and Pilling2014), but many patients fail to respond to treatment (Blanco et al., Reference Blanco, Heimberg, Schneier, Fresco, Chen, Turk and Liebowitz2010; Davidson et al., Reference Davidson, Foa, Huppert, Keefe, Franklin, Compton and Gadde2004).
Novel treatments that exploit technology and cognitive-neuroscience knowledge may help to address these challenges (Gober, Lazarov, & Bar-Haim, Reference Gober, Lazarov and Bar-Haim2021; Mohr, Burns, Schueller, Clarke, & Klinkman, Reference Mohr, Burns, Schueller, Clarke and Klinkman2013). One such treatment is gaze-contingent music reward therapy (GC-MRT), an eye-tracking-based attention bias modification (ABM) protocol designed to target threat-related attention in SAD (Armstrong & Olatunji, Reference Armstrong and Olatunji2012; Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & van IJzendoorn, Reference Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg and van IJzendoorn2007; Lazarov, Abend, & Bar-Haim, Reference Lazarov, Abend and Bar-Haim2016; Lazarov, Pine, & Bar-Haim, Reference Lazarov, Pine and Bar-Haim2017; Pergamin-Hight, Naim, Bakermans-Kranenburg, van IJzendoorn, & Bar-Haim, Reference Pergamin-Hight, Naim, Bakermans-Kranenburg, van IJzendoorn and Bar-Haim2015). In GC-MRT, patients' gaze is monitored during free viewing of matrices consisting of disgusted and neutral faces. A music track selected by each patient plays during fixations on neutral faces but stops during fixation on disgusted faces. Thus, via gaze-contingent operant conditioning, patients gradually learn to allocate their attention to neutral over threat faces. Compared to previous ABM protocols, applying variations of the dot-probe task (MacLeod, Mathews, & Tata, Reference MacLeod, Mathews and Tata1986), GC-MRT's free-viewing matrix task holds better internal consistency and test–retest reliability, offering clearer view of underlying mechanisms and target engagement (Lazarov et al., Reference Lazarov, Abend and Bar-Haim2016, Reference Lazarov, Pine and Bar-Haim2017; Shamai-Leshem et al., Reference Shamai-Leshem, Abend, Arad, Azriel, Chong, de Jong and Lazarov2023). Importantly, GC-MRT shows favorable clinical outcomes: two open trials of GC-MRT in adults (Umemoto et al., Reference Umemoto, Cole, Allison, Dolan, Lazarov, Auerbach and Schneier2021) and children (Linetzky, Kahn, Lazarov, Pine, & Bar-Haim, Reference Linetzky, Kahn, Lazarov, Pine and Bar-Haim2019) with SAD reported a significant pre-to-post clinical improvement with large effect sizes ($\eta _p^2 = 0.29$ and Cohen's d = 1.43, respectively), high treatment adherence, and treatment credibility. One randomized controlled trial (RCT) (Lazarov et al., Reference Lazarov, Pine and Bar-Haim2017) indicated greater efficacy of GC-MRT relative to a stringent control, and a second RCT (Arad et al., Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023) found comparably greater symptom reductions in GC-MRT and SSRI relative to a waitlist control, with no difference in efficacy between them. These RCTs also demonstrated cognitive target engagement (i.e. a reduction in dwell time on threatening stimuli), and a near transfer-of-learning effect in the presence of a new set of face stimuli not used in training. Here, we examine treatment-related changes in brain function during an implicit threat processing task in this second RCT before and after GC-MRT, SSRI, or a wait period.
and Cohen's d = 1.43, respectively), high treatment adherence, and treatment credibility. One randomized controlled trial (RCT) (Lazarov et al., Reference Lazarov, Pine and Bar-Haim2017) indicated greater efficacy of GC-MRT relative to a stringent control, and a second RCT (Arad et al., Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023) found comparably greater symptom reductions in GC-MRT and SSRI relative to a waitlist control, with no difference in efficacy between them. These RCTs also demonstrated cognitive target engagement (i.e. a reduction in dwell time on threatening stimuli), and a near transfer-of-learning effect in the presence of a new set of face stimuli not used in training. Here, we examine treatment-related changes in brain function during an implicit threat processing task in this second RCT before and after GC-MRT, SSRI, or a wait period.
Prior work suggests that SSRI treatment alters neural responses to social threats in the amygdala (Faria et al., Reference Faria, Appel, Åhs, Linnman, Pissiota, Frans and Furmark2012; Furmark et al., Reference Furmark, Appel, Michelgård, Wahlstedt, Åhs, Zancan and Fredrikson2005, Reference Furmark, Tillfors, Marteinsdottir, Fischer, Pissiota, Långström and Fredrikson2002; Giménez et al., Reference Giménez, Ortiz, Soriano-Mas, López-Solà, Farré, Deus and Merlo-Pich2014; Gingnell et al., Reference Gingnell, Frick, Engman, Alaie, Björkstrand, Faria and Furmark2016; Klumpp & Fitzgerald, Reference Klumpp and Fitzgerald2018; Phan et al., Reference Phan, Coccaro, Angstadt, Kreger, Mayberg, Liberzon and Stein2013), insula (Giménez et al., Reference Giménez, Ortiz, Soriano-Mas, López-Solà, Farré, Deus and Merlo-Pich2014; Schneier, Pomplun, Sy, & Hirsch, Reference Schneier, Pomplun, Sy and Hirsch2011), anterior cingulate cortex (ACC) (Burkhouse et al., Reference Burkhouse, Kujawa, Hosseini, Klumpp, Fitzgerald, Langenecker and Phan2018; Giménez et al., Reference Giménez, Ortiz, Soriano-Mas, López-Solà, Farré, Deus and Merlo-Pich2014; Schneier et al., Reference Schneier, Pomplun, Sy and Hirsch2011), medial prefrontal cortex (mPFC) (Burkhouse et al., Reference Burkhouse, Kujawa, Hosseini, Klumpp, Fitzgerald, Langenecker and Phan2018; Giménez et al., Reference Giménez, Ortiz, Soriano-Mas, López-Solà, Farré, Deus and Merlo-Pich2014; Phan et al., Reference Phan, Coccaro, Angstadt, Kreger, Mayberg, Liberzon and Stein2013), hippocampus (Pantazatos, Talati, Schneier, & Hirsch, Reference Pantazatos, Talati, Schneier and Hirsch2014), and temporal cortex (Pantazatos et al., Reference Pantazatos, Talati, Schneier and Hirsch2014; Phan et al., Reference Phan, Coccaro, Angstadt, Kreger, Mayberg, Liberzon and Stein2013; Schneier et al., Reference Schneier, Pomplun, Sy and Hirsch2011). These studies used various threat processing paradigms, ranging from public speaking challenges to cognitive tasks applying visual presentations of socially threatening faces or words. Within these tasks, a distinction is made between tasks involving explicit emotion processing, where participants rate or respond to an emotional feature of a stimulus (e.g. indicating whether two faces express a similar emotion); and tasks involving implicit emotion processing, where stimuli contain emotional features, but participants do not rate or respond to these features. Importantly, these two types of tasks engage different neuro-cognitive processes (Critchley et al., Reference Critchley, Daly, Phillips, Brammer, Bullmore, Williams and Murphy2000; Fusar-Poli et al., Reference Fusar-Poli, Placentino, Carletti, Landi, Allen, Surguladze and Politi2009; Mathersul et al., Reference Mathersul, Palmer, Gur, Gur, Cooper, Gordon and Williams2009; Norman, Polyn, Detre, & Haxby, Reference Norman, Polyn, Detre and Haxby2006; Pantazatos, Talati, Pavlidis, & Hirsch, Reference Pantazatos, Talati, Pavlidis and Hirsch2012). Whereas most of the above-mentioned studies applied explicit threat processing tasks (Burkhouse et al., Reference Burkhouse, Kujawa, Hosseini, Klumpp, Fitzgerald, Langenecker and Phan2018; Gingnell et al., Reference Gingnell, Frick, Engman, Alaie, Björkstrand, Faria and Furmark2016; Phan et al., Reference Phan, Coccaro, Angstadt, Kreger, Mayberg, Liberzon and Stein2013; Schneier et al., Reference Schneier, Pomplun, Sy and Hirsch2011), Pantazatos et al. (Reference Pantazatos, Talati, Schneier and Hirsch2014) used a task involving implicit processing of social threat. The neural findings associated with these two types of tasks may differ. For example, Pantazatos et al. (Reference Pantazatos, Talati, Schneier and Hirsch2014) reported functional changes in the hippocampus, not evident in studies applying explicit threat processing tasks to test SSRI's neural effects.
