


Introduction
Continuity of care (CoC) is a core pillar of primary care, alongside accessibility, comprehensiveness and coordination (Starfield, Reference Starfield1992; Adam and Watson, Reference Adam and Watson2018). More recently, continuity has been defined as ‘the extent to which a person experiences an ongoing relationship with a clinician and the coordinated clinical care that progresses smoothly as the patient moves between different parts of the health service’ (Couchman et al., Reference Couchman, Ejegi-Memeh, Mitchell and Gardiner2023). The concept is multifaceted and is interpreted differently by patients, clinicians and policymakers. Haggerty’s widely cited CoC framework delineates three key dimensions: relational, informational, and management continuity (Haggerty et al., Reference Haggerty, Reid, Freeman, Starfield, Adair and McKendry2003; Burch et al., Reference Burch, Whittaker, Bower and Checkland2024). Relational continuity refers to an ongoing therapeutic relationship between a patient and their healthcare provider, fostering trust and personalized care (Burch et al., Reference Burch, Whittaker, Bower and Checkland2024). Informational continuity ensures that clinicians and patients have seamless access to medical records, past consultations, and diagnostic results. Managerial continuity, meanwhile, emphasizes coordinated, coherent, and adaptive care over time, particularly for patients with complex or chronic conditions. This framework, while still influential, predates the digital era and does not fully capture the complexities of modern general practice where informational and managerial continuity often blur (Greenhalgh et al., Reference Greenhalgh, Shaw, Alvarez Nishio, Byng, Clarke, Dakin, Faulkner, Hemmings, Husain, Kalin, Ladds, Moore, Rosen, Rybczynska-Bunt, Wherton and Wieringa2022). Emerging perspectives thus propose the concept as being multi-dimensional and more complex.
International evidence suggests that strong continuity is associated with reduced mortality, improved chronic disease management, increased medication adherence, reduced hospital attendance and greater clinician job satisfaction (Guthrie et al., Reference Guthrie, Saultz, Freeman and Haggerty2008; Gray et al., Reference Gray, Sidaway-Lee, White, Thorne and Evans2018; Baker et al., Reference Baker, Freeman, Haggerty, Bankart and Nockels2020). Despite its recognized importance, CoC is under threat. The decline in relational continuity has been identified as one of the most concerning consequences of mounting pressures in general practice (Seddon et al., Reference Seddon, Friedrich, Wadd, Dicks, Scott, Robinson and Walker2024). The General Practice Patient Survey (GPPS) showed that patients always or almost always/a lot of the time saw their preferred GP 50.2% in 2018, however, this has fallen to 35.4% in 2023 (GP Survey, 2018, 2023). Discontinuity has been linked to poorer treatment adherence, increased hospitalizations, and lower patient satisfaction (Gray et al., Reference Gray, Sidaway-Lee, White, Thorne and Evans2018). Contributing factors include larger practices, diverse clinical roles and systems focused on rapid access, sometimes at the expense of sustained patient–clinician relationships (Tammes et al., Reference Tammes, Purdy, Salisbury, MacKichan, Lasserson and Morris2017). Alongside these pressures, continuity has been shaped by significant policy and structural changes. Since 2014, initiatives such as the named GP scheme, the introduction of extended access appointments, the development of Primary Care Networks (PCNs), and the more recent shift towards increasing online access and community-based GP-led care have significantly changed how care is organized and delivered (Dineen et al., Reference Dineen, Engamba, Khan, Sidaway-Lee, Duncan, Watson, Evans and Pereira Gray2025).
While policy emphasis on CoC is growing, existing reviews are fragmented in scope and outdated in context. One recent scoping review focused on interventions to improve relational continuity, such as personal patient lists or booking systems, based on literature from 2002 onwards. However, it provided limited insight into measurement approaches, outcomes, barriers, or broader care contexts (Fox et al., Reference Fox, Dickson, Burch, Hind and Hawksworth2024). Hersch et al. outlined the four most common measurement approaches for CoC, however, the discussion was not situated in the UK context and did not address the benefits and challenges associated with each approach (Hersch et al., Reference Hersch, Klemenhagen and Adam2024). A July 2025 systematic review examined the trade-offs between access and continuity, drawing mainly on international studies and without UK-specific focus or attention to wider patient, staff and system outcomes (Goff et al., Reference Goff, Hindi, Hammond and Jacobs2025). Other reviews have examined continuity in the context of care coordination or chronic disease management internationally, but do not capture the full picture of continuity in post-2015 UK primary care, particularly amid NHS reforms and the expansion of PCNs. This period has been characterized by significant structural and policy changes, which have altered how care is organized and delivered. Therefore, to our knowledge, no comprehensive synthesis exists that maps when, and for whom continuity matters, how it is measured, its impacts, the systemic challenges to sustaining it, and which interventions are effective within current UK primary care. This gap highlights the need for a timely, holistic scoping review to inform policy, guide practice, and shape future research.
Methods
This review aimed to explore key aspects of CoC in primary care, including identifying when it is most critical, the tools and measures used to assess it, its impact on patient care and outcomes, and the major challenges associated with maintaining it. A scoping review design was chosen to provide a rapid summary of research conducted in the last 10 years to inform a more detailed future analysis of continuity outcomes and potential benefits or unintended consequences. The review followed the PRISMA Scoping Review guidelines.
