


Introduction
According to the American Heart Association, in the United States (US), the Black population is experiencing a disproportionately higher rate of cardiovascular disease and diabetes compared to their non-Hispanic White counterparts. 1 Additionally, they have one of the highest rates of hypertension globally. 1 Most studies exploring the health status of Black people do so considering them as one homogenous group. However, research shows that there are differences within the Black population based on whether they were born in the US or outside the US. For example, foreign-born Black people tend to practice more healthy behaviors, including having healthier dietary patterns, Reference Lancaster, Watts and Dixon2 lower alcohol use, Reference Lucas, Barr-Anderson and Kington3 tobacco use, and being more physically active, Reference Lucas, Barr-Anderson and Kington3,Reference Singh and Siahpush4 when compared to Black people born in the US. Reference Lancaster, Watts and Dixon2 Furthermore, foreign-born Black people have lower risk for morbidity and all-cause mortality related to lifestyle factors compared to Black people born in the US, but this difference has been shown to decrease with longer time spent in the US. Reference Singh and Siahpush4
The body roundness index (BRI) is a novel body composition assessment developed by Thomas and his colleagues in the US. Reference Thomas, Bredlau and Bosy-Westphal5 However, while the tool has been used extensively in research in China, Peru, and Spain, it has yet to gain widespread adoption in the US. Reference Rico-Martín, Calderón-García, Sánchez-Rey, Franco-Antonio, Martínez Alvarez and Sánchez Muñoz-Torrero6 The index is inexpensive yet has been shown to have considerably more accurate chances of predicting body fat and visceral adiposity as compared to traditional standard assessments such as body mass index (BMI). Reference Thomas, Bredlau and Bosy-Westphal5,Reference Rico-Martín, Calderón-García, Sánchez-Rey, Franco-Antonio, Martínez Alvarez and Sánchez Muñoz-Torrero6 There are, however, few studies exploring the heterogeneity of the US Black population by body composition, specifically using the BRI. In this study, we evaluated the relationship between nativity and BRI among non-Hispanic Black people using data from the National Health and Nutrition Survey (NHANES). It was hypothesized that US-born non-Hispanic Black people would have higher BRI scores compared to foreign-born Black people.
Methods
A sample of non-Hispanic Black adults was selected from four cycles of the NHANES, 2011 to 2018. NHANES is a publicly available dataset, representing a nationally representative sample, that is collected using a multistage cross-sectional design. It is conducted yearly to evaluate the health and nutritional status of people in the US. NHANES consists of interviews, physical examinations, and laboratory testing on approximately 5,000 people annually to gather data on chronic conditions, dietary intake, health indicators, risk factors, and other health-related variables. Details of the study design and data collection procedures are publicly accessible. 7 This sample of non-Hispanic Black adults included only participants aged 20 years older who were not pregnant and had completed all NHANES’ demographics surveys, the anthropometrics, and two days of 24-h dietary recalls with valid data on all variables of interest.
Measures
Dependent variable
BRI, a continuous variable, was calculated using the following formula.
364.2–365.5* {1-[(waist circumference (meters)/2 π)/(0.5*height (meters))]2}½. Reference Thomas, Bredlau and Bosy-Westphal5,Reference Rico-Martín, Calderón-García, Sánchez-Rey, Franco-Antonio, Martínez Alvarez and Sánchez Muñoz-Torrero6
The index is designed to predict body fat and visceral adiposity, with higher scores representing increasing central adiposity.
Independent variable of interest
NHANES does not directly capture “birthplace” as a distinct variable. However, race and country of birth data are available, which allowed the authors to derive a categorical variable, “nativity,” used to identify Black participants and classify them as born inside or outside the US. Specifically, participants’ responses to the questions, “What race or races do you consider yourself to be?” and “Do you consider yourself to be of Hispanic, Latino, or of Spanish origin?” Responses to these questions are recoded and reported in the public use version of the NHANES datasets as race/Hispanic origin. A subset of only non-Hispanic Black participants were selected for these analyses. Participants also answered the question “In what country were you born?” Response options were “50 states or DC” or “Others.” It is also worth noting that countries of origin were asked, but this identifying information was not provided in the public use dataset. Therefore, in this study, nativity was defined as a two category variable (i.e., US-born and foreign-born).