Data on ABM-associated changes in neural responses to social threats also indicate altered amygdala response (Britton et al., Reference Britton, Suway, Clementi, Fox, Pine and Bar-Haim2014; Månsson et al., Reference Månsson, Carlbring, Frick, Engman, Olsson, Bodlund and Andersson2013; Taylor et al., Reference Taylor, Aupperle, Flagan, Simmons, Amir, Stein and Paulus2013), and changes in neural activation within the PFC (Browning, Holmes, Murphy, Goodwin, & Harmer, Reference Browning, Holmes, Murphy, Goodwin and Harmer2010; Eldar & Bar-Haim, Reference Eldar and Bar-Haim2010; Shechner & Bar-Haim, Reference Shechner and Bar-Haim2016; Taylor et al., Reference Taylor, Aupperle, Flagan, Simmons, Amir, Stein and Paulus2013). Here too, the variability in neural findings may be partly attributed to differences in methods applied to manipulate threat processing. For example, whereas Månsson et al. (Reference Månsson, Carlbring, Frick, Engman, Olsson, Bodlund and Andersson2013) and Taylor et al. (Reference Taylor, Aupperle, Flagan, Simmons, Amir, Stein and Paulus2013) used explicit matching of facial expressions, Hariri et al. (Reference Hariri, Mattay, Tessitore, Kolachana, Fera, Goldman and Weinberger2002), Britton et al. (Reference Britton, Suway, Clementi, Fox, Pine and Bar-Haim2014) and Eldar and Bar-Haim (Reference Eldar and Bar-Haim2010) assessed neural responses during performance on the dot-probe task, involving implicit threat processing. Additionally, unlike the above-mentioned tasks, in the dot-probe task the presentation of faces is followed by a target, thus the faces and the target stimulus are not processed simultaneously. Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) used a task in which implicit emotion processing took place. This task also involved direct (respond to faces) and indirect (respond to bars appearing alongside faces) processing. Importantly, this combination of implicit emotion processing during allocation of attention toward or away from faces makes it highly relevant for testing neural correlates of GC-MRT – an ABM protocol facilitating the modification of attention toward and away from faces using operant conditioning which is implicitly based on the faces' emotional valence.
Two studies specifically focused on neural correlates of GC-MRT (Umemoto et al., Reference Umemoto, Cole, Allison, Dolan, Lazarov, Auerbach and Schneier2021; Zhu et al., Reference Zhu, Lazarov, Dolan, Bar-Haim, Dillon, Pizzagalli and Schneier2023). These studies, however, examined pre-treatment predictors of clinical improvement. To our knowledge, no studies reported on pre- to post-GC-MRT treatment changes in neural activation during threat processing.
The current study examines common and specific effects of GC-MRT and SSRI pharmacotherapy on brain function during implicit social threat processing in patients with SAD. Functional magnetic resonance imaging (fMRI) data was collected at baseline and post-treatment, or an equivalent waiting period in a control group. To focus analyses on changes in neural activation when participants perform task demands that either match or contradict trained attentional patterns in GC-MRT, we used a task adapted from (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010), and followed their analytic approach. Treatment-related changes in neural activation were tested by placing conflicting demands on attention. To this end, a computation of a training incongruent v. training congruent signal contrast was performed, reflecting brain response to conditions that are incompatible with the GC-MRT training direction. Compared to trials in which the direction of patients' attention conforms with their training, trials in which the attentional demands conflict with the training are generally expected to elicit greater activation in brain regions associated with attention control (Bishop, Duncan, Brett, & Lawrence, Reference Bishop, Duncan, Brett and Lawrence2004; Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010; MacDonald, Cohen, Andrew Stenger, & Carter, Reference MacDonald, Cohen, Andrew Stenger and Carter2000). The following hypotheses were tested in relation to this contrast:
Hypothesis 1: We expected that relative to the waitlist control, GC-MRT and SSRI would alter function within a neural circuit in which aberrant functioning was previously reported in SAD, and which has been suggested to be affected following SAD treatment (Brühl, Delsignore, Komossa, & Weidt, Reference Brühl, Delsignore, Komossa and Weidt2014; Etkin & Wager, Reference Etkin and Wager2007). Specifically, considering existing evidence on neural activation during implicit emotion processing in SAD (Blair et al., Reference Blair, Geraci, Korelitz, Otero, Towbin, Ernst and Pine2011, Reference Blair, Shaywitz, Smith, Rhodes, Geraci, Jones and Pine2008; Gentili et al., Reference Gentili, Gobbini, Ricciardi, Vanello, Pietrini, Haxby and Guazzelli2008; Klumpp, Post, Angstadt, Fitzgerald, & Phan, Reference Klumpp, Post, Angstadt, Fitzgerald and Phan2013b), the effect of treatment on it (Britton et al., Reference Britton, Suway, Clementi, Fox, Pine and Bar-Haim2014; Burkhouse et al., Reference Burkhouse, Kujawa, Hosseini, Klumpp, Fitzgerald, Langenecker and Phan2018, Reference Burkhouse, Kujawa, Klumpp, Fitzgerald, Monk and Phan2017; Eldar & Bar-Haim, Reference Eldar and Bar-Haim2010; Pantazatos et al., Reference Pantazatos, Talati, Schneier and Hirsch2014), and the relevance of the tested contrast to visual processing and attention control functions (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010), we expected that these alterations would occur in parieto-occipital regions, ACC, and PFC. Evidence on the directionality of change is inconsistent, with some studies reporting increases, others reporting decreases, and some reporting no changes in activation within these regions. Given the diversity of brain regions involved, the inconsistent findings concerning change direction, and the limited previous evidence on GC-MRT-related neural changes, we decided to use a conservative whole brain analysis to identify treatment-related changes in the current study.