Identifying the research questions
Our review questions were designed to align with recent and planned NHS policy reforms, including those outlined in the NHS’s Neighbourhood Health Guidelines 2025/26 (NHS England, 2024b). This review aimed to synthesize and critically evaluate the existing literature on continuity of care in UK primary care settings since 2015, addressing the following questions:
-
1. When does continuity of care matter most in the context of post-2015 UK primary care reforms?
-
2. What tools and measures are used to assess continuity in primary care?
-
3. What are the reported improvements to patient care and outcomes?
-
4. What are the key identified challenges to maintaining continuity of care within post-2015 UK primary care systems?
-
5. What are the reported interventions aimed at enhancing continuity?
Identifying relevant studies
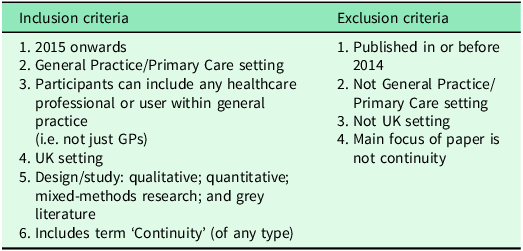
We searched Medline (OvidSP), Embase (OvidSP), and CINAHL (EBSCOHost) in 2024, using Medical Subject Headings (MeSH) and free-text terms (see Supplementary Figure 2). Studies were included if published in English between 2015 and 2024. These dates were selected to enable study of the impact of three important changes in the delivery of UK primary care and allow sufficient time for the implementation of these policies and their effects on continuity and related outcomes to be reflected in the published literature. Beginning in 2015, GPs in England have been required to provide every registered patient with a named GP responsible for their care. In 2018, extended access services were introduced to improve patient access to general practice. In 2019, PCNs were introduced as part of the NHS Long-Term Plan. The networks were designed to incentivise general practices to work together in groups covering populations of between 30–50,000 patients (Burch and Whittaker, Reference Burch and Whittaker2022; Goff et al., 2023; Tammes et al., Reference Tammes, Payne, Salisbury, Chalder, Purdy and Morris2019). Continuity of care has declined over this period and has been the focus of sustained policy and professional concern in UK general practice, further justifying an emphasis on recent structures and incentives (Levene et al., Reference Levene, Baker, Newby, Couchman and Freeman2024; Murphy and Salisbury, Reference Murphy and Salisbury2020; Pettigrew et al., Reference Pettigrew, Petersen, Mays and Cromwell2024). The review was restricted to UK-based studies to maintain contextual coherence with the organization of NHS general practice and with UK-specific policy changes. This approach is consistent with other UK-focused syntheses (Fox et al., Reference Fox, Dickson, Burch, Hind and Hawksworth2024). Grey literature, including policy reports and bibliographies, were also reviewed (Table 1).
Inclusion and exclusion criteria

Study selection
Records were de-duplicated and uploaded into the EPPI-reviewer database. Title and abstracts of papers were double screened (NK, RA, IS, NA, AL) against the inclusion criteria. Disagreements between authors were discussed until a consensus was reached through regular data clinics conducted with EO-B and SP.
Charting the data
A standardized data extraction sheet was developed using Excel and included papers were double-screened at full-text and discrepancies were discussed in data clinics to ensure consistency in collecting key information (see Supplementary Figure 2). This included feedback and adaptations following Patient and Public Involvement (co-applicant TC) to review and refine codes and help develop the study protocol to ensure analysis was relevant to patient and carer perspectives and priorities.
Collating, summarizing and reporting the results
Emerging findings were reviewed and refined during data clinics involving all members of the research team.
Results
The initial search yielded 1619 papers. 377 studies were excluded based on title and abstract screening and a further 222 were excluded at full-text screening based on our exclusion criteria (Figure 1). 180 papers were included and were fully screened using the data extraction sheet (Supplementary Figure 1). Of these, 95 employed quantitative methodologies, including conceptual, observational, and case studies, as well as reports and opinion pieces. Additionally, 76 studies utilized qualitative approaches, such as systematic reviews, cross-sectional studies, and cohort analyses. 9 studies adopted a mixed-methods design.
Flowchart of selection of articles for review.

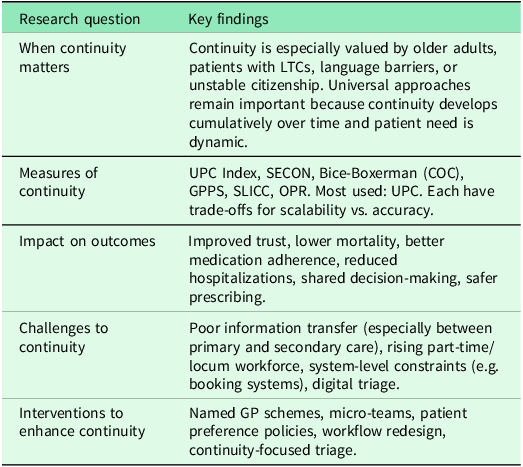
The findings presented below apply specifically to UK primary care in the period since 2015, reflecting evidence generated following significant changes in UK health policy. These findings, which are summarized in Table 5, generate new insights regarding the contexts and mechanisms of CoC in primary care.
Research question 1: When to prioritize continuity of care
Current evidence identifies patient populations who strongly value or prioritize CoC. Patients with long-term conditions (LTCs) that require years of ongoing management such as chronic kidney disease (Brand and Pollock, Reference Brand and Pollock2018), and rheumatoid arthritis (RA) (Machin et al., Reference Machin, Hider, Dale and Chew-Graham2017), and those with complex care needs (Rhodes et al., Reference Rhodes, Campbell and Sanders2016; Greenhalgh et al., Reference Greenhalgh, Shaw, Alvarez Nishio, Byng, Clarke, Dakin, Faulkner, Hemmings, Husain, Kalin, Ladds, Moore, Rosen, Rybczynska-Bunt, Wherton and Wieringa2022; Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), valued CoC more highly than other patients. Relational continuity was valued in older adults (≥65 years) and patients with multimorbidity (Leniz et al., Reference Leniz, Gulliford, Higginson, Bajwah, Yi, Gao and Sleeman2022). Its importance was further amplified for those facing language barriers (Rhodes et al., Reference Rhodes, Campbell and Sanders2016, Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), unstable citizenship status or those who were socioeconomically deprived, with it being more crucial for ethnically diverse groups (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). While the review identified groups that prioritize continuity, none of the included studies provided evidence that clinical benefits were only limited to certain patient groups.
Patients with LTCs wanted their General Practitioner (GP) to be clinically competent, to listen, and take time with them, still demonstrating trust and respect irrespective of whether they have seen them before in situations where continuity was not possible (Murphy and Salisbury, Reference Murphy and Salisbury2020). However, this can contribute to the misconception from practices and patients that ‘any GP will do’, despite evidence that patients who experience CoC usually appreciate its benefits and usually seek it (Gray et al., Reference Gray, Sidaway-Lee, Johns, Rickenbach and Evans2023).
