


Introduction
Facing the COVID-19 pandemic led to experiencing great emotional anxiety and distress (Ahmad et al., Reference Ahmad, Mazhar, Almerico and Senes2025), with an increase in depression (Santosha et al., Reference Santosha, Tiwari, Chand, Dikkatwar, Roy and Bindu2025). However, not everyone developed anxiety and depression during the pandemic, and some people even experienced post-traumatic growth after the pandemic ended (Berg et al., Reference Berg, Lin, Beebe and Ondrasek2024). These results suggest that there were moderating or mediating factors that were able to buffer the negative effects of the pandemic. One factor that has been shown to mediate and protect against psychopathology during confinement was the ability to engage in meaning making in adverse situations during the COVID-19 pandemic (Vieveen et al., Reference Vieveen, Yildiz, Korfage, Witkamp, Becqué, van Lent, Pasman, Zee, Onwuteaka-Philipsen, van der Heide and Goossensen2025).
The study of meaning in life as a protective factor was originally proposed by Viktor Frankl (Reference Frankl1959/1985), who suggested that meaning in life is the fundamental motivational force of human beings and a prerequisite for personal self-realization. Meaning in life includes the facets of mattering, purpose, and coherence in life, and it is related to the perception of responsibility in one’s life (Martela & Steger, Reference Martela and Steger2016). There is a certain consensus in the specialized literature that meaning in life is composed of two dimensions: Presence of meaning in life and the search for meaning in life (Steger et al., Reference Steger, Frazier, Oishi and Kaler2006). On the one hand, the presence of meaning is an experience in which a person understands the meaning of their life and feels that it is significant. This experience leads them to feel a sense of purpose, authenticity, and an understanding of their place in the world. It makes it possible to conceptualize how individuals understand themselves, the world, and their relationship with the world (He et al., Reference He, Wang, Steger, Ji, Jing, Liu and Ye2023; Steger et al., Reference Steger, Kashdan, Sullivan and Lorentz2008). On the other hand, the search for meaning refers to individuals’ dynamic and active effort to establish and/or increase their understanding of meaning, purpose, and the importance of their lives (Steger et al., Reference Steger, Kashdan, Sullivan and Lorentz2008).
Previous studies confirmed that greater feelings of the presence of meaning in life are positively associated with better physical health outcomes, including longevity, across countries, measures, and time frames (Sutin et al., Reference Sutin, Luchetti, Karakose, Stephan and Terracciano2025), and that the presence of meaning is negatively related to depressive and anxious symptoms (He et al., Reference He, Wang, Steger, Ji, Jing, Liu and Ye2023), suicide risk (Deska et al., Reference Deska, Mirocha, Bak, Mirgos-Wierzchowska, Kosmalski, Rozycka-Kosmalska and Pietras2025), and psychopathology and suicidal ideation (Marco et al., Reference Marco, Cañabate, Pérez and Llorca2017). These findings have been consistent across all studies, suggesting that the presence of meaning has been shown to help individuals improve their expectations and hopes and cope with negative situations by reducing symptoms of depression and anxiety (He et al., Reference He, Wang, Steger, Ji, Jing, Liu and Ye2023). Moreover, individuals who have a clear sense of meaning experience wellbeing and the potential to thrive despite adverse events (Elemo et al., Reference Elemo, Kara and Rostamzadeh2024; Newman et al., Reference Newman, Schneider and Stone2022). With regard to the COVID-19 pandemic, several studies have found that high levels of presence of meaning reduced fear of COVID-19 (e.g., Baños et al., Reference Baños, Desdentado, Vara, Escrivá-Martínez, Herrero, Miragall and Tomás2023). One possible explanation for the protective effect of the presence of meaning could be thought of as positive affect (Guo et al., Reference Guo, Yang, He, Tian, Wang, Zhang, Liu, Liu, Zhu and Wu2024), given that the presence of meaning predicts positive affect (Barnett et al., Reference Barnett, Moore and Garza2019) and positive affect is a predictor of mental health and well-being during the COVID-19 pandemic (Minihan et al., Reference Minihan, Songco, Fox, Ladouceur, Mewton, Moulds, Pfeifer, Van Harmelen and Schweizer2024).
