


No CrossRef data available.
Article contents
- Abstract
- Introduction
- Historical and scientific basis for instituting contact precautions for patients with proven or suspected SARS-CoV-2 infection at onset of the COVID-19 pandemic
- Subsequent data supports airborne and droplet but not fomite transmission of SARS-CoV-2
- The consequences of ongoing contact precautions for patients with COVID-19
- Proposed future steps
- Financial support
- Competing interests
- References
Discontinuing contact precautions for COVID-19: the science says its time
Published online by Cambridge University Press: 05 June 2026
Article contents
- Abstract
- Introduction
- Historical and scientific basis for instituting contact precautions for patients with proven or suspected SARS-CoV-2 infection at onset of the COVID-19 pandemic
- Subsequent data supports airborne and droplet but not fomite transmission of SARS-CoV-2
- The consequences of ongoing contact precautions for patients with COVID-19
- Proposed future steps
- Financial support
- Competing interests
- References
Abstract
The Centers for Disease Control and Prevention has recommended contact precautions for healthcare personnel caring for COVID-19 patients since the beginning of the pandemic. However, current scientific evidence points to transmission through small respiratory droplets or aerosols and not contaminated fomites as the dominant routes of transmission of SARS-CoV-2. We believe science shows there is no benefit and thus only negative consequences to patients, the environment, and the U.S healthcare system associated with ongoing contact precautions for patients with SARS-CoV-2 infection, and we advocate for updated guidelines reflecting current science.
Information
- Type
- Commentary
- Information
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution and reproduction, provided the original article is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution and reproduction, provided the original article is properly cited.- Copyright
- © The Author(s), 2026. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
References
Cai, J, Sun, W, Huang, J, Gamber, M, Wu, J, He, G. Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020. Emerg Infect Dis 2020;26:1343–1345.CrossRefGoogle ScholarPubMed
Pastorino, B, Touret, F, Gilles, M, de Lamballerie, X, Charrel, RN. Prolonged infectivity of SARS-CoV-2 in fomites. Emerg Infect Dis 2020;26:2256–2257.CrossRefGoogle ScholarPubMed
Doremalen van, N, Bushmaker, T, Morris, DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New England Journal of Medicine 2020;382:1564–1567.CrossRefGoogle Scholar
Lewis, D. COVID-19 rarely spreads through surfaces. So why are we still deep cleaning? Nature 2021;590:26–28.CrossRefGoogle ScholarPubMed