Although several studies identified groups who value continuity, few directly compared preferences across different populations. For example, Machin et al., found that poor CoC was perceived as a barrier to discussing mood problems in patients with RA. However, as their study focused exclusively on this group, it remains unclear whether this reliance on continuity is greater than in other conditions. In contrast, Ladds et al., observed that while many patients with long-term or complex conditions prioritize relational continuity with their GP, others, particularly those without complex needs, may be more willing to exchange provider familiarity for timely access or convenience (Greenhalgh et al., Reference Greenhalgh, Shaw, Alvarez Nishio, Byng, Clarke, Dakin, Faulkner, Hemmings, Husain, Kalin, Ladds, Moore, Rosen, Rybczynska-Bunt, Wherton and Wieringa2022; Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023).
While patient preferences have been shown to vary, studies have also investigated cases in which clinicians have made deliberate efforts to maintain CoC in high-risk cases, such as suspected cancer (Nicholson et al., Reference Nicholson, Goyder, Bankhead, Toftegaard, Rose, Thulesius, Vedsted and Perera2018; Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), and vulnerable groups such as those with intellectual disabilities (Thomas et al., Reference Thomas, Atherton, Dale, Smith and Crawford2023). In these cases, GPs took on a heightened role as integrators to try and prevent patients from falling through the gaps in care (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). GPs reinforced this prioritization, emphasizing CoC’s role in managing care transitions (Rhodes et al., Reference Rhodes, Campbell and Sanders2016) and sensitive consultations involving stigmatized health issues (Rhodes et al., Reference Rhodes, Campbell and Sanders2016).
Research question 2: Tools and measures used to assess continuity in primary care
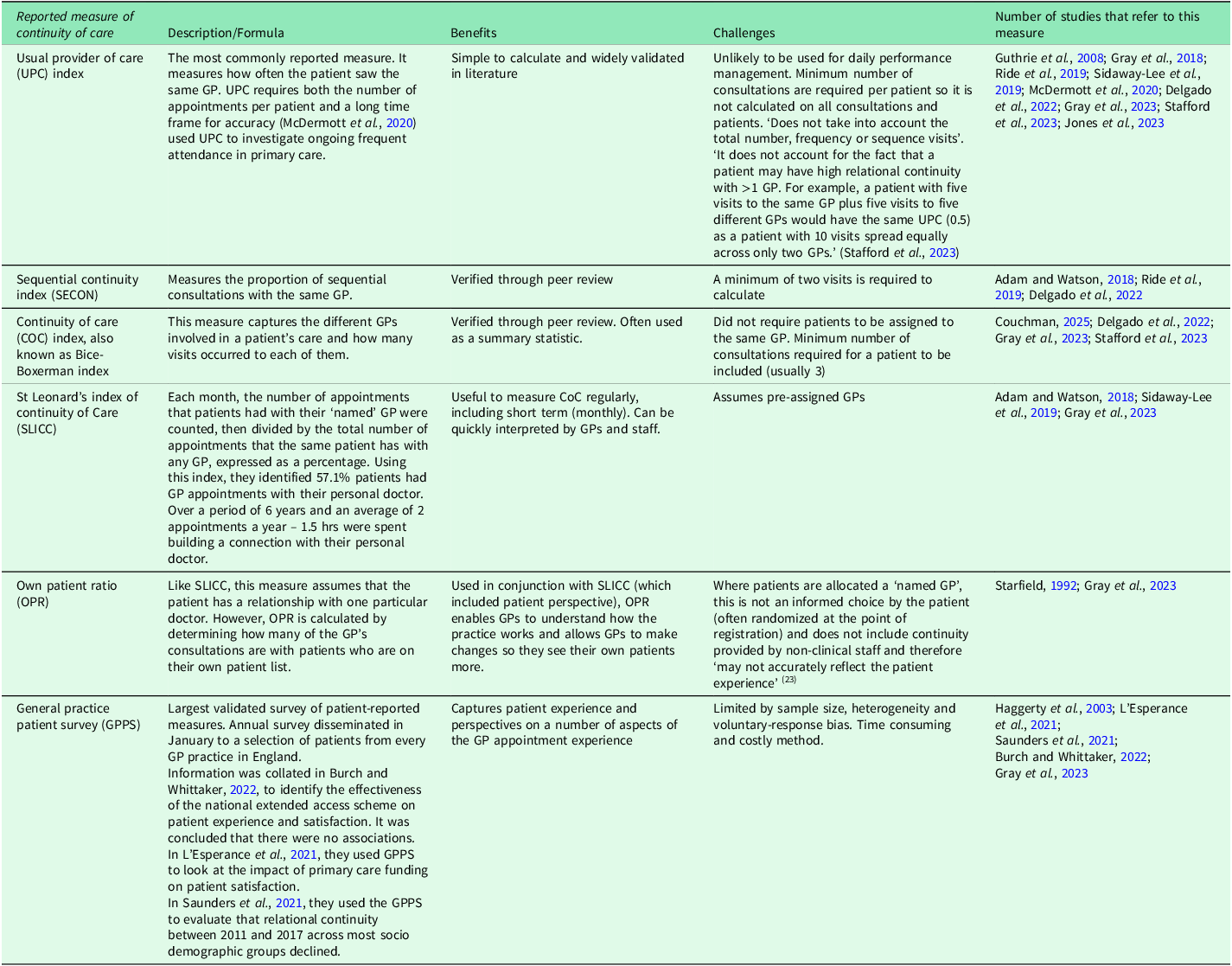
Eleven papers addressed continuity measures (Table 2) that were exclusively concerned with relational continuity and omitted managerial and informational continuity. The field is still evolving, with no consensus on the best measure. Most quantitative studies used whole-population continuity metrics at a practice or patient level, derived from administrative data, rather than measures designed for specific subgroups. The Usual Provider of Care (UPC) Index was most commonly reported, while the GPPS was most used in data analysis.