Covariates
Covariates included biological sex, marital status, education, poverty-to-income ratio (<1.3, 1.3 to <2.0, and ≥2.0), and dietary quality. Dietary intake was computed based on participants’ total nutrient intakes from two non-consecutive days of dietary recalls. Using the USDA’s Food Patterns Equivalents Database (FPED), dietary intake data were converted into food components according to the Healthy Eating Index (HEI). The HEI measures how well someone’s diet follows fundamental recommendations from the Dietary Guidelines for Americans 8 and quantifies overall diet quality on a 0–100 scale based on compliance with dietary guidance across 13 intake components. 8–10 A higher total score indicates better alignment with expert recommendations for higher intakes of “adequacy components” and limited intakes of “moderation components.” The standardized metric allows diet quality to be evaluated and tracked across populations. HEI scores were grouped as good (>80), fair (51–80), or poor (<51), consistent with previously published literature. Reference Lara-Breitinger, Medina Inojosa and Li11 Age was found to be normally distributed by nativity and therefore left as a continuous variable.
Data analysis
The statistical software SAS version 9.4 (SAS Institute Inc., Cary, NC, 2012) and the SAS Survey features were used to compute inferential statistics while accounting for the complex multistage probability sampling methodology, oversampling procedures, and sample weights inherent in the NHANES study design. Thus, the appropriate NHANES-provided sampling weights (WTMEC8YR), strata (SDMVSTRA), and cluster (SDMVPSU) variables to adjust for survey design features. Univariate analyses were used to assess normality. Mean differences and frequency distributions were evaluated using analysis of variance/t-tests. Chi-square tests were computed to assess for differences in demographic characteristics and nativity. A multilinear regression model was used to determine the association between nativity and BRI after adjusting for all