National Center for Chronic Disease Prevention and Health Promotion (U.S.). Division of diabetes translation. interim infection prevention and control recommendations for patients with suspected or confirmed coronavirus disease 2019 (COVID-19) in healthcare settings: March 19, 2020. https://stacks.cdc.gov/view/cdc/86043. Published March 19, 2020. Accessed February 27, 2026.Google Scholar
Centers for Disease Control and Prevention. Centers for disease control and prevention. Infection control guidance: SARS-CoV-2. https://www.cdc.gov/covid/hcp/infection-control/index.html. Published June 24, 2024. Accessed February 21, 2026.Google Scholar
Katelaris, AL, Wells, J, Clark, P, et al. Epidemiologic evidence for airborne transmission of SARS-CoV-2 during church singing, Australia, 2020. Emerg Infect Dis 2021;27:1677–1680.CrossRefGoogle ScholarPubMed
Shen, Y, Li, C, Dong, H, et al. Community outbreak investigation of SARS-CoV-2 transmission among bus riders in Eastern China. JAMA Intern Med 2020;180:1665–1671.CrossRefGoogle ScholarPubMed
Buonanno, G, Morawska, L, Stabile, L. Quantitative assessment of the risk of airborne transmission of SARS-CoV-2 infection: prospective and retrospective applications. Environ Int 2020;145:106112.CrossRefGoogle ScholarPubMed
Centers for Disease Control and Prevention. Science brief: SARS-CoV-2 and surface (Fomite) transmission for indoor community environments, 2021. https://stacks.cdc.gov/view/cdc/104762. Published March 24, 2021. Accessed February 27, 2026.Google Scholar
Kutter, JS, de Meulder, D, Bestebroer, TM, et al. SARS-CoV and SARS-CoV-2 are transmitted through the air between ferrets over more than one meter distance. Nat Commun 2021;12:1653.CrossRefGoogle ScholarPubMed
Port, JR, Yinda, CK, Owusu, IO, et al. SARS-CoV-2 disease severity and transmission efficiency is increased for airborne compared to fomite exposure in Syrian hamsters. Nat Commun 2021;12:4985.CrossRefGoogle ScholarPubMed
Siddiqui, ZK, Conway, SJ, Abusamaan, M, et al. Patient isolation for infection control and patient experience. Infect Control Hosp Epidemiol 2019;40:194–199.CrossRefGoogle ScholarPubMed
Mehrotra, P, Croft, L, Day, HR, et al. Effects of contact precautions on patient perception of care and satisfaction: a prospective cohort study. Infect Control Hosp Epidemiol 2013;34:1087–1093.CrossRefGoogle ScholarPubMed
Guilley-Lerondeau, B, Bourigault, C, Guille des Buttes, AC, Birgand, G, Lepelletier, D. Adverse effects of isolation: a prospective matched cohort study including 90 direct interviews of hospitalized patients in a French University Hospital. Eur J Clin Microbiol Infect Dis 2017;36:75–80.CrossRefGoogle Scholar