Hypothesis 2: GC-MRT and SSRI would induce distinct treatment-specific functional changes. Considering the reported neural correlates of ABM for SAD (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010; Eldar & Bar-Haim, Reference Eldar and Bar-Haim2010; Taylor et al., Reference Taylor, Aupperle, Flagan, Simmons, Amir, Stein and Paulus2013; Umemoto et al., Reference Umemoto, Cole, Allison, Dolan, Lazarov, Auerbach and Schneier2021; Zhu et al., Reference Zhu, Lazarov, Dolan, Bar-Haim, Dillon, Pizzagalli and Schneier2023), and the role of attention control in the mechanisms underlying ABM (Shechner & Bar-Haim, Reference Shechner and Bar-Haim2016), we expected that GC-MRT will be associated with alterations in the ACC and PFC, two key areas associated with attention control. In addition, based on Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010), we expected greater recruitment of these areas at post-treatment in GC-MRT patients when they are specifically required to direct attention opposite to their trained direction (i.e. the incongruent>congruent contrast), reflecting greater effort to control attention.
Hypothesis 3: Within the GC-MRT group, greater clinical improvement would relate to greater functional change in areas associated with attention control.
Additional separate exploratory analyses were conducted to examine changes in neural response to threat compared to neutral faces occurring during direct face processing (i.e. when patients are instructed to process faces) and indirect face processing (i.e. when patients are instructed to process bars appearing alongside faces).
Methods and materials
Participants
For the full protocol, sample-size determination, randomization, and blinding details see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023) (ClinicalTrials.gov Identifier: NCT03346239). Of the 105 enrolled patients, 8 were ineligible for MRI procedures, 15 did not provide post-treatment MRI data, and one was excluded due to low accuracy on the task (<70%). Pre-to-post analyses (162 MRI scans) were conducted on 81 participants (mean [s.d.] age = 29.62 [7.05] years, 49 females): GC-MRT (n = 29), SSRI (n = 22), and waitlist control [WL, n = 30] (see online Supplementary Fig. S4). Groups did not differ in demographic or clinical characteristics at baseline (see online Supplementary Table S3). No patients in the GC-MRT group received SSRI treatment during their participation in the trial. Participants provided a written informed consent as approved by the local IRBs.
Treatments
SSRI treatment followed a standard 12-week protocol of Escitalopram (Kasper, Stein, Loft, & Nil, Reference Kasper, Stein, Loft and Nil2005). This flexible dose protocol started from 5 mg and increased to 20 mg according to patients' response. Meetings with a psychiatrist occurred at weeks 1, 3, 6, and 12 of treatment.
For a detailed description of the GC-MRT protocol see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023). Ten GC-MRT sessions were delivered – 8 twice-weekly over four weeks and two additional sessions at weeks 8 and 11. For each session patients selected a music track they wanted to listen to. Patients then viewed 30 matrices comprised of 16 faces each – 8 disgust (threat) faces and 8 neutral faces. Faces were taken from the Karolinska Directed Emotional Faces database (KDEF; Lundqvist, Flykt, and Öhman, Reference Lundqvist, Flykt and Öhman1998). Gaze was tracked throughout, and music was played only when fixating on neutral faces and stopped when fixating on disgusted faces. This gaze-contingent operant conditioning procedure induces attentional preference for neutral over threat faces.
The WL group received 8 sessions of GC-MRT, delayed by 12 weeks.
Neuroimaging attention task
A task adapted from Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) was used (Fig. 1). Each trial began with a fixation cross (500 ms), followed by a face flanked by two bars (200 ms). Participants' attention was manipulated by instructing them to either identify the gender of the face (‘attend face’ blocks) or determine whether the flanking bars are aligned (‘attend bars’ blocks). Eight blocks of 20 trials each (160 total) were presented. In each block disgusted and neutral faces appeared with equal frequency. Faces were taken from the KDEF database (Lundqvist et al., Reference Lundqvist, Flykt and Öhman1998); importantly, actors that appeared in the attention task were different from actors that appeared in GC-MRT training. Task structure was factorial: two levels of emotion (disgust/neutral) by two levels of attention (toward/away from the presented face). This enabled an analysis contrasting brain function during conditions congruent with GC-MRT training (attending toward neutral faces and away from threat faces) with brain function during conditions incongruent with GC-MRT training (attending toward threat faces and away from neutral faces). Participants had up to 3250 ms to respond, followed by a jittered inter-trial interval ranging 50–3050 ms (mean duration 1550 ms). Every two blocks (‘attend face’/‘attend bars' presented in a random order) were performed within a single run with a short break between runs. The stimuli set used in the fMRI task differed from the set used during GC-MRT sessions to avoid a potential effect of familiarity on neural response. The task was run using Presentation (Neurobehavioral Systems Inc., USA, http://www.neurobs.com/). For a pre-treatment manipulation check and test-retest reliability of the task, see online Supplementary Material.
During the fMRI task, participants were instructed to indicate either the gender of the face or whether the flanking bars are aligned. In each block, half of the trials included a disgusted face and half of the trials included a neutral face. fMRI, functional magnetic resonance imaging.

Image acquisition and preprocessing
MRI data was acquired on a Siemens Magnetom Prisma 3 T scanner (Siemens, Erlangen, Germany), using a 64 channel phased array head coil. The protocol comprised structural and functional MRI scans as following: high resolution anatomical localizer image (MPRAGE): TR = 1750 ms, TE = 2.61 ms, TI = 900 ms, flip angle = 8o, isotropic resolution of 1mm3. Functional MRI was obtained by multiband echo-plannar imaging (EPI, University of Minnesota sequence) to acquire blood-oxygen-level-dependent (BOLD) sensitive images: TR = 2000 ms; TE = 30 ms; flip angle = 82°; IPAT = 2, multiband factor = 2, isotropic resolution of 2mm3 and 66 axial slices 2 mm thick (no gap) to ensure full brain coverage. Additionally, field-maps were acquired using two opposite coded (AP, PA) echo-plannar scans: TR = 8152 ms; TE = 66 ms; flip angle = 90°; multiband factor = 1; isotropic resolution of 2mm3 and 66 axial slices 2 mm thick (no gap). All images were acquired in the anterior commissure – posterior commissure (AC–PC) line extending down from the top of the brain.
Functional images were pre-processed using the FMRIB Software Library, version 6.0.0 (Oxford University, Oxford, United Kingdom, http://www.fmrib.ox.ac.uk/fsl) (Jenkinson, Beckmann, Behrens, Woolrich, & Smith, Reference Jenkinson, Beckmann, Behrens, Woolrich and Smith2012). The following steps were conducted: removal of non-brain structures using BET (Smith, Reference Smith2002); temporal high pass filtering with a cut off of 100s; fieldmap-based distortion-correction; rigid body motion correction, aligned to middle volume as an initial template image, using MCFLIRT (Jenkinson, Bannister, Brady, & Smith, Reference Jenkinson, Bannister, Brady and Smith2002); spatial smoothing with a 5 mm isotropic Gaussian kernel. To normalize images to the Montreal Neurological Institute (MNI) template, low-resolution EPI images were first registered to higher-resolution EPI reference images (expanded functional images), then to a high resolution T1 images (using a linear, normal search registration) (Jenkinson et al., Reference Jenkinson, Bannister, Brady and Smith2002; Jenkinson & Smith, Reference Jenkinson and Smith2001), then to the 152T1 MNI template (using a non-linear registration) (Andersson, Jenkinson, & Smith, Reference Andersson, Jenkinson and Smith2007).