Reported measures of continuity of care

Research question 3: Reported improvements to patient care and outcomes
At a population level, higher CoC has been associated with reduced mortality (Gray et al., Reference Gray, Sidaway-Lee, White, Thorne and Evans2018; Mahase, Reference Mahase2020), likely due to its role in fostering stronger doctor-patient relationships. Research has also shown that patients exhibit greater trust and comfort when consulting a GP with prior knowledge of their medical history (Turner et al., Reference Turner, Percival, Kessler and Donovan2017; Donaghy et al., Reference Donaghy, Sweeney, Henderson, Angus, Cullen, Hemphill, Wang, Guthrie and Mercer2023). It is faster and more efficient to deal with patient problems as successive consultations with the same patients build ‘accumulated knowledge’. Additionally, when GPs have a strong rapport with their patients and clinical responsibilities are clearly defined, practice operations run more smoothly (Gray et al., Reference Gray, Sidaway-Lee and Evans2022).
Conversely, patients report reluctance to disclose sensitive information to unfamiliar GPs, often preferring extended wait times to see their preferred clinician (Donaghy et al., Reference Donaghy, Sweeney, Henderson, Angus, Cullen, Hemphill, Wang, Guthrie and Mercer2023). This preference is particularly emphasized when involving high stakes decisions such as DNACPR (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), and mental health concerns (Turner et al., Reference Turner, Percival, Kessler and Donovan2017; Donaghy et al., Reference Donaghy, Sweeney, Henderson, Angus, Cullen, Hemphill, Wang, Guthrie and Mercer2023). Patients also seemed to associate longitudinal familiarity with improved diagnostic accuracy, enabling earlier detection of physical and mental health changes (Donaghy et al., Reference Donaghy, Sweeney, Henderson, Angus, Cullen, Hemphill, Wang, Guthrie and Mercer2023), and thereby reducing the perceived risk of misdiagnosis (Rhodes et al., Reference Rhodes, Campbell and Sanders2016). This relational continuity establishes a therapeutic environment allowing mutual trust, creating psychological safety when sharing sensitive health issues and discussing difficult problems (Nowak et al., Reference Nowak, Sheikhan, Naidu, Kuluski and Upshur2021).
Patients with multimorbidity found it beneficial to not repeat their complex histories (Engamba et al., Reference Engamba, Steel, Howe and Bachman2019), or ‘re-educate and re-inform’ doctors at each appointment (Mason et al., Reference Mason, Nanton, Epiphaniou, Murray, Donaldson, Shipman, Daveson, Harding, Higginson, Munday, Barclay, Dale, Kendall, Worth and Boyd2016). Doctors identified that continuity facilitated longitudinal assessment of patients’ health status, including monitoring of mobility, cognitive function, speech patterns and overall well-being (McKelvie et al., Reference McKelvie, Moore, Croxson, Lasserson and Hayward2019), thereby supporting decision-making, allowing safer and more efficient practice (Greenhalgh et al., Reference Greenhalgh, Shaw, Alvarez Nishio, Byng, Clarke, Dakin, Faulkner, Hemmings, Husain, Kalin, Ladds, Moore, Rosen, Rybczynska-Bunt, Wherton and Wieringa2022; Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). CoC also contributed to enhanced patient perceived validation of health concerns and enhanced shared decision-making with GPs (Nowak et al., Reference Nowak, Sheikhan, Naidu, Kuluski and Upshur2021).
Strong relational continuity was reported to allow GPs to provide personalized medical recommendations, which may enhance medication adherence and consequently reduce hospitalizations (Barker et al., Reference Barker, Lloyd and Steventon2016; Dew and Wilkes, Reference Dew and Wilkes2018; Nowak et al., Reference Nowak, Sheikhan, Naidu, Kuluski and Upshur2021; Tammes et al., Reference Tammes, Payne and Salisbury2022). Studies demonstrated that patients exhibit greater compliance with treatment regimes and monitoring protocols when relational continuity was present (Tammes et al., Reference Tammes, Payne and Salisbury2022), with qualitative research identifying perceived interpersonal accountability as a contributing factor (Turner et al., Reference Turner, Percival, Kessler and Donovan2017). Greater CoC was also associated with increased statin prescriptions and improved adherence to statins for secondary prevention in patients aged 30 or older with cardiovascular disease-related conditions (Tammes et al., Reference Tammes, Payne and Salisbury2022). Additionally, patients experienced better efficiency of diagnosis and chronic disease management in high CoC scenarios (Nowak et al., Reference Nowak, Sheikhan, Naidu, Kuluski and Upshur2021).
Patients who were previously frequent attenders had a decreased GP consultation rate after receiving more CoC through a ‘ named GP’ initiative (Barnes et al., Reference Barnes, Cramer, Thomas, Sanderson, Hollinghurst, Metcalfe, Jackson, Record, Thorley and Kessler2019), while patients who were unable to see their nominated GP described having to book several appointments for the same problem (Chilton et al., Reference Chilton, Bradley and Mitchell2021). This fragmented care experience was associated with perceived stigmatization as a ‘nuisance patient’ and subsequent negative psychosocial outcomes, including increased frustration and anxiety (Chilton et al., Reference Chilton, Bradley and Mitchell2021). Conversely, Goff et al. (Reference Goff, Jacobs, Hammond, Hindi and Checkland2024a) found that new working arrangements in Primary Care Networks undermined healthcare professionals’ ability to maintain relational continuity. These changes also caused patients to experience greater inefficiencies when trying to access care.
Research question 4: Key identified challenges to maintaining continuity of care in modern primary care
Systemic challenges at the primary to secondary care interface, such as delays in information transfer, inadequate referral and discharge communications, inaccessible diagnostic results, fragmented electronic systems, and the unstructured redistribution of tasks between clinicians, represent significant barriers to CoC. These barriers may also arise as consequences of a lack of continuity itself, and a feedback loop is created in which poor continuity contributes to breakdowns in communication and role clarity, which in turn further erode the system’s ability to maintain CoC (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). Maintaining CoC has become increasingly difficult in contemporary health systems (Gray et al., Reference Gray, Sidaway-Lee, Johns, Rickenbach and Evans2023), due to a range of systemic pressures. These include rising workloads, workforce shortages, and growing reliance on locum or part-time staff. Together, these challenges contribute to fragmented care delivery and compromise both patient safety and outcomes. These are significant issues that must be addressed.