Regarding the search for meaning, previous studies show that it is related to depression, anxiety, and distress (He et al., Reference He, Wang, Steger, Ji, Jing, Liu and Ye2023; Steger et al., Reference Steger, Frazier, Oishi and Kaler2006). Seekers of meaning report worse relationships and lower self-acceptance, and they are more anxious, ruminative, and unhappy about their past and present experiences (Steger et al., Reference Steger, Kashdan, Sullivan and Lorentz2008). Furthermore, when people search for meaning and do not find it, they are at risk of developing psychopathology and even suicidal tendencies (Steger, Reference Steger2022). Previous studies consistently found that the search for meaning predicts negative affect (Barnett et al., Reference Barnett, Moore and Garza2019; Newman et al., Reference Newman, Schneider and Stone2022). Thus, it is possible that negative effect is a consequence of the search for meaning (Guo et al., Reference Guo, Yang, He, Tian, Wang, Zhang, Liu, Liu, Zhu and Wu2024; Newman et al., Reference Newman, Nezlek and Thrash2018) and a predictor of mental health problems during the COVID19 pandemic (Minihan et al., Reference Minihan, Songco, Fox, Ladouceur, Mewton, Moulds, Pfeifer, Van Harmelen and Schweizer2024).
An appropriate framework with which to understand how meaning in life acts as a protective factor against unforeseen events is the Meaning Making Model (MMM) (Park, Reference Park2010). The MMM differentiates between global meaning and situational meaning. Global meaning refers to an individual’s general orienting system—the broader beliefs, goals, and sense of purpose that shape the way they view the world and interpret life experiences overall. Situational meaning refers to the meaning assigned to a specific event or situation—how a person interprets and makes sense of a particular instance in light of their global meaning system.
This model suggests that when global meaning is violated by a highly stressful or traumatic event, meaning-making processes are activated, forming a new situational meaning. Therefore, the person will adapt to the situation if the new situational meaning is congruent with the global meaning because this will result in the presence of meaning, which will buffer clinical symptoms. However, if the new meaning is incongruent with the global meaning, the person will experience negative emotions (including depression, emptiness, and distress) (Dalgleish, Reference Dalgleish2004; Everly & Lating, Reference Everly and Lating2004; Milman et al., Reference Milman, Lee, Neimeyer, Mathis and Jobe2020). These emotions lead the person to activate meaning-search processes (which will increase distress, anxiety, and negative affect) until they find a new situational meaning that is congruent with the global meaning. When the new situational meaning is congruent with the global meaning, the presence of meaning occurs, and so the search for meaning is reduced. This presence of meaning would be associated with positive affect (Park, Reference Park2010).
Previous studies based on the MMM have confirmed its utility. For example, Chen et al. (Reference Chen, Wang, He, Ji, Liu and Ye2021), in a sample with high school students, found that the search for meaning acts through two pathways: directly (search increases depressive symptoms) and indirectly (through presence, the search decreases depressive symptoms). Additionally, Negri et al. (Reference Negri, Conte, Caldiroli, Neimeyer and Castiglioni2023) found that participants whose core beliefs were more violated by the pandemic experienced worse mental health conditions.
According to the previously mentioned studies, the models that have attempted to explain the relationship between traumatic, stressful events’ meaning and clinical symptoms have been conducted in a piecemeal fashion (Park, Reference Park2022). The studies carried out using the MMM to explain the relationship between traumatic or stressful events and clinical symptoms have been two-pathway models (e.g., Chen et al., Reference Chen, Wang, He, Ji, Liu and Ye2021). However, according to the previous studies, we could hypothesize that the relationship between the violation of global meaning and clinical symptoms could be better explained through a three-pathway model with several mediating variables: (a) The violation of global meaning directly predicts anxiety and depression; (b) The violation of global meaning indirectly, through searching for meaning and negative affect, increases clinical symptoms; and (c) The violation of global meaning indirectly, through the presence of meaning and positive affect, buffers clinical symptoms. However, although previous studies suggest these three pathways, the adequacy of this three-pathway model has not yet been verified.
Thus, in order to develop prevention programs or improve current psychological treatments for people facing unforeseen and traumatic events, it is necessary to confirm whether a three-way model could explain the relationships between the violation of global meaning after an unforeseen event and clinical symptoms such as depression, anxiety, and somatization better than two-way models (Park et al., Reference Park2016).
The objective of this study is to analyze which model (two-pathway model vs three-pathway model) has a better fit in explaining the association between the violation of global meaning and clinical symptoms such as somatization, anxiety, and depression in participants during the COVID-19 pandemic.