To reduce artifacts, Independent Component Analysis (ICA) was performed using Multivariate Exploratory Linear Optimized Decomposition into Independent Components (MELODIC). Components from ten participants were hand classified as ‘noise’ or ‘signal’ (Griffanti et al., Reference Griffanti, Douaud, Bijsterbosch, Evangelisti, Alfaro-Almagro, Glasser and Smith2017). Then, using this hand-classified training dataset, data was cleaned with FMRIB's ICA-based Xnoiseifier (FIX, version 1.066). This procedure also included motion confounds cleanup with highpass filtering.
An event-related design was used for the task. 500 ms events (‘attend toward threat’, ‘attend toward neutral’, ‘attend away from threat’, ‘attend away from neutral’) were convolved with a canonical double-gamma HRF to generate the model regressors.
Social anxiety
The primary clinical outcome was total score on the clinician-administered Liebowitz Social Anxiety Scale (LSAS) (Liebowitz, Reference Liebowitz1987). Cronbach's alphas in the current study were 0.86 and 0.92 at pre- and post-treatment, respectively.
General procedure
Following a baseline clinical evaluation, participants completed an MRI session consisting of structural, resting state, and the attention task. Then, participants were randomly assigned to 12 weeks of SSRI, GC-MRT, or WL. In week 13, a clinical evaluation and a second MRI session with the same parameters as the baseline session took place. The study was conducted from July 2018 to December 2021.
Statistical analyses
Clinical effects were tested using a repeated-measures analysis of variance (ANOVA) with group (GC-MRT, SSRI, WL control) as a between-subjects factor and time (baseline, post-treatment) as a within-subject factor. Significant ANOVA results were followed by pairwise corrected independent samples t tests.
The effects of group, time, congruency with GC-MRT training, and group-by-time-by-congruency interaction on task accuracy and reaction-time (RT), were tested using repeated-measures ANOVAs with group (GC-MRT, SSRI, WL control) as a between-subjects factor and time (baseline, post-treatment) and congruency (incongruent trials, congruent trials) as within-subject factors. The task was designed to be behaviorally insensitive (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) and therefore allowed interpretation of the imaging data not confounded by behavioral differences between groups or time-points.
Imaging data analyses used FMRIB Software Library (FSL), version 6.0.0 (Oxford University, Oxford, United Kingdom, http://www.fmrib.ox.ac.uk/fsl) (Jenkinson et al., Reference Jenkinson, Beckmann, Behrens, Woolrich and Smith2012). Incongruent>congruent blood-oxygen-level-dependent (BOLD) signal contrast maps were computed: training-incongruent trials were ‘attend face’ trials with disgusted faces and ‘attend bars’ trials with neutral faces, and training-congruent trials were ‘attend face’ trials with neutral faces and ‘attend bars’ trials with disgusted faces. This contrast probed specific alterations in threat-related attentional processes – the target of GC-MRT. Specifically, following the logic of Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010), the selected contrast enabled testing neural activation associated with attention allocation patterns that are opposite to the pattern to which GC-MRT patients were trained (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010), and presumably requiring greater neural recruitment to oppose. Contrast images were calculated individually for each participant in each run, and then collapsed across all four runs to generate post>pre contrast maps.
The statistical analyses used to test hypotheses 1 and 2 were modeled after a recently published paper by Goldin et al. (Reference Goldin, Thurston, Allende, Moodie, Dixon, Heimberg and Gross2021), using a similar design to address similar questions. To test hypothesis 1, treated patients (GC-MRT/SSRI) were compared to WL participants on the post>pre contrast maps. To test hypothesis 2, GC-MRT patients were compared to SSRI patients on the post>pre contrast maps. For hypothesis 3, the correlations between pre-to-post clinical change (total LSAS difference score) and pre-to-post activation change (incongruent>congruent contrast difference maps) were tested. Although our hypotheses suggest potential effects in specific brain regions, given the scarcity of evidence on neural changes following GC-MRT and the possibility that this new treatment may affect additional unpredicted brain regions, we opted to apply a conservative whole-brain analytic approach and bidirectional hypotheses testing. Of note, although we defined the post>pre as the positive contrast when computing brain maps, the opposite direction of change, i.e., pre>post contrast, could also be represented in clusters with negative z values. This way, both contrasts were tested, and a bidirectional approach was maintained both for the group and time variables. Whole brain analyses were corrected for multiple comparisons using parametric cluster-based correction. A cluster forming threshold of z > 2.3 was applied at the voxel level, followed by an FWE correction at a significance level of p < 0.05 that was applied to the resulting clusters. This approach, combining voxel-level thresholding and FWE correction, is widely used in fMRI studies. It is also the default correction approach in FSL. Similar thresholds for cluster forming and FWE correction (z > 2.3; p < 0.05) have been applied in a number of fMRI studies in psychopathology (e.g. Aghajani et al., Reference Aghajani, Veer, van Hoof, Rombouts, van der Wee and Vermeiren2016; Foerde, Steinglass, Shohamy, & Walsh, Reference Foerde, Steinglass, Shohamy and Walsh2015; Walsh et al., Reference Walsh, Eisenlohr-Moul, Minkel, Bizzell, Petty, Crowther and Dichter2019; White et al., Reference White, Shirer, Molfino, Tenison, Damoiseaux and Greicius2013), and specifically by Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) from whom the task used in the current study was adapted.
Two additional contrasts were used to explore changes in neural response to threat during direct (i.e. when patients are instructed to process the faces) or indirect (i.e. when patients are instructed to process the bars) face processing. Threat v. neutral contrasts were computed separately for ‘attend face’ trials (i.e. contrasting toward threat trials v. toward neutral trials) and ‘attend bars’ trials (i.e. contrasting away from threat trials v. away from neutral trials). An additional contrast, toward neutral v. away from threat, was also tested. Group comparisons (treated patients v. WL patients and GC-MRT v. SSRI patients) of pre-to-post changes were performed using these separate contrasts as described for the ‘incongruent v. congruent’ contrast.
Between-group and between-time differences in framewise displacement were tested to verify that significant effects emerged from the above-mentioned analyses were not related to head motion differences (see online Supplementary Material). Localization of significant clusters was based on peak coordinates reported in previous studies. For further specification, distinct clusters within the ACC were numbered from rostral (specified as ‘ACC1’) to caudal (specified as ‘ACC3’).