The lack of communication between primary and secondary care and other settings of healthcare delivery, has become a major challenge when trying to provide patients with consistent care. Hospital discharge summaries outlining patients’ hospital admissions exhibited suboptimal completion with documentation inconsistencies and significant delays in dissemination (Coyle et al., Reference Coyle, Studd, ElSiofy and Gelfer2020; Scarfield et al., Reference Scarfield, Shepherd, Stapleton, Starks, Benn, Khalid, Dayment, Moate, Mohamed and Lee2022). This was also highlighted as a challenge in the transition between CAMHS and the adult mental health services where ‘patients fall through the gaps’ (Appleton et al., Reference Appleton, Loew and Mughal2022).
Part‑time working, greater use of allied health professionals, and reliance on locums have all been linked to declining continuity in recent years (McKelvie et al., Reference McKelvie, Moore, Croxson, Lasserson and Hayward2019; Engamba et al., Reference Engamba, Steel, Howe and Bachman2019; Khan et al., Reference Khan, Rudoler, McDiarmid and Peckham2020; Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). Locum doctors, often described as ‘professionally isolated’ (Ferguson and Walshe, Reference Ferguson and Walshe2019), have voiced concerns about having access to less information than patients’ regular doctors. McKelvie highlights this issue, stating: ‘Locum GPs … were very aware of the reduced information that they had in comparison with the patients’ regular doctor.’ (McKelvie et al., Reference McKelvie, Moore, Croxson, Lasserson and Hayward2019: 4). Similarly, newly qualified foundation doctors, who are responsible for producing over 90% of discharge summaries, face challenges in determining what information to include in these letters (McKelvie et al., Reference McKelvie, Moore, Croxson, Lasserson and Hayward2019). Boddy notes: ‘Over 90% of discharge summaries are authored by newly qualified foundation doctors, who struggle to analyse the information to include and lack insight into the importance of communication for the recipient GP’ (Boddy et al., Reference Boddy, Barclay, Bashford and Clarkson2022: 2). Secondary prevention of Acute Coronary Syndrome is contingent upon strict medication adherence, yet discharge transitions frequently present substantial barriers. These include incomplete or inaccurate medication history, failure to communicate therapeutic modifications, and inadequate information to primary care providers (Goldman and Harte, Reference Goldman and Harte2020).
Several systemic challenges to CoC were identified in the literature. Among these were constraints on GP availability (Barnes et al., Reference Barnes, Cramer, Thomas, Sanderson, Hollinghurst, Metcalfe, Jackson, Record, Thorley and Kessler2019), with many GPs in portfolio careers working fewer clinical sessions (Saunders et al., Reference Saunders, Flynn, Massou, Lyratzopoulos, Abel and Burt2021). Additionally, maintaining relational continuity was found to impose significant time burdens on GPs, potentially compromising workforce sustainability (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023). Further operational barriers included inflexible appointment scheduling systems (Barnes et al., Reference Barnes, Cramer, Thomas, Sanderson, Hollinghurst, Metcalfe, Jackson, Record, Thorley and Kessler2019), and inadequate clinical workflow structures (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), both requiring redesign by the practice team to enhance appropriate utilization of electronic health records to facilitate informational continuity (Ladds et al., Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023).
Studies consistently show that some ethnic minority groups experience lower CoC, access and interpersonal care in general practice (Saunders, Reference Saunders, Flynn, Massou, Lyratzopoulos, Abel and Burt2021; Stafford et al., Reference Stafford, Bécares, Hayanga, Ashworth and Fisher2023). Indeed, although data from the GPPS show a decline in relational continuity between 2011 and 2017 across most sociodemographic groups, this decline was more pronounced among ethnic minority patients than among those of White ethnicity (Stafford et al., Reference Stafford, Bécares, Hayanga, Ashworth and Fisher2023). It has been suggested that these disparities may stem from unequal resource distribution, including underfunded practices and ‘underdoctoring’ in deprived areas where ethnic minorities are overrepresented. (Stafford et al., Reference Stafford, Bécares, Hayanga, Ashworth and Fisher2023). The association between ethnicity and continuity, even after controlling for area deprivation, suggests that language barriers and sociocultural norms may create further obstacles and affect whether patients from some ethnic minority groups seek continuity of care (Stafford et al., Reference Stafford, Bécares, Hayanga, Ashworth and Fisher2023). Together, these structural and interpersonal factors may undermine CoC and exacerbate health inequalities.
Research question 5: Reported interventions aimed at enhancing continuity
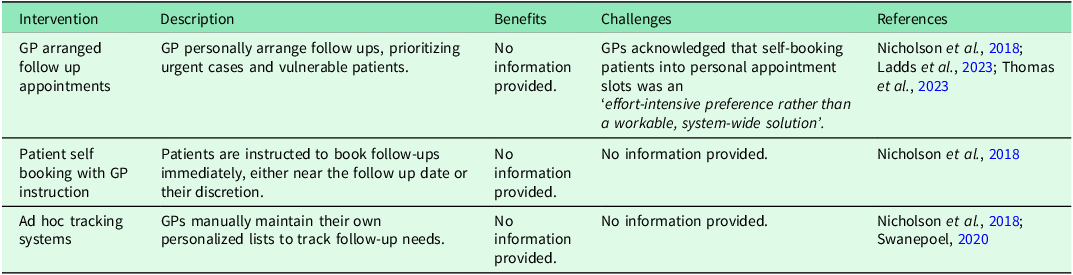
Tables 3 and 4 summarize the formal and informal interventions used by GP practices to enhance CoC. While formal interventions are embedded in organizational or contractual systems, informal interventions rely on individual or team initiative and are often undocumented. While beneficial these interventions faced implementation challenges and some relied heavily on GP efforts, proving less sustainable. The tension between continuity and accessibility persisted across interventions.