Method
Participants
The study sample consisted of N = 1106 participants with an age mean of 34.70 (SD = 12.07). A total of 59.9%, n = 663, of the participants were residents of Spain, whereas 40.1%, n = 443, resided in South American countries. Regarding gender, 77.3%, n = 854, were women, and 22.7%, n = 252, were men, and all of them were Spanish speaking. Regarding sociodemographic characteristics: 69.2%, n = 765, were working, and 30.8%, n = 341, were students. Regarding marital status, 55.2%, n = 611, were married, and 54.8%, n = 495, were single, divorced, or widowed. Moreover, 57.9%, n = 640, had children, and 42.1%, n = 466, did not. Regarding clinical characteristics, 83.9% (n = 928) had not been diagnosed with any illness other than COVID-19, whereas 16.1% (n = 178) had. A total of 86.6% (n = 958) had not been diagnosed with a mental disorder, whereas 13.4% (n = 148) had been diagnosed with mental disorders. Participants had been in mandatory quarantine for 38.91 (49.08) days.
Procedure
The inclusion criteria for the study were: being over 18 years old and a Spanish speaker. The sample was collected through an online survey created ad hoc by the research team. The snowball sampling technique was used. The procedure for collecting the sample was as follows. The research team shared the survey with their colleagues and students from the undergraduate and master’s programs they taught. These contacts committed to recruiting five people each, who were then invited to participate in the research. The evaluation protocol was active for 1 year, starting in May 2020 and ending in May 2021. During this period of the COVID-19 pandemic in Europe and America, lockdown measures were imposed. Participation was completely voluntary, and no compensation was provided. Before participating in the study, participants were asked to read an information sheet about the study, and if they agreed, they were asked to sign the informed consent. Additionally, the study was approved by the ethics committee of the University of Valencia with registration code 2551253.
Measures
Meaning in Life Questionnaire (MLQ)
The MLQ is a self-reported questionnaire made up of 10 items developed to assess the two main dimensions of meaning in life: Presence and Search for meaning in life. The items are rated on a 7-point scale ranging from 1 (absolutely false) to 7 (absolutely true). Each subscale is composed of five items. The subscale scores are calculated by using the sum of the items on each subscale (Steger et al., Reference Steger, Frazier, Oishi and Kaler2006). Higher scores indicate greater Presence and Search for meaning, respectively. In our sample, the two subscales have shown adequate reliability, with coefficients (α = 0.86) for the Presence subscale and (α = 0.93) for the Search subscale (Marco et al., Reference Marco, Privado, Guillen, Quero, Pérez, Baños and Tormo2022; Steger et al., Reference Steger, Frazier, Oishi and Kaler2006).
Brief Symptom Inventory-18 (BSI-18)
To measure psychological distress in the past 7 days, a 5-point Likert scale was used (0 = not at all; 4 = extremely). It consists of three subscales: Somatization (6 items), Depression (6 items), and Anxiety (6 items). The Spanish validation conducted by Andreu and colleagues (Reference Andreu, Galdon, Dura, Ferrando, Murgui, Garcia and Ibanez2008) was used. In our sample, the three subscales have shown adequate reliability, with coefficients (α = .88) for Depression, (α = 0.90) for Anxiety, and (α = 0.89) for Somatization (Derogatis, Reference Derogatis2000).
The Global Meaning Violation Scale (GMVS)
This instrument assesses the extent to which the participant feels that the event (e.g., COVID-19 pandemic) violates their global meaning regarding: the idea that the world is fair, that the world is controlled by God or other forces, that the participant is in control, or that the world is good and safe. Thus, it is a scale that measures global meaning according to the MMM (Park, Reference Park2010, Reference Park2016). It consists of three 7-point Likert scales (0 = not true at all; 6 = completely true): intrinsic goal disruption (5 items), global meaning disruption (5 items), and extrinsic goal disruption (3 items). However, for this study, only the global meaning disruption scale was used, which refers to beliefs such as security and justice. Because no validated Spanish version exists, an experimental ad hoc translated version was used for this study, and this version is being validated in parallel studies. In our sample, the GMVS subscale has shown adequate reliability, with a coefficient (α = 0.86) (Park et al., Reference Park2016).