To interpret significant results and explore significance and direction of change within each group and time-point, post-hoc analyses were performed using the average percent signal change within each significant cluster (Anticevic et al., Reference Anticevic, Hu, Zhang, Savic, Billingslea, Wasylink and Pittenger2014; Su et al., Reference Su, Blamire, Watson, He, Hayes and O'Brien2016). For hypotheses 1 and 2, these analyses were performed as follows: First, simple effects of group and time were tested using independent samples t tests and paired samples t tests, respectively. For completeness, exploratory time-simple-effect tests for each of the treatment groups (GC-MRT, SSRI) were performed for the clusters extracted from the treatment v. WL main analysis; and a time-simple-effect was tested within the WL group for the cluster extracted from the GC-MRT v. SSRI main analysis. Finally, for clusters in which there were significant baseline between-group differences in mean BOLD signal change, we conducted additional analyses controlling for baseline BOLD signal change as a covariate; these tests for baseline group differences and subsequent covariate analyses are described in the online Supplementary Material. For hypothesis 3, exploratory post-hoc analysis included averaging the percent signal change within the examined cluster both at baseline and at post-measurement, then calculating the difference between the two time-points for each participant. A simple correlation coefficient was used to test the association between this activation change and change in total LSAS scores. Fisher's r-to-Z transformations were used to compare the magnitude of these correlations between groups. To test whether activation-symptom correlation specifically characterized brain regions that emerged as sensitive to intervention in the current study, we also applied this analysis using the mean activation change within the significant clusters that emerged from analyses performed for hypotheses 1 and 2. All these follow-up analyses were conducted using IBM SPSS Statistics, version 28.0.
Results
Data analysis included 81 patients (GC-MRT: n = 29; SSRI: n = 22; WL: n = 30).
Demographics and clinical outcomes
Clinical outcomes in MRI-completers resembled those noted in the full sample (Arad et al., Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023). This involved a significant Time-by-Group interaction (F[2, 78] = 10.00, $\eta _p^2 = 0.20$ [90% CI 0.07 to 0.32]). Follow-up analyses indicated that both GC-MRT and SSRI were associated with lower symptoms post-treatment compared to the WL control group (GC-MRT: t[57] = −3.56. p < 0.001, d = −0.93 [95% CI −1.46 to −0.38]; SSRI: t[50] = −3.49. p < 0.001, d = −0.98 [95% CI −1.56 to −0.39]). No significant difference in LSAS scores was noted between GC-MRT and SSRI post-treatment (p = 0.95). For detailed clinical results of the full sample, including Clinically Significant Change and Reliable Change, see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023). Also see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023) for a description of cognitive target engagement (i.e. changes in dwell time on threat faces) among GC-MRT patients.
[90% CI 0.07 to 0.32]). Follow-up analyses indicated that both GC-MRT and SSRI were associated with lower symptoms post-treatment compared to the WL control group (GC-MRT: t[57] = −3.56. p < 0.001, d = −0.93 [95% CI −1.46 to −0.38]; SSRI: t[50] = −3.49. p < 0.001, d = −0.98 [95% CI −1.56 to −0.39]). No significant difference in LSAS scores was noted between GC-MRT and SSRI post-treatment (p = 0.95). For detailed clinical results of the full sample, including Clinically Significant Change and Reliable Change, see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023). Also see Arad et al. (Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023) for a description of cognitive target engagement (i.e. changes in dwell time on threat faces) among GC-MRT patients.
Neuroimaging
Task behavioral performance
Per design, the attentional task was behaviorally insensitive (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) with high accuracy at pre- (M = 91%, s.d. = 8%) and post-treatment (M = 92%, s.d. = 9%). There were no significant effects of time, group, congruency, or time-by-group-by-congruency interaction on accuracy (ps> 0 .22). As expected, there was a significant main effect of time on RT, with lower RTs at post-treatment scans compared to baseline scans (F[1, 78] = 23.43, $\eta _p^2 = 0.23$ [90% CI 0.10 to 0.35]). There were no significant effects of group, congruency, or time-by-group-by-congruency interaction on RT (ps > 0.17). For additional analyses of behavioral performance conducted separately for all four task conditions, see online Supplementary Material.
[90% CI 0.10 to 0.35]). There were no significant effects of group, congruency, or time-by-group-by-congruency interaction on RT (ps > 0.17). For additional analyses of behavioral performance conducted separately for all four task conditions, see online Supplementary Material.
Treatments v. waitlist control (hypothesis 1)
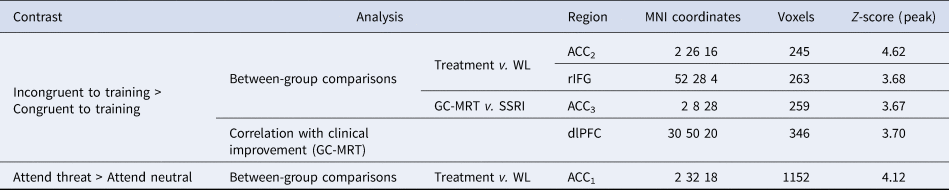
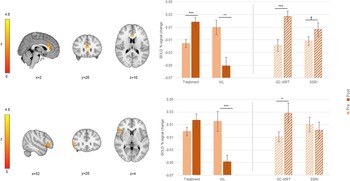
When required to direct attention contrary to GC-MRT training (incongruent>congruent contrast), treated patients showed greater pre-to-post increase in BOLD signal change in ACC2 (one of the two more rostral of the significant ACC clusters) and the right inferior frontal gyrus (rIFG), compared to WL participants (Table 1 and Fig. 2). In ACC2, a significant activation increase was noted among treated patients (t[50] = −4.34, p < 0.001, d = −0.61 [95% CI −0.90 to −0.31]) whereas WL patients showed a significant decrease in activation (t[29] = 3.36, p = .002, d = 0.61 [95% CI 0.22 to 1.00]). In the rIFG, WL participants showed an activation decrease (t[29] = 4.19, p < 0.001, d = 0.76 [95% CI 0.35 to 1.17) whereas treated patients showed no change in activation (t[50] = −1.59, p = 0.12, d = −0.22 [95% CI −0.50 to 0.06]).
Significant clusters emerged for the incongruent>congruent contrast and the attend-threat>attend-neutral contrast (direct threat processing), in group comparisons of pre-to-post BOLD activation increase and correlation tests of clinical improvement and pre-to-post BOLD activation increase association

BOLD, blood-oxygen-level-dependent; WL, waitlist; GC-MRT, gaze contingent music reward therapy; SSRI, serotonin reuptake inhibitors; ACC, anterior cingulate cortex; rIFG, right inferior frontal gyrus; dlPFC, dorsolateral prefrontal cortex; MNI, Montreal neurological institute.
Clusters within the ACC are numbered from rostral (ACC1) to caudal (ACC3).
ACC2 and rIFG clusters in which pre-to-post increase in BOLD signal change (incongruent>congruent contrast) was different between treatment (GC-MRT and SSRI) and WL patients; and the mean BOLD signal change within every significant cluster, by group and time. Separate post-hoc analyses for GC-MRT and SSRI patients are also presented (striped bars). For simplicity, only time simple-effects significance is labeled (*** p < 0.001; ** p < 0.01; *p < 0.05; † p = 0.056). BOLD, blood-oxygen-level-dependent; GC-MRT, gaze contingent music reward therapy; SSRI, serotonin reuptake inhibitors; WL, waitlist. Error bars represent standard errors.