Morgan, DJ, Pineles, L, Shardell, M, et al. The effect of contact precautions on healthcare worker activity in acute care hospitals. Infect Control Hosp Epidemiol 2013;34:69–73.CrossRefGoogle ScholarPubMed
Martin, EM, Russell, D, Rubin, Z, et al. Elimination of routine contact precautions for endemic MRSA and VRE: a retrospective quasi-experimental study. Infect Control Hosp Epidemiol 2016;37:1323–1330.CrossRefGoogle Scholar
Martin, E, Morgan, DJ, Pryor, R, Bearman, G. Contact precautions for MRSA and VRE: where are we now? A survey of the Society for Healthcare Epidemiology of America Research Network. Antimicrob Steward Healthc Epidemiol 2024;4:e137.CrossRefGoogle Scholar
Stern, RA, Bashaw, K, Shackelford, CE, Talbot, TR. The unintended burden of transmission-based precautions for suspected COVID-19 in the ambulatory setting. Infect Control Hosp Epidemiol 2025;46:951–953.CrossRefGoogle ScholarPubMed
Stern, RA, Bashaw, K, Talbot, TR. Isolating the burden of transmission-based precautions for COVID-19: walk-in clinic-based healthcare personnel perspectives. Infect Control Hosp Epidemiol 2025;46:959–960.CrossRefGoogle ScholarPubMed
Novo, MAFM, Silva, LFDO, dos Alves D.F., S, Wachholz, PA, dos Nunes-Nogueira, VS. A microcost analysis of the use of personal protective equipment during and before the COVID-19 pandemic from a hospital perspective. Value Health Reg Issues 2024;42:100984.CrossRefGoogle ScholarPubMed
Bureau of Labor Statistics. CPI inflation calculator. U.S. Department of Labor. https://www.bls.gov/data/inflation_calculator.htm. Accessed February 27, 2026.Google Scholar
INTCO Medical. INTCO medical gets dual certifications for gloves. https://www.intcomedical.com/news/info/INTCO-Medical-Achieves-Dual-LCA-Carbon-Footprint-Certifications.html. Published July 16, 2025. Accessed February 27, 2026.Google Scholar
Medline Industries LP. Medline disposable open-back SMS cover gown (NON27SMS5). https://www.medline.com/ce/product/Medline-Disposable-OpenBack-SMS-Cover-Gown/Z05-PF129591?sku=MDPNON27SMS5. Accessed March 12, 2026.Google Scholar
Rodriguez-Nava, G, Diekema, DJ, Salinas, JL. Reconsidering the routine use of contact precautions in preventing the transmission of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) in healthcare settings. Infect Control Hosp Epidemiol 2023;44:1035–1037.CrossRefGoogle ScholarPubMed
Rabin, AS, Marr, LC, Blumberg, HM. Doff Thy Gown—shedding contact precautions for COVID-19. Clin Infect Dis 2024;79:585–587.CrossRefGoogle ScholarPubMed
Washington State Department of Health. COVID-19 Personal Protective Equipment (PPE) Recommendations for Healthcare Personnel (DOH 420-665). https://doh.wa.gov/sites/default/files/2025-06/420-665-WA-HCP-COVID19-PPERecommendations.pdf. Accessed February 27, 2026.Google Scholar