Formal interventions aimed at enhancing continuity

Informal interventions aimed at enhancing continuity

Summary of key findings

Discussion
The evidence base supporting the value of continuity in primary care is burgeoning. However, the concept of continuity is multidimensional, and its meaning varies between patients, clinicians and policymakers (Sheaff et al., Reference Sheaff, Halliday, Ovretveit, Byng, Exworthy, Peckham and Asthana2015). Its implementation must remain adaptable to shifting healthcare needs, patient preferences and systemic constraints to preserve clinical relationships and care quality. Although the evidence supporting CoC is robust, its routine assessment remains insufficiently integrated into clinical practice. The review has focused on literature relating to UK general practice since 2015. This period witnessed significant policy changes in UK primary care. The discussion first considers the impact of these recent policy changes, before reflecting on the five research questions.
Beginning in 2015, UK general practice has undergone three significant national reforms: the named accountable GP scheme (2014/15), universal extended access (2018), and the introduction of PCNs (2019). While a scoping review cannot definitively establish causality, these important shifts have coincided with a continued decline in patient reported CoC, from 50.2% in 2018 to 35.4% in 2023 (GP Survey, 2018, 2023).
Evidence from evaluations of the named accountable GP policy suggests that administratively allocating a GP does not, by itself, produce relational continuity. Tammes et al. (Reference Tammes, Payne, Salisbury, Chalder, Purdy and Morris2019) found that the scheme was not associated with improvements in either continuity of care or rates of unplanned hospitalization, concluding that more sophisticated interventions are needed beyond mere administrative allocation. This failure has been attributed to the fact that the policy did not guarantee patients would actually see their named clinician at a time of rising GP workloads and part-time working patterns (Couchman et al., Reference Couchman, Ejegi-Memeh, Mitchell and Gardiner2023).
The introduction of universal extended access was designed to improve appointment availability, particularly for working adults. However, while the scheme improved satisfaction with appointment times for those in full-time employment, it had a negative impact on relational continuity. Mou et al. (Reference Mou, Lau, Burch and Whittaker2025) found that providing these additional access days negatively impacted patients’ experience of continuity of care, though this effect was not linear relative to the number of extra days. This suggests a policy-driven trade-off where prioritizing rapid access frequently occurs at the expense of sustained patient–clinician relationships.
PCNs show mixed effects on continuity. Qualitative evidence indicates that larger-scale care provision can undermine relational continuity by requiring clinicians to work across multiple sites or provide remote consultations for pooled patient lists, leading to ‘fragmented care’ (Goff et al., Reference Goff, Jacobs, Hammond, Hindi and Checkland2024b). By contrast, recent quantitative data from Odebiyi et al. (Reference Odebiyi, Gibson, Goff, Hindi, Hammond, Checkland, Sutton and Jacobs2025) suggests that larger practice networks and those with pre-existing inter-practice collaborations were actually associated with better continuity. This suggests that while the organizational shift can fragment individual relationships, well-integrated and properly staffed networks may offer a protective structural effect.
In relation to the first research question, the findings indicate that continuity is a priority for vulnerable groups, including patients with LTCs and those facing language barriers or trauma. While the literature identifies certain populations who most value continuity, as noted by Dineen et al. (Reference Dineen, Engamba, Khan, Sidaway-Lee, Duncan, Watson, Evans and Pereira Gray2025), there remains limited empirical evidence demonstrating that these groups derive disproportionately greater clinical benefit. Identification of ‘high-risk’ groups, who are perceived to need continuity most, are sometimes conflated with selective strategies to only offer continuity to certain populations. This approach undermines the importance of accumulating continuity over time and the dynamic nature of illness fluctuations and progressions. Indeed, Pahlavanyali et al. (Reference Pahlavanyali, Hetlevik, Baste, Blinkenberg and Hunskaar2024) note that CoC ‘does not evolve only over certain disease-related consultations and it takes time for doctors to build a relationship with ‘accumulated knowledge’ about their patients’. Similarly, Owen-Boukra et al. found that ‘the growth and implementation of cumulative knowledge can flourish through interactions with patients and peers’ (Reference Owen-Boukra, Burford, Cohen, Duddy, Dunn, Fadia, Goodman, Henry, Lamb, Ogden, Rapley, Rees, Roberts, Royer-Gray, Vance, Wong and Park2026). General practice serves universal healthcare needs with longitudinal comprehensive care. Embedding continuity throughout the whole healthcare system is therefore likely to be more successful across time.
The concept of relational injury may be particularly important when considering vulnerable patients. This is the idea that adverse experience or developmental trauma can impair an individual’s ability to engage with healthcare systems. As Burley argues, for those with severe relational injury, CoC is not the context within which care needs to happen, rather it is the care that needs to happen (Burley, Reference Burley2024; Polnay et al., Reference Polnay, Pugh, Barker, Bell, Beveridge, Burley, Lumsden, Mizen, Wilson, Polnay, Pugh, Barker, Bell, Beveridge, Burley, Lumsden, Mizen and Wilson2023). In this sense, a sustained relationship with a GP could act as a reparative experience, offering the consistency and stability often missing in patients’ lives. This was echoed by a GP involved in the CARE Plus Intervention, who reflected that ‘we are quite often the only person that brings consistency and continuity’ (Mercer et al., Reference Mercer, O’Brien, Fitzpatrick, Higgins, Guthrie, Watt and Wyke2016). Such perspectives highlight the value of continuity as a form of care that actively addresses psychological and relational needs.
In relation to the second research question, the findings indicate that tools to measure continuity focused on relational continuity, with the UPC most commonly reported and GPPS most frequently used for analysis. While several tools have been developed to measure continuity [Table 2], they often fail to capture qualitative dimensions (e.g. trust, care coordination) or address equity gaps. Certain demographic groups such as ethnic minority groups were found to be notably underrepresented. For example, the 2024 GP survey found that 42% of white patients ‘always/almost always’ accessed their preferred healthcare professional, compared to 34–38% of patients from mixed, Asian, Black, or other ethnicities (NHS England, 2024a). This inequity reflects the Inverse Care Law, first coined by Julian Hart in 1971 who stated ‘The availability of good medical care tends to vary inversely with the need for it in the population served’ (Hart, Reference Hart1971; 1). As noted in The Lancet, positioning this principle at the foreground of policy and healthcare planning could guide efforts to improve health equity and social justice in the coming decades (The Lancet, 2021). Models such as CARE Plus, developed to support patients in areas of high social deprivation, emphasize relational continuity as a core principle (Mercer et al., Reference Mercer, O’Brien, Fitzpatrick, Higgins, Guthrie, Watt and Wyke2016). Evidence from such interventions demonstrates that continuity is central to delivering high-quality care, particularly for vulnerable groups who are otherwise less likely to experience it.