Simple effects analyses performed separately for the two treatment groups revealed that for both ACC2 and rIFG clusters, activation increased in the GC-MRT group (ACC2: t[28] = −3.96, p < 0.001, d = −0.73 [95% CI −1.14 to −0.32]; rIFG: t[28] = −2.35, p = 0.03, d = −0.44 [95% CI −0.81 to −0.05]). For SSRI patients, ACC2 activation increase was marginally significant (t[21]= −2.02, p = 0.056, d = −0.43 [95% CI −0.86 to 0.11]), and rIFG activation did not significantly change (t[21] = 0.75, p = 0.46, d = 0.16 [95% CI −0.26 to 0.58]) (Fig. 2).
GC-MRT v. SSRI (hypothesis 2)
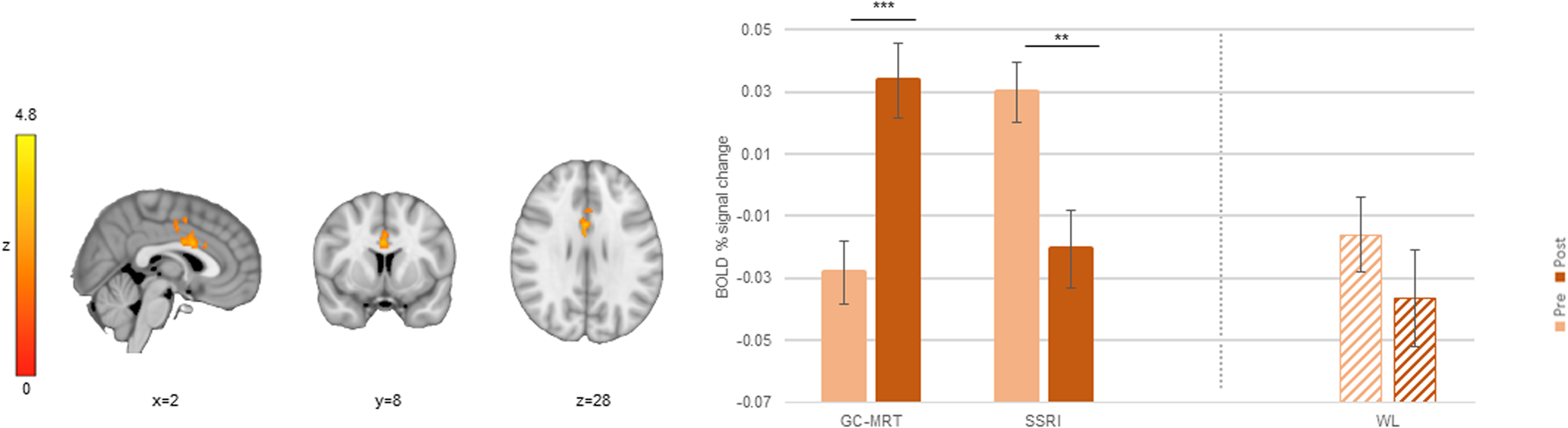
Compared to SSRI patients, GC-MRT patients showed a greater pre-to-post increase in incongruent>congruent signal change in ACC3 (the more caudal of the significant ACC clusters; see Table 1 and Fig. 3). Follow-up analyses indicated a significant pre-to-post increase in neural activation within this cluster among GC-MRT patients (t[28] = −4.24, p < 0.001, d = −0.79 [95% CI −1.20 to −0.36), whereas the opposite pattern emerged in SSRI patients (t[21] = 3.61, p = 0.002, d = 0.77 [95% CI 0.28 to 1.24]).
An ACC3 cluster in which pre-to-post increase in BOLD signal change (incongruent>congruent contrast) was different between GC-MRT and SSRI patients; and the mean BOLD signal change within this significant cluster, by group and time. Post-hoc analysis within this region is also presented for WL participants (striped bars). For simplicity, only time simple-effects significance is labeled (*** p < 0.001; ** p < 0.01). BOLD, blood-oxygen-level-dependent; GC-MRT, gaze contingent music reward therapy; SSRI, serotonin reuptake inhibitors; WL, waitlist. Error bars represent standard errors.

Applying a simple effect analysis on the same cluster in the WL control group indicated no significant pre-to-post change in mean signal change (t[29] = 1.07, p = 0.29, d = 0.19 [95% CI −0.17 to 0.55]) (Fig. 3).
Neural change – clinical change association (hypothesis 3)
Whole brain analysis revealed that in the GC-MRT group, a positive correlation was noted between pre-to-post symptom change and incongruent>congruent activation change, within a single cluster in the dorsolateral prefrontal cortex (dlPFC) (see Table 1 and Fig. 4). Follow-up analysis indicated a strong correlation between symptom change and this cluster's averaged activation change (r = 0.75, p < 0.001, R2 = 0.56 [95% CI 0.34 to 0.78]) (Fig. 4). For the SSRI and WL groups, the correlations between symptom change and averaged activation change within this cluster were not significant (all ps > 0.39); r-to-Z transformations showed that the observed correlation in the GC-MRT group was greater than the correlations in the SSRI and WL groups (r-to-Zs = 3.29 and 4.13, ps < 0.001, respectively). No significant clusters emerged for clinical and neural change correlations in the SSRI or WL groups. No significant correlations were found between symptom change and activation change within brain regions in which significant clusters were found in hypothesis 1 and 2 (See online Supplemental Table S4).
A dlPFC cluster in which pre-to-post increase in BOLD signal change (incongruent>congruent contrast) was significantly correlated with clinical improvement among GC-MRT patients. The scatter plot presents the correlation between the mean BOLD signal change within this cluster and the clinical change (GC-MRT: r = 0.75, p < 0.001, R2 = 0.56; SSRI and WL: ps > 0.39). BOLD, blood-oxygen-level-dependent; GC-MRT, gaze contingent music reward therapy.

Direct and indirect threat processing
Treated patients showed greater pre-to-post increase in BOLD signal change in ACC1 compared to WL participants (Table 1 and Fig. 5) during direct processing of threat faces. In ACC1, a significant increase in attend threat > attend neutral activation increase was noted among treated patients (t[50] = −2.69, p < 0.01, d = −0.38 [95% CI −0.66 to −0.09]) whereas WL participants showed a significant decrease in activation (t[29] = 4.85, p < 0.001, d = 0.88 [95% CI 0.46 to 1.30). A separate simple effects analyses for the two treatment groups showed a non-significant trend level increase in both GC-MRT and SSRI groups (GC-MRT: t[28] = −1.90, p = 0.068, d = −0.35 [95% CI −0.72 to 0.03]; SSRI: t[21] = −1.89, p = 0.073, d = −0.40 [95% CI −0.83 to 0.04]) (Fig. 5). In this brain region, there were no significant pre-to-post activation changes during indirect threat processing (attend threat > attend neutral contrast) (see online Supplement Fig. S5). No group differences were evident during indirect threat processing or for the toward neutral v. away from threat contrast.