Victorian Department of Health. COVID-19 infection prevention and control guidelines. https://www.health.vic.gov.au/covid-19-infection-prevention-control-guidelines/print-all. Accessed March 12, 2026.Google Scholar
Massachusetts Department of Public Health. COVID-19 PPE, testing, and resources. https://www.mass.gov/info-details/covid-19-ppe-testing-and-resources. Published 2026. Accessed May 3, 2026.Google Scholar
Sutjipto, S, Aung, AH, Soon, MML, et al. Plastic waste and COVID-19 incidence among hospital staff after deescalation in PPE use. JAMA Netw Open 2025;8:e255264.CrossRefGoogle ScholarPubMed
Centers for Disease Control and Prevention. Surveillance and data analytics: COVID-19. https://www.cdc.gov/covid/php/surveillance/index.html. Published March 19, 2026. Accessed May 3, 202.Google Scholar
Onakpoya, IJ, Heneghan, CJ, Spencer, EA, et al. SARS-CoV-2 and the role of fomite transmission: a systematic review. F1000Res 2021;10:233.CrossRefGoogle ScholarPubMed
ocha, ALS, Pinheiro, JR, Nakamura, TC, et al. Fomites and the environment did not have an important role in COVID-19 transmission in a Brazilian mid-sized city. Sci Rep 2021;11:15960.Google Scholar
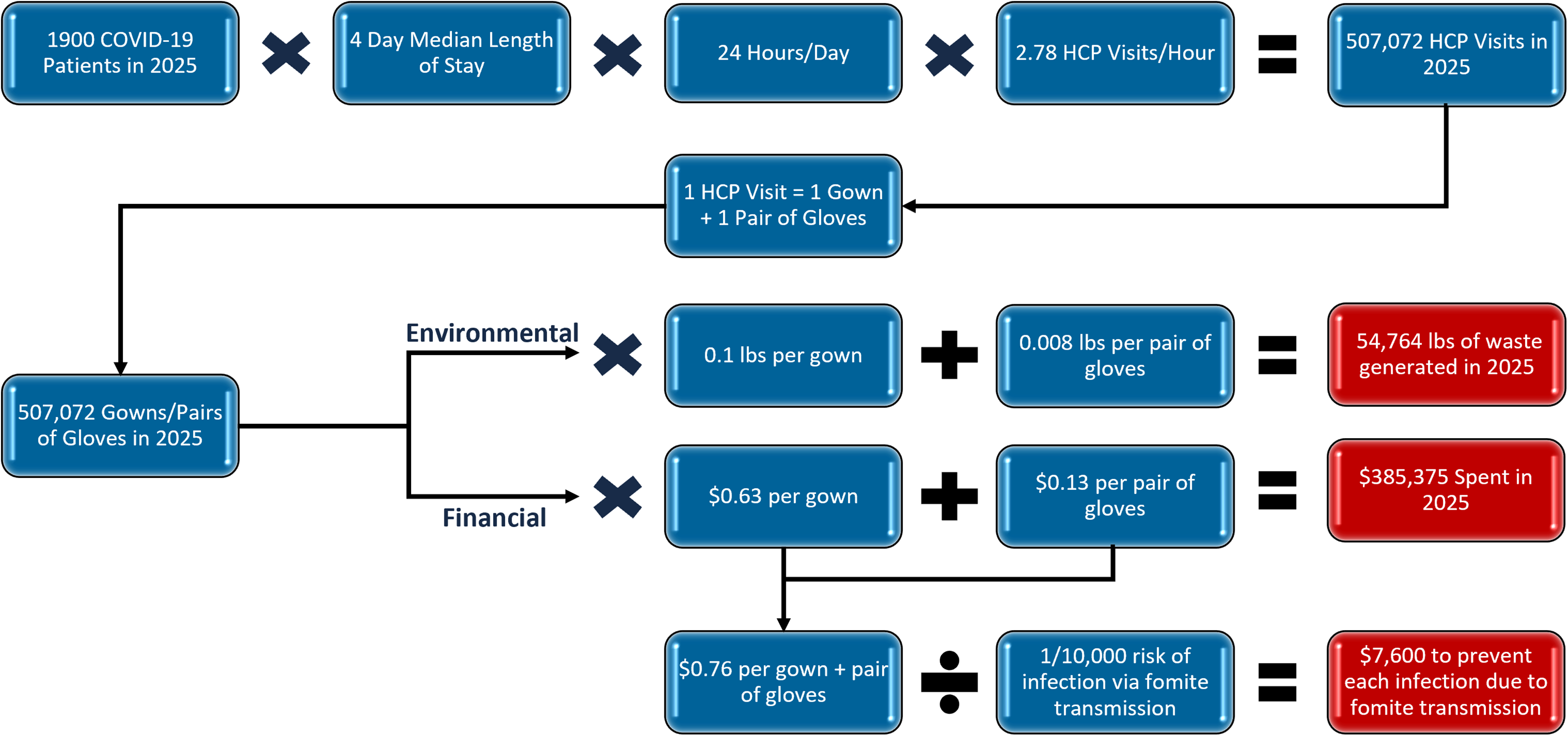
Figure 1. Figure 1 long description.Financial & environmental impact of COVID-19 contact precautions at UC San Diego Health in 2025.
 You have
Access
You have
Access
 Open access
Open access
Introduction
The COVID-19 pandemic prompted a worldwide effort to understand the pathogenicity and transmission of a new virus at unprecedented speed. With limited data, the Centers for Disease Control and Prevention (CDC) provided guidance on how to minimize the transmission of infection. Consistent with previous outbreaks of high consequence and novel respiratory viruses, the CDC wisely recommended a comprehensive strategy including usage of an N95 respirator, eye protection, and contact precautions (gowns and gloves) to prevent the transmission of SARS-CoV-2 in the healthcare setting at the beginning of the COVID-19 pandemic before the routes of transmission had been fully elucidated. Three years after the end of the pandemic was declared, we posit that there is ample data to remove contact precautions from national and state guidelines. In this commentary, we explore the historical and scientific basis for the initial COVID-19 contact precaution recommendation, subsequent data emphasizing respiratory droplet and aerosol transmission, the consequences of the ongoing use of contact precautions, and propose a streamlined guide to safely care for patients with COVID-19.