The Positive and Negative Affect Scale (PANAS)
This is an instrument that measures both positive and negative affect. It consists of two 5-point Likert scales (1 = very slightly or not at all; 5 = extremely): positive affect (10 items) and negative affect (10 items). The score for each subscale is computed by summing the scores on each item, ranging from 10 to 50 points, with higher scores indicating a greater presence of the specific affect. The Spanish version and adaptation by López-Gómez and colleagues (Reference Lopez-Gomez, Hervas and Vazquez2015) was used. In our sample, the two subscales have shown adequate reliability, with coefficients (α = 0.92) for positive affect and (α = 0.87) for negative affect (Watson et al., Reference Watson, Clark and Tellegen1988).
Statistical Analysis
First, the distribution of the study measures, Pearson correlations, and internal consistency were calculated using Cronbach’s Alpha with the SPSS V. 23 statistical package. Second, two models were estimated: one model in which there were direct and indirect effects between schema violation and clinical symptoms through meaning in life and both positive and negative affect, and another model in which there were only indirect effects. The absolute goodness-of-fit indices used to measure the fit of the models to the empirical data were: χ2/df (Bentler & Bonett, Reference Bentler and Bonett1980), with values < 3 indicating a good fit; the Goodness-of-Fit Index (GFI) (Jöreskog & Sörbom, Reference Jöreskog and Sörbom1993), with values > 0.95 considered a good fit; the Standardized Root Mean Square Residual (SRMR) (Hooper et al., Reference Hooper, Coughlan and Mullen2008), with values < 0.08 indicating a good fit. The incremental fit indices that compared the resulting model with the null model were: the Normed Fit Index (NFI) (Bentler & Bonett, Reference Bentler and Bonett1980); values > 0.95 indicate good fit and that the empirical model is significantly different from the null model. Moreover, the parsimony indices that evaluated the fit of the examined model based on the number of estimators were the following: the Parsimony Goodness of Fit Index (PGFI) (Jöreskog & Sörbom, Reference Jöreskog and Sörbom1993) and the Parsimony Normed Fit Index (PNFI) (James et al., Reference James, Mulaik and Brett1982), with values > 0.50 indicating a good fit. The sample consisted of 1,297 participants to estimate eight indicators: 1297/8 = 162.13 ≈ 162 participants per indicator. This value significantly exceeds the recommended criteria of a minimum of 100 participants and 10 times the number of indicators (Byrne, Reference Byrne2001). These analyses were performed using AMOS V.7 (Arbuckle, Reference Arbuckle2006).
Patient and Public Involvement
The individuals comprising the sample were invited to participate via social media, where the objective of the study was explained and informed consent was obtained. Their participation was limited exclusively to completing the online questionnaires. No individuals other than the authors were involved in any other stages of the research process or in the writing of the manuscript.
Results
Descriptive statistics, internal consistency, and correlations. Table 1 shows the descriptive statistics (means and standard deviations) and the distribution (skewness and kurtosis) of the measures used. All the variables exhibit a normal distribution, given that no skewness greater than 2 or kurtosis greater than 7 in absolute value was found (West et al., Reference West, Finch, Curran and Hoyle1995). Regarding consistency (Cronbach’s α), all the measures present values greater than 0.70, which is considered the minimum acceptable level for the precision of a measure (Hair et al., Reference Hair, Anderson, Tatham and Black1999). As Table 1 reveals, Global meaning violation (GMVS) was highly and positively (Cohen, Reference Cohen1992) associated with Anxiety (r = .63; p < .001) and Somatization (BSI) (r = .57; p < .001), moderately associated with Depression (BSI) (r = .49; p < .001), Negative Affect (PANAS) (r = .48; p < .001), and Search (MLQ) (r = .45; p < .001), and marginally associated with Presence (MLQ) (r = .13; p < .001). Search for meaning was positively and moderately associated with Negative Affect (PANAS) (r = .44; p < .001), Anxiety (BSI) (r = .44; p < .001), Somatization (BSI) (r = .43; p < .001), and Depression (BSI) (r = .39; p < .001). Presence of Meaning was highly and positively associated with positive affect (PANAS) (r = .62; p < .001) and moderately and negatively associated with Depression (BIS) (r = .35; p < .001), and it had a low and negative association with negative affect (PANAS) (r = −.15; p < .001). Positive affect (PANAS) was negatively and moderately associated with depression (r = −.45; p < .001), and it had a low association with Negative Affect (PANAS), Anxiety (BSI) (r = −.23; p < .001), and Somatization (BSI) (r = −.19; p < .001). Negative Affect (PANAS) was highly and positively associated with Anxiety (r = −.78; p < .001), Depression (BSI) (r = −.69; p < .001), and Somatization (BSI) (r = −.67; p < .001). Somatization was highly and positively associated with Anxiety (r = .83; p < .001) and Depression (BSI) (r = .73; p < .001), and Anxiety was highly and positively associated with Depression (BSI) (r = .78; p < .001).