covariates. Regression outputs including beta coefficients, t-statistics, and p-values were generated. Significance of the results were considered at P < 0.05. Lastly, BMI categories were computed based on measured height and weight. These categories are consistent with clinical guidelines for the identification of overweight and obesity in adults. 12 Average BRI scores, including the range of scores, were computed for each BMI category. This analysis was done to demonstrate the wide range of BRI scores within each established weight category. BMI or BMI category was not included as a covariate in the linear regression analysis because BRI and BMI are computed using similar data and therefore, highly correlated.
Results
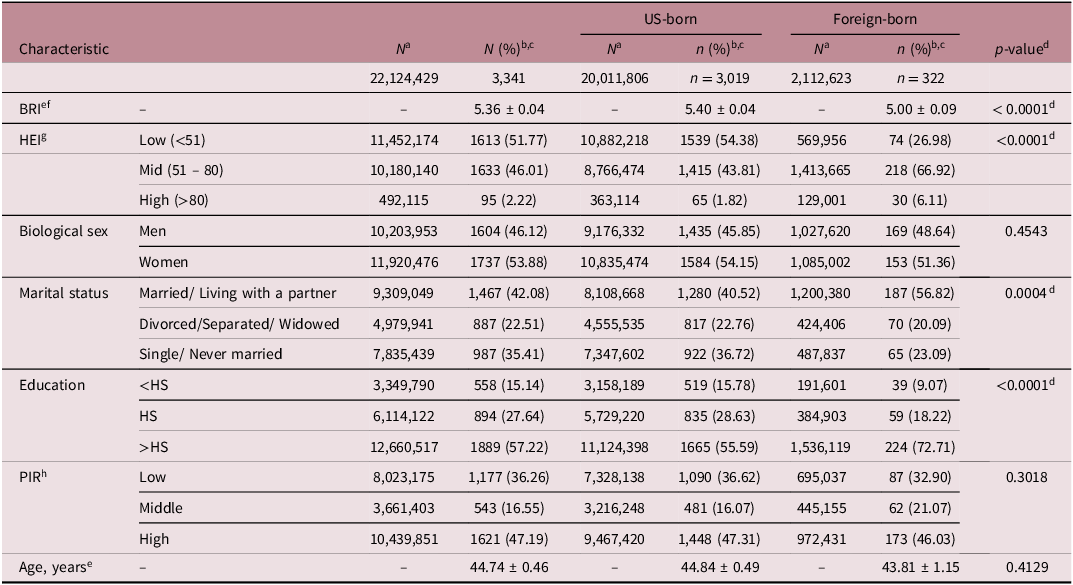
Among the 3341 non-Hispanic Black participants, 3019 (90.4%) were US-born, and 322 (9.6%) were foreign-born Black people (Table 1). The average BRI, mean ± standard error (SE), was 5.36 ± 0.04. In the univariate analyses, US-born Black people had significantly higher BRI scores than foreign-born Black people, 5.40 ± 0.04 versus 5.00 ± 0.09, P < 0.0001. The frequency of HEI scores that fell in the mid or high categories was significantly higher for foreign-born Black people than US-born Black people (73.03% vs 45.63%, P < 0.0001. Foreign-born Black people were more likely to be married or living with a partner compared to US-born Black people (56.82% vs 40.52%, P < 0.0005). They were also more likely to have more than a high school education compared to their US-born Black counterparts (72.71% vs 55.59%; P < 0.0001).
Sample characteristics of non-Hispanic Blacks by nativity: national health and nutrition examination survey (NHANES 2011–2018 (n = 3341)
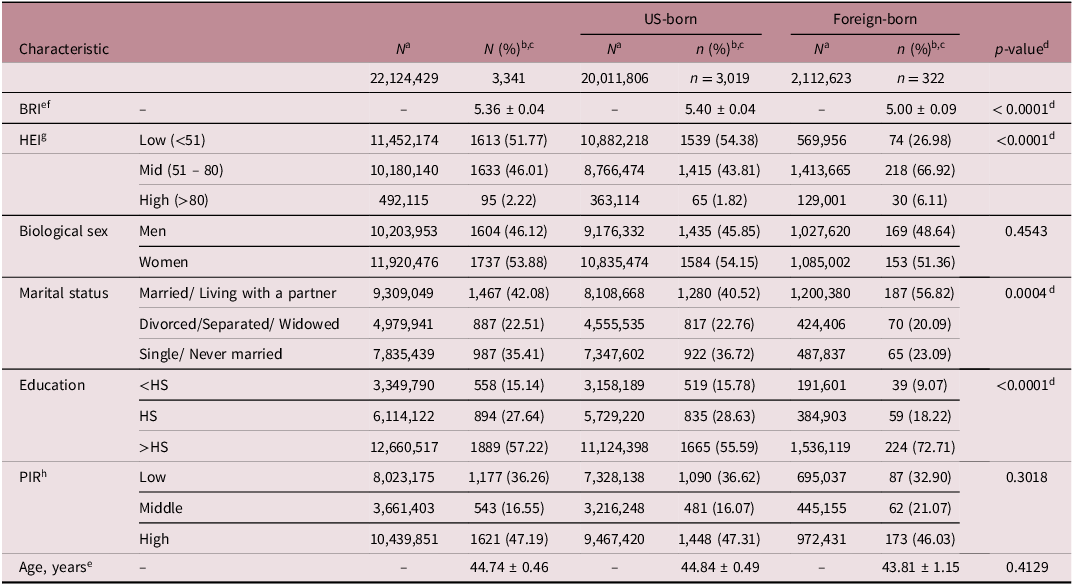
a N = weighted sample number.
b n = sample size.
c % = weighted percentage.
d P-value for Chi-Square and t-tests for each characteristic by country of origin. P < 0.05, significant.
e Mean ± SE; SE, Standard Error.
f BRI = Body Roundness Index.
g HEI, Healthy Eating Index.
h PIR, Poverty-Income Ratio.