The third research question concerns CoC and clinical, patient-reported and systems outcomes. CoC has been associated with improved doctor-patient relationships, better medication adherence, lower mortality, reduced hospitalization and the implementation of shared decision-making and personalized care. However, these benefits exist alongside ongoing tensions between sustaining long-term GP-patient relationships and ensuring timely access. While policies designed to expand rapid access, such as the introduction of extended access services, often focus on the ‘supply’ of appointments, GP workforce numbers, and waiting times, they risk unintentionally undermining relational continuity (Fisher et al., Reference Fisher, Beech, Alderwick, Price, Ansari, Dixon-Woods and Sinnott2024). Policy initiatives like Jess’s Rule illustrates the practical consequences of prioritizing rapid access over continuity, highlighting that patients who attend repeatedly with persistent or worsening symptoms benefit when clinicians maintain ongoing relationships and review patterns over time; clinicians are encouraged to ‘reflect, review and rethink’ in these cases (Couchman, Reference Couchman2025). This reinforces the idea that patient demand is not fixed; Owen-Boukra et al. (Reference Owen-Boukra, Burford, Cohen, Duddy, Dunn, Fadia, Goodman, Henry, Lamb, Ogden, Rapley, Rees, Roberts, Royer-Gray, Vance, Wong and Park2026) argue that it is dynamic and shaped by the interactions between patients, GPs and practices. When patients feel known, trusted, and ‘looked after’, their sense of uncertainty decreases, and their help-seeking often becomes more measured, reducing the volume and urgency of appointments. The candidacy framework emphasizes how patients recognize their needs, navigate services, and are judged eligible for care (Dixon-Woods et al., Reference Dixon-Woods, Cavers, Agarwal, Annandale, Arthur, Harvey, Hsu, Katbamna, Olsen, Smith, Riley and Sutton2006). While increasing the permeability of access may facilitate entry into the system, it risks eroding the relational aspects of care that underpin continuity. Striking the right balance remains a central challenge for primary care. The new 10-year plan seeks to address this by implementing neighbourhood health centres. These centres aim to create healthier communities by shifting care from hospitals to local or home settings, focusing on prevention, and leveraging digital solutions to enhance health management, all supporting both accessibility and continuity (NHS England, 2025).
In relation to the fourth research question, the findings highlight the challenges of maintaining CoC, including poor information transfer between primary and secondary care, system-level constraints such as booking systems and digital triage, and the rising use of part-time and locum staff. These barriers may disproportionately affect ethnic minority groups, people living in deprived areas, and those with limited English proficiency or literacy, as longstanding socioeconomic, cultural, language- and disability-related factors, alongside structural and technical limitations, reduce engagement, especially with digital healthcare (Turnbull et al., Reference Turnbull, Prichard, MacLellan and Pope2024). This reflects an ‘inverse continuity law’ whereby patients who may have the greatest need are least likely to receive it (Dineen et al., Reference Dineen, Engamba, Khan, Sidaway-Lee, Duncan, Watson, Evans and Pereira Gray2025). These practical challenges are further compounded by limitations in how continuity is measured, as the CoC measures identified in this scoping review, and discussed in response to our second research question, focus solely on relational continuity and bi-directional patient-GP interactions, can overlook additional benefits of informational (e.g. review of a discharge letter resulting in a phone call to a patient and subsequent patient advocacy work by the GP) and managerial continuity. Such omissions highlight the importance of broader frameworks, like those proposed by Ladds et al. (Reference Ladds, Greenhalgh, Byng, Rybczynska-Bunt, Kalin and Shaw2023), and the House of Care model (Coulter et al., Reference Coulter, Kramer, Warren and Salisbury2016), which emphasizes teamwork, collaborative and community-focused care to improve outcomes.
While many of the articles identified in this review described part-time working as a significant contributor to the decline in relational continuity, international evidence suggests that clinical hours are not an absolute determinant of a clinician’s ability to provide continuous care. For example, in Norway, where GPs often work clinical sessions only three to four days a week, exceptionally high continuity scores (averaging 85%) are still achieved. This is often facilitated by patients’ willingness to wait for their personal GP for non-urgent matters and the provision of scheduled gaps for non-planned consultations (Sandvik, Reference Sandvik2024). Furthermore, a study of Australian GP trainees found that a registrar’s full-time or part-time status had no significant association with the level of continuity they provided to their patients (Pearlman et al., Reference Pearlman, Morgan, van Driel, Henderson, Tapley, McElduff, Scott, Spike, Thomson and Magin2016). These findings suggest that with effective practice organization and a patient-centred approach to scheduling, offering high-quality continuity remains feasible within a part-time workforce.
Finally, in relation to the fifth research question, the study identified a range of formal and informal interventions aimed at enhancing continuity. Formal interventions referred to system-wide strategies often embedded in contracts, organizational models, or digital infrastructure. However, informal interventions were characterized as more locally developed, ad hoc practices led by individual GPs or teams which were not formally mandated and often relied on personal initiative. This distinction was also noted in a scoping review which found that, for many GP practices, CoC is delivered as part of routine day-to-day work and often goes undocumented, and is rarely captured in the existing literature (Fox et al., Reference Fox, Dickson, Burch, Hind and Hawksworth2024). There seems to be a place for both formal and informal CoC as health systems are complex, and no single approach is likely to be sufficient. The future of continuity interventions may lie in integrating these approaches, ensuring that national frameworks create space and support for local innovations while minimizing reliance on individual effort. Embedding evaluation within such interventions will also be crucial to understand not only their effectiveness, but also their unintended impacts.