Descriptives, distribution, internal consistency, and Pearson correlations of the measures

Note. BSI = Brief Symptom Inventory–18; GMVS = Global Meaning Violation Scale; MLQ = Meaning in Life Questionnaire; PANAS = The Positive and Negative Affect Scale.
* = p < .05, ** p < .001.
Mediational Model
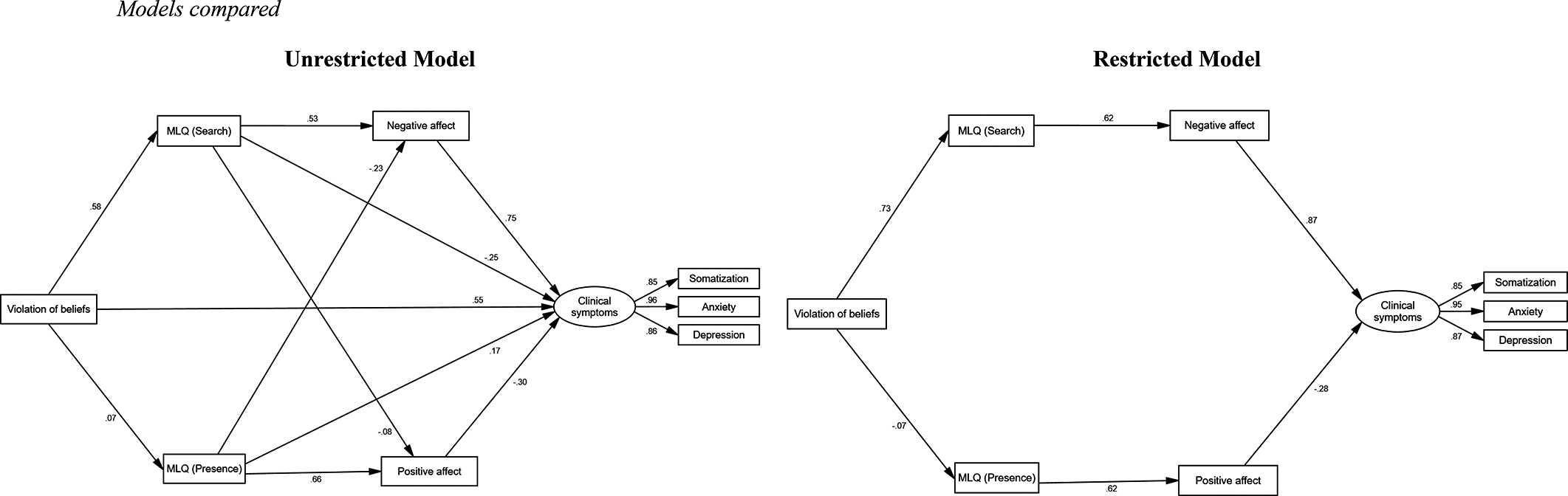
To estimate the two models, the procedure outlined by Holmbeck (Reference Holmbeck1997) and Ato and Vallejo (Reference Ato and Vallejo2011) was followed. One model included mediational (indirect) effects of meaning in life and affect between schema violation and clinical symptoms (restricted model), and the other model included both direct and indirect effects between these measures (unrestricted model). In both cases, the models were estimated using unweighted least squares, due to the lack of multivariate normality. This was determined because the bootstrap procedure by Bollen-Stine (Reference Bollen, Stine, Bollen and Long1993), which was used to test this assumption, was statistically significant (p = .005). Figure 1 shows the two models tested. The restricted model presents a moderate fit to the data (χ2/df = 65773.25, GFI = 0.961, NFI = 0.933, PGFI = 0.507, PNFI = 0.633, SRMR = 0.117), whereas the unrestricted model fits the data quite well (χ2/df = 36189.09, GFI = 0.984, NFI = 0.973, PGFI = 0.383, PNFI = 0.486, SRMR = 0.074). It should be noted that the χ2/df values are quite high in both models, due to the large sample size, which tends to increase the χ2 value.
Models compared.