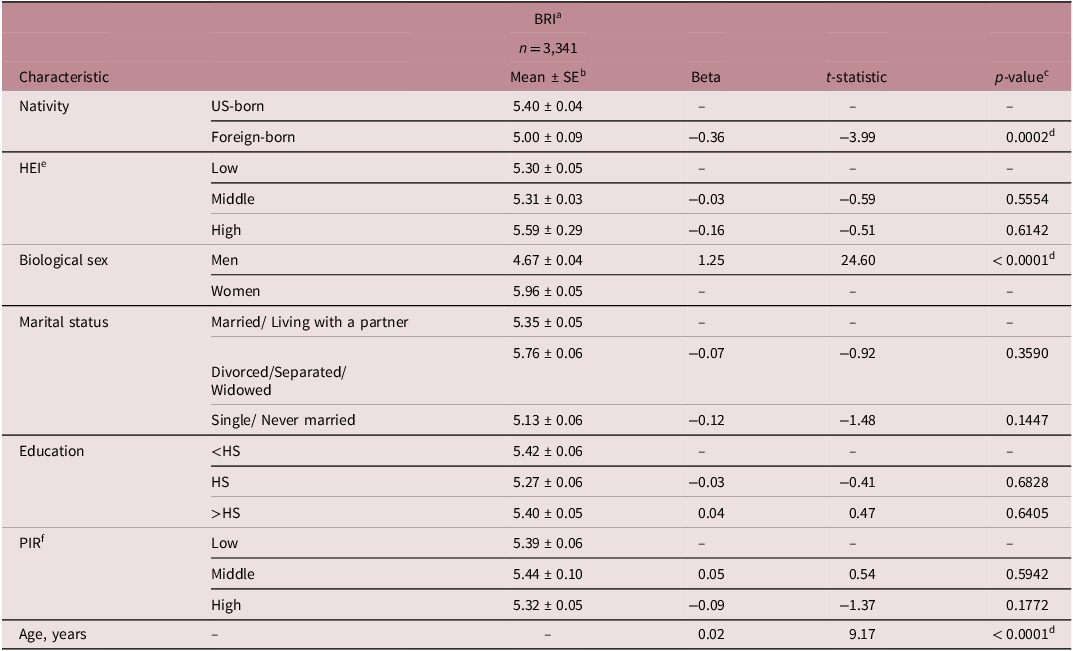
The multiple regression model explained 26.3% of the variation in BRI scores (Table 2). After adjusting for sociodemographic characteristics and HEI, BRI scores were significantly lower in foreign-born Black people when compared to US-born Black people (5.00 ± 0.09 versus 5.40 ± 0.04 ; β = −0.36; t 61 = −3.99; P = 0.0002). (Table 2). BRI did not differ by marital status, education, or poverty-to-income ratio, nor was BRI associated with HEI. There was a significant association between BRI and biological sex, such that men were more likely to have lower BRI than women (4.67 ± 0.04 versus 5.96 ± 0.05; β = −1.25; t 61 = 24.60; P < 0.0001). Additionally, every one-year increase in age was associated with a 0.02-unit increase in BRI (β = 0.02; t 61 = 9.17; P < 0.0001). Lastly, mean BRI increased from underweight to extremely obese; however, the range of BRI scores within each weight category was quite large (Table 3).