An ACC1 cluster in which pre-to-post increase in BOLD signal change during direct threat processing (toward threat > toward neutral) was different between treatment (GC-MRT and SSRI) and WL patients; and the mean BOLD signal change within this cluster, by group and time. Separate post-hoc analyses for GC-MRT and SSRI patients are also presented (striped bars). For simplicity, only time simple-effects significance is labeled (*** p < 0.001; ** p < 0.01; GC-MRT: † p = 0.068; SSRI: † p = 0.073). BOLD, blood-oxygen-level-dependent; GC-MRT, gaze contingent music reward therapy; SSRI, serotonin reuptake inhibitors; WL, waitlist. Error bars represent standard errors.

Discussion
We investigated common and specific effects of GC-MRT and SSRI treatments on brain function during social threat processing. Three key findings emerged: (a) activation changes in a rostral region of the ACC and in the rIFG differentiated between treated (GC-MRT/SSRI patients) and non-treated waitlist patients; (b) activation changes in a distinct, caudal cluster within the ACC, differentiated between GC-MRT and SSRI patients; and (c) GC-MRT patients showed a strong association between clinical improvement and dlPFC activation change when required to act against the action they were trained for in treatment (i.e. attend threat rather than neutral faces). Together, these results suggest both common and unique treatment effects of attention bias modification and SSRI on brain function.
Within the regions that differentiated between treated and non-treated patients (ACC1, ACC2, and rIFG), patients in the WL group exhibited decrease in activation in the second session, possibly reflecting habituation to the previously encountered stimuli. In contrast, activation in these areas increased significantly among treated patients, suggesting a treatment-related effect. The ACC has been associated with downregulation of emotional responses and mediation of cognitive influences on emotion (Bush, Luu, & Posner, Reference Bush, Luu and Posner2000; Holroyd & Umemoto, Reference Holroyd and Umemoto2016; Segalowitz & Dywan, Reference Segalowitz and Dywan2008; Stevens, Hurley, & Taber, Reference Stevens, Hurley and Taber2011). The current findings converge with previous reports on functional changes within these brain regions following clinically effective pharmacological and cognitive-behavioral interventions for SAD (Carlson et al., Reference Carlson, Fang, Koster, Andrzejewski, Gilbertson, Elwell and Zuidema2022; Giménez et al., Reference Giménez, Ortiz, Soriano-Mas, López-Solà, Farré, Deus and Merlo-Pich2014; Goldin, Manber, Hakimi, Canli, & Gross, Reference Goldin, Manber, Hakimi, Canli and Gross2009a; Goldin, Manber-Ball, Werner, Heimberg, & Gross, Reference Goldin, Manber-Ball, Werner, Heimberg and Gross2009b; Klumpp, Fitzgerald, & Phan, Reference Klumpp, Fitzgerald and Phan2013a; Månsson et al., Reference Månsson, Carlbring, Frick, Engman, Olsson, Bodlund and Andersson2013). The ACC is a part of the salience network, a neural network attuned to the salience of external and internal stimuli (Seeley, Reference Seeley2019; Seeley et al., Reference Seeley, Menon, Schatzberg, Keller, Glover, Kenna and Greicius2007). The salience network is also specifically involved in detecting changes in facial emotion expressions (Luo et al., Reference Luo, Qin, Fernández, Zhang, Klumpers and Li2014; Rosen et al., Reference Rosen, Sheridan, Sambrook, Dennison, Jenness, Askren and McLaughlin2018). Irregular function of the salience network was reported in patients with SAD (see: Kim and Yoon, Reference Kim and Yoon2018). Therefore, the current findings may represent treatment-related changes in salience network function.
The rIFG has been associated with inhibitory control, including the intention to stop or slow action, or to suppress an urge for action (Aron, Robbins, & Poldrack, Reference Aron, Robbins and Poldrack2004, Reference Aron, Robbins and Poldrack2014; Rubia, Smith, Brammer, & Taylor, Reference Rubia, Smith, Brammer and Taylor2003; Shadli et al., Reference Shadli, High, Byers, Gibbs, Steller, Glue and McNaughton2020; Verbruggen & Logan, Reference Verbruggen and Logan2008); this may suggest that the two active treatments for SAD applied in the current study are related to enhanced recruitment of inhibitory brain functions when patients are instructed to divert their attention away from neutral stimuli and toward threatening ones. Such change in inhibitory functions may be particularly relevant for patients in the GC-MRT group, due to the requirement in the applied task to respond contrary to the pattern they had practiced repeatedly during treatment. Considering that the interaction effect for the rIFG was partially driven by a decrease in activation in the WL group, it may be argued that these changes are also related to habituation to the task in this group. According to this interpretation, it is possible that treatment countered this basic habituation effect. Notably, follow-up analyses indeed suggest that whereas GC-MRT patients show significant increases in both ACC2 and rIFG activations from pre- to post-treatment, SSRI patients showed only a trend level increase in ACC2 and a non-significant change in rIFG. The similar pattern of treatment-related ACC2 activation increase in both treated groups potentially reflect a change in general threat monitoring mechanisms tapped into by both the GC-MRT (see results from Browning et al. (Reference Browning, Holmes, Murphy, Goodwin and Harmer2010)) and SSRI protocols, and that the rIFG may be more specifically affected by GC-MRT than by SSRI. This interpretation is also in line with the results of the exploratory analysis indicating a similar pattern of change in a close and overlapping region of the rostral ACC (ACC1) during direct, but not indirect, threat processing. Thus, the noted activation changes in the rostral ACC could reflect changes in a more general response to direct threat processing following treatment, that potentially drives the findings that emerged in ACC2 in training incongruent v. congruent activation.
Importantly, the direct comparison between the two active treatments in the current study revealed treatment-specific changes. Patients receiving GC-MRT showed pre- to post-treatment increase in ACC3 activation, whereas the opposite pattern was noted for SSRI patients. Post-hoc analyses further indicate that within this specific cluster, activation among WL participants did not significantly change and was similar in pattern to that of the SSRI group. While the cluster differentiating between treated to non-treated patients in general was located more rostral within the ACC (ACC2), the cluster distinguishing pre-to-post treatment changes between GC-MRT and SSRI was found more caudal (ACC3). The rostral section of the ACC is often described as the ‘affective’ ACC division, and has been associated with emotional conflict and emotion suppression in healthy individuals, and with symptom provocation in anxiety (Bush et al., Reference Bush, Luu and Posner2000; Drevets & Raichle, Reference Drevets and Raichle1998; Etkin, Egner, Peraza, Kandel, & Hirsch, Reference Etkin, Egner, Peraza, Kandel and Hirsch2006; Polli et al., Reference Polli, Barton, Cain, Thakkar, Rauch and Manoach2005). The caudal ACC is typically considered as the ‘cognitive’ sub-region, reported to be activated when reduction of cognitive conflict is required in divided-attention and working-memory tasks (Bush et al., Reference Bush, Luu and Posner2000; Drevets & Raichle, Reference Drevets and Raichle1998; Kerns et al., Reference Kerns, Cohen, MacDonald, Cho, Stenger and Carter2004; Polli et al., Reference Polli, Barton, Cain, Thakkar, Rauch and Manoach2005). It is conceivable that GC-MRT patients, who deliberately practiced diverting their gaze away from threat faces and toward neutral faces, needed to recruit more caudal-ACC resources when faced with the opposite requirement in the fMRI task (i.e. attending toward threatening faces and away from neutral faces).