Historical and scientific basis for instituting contact precautions for patients with proven or suspected SARS-CoV-2 infection at onset of the COVID-19 pandemic
Early in the pandemic, the method of transmission of SARS-CoV-2 was unclear, with early research suggesting that fomites could be a significant source of transmission. Reference Cai, Sun, Huang, Gamber, Wu and He1–Reference Doremalen van, Bushmaker and Morris3 For this reason, the CDC recommended in March 2020 that healthcare personnel (HCP) treating patients with suspected or proven COVID-19 adhere to both modified airborne and contact precautions, i.e., an N95 respirator, gown, gloves, and eye protection. Reference Lewis4,5 By May of 2020, however, the CDC determined fomites to be an unlikely route of transmission, but difficulty in completely ruling out fomite transmission led to an abundance of caution. Six years later, this CDC infection-control recommendation driving healthcare policy for patients with suspected or proven COVID-19 remains in effect and is widely followed by US hospitals. 6
Subsequent data supports airborne and droplet but not fomite transmission of SARS-CoV-2
Understanding of the transmission of SARS-CoV-2 has evolved. For example, clinical studies evaluating “superspreader” events have provided compelling evidence for airborne and droplet transmission through identifications of patterns of transmission based on spatial clustering in poorly ventilated environments. Reference Katelaris, Wells and Clark7,Reference Shen, Li and Dong8 Similarly, quantitative modeling analysis of these same events has demonstrated that aerosols are the main route of transmission, with the risk of infection via fomite estimated to be less than 1 in 10,000. Reference Buonanno, Morawska and Stabile9,10 Likewise, animal studies evaluating transmission of SARS-CoV-2 have consistently demonstrated that while transmission via fomite is theoretically possible, airborne and droplet are by far the dominant routes of transmission and result in more severe disease. Reference Kutter, de Meulder and Bestebroer11,Reference Port, Yinda and Owusu12
The consequences of ongoing contact precautions for patients with COVID-19
Given negligible fomite transmission, contact precautions are not protecting HCP or patients from contracting COVID-19; rather, contact precautions are having detrimental effects. Studies of patients on contact precautions for multidrug-resistant organisms (MDRO) report lower staff responsiveness (63% vs 51%) and more problems with inpatient care. Patients on contact precautions are three times less likely to be satisfied with healthcare worker assistance compared with patients not on contact precautions. Reference Siddiqui, Conway and Abusamaan13–Reference Guilley-Lerondeau, Bourigault, Guille des Buttes, Birgand and Lepelletier15 They also have fewer visitors when compared to patients not on contact precautions and have higher in-hospital anxiety scores. Reference Guilley-Lerondeau, Bourigault, Guille des Buttes, Birgand and Lepelletier15,Reference Morgan, Pineles and Shardell16 Additionally, HCP are less likely to interact with patients on contact precautions (2.78 vs 4.37 visits per hour). Reference Morgan, Pineles and Shardell16 This may be, at least in part, due to the time needed to don and doff gowns, which was estimated to take 45,277 hours/year for two California hospitals according to a 2016 study by Martin et al. Reference Martin, Russell and Rubin17 These observations have contributed to the rationale for many US healthcare institutions to stop requiring contact precautions for highly endemic methicillin-resistant Staphylococcus aureus or vancomycin-resistant Enterococcus. Reference Martin, Morgan, Pryor and Bearman18
These detrimental effects are not limited to the inpatient setting. The requirement to don and doff personal protective equipment (PPE) for confirmed or suspected COVID-19 has been estimated to add 3.9 minutes per outpatient encounter. Reference Stern, Bashaw, Shackelford and Talbot19 In a recent survey of HCP practicing at walk-in clinics, 54% reported that isolation precautions increased burden on HCP, 69% reported increased time required per patient encounter due to donning and doffing of PPE, and 46% reported that PPE increased difficulty associated with collection and management of specimens. Reference Stern, Bashaw and Talbot20
There are also financial and environmental impacts of contact precautions for patients with suspected or proven COVID-19. Based on data for our academic institution, we estimate the added financial cost of utilizing gowns and gloves to care for 1900 patients admitted with COVID-19 in 2025 was $385,375 (Figure 1). Reference Novo, Silva, dos Alves D.F., Wachholz and dos Nunes-Nogueira21,22 To assess the environmental cost, we estimated the waste produced and calculated that this practice generated 54,764 pounds of discarded gloves and gowns at our institution in 2025. 23,24 These figures reflect the burden at a single hospital system; when extrapolated across the entire healthcare system the financial and environmental cost of contact precautions for patient with suspected or proven COVID-19 would be magnified many fold. Furthermore, this policy is not cost-efficient. We estimate $7,600 would need to be spent on gowns and gloves to prevent a single case of COVID-19 transmitted via fomite. Admittedly, these calculations rely heavily on generalized assumptions and lack nuance; nonetheless, because this analysis does not account for usage of gowns and gloves by visitors of patients with COVID-19, costs of waste disposal, or usage of gowns and gloves in the outpatient setting, these results certainly underestimate the true cost of this policy.