Implications for policy and practice
Recent UK policy reforms have yielded varied results: while the named GP scheme had no measurable impact on continuity, universal extended access has often exacerbated discontinuity, and PCNs have shown mixed effects depending on their internal integration. Strengthening CoC therefore requires system-wide commitment alongside other primary care priorities. Policymakers should align financial incentives to reward care coordination, shifting focus from volume-driven metrics to patient-centred outcomes. Indeed, in February 2024 NHS England announced that the GP Contract Regulations would be amended to explicitly require continuity of care to be considered when deciding how best to respond to patient enquiries (NHS England, 2024c.) Clinically, professional training should emphasize the value of relationships as a core expectation. Researchers must examine digital tools, assessing both their potential to enhance and disrupt CoC (e.g. unintended consequences, such as inequalities in access and experience) (Dineen et al., Reference Dineen, Engamba, Khan, Sidaway-Lee, Duncan, Watson, Evans and Pereira Gray2025). Combined, these measures could rebalance primary care toward responsive and proactive, relationship-based care. Within the UK, England has seen the recent introduction of the ‘Ten Year Plan’. This emphasizes the need to shift towards digital, preventive and community-based care (NHS England, 2025). This policy offers a key opportunity in general practice to embed universal approaches to CoC across relational, informational and management systems. Research is crucial to explore the impact these changes have on patients, staff and equitable provision of care.
Limitations
This review included only English-language studies published after 2015 and focused on the UK, possibly excluding relevant interventions from other healthcare systems. Additionally, the included studies did not allow disaggregation by CoC type (relational, informational, managerial), limiting insights into targeted interventions. This review draws on a wide range of literature that varied in methodological approaches. As studies are not homogenous, our analysis attends to the commonalities and differences across papers rather than seeking to make direct comparison. The diversity of sources was necessary to capture the breadth of current work on CoC and to reflect the complexity of the topic.
Future research directions
Future studies should measure and understand CoC across all dimensions, including relational, informational, and managerial continuity, as well as qualitative factors such as trust and coordination. Equity-focused research is needed to address disparities among ethnic minority and socially deprived populations, for example exploring the bi-directional work of CoC (e.g. addressing patient needs for advocacy and gate-opening, alongside responding to patient requests and preferences) A realist review framework, for example, can guide exploration of who benefits from relational continuity and under what conditions (Tzortziou Brown et al., Reference Tzortziou Brown, Park, Mahtani, Taylor, Owen-Boukra, Taylor, Richards, Begum and Wong2025).
While this review prioritized recent UK policy impacts, future evidence syntheses should extend the search period prior to 2015 to capture long-term historical trends that predate current regulatory frameworks. Furthermore, researching structurally similar international primary care systems is recommended to help distinguish universal challenges in delivering continuity from those driven specifically by NHS funding and policy levers. Cross-national registry studies and international qualitative syntheses could provide useful methodological templates. Combining population-level administrative data with in-depth qualitative work can both quantify impacts and explain mechanisms. Adopting such mixed, comparative designs would help to identify which continuity-enhancing interventions are transferable across systems and which require local adaptation (Coombs et al., Reference Coombs, Cohen, Duddy, Mahtani, Owen, Roberts, Saini, Foster and Park2023; Nowak et al., Reference Nowak, Sheikhan, Naidu, Kuluski and Upshur2021; Pahlavanyali et al., Reference Pahlavanyali, Hetlevik, Baste, Blinkenberg and Hunskaar2024).
This review highlights the importance of inclusion, as CoC may not be experienced equally. Current studies, however, provide limited analysis of the underlying mechanisms driving these disparities. Future research should examine how structural, organizational and interpersonal factors contribute to ethnic variation in continuity and should prioritize designs that can detect and explain these inequities.
Further investigation of digital and hybrid care models is warranted, including their impact on continuity and health inequalities. Longitudinal and cross-national studies can clarify sustainability and transferability of interventions. Research should also examine systemic and workforce influences, such as incentives, team models, and working patterns, and the patient perspective, particularly for those with multimorbidity, mental health needs, or relational injury, to strengthen continuity and improve outcomes in primary care.
Conclusions
Continuity of care remains a cornerstone of effective general practice, but its disruption under ongoing NHS pressures necessitates urgent action. This study highlights reported measures and interventions, particularly integrated solutions that combine workforce redesign, digital integration, and patient-centred metrics, as potential pathways forward. Future research should explore how, why, and under what conditions these interventions may or may not enhance practice. Additionally, thorough evaluation is needed to assess the feasibility and impact of these strategies on continuity, equitable access, workforce sustainability and overall patient health outcomes in real-world settings.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1463423626101212.
Acknowledgements
The completion of this review would not have been possible without the expertise, invaluable guidance, and unwavering patience of all the supervising authors. Their continuous support and constructive feedback were instrumental in shaping the quality of this work.
Author contributions
Nikita Kartikapallil: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing – original draft, writing – review & editing. Nicolle Caicedo Arroyave: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing – original draft, writing – review & editing. Jonathan Taylor: data curation, formal analysis, project administration, supervision, writing – review & editing. Ishveer Sanghera: data curation, formal analysis, investigation, project administration, supervision, writing – original draft, writing – review & editing. Mohammad Reduanul Alam: formal analysis, investigation, writing – review & editing. Annabel Lines: formal analysis, investigation, writing – review & editing. Emily Owen-Boukra: conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, supervision, writing – original draft, writing – review & editing. Tanya Cohen: conceptualization, formal analysis, writing – review & editing. Nia Roberts: data curation, investigation, resources. Victoria Tzortziou Brown: formal analysis, writing – review & editing. Geoff Wong: formal analysis, investigation, writing – original draft, writing – review & editing. Kamal Mahtani: formal analysis, writing – review & editing. Sophie Park: conceptualization, formal analysis, investigation, methodology, supervision, writing – original draft, writing – review & editing.
Funding statement
This review was conducted without formal research funding as part of a student project.
Competing interests
No conflicts of interest to declare.
Ethical standards
Ethical approval was not required for this review.
All persons listed as authors have read and approved the submission of this manuscript.





 Open access
Open access