When comparing the tested models, we found statistically significant differences between them based on the number of parameters (Δχ25 = 743044.25, p < .001). Therefore, we should opt for the unrestricted model (Ato & Vallejo, Reference Ato and Vallejo2011; Holmbeck, Reference Holmbeck1997). This model includes both direct and indirect effects between schema violation and clinical symptoms through meaning in life and affect. Additionally, the unrestricted model, as mentioned above, provides a better fit to the data.
According to Cohen’s (Reference Cohen1992) criteria for linear regression, a value of f 2 = R 2/(1 − R 2) of 0.02 represents a small effect size, 0.15 represents a medium effect size, and 0.35 represents a large effect size. By rearranging the formula for r, we find that r = .14 would indicate a small effect size, .36 a medium effect size, and .51 a large effect size. Taking these values as a reference, in the unrestricted model, we can see that schema violation directly influences search (meaning in life) (β = .58), but not presence (meaning in life). Additionally, schema violation explains clinical symptoms (β = .55). Search influences negative affect (β = .53) and clinical symptoms (β = −.25). Presence influences negative affect (β = −.23), positive affect (β = .66), and clinical symptoms (β = .17). Affect influences clinical symptoms (β = .75 for negative affect, β = −.30 for positive affect). Furthermore, schema violation, in addition to the direct effect on clinical symptoms, presents an indirect effect through search and negative affect. All the measures together explain 90% of the variance in clinical symptoms (R 2 = 0.90).
Discussion
The objective of this study was to analyze which model (two-pathway model vs three-pathway model) has a better fit in explaining the association between the violation of global meaning and clinical symptoms such as somatization, anxiety, and depression in participants during the COVID-19 pandemic.
The results suggest that the violation of schemas affects depression and anxiety symptoms through three pathways: (a) Path one, directly, schema violation explains clinical symptoms; (b) Path two, indirectly, schema violation explains clinical symptoms through the search for meaning and negative effect; and (c) Path three, the presence of meaning explains positive affect and buffers clinical symptoms. The three-pathway model of the association between violation of schemas and psychopathology explains 90% of the variance in clinical symptoms.
Regarding the first pathway, we found that the violation of global meaning directly predicts symptoms of anxiety and depression. This result confirms the study by Negri et al (Reference Negri, Conte, Caldiroli, Neimeyer and Castiglioni2023), which found that those whose core beliefs were more violated by the pandemic had worse mental health conditions. Second, our results confirm previous studies that found that the search for meaning had a direct effect on increasing symptoms of depression and anxiety (Chen et al., Reference Chen, Wang, He, Ji, Liu and Ye2021), and that the search for meaning and negative affect were positively associated in participants during the COVID-19 pandemic (Newman et al., Reference Newman, Schneider and Stone2022). Therefore, we can suggest that this path (search-negative affect-clinical symptoms) is consistent across different samples and different countries. Moreover, our study confirms a result that has been repeated in many previous studies, namely, the protective effect of the presence of meaning against depression (Steger, Reference Steger2022). However, we have suggested that the mediator between presence and depression symptoms is positive affect, and so the second pathway (presence-positive affect-clinical symptoms) has also been confirmed. Our results are consistent with previous studies carried out during the COVID-19 pandemic (Elemo et al., Reference Elemo, Kara and Rostamzadeh2024; Steger, Reference Steger2022), and they confirm the usefulness of the MMM (Park, Reference Park2010) in explaining the relationship between coping with an unforeseen event and clinical symptoms.
We found that the presence of meaning and the search for meaning were not associated. This result is similar to a previous study that indicated that there were two independent dimensions of meaning (Damasio & Koller, Reference Damasio and Koller2015; Góngora & Solano, Reference Góngora and Solano2011). However, our results are contrary to Chen et al. (Reference Chen, Wang, He, Ji, Liu and Ye2021), who found a moderate association in Chinese students, or Elemo et al. (Reference Elemo, Kara and Rostamzadeh2024), who found a high and positive association in Iranian participants. There is a broad consensus in specialized research about the cultural differences in the relationship between presence and search for meaning (Steger et al., Reference Steger, Frazier, Oishi and Kaler2006). Because our samples belong to Anglo-Saxon countries, the relationship between presence and search is minimal or non-existent (Newman et al., Reference Newman, Schneider and Stone2022; Steger et al., Reference Steger, Frazier, Oishi and Kaler2006).