Moreover, GC-MRT patients showed a strong association between clinical improvement and dlPFC activation change when faced with this requirement. These findings join the results of an earlier study (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010) using the same task, in which hyperactivation of the dlPFC was noted among individuals who were requested to act contrary to the attentional pattern they had trained for in a manual reaction-time-based ABM intervention (Browning et al., Reference Browning, Holmes, Murphy, Goodwin and Harmer2010). Of note, the dlPFC is also involved in emotion categorization (Cacioppo, Crites, Berntson, & Coles, Reference Cacioppo, Crites, Berntson and Coles1993; Freedman, Riesenhuber, Poggio, & Miller, Reference Freedman, Riesenhuber, Poggio and Miller2003; Zwanzger et al., Reference Zwanzger, Steinberg, Rehbein, Bröckelmann, Dobel, Zavorotnyy and Junghöfer2014). It is possible that GC-MRT uniquely affected dlPFC function leading to the use of a different categorization strategy during the attention task. This difference could be manifested in the noted association between symptom change and dlPFC activation during task performance. Although the findings in Browning et al., (2010) suggest that the dlPFC may be sensitive to cognitive changes following ABM, interpreting the activation-symptom correlation found in the dlPFC in the current study may be challenging, considering that this brain region did not emerge as sensitive to shared (hypothesis 1) or distinct (hypothesis 2) treatment effects.
The current results also correspond with a study describing heightened error-related negativity (ERN) as a predictor of GC-MRT clinical efficacy for SAD (Umemoto et al., Reference Umemoto, Cole, Allison, Dolan, Lazarov, Auerbach and Schneier2021). The ERN is thought to be generated in the caudal part of the ACC (Cavanagh & Shackman, Reference Cavanagh and Shackman2015; Holroyd & Umemoto, Reference Holroyd and Umemoto2016; Yeung, Botvinick, & Cohen, Reference Yeung, Botvinick and Cohen2004). It is therefore possible that GC-MRT specifically elevates threat-related attention processing in this brain region assisting patients with SAD to down-regulate their predisposed hypersensitivity to social threats, gain better ability to disengage from such threats, and subsequently experience relief in SAD symptoms.
A few limitations of the current study should be noted. First, although the use of a waitlist control affords an important read of the effects of repeated assessments on brain function, this condition limits the capacity to differentiate specific neural effects of active treatment components from those of non-specific treatment effects. Future studies on the neural correlates of these treatments may wish to test their effects on brain function in comparison to placebo pills and a sham computerized training control, for the SSRI and GC-MRT treatments, respectively (Lazarov et al., Reference Lazarov, Pine and Bar-Haim2017). Future studies may also wish to compare GC-MRT to CBT. Whereas we decided to contrast GC-MRT with a treatment that potentially relies on different mechanisms of actions, it may also be valuable to examine whether GC-MRT and CBT – both targeting cognitive processes and attentional patterns specifically – have common neural mechanisms. Second, differential drop-out rates between the groups may affect the generalizability of the current findings; specifically, the higher drop-out in the SSRI group could have affected the characteristics of the final sub-sample on which analyses were performed. Third, fMRI scans took place at baseline and post-treatment. An addition of interim mid-treatment scans could shed additional light on potential between-treatments differences in the trajectories of neural changes over time. However, it is worth noting that the clinical effect of GC-MRT has been shown to last at least three months (Lazarov et al., Reference Lazarov, Pine and Bar-Haim2017), and that the rate of clinical improvement over time in the current sample closely overlapped in GC-MRT and SSRI treatment (see: Arad et al., Reference Arad, Azriel, Pine, Lazarov, Sol, Weiser and Bar-Haim2023). Fourth, the current study was not powered to test for all possible main and interaction effects using an omnibus whole-brain mixed ANOVA. Future studies could use larger samples to enable such an analysis. Fifth, the currently reported decrease in activation among WL patients, interpreted here as reflecting a habituation effect, may suggest that the attention task has low test-retest reliability. Although the accuracy and RT measures derived from the task indicate adequate reliability, correlations between pre- and post-scans in WL patients suggest low reliability. Unfortunately, low test-retest reliability often characterizes fMRI tasks, and call for the development of more stable and reliable measures (Bennett & Miller, Reference Bennett and Miller2010; Elliott et al., Reference Elliott, Knodt, Ireland, Morris, Poulton, Ramrakha and Hariri2020; Noble, Scheinost, & Constable, Reference Noble, Scheinost and Constable2019, Reference Noble, Scheinost and Constable2021). Future studies may wish to test long-term functional changes of GC-MRT using additional follow-up measurements. Previous findings indicate long-term clinical effects for GC-MRT (Lazarov et al., Reference Lazarov, Pine and Bar-Haim2017), which could be mirrored by certain sustained neural effects over time. Lastly, considering that SAD has been associated with aberrant patterns of neural connectivity during social threat processing (Evans, Bar-Haim, Fox, Pine, & Britton, Reference Evans, Bar-Haim, Fox, Pine and Britton2020; Gold et al., Reference Gold, Shechner, Farber, Spiro, Leibenluft, Pine and Britton2016; Gorka et al., Reference Gorka, Fitzgerald, Labuschagne, Hosanagar, Wood, Nathan and Phan2015; Pantazatos et al., Reference Pantazatos, Talati, Schneier and Hirsch2014; Sequeira et al., Reference Sequeira, Rosen, Silk, Hutchinson, Allen, Jones and Ladouceur2021), future studies could extend the current findings by testing whether GC-MRT induces changes in the functional associations between different brain regions. Such studies may focus on the connectivity between the regions described here as functionally changing following GC-MRT, their connectivity with the limbic system (Brühl et al., Reference Brühl, Delsignore, Komossa and Weidt2014; Etkin & Wager, Reference Etkin and Wager2007; Sylvester et al., Reference Sylvester, Corbetta, Raichle, Rodebaugh, Schlaggar, Sheline and Lenze2012; Xu et al., Reference Xu, Van Dam, Feng, Luo, Ai, Gu and Xu2019), and the relations between these connectivity patterns and SAD symptom change.
In conclusion, the current study shows that both GC-MRT and SSRI are effective treatments for SAD and lead to changes in brain function during implicit social threat processing. These changes take place in brain regions associated with attention control and inhibitory functions, supporting the role of such basic cognitive processes in the maintenance of SAD symptoms. The results also highlight the potential of targeting these neuro-cognitive processes through focused therapeutic interventions. The results further suggest treatment-specific neural pathways of clinical change in the ACC and dlPFC, suggesting that patients with SAD who do not fully benefit from SSRIs or GC-MRT may potentially benefit from the alternative treatment, or from a combination of the two.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291724001521.
Funding statement
The study was partially funded by JOY Ventures, Grant# R01- 30-2017-8156 and NIMH-Intramural Project, ZIAMH002781.
Competing interests
The authors report no potential conflicts of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.






 Open access
Open access