Multilinear regression analyses assessing the relationship between BRI and nativity among non-hispanic black people participating in the NHANES, 2011–2018, (R 2 = 0.263)
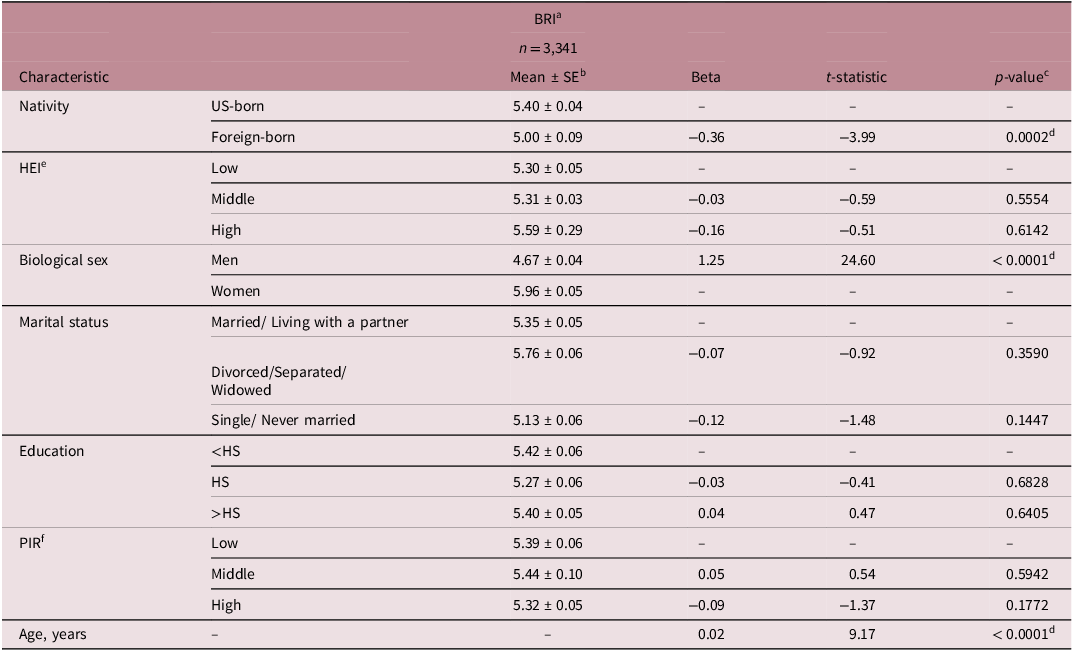
a BRI, Body Roundness Index.
b SE, Standard Error.
c P value for the Multiple Linear Regression Model.
d P < 0.05, significant.
e Healthy Eating Index.
f PIR, Poverty-Income Ratio.
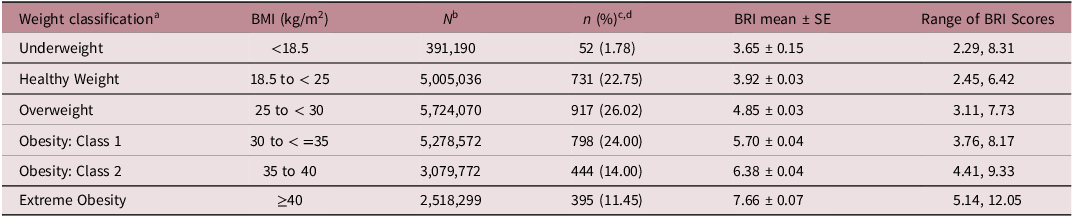
Descriptive statistics highlighting the average and range of BRI scores within the national institutes of health weight classification categories: national health and nutrition examination survey (NHANES) 2011–2018
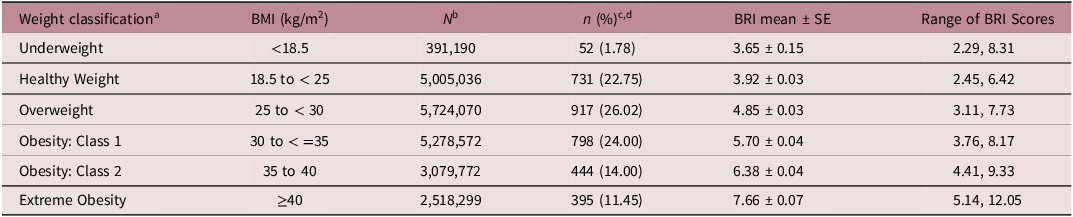
a Weight classification: NHANES participants were grouped by weight classification categories designated by the NIH. 12
b N = weighted sample number.
c n = sample size.
d % = weighted percentage.
SE, Standard Error.
Discussion
In this study, BRI means increased as BMI category increased from underweight (lowest) to extremely obese (highest). A study by Thomas et al. Reference Thomas, Bredlau