Financial & environmental impact of COVID-19 contact precautions at UC San Diego Health in 2025.
Figure 1. Long description
There were 1900 patients hospitalized with COVID-19, each with a median length of stay of 4 days and an average of 2.78 healthcare personnel (HCP) visits per hour, corresponding to 507,072 HCP visits annually. Each visit required one gown and one pair of gloves. At 0.1 lb per gown and 0.008 lb per pair of gloves, this resulted in an estimated 54,764 lb of waste. The per-unit costs are $0.63 per gown and $0.13 per pair of gloves, totaling $385,375 annually. The combined cost per patient⏧HCP interaction is $0.76. Assuming a fomite transmission risk of 1 in 10,000 per encounter, the estimated cost to prevent one infection via fomite transmission is $7,600.
Proposed future steps
Discontinuation of the routine use of contact precautions for patients with SARS-CoV-2 is unlikely to be considered a radical policy change in 2026, with experts having called for reconsideration of this practice since 2023. Reference Rodriguez-Nava, Diekema and Salinas25,Reference Rabin, Marr and Blumberg26 Many countries (e.g. Australia, The European Union, and Singapore) and some U.S. states have already relaxed contact precautions; both the Massachusetts and Washington Departments of Health now recommend the routine use of gowns and gloves only when contact with potentially infectious material is anticipated. Reference Rabin, Marr and Blumberg26–29 While subsequent data from this policy change are limited, a single retrospective study from Singapore showed discontinuation of contact precautions resulted in significant cost and environmental savings with no increase in infection rate among HCP or patients. Reference Sutjipto, Aung and Soon30 A similar outcome would be anticipated in the United States, where CDC surveillance and data analytics demonstrate substantially decreased test positivity, emergency room visits due to COVID-19, hospitalization rates, and deaths due to COVID-19 in 2026 when compared to rates from the peak of the pandemic. 31 Collectively, these data suggest that SARS-CoV-2 infection is currently associated with lower transmission and clinical severity, further reducing the likelihood that relaxation of contact precautions would result in increased nosocomial transmission and harm. Such a policy change would align with influenza infection control practices. Notably, viable influenza virus can be recovered from environmental surfaces at low levels, whereas no published studies have demonstrated recovery of viable SARS-CoV-2 from fomites. Reference Onakpoya, Heneghan and Spencer32,Reference ocha, Pinheiro and Nakamura33
We recommend the thoughtful discontinuation of contact precautions for COVID-19. At a health-system level, prospective monitoring of hospital-onset COVID-19 should be continued. At county and state agencies, systems should collect data and analyze and respond if hospital-onset clusters of SARS-CoV2 infection rates among HCP or patients occur without an increase in the prevalence in the community.
In summary, CDC guidance at the start of the pandemic was thoughtful and appropriately cautious in the face of a novel and lethal respiratory pathogen. However, our understanding of SARS-CoV-2 transmission has evolved since the beginning of the pandemic. For the sake of the environment, the financial viability of our healthcare system, and our HCPs, patients, and visitors, we should no longer mandate contact precautions for patients with suspected or confirmed COVID-19. The science says it’s time.
Acknowledgements
None.
Financial support
The authors declare that they have no competing interests, financial, or nonfinancial disclosures.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. DMS has consulted for Hyundai Biosciences, Model Medicines, Pfizer, and Gilead.