Our results showed that the violation of global meaning is moderately and positively associated with the search for meaning. This result is consistent with previous studies that found that the disruption of global meaning triggers a meaning-making process (Park, Reference Park2016). If a new situational meaning is incongruent with the global meaning, negative affect develops, and if this fruitless search persists, symptoms of anxiety and depression appear. Similarly, we found that schema violation is marginally associated with the presence of meaning. This result is consistent with the MMM model (Park, Reference Park2010), given that it is possible that, after an unexpected event, participants develop a new situational meaning that is congruent with the global meaning, which produces adequate adaptation after the disruption of global meaning (Park Reference Park2022).
The confirmation of the three-pathway model could have important theoretical and clinical implications. Theoretically, we have presented a new three-pathway model that explains the relationship between global meaning violations and anxiety and depression symptoms through two mediators: the search for and presence of meaning and positive and negative affect. This model provides new insights into the research on meaning in life and clinical symptoms. Furthermore, it confirms and reinforces the meaning-making model, the theoretical framework on which it is based.
The construction of meaning depends on cultural, social, and religious constructs such as life goals, responsibility, and freedom (Torres-Blasco et al., Reference Torres-Blasco, Castro-Figuero, Garduño-Ortega and Costas-Muñiz2020), and our sample consisted of participants from Spain and various South American countries. Therefore, we can suggest that it is a model that can be applied in different countries with different Spanish-speaking cultures.
The three-pathway model has clinical implications for the assessment, prevention, and treatment of people who are coping with unforeseen negative situations, such as emotional losses, grief, or posttraumatic stress. On the one hand, it shows the importance of evaluating the constructs of violations of global meaning, presence, and search for meaning, and affect in participants with clinical symptoms. Moreover, fostering the construction of meaning in life for individuals undergoing transitions or significant life changes could be an effective strategy to prevent clinical symptoms (Marco et al., Reference Marco, Privado, Guillen, Quero, Pérez, Baños and Tormo2022). Finally, considering these findings, future research could explore whether adding an intervention component focused on enhancing dimensions of meaning in life might increase the effectiveness of evidence-based treatments for clinical symptoms, such as Cognitive Behavioral Therapy, Behavioral Activation Therapy, Interpersonal Therapy, Reminiscence Therapy, or Dialectical Behavior Therapy (Cuijpers et al., Reference Cuijpers, Miguel, Harrer, Plessen, Ciharova, Ebert and Karyotaki2023).
In this sense, some studies already indicate that meaning-based psychotherapies are effective in improving depression (Marco et al., Reference Marco, Castejón, Isern, Grau and Pérez2023, Reference Marco, Llombart, Romero, García-Conde, Corral, Guillen, Botella and Perez2024).
The main limitation of the study is that it is cross-sectional, and so we cannot establish directionality in the influence of the variables or causality. Thus, future longitudinal studies will be necessary to confirm the three-pathway Model of Meaning Making. Furthermore, other variables may influence the relationship between the search for meaning and clinical symptoms. For example, Chen et al. (Reference Chen, Wang, He, Ji, Liu and Ye2021) found that, in participants with severe life events, the search for meaning predicted clinical symptoms, but in mild or moderate life events, the presence of meaning buffered the negative effects of the search. Therefore, future studies should consider the perceived severity of the event. Furthermore, the sample was collected through an online survey, and although we assessed the participants’ levels of depression, anxiety, and somatization, these results cannot be generalized to a clinical sample because the participants were not assessed through clinical interviews. Finally, another limitation is that the “snowball” procedure was used to select the sample. This procedure limits control over the way the sample is composed, which means that its representativeness cannot be guaranteed. Therefore, future research would need to confirm the three-pathway model in a clinical population with high levels of anxiety and depression.
In conclusion, this is the first study to suggest the importance of considering a three-pathway model between meaning-making violations and clinical symptoms and assessing and intervening in the search for and presence of meaning variables to mitigate depression and anxiety in adverse situations.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Author contribution
Marco, J.H. served as lead for conceptualization, methodology, formal analysis, investigation, writing the original draft, and reviewing and editing. Privado, J. served in a supporting role in conceptualization, data analysis, and investigation, and contributed to reviewing and editing. Tormo-Irun, P, and Guillen V. were responsible for resources and supervision and contributed to conceptualization, reviewing, and editing.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors have no conflicts of interest to declare.


 Open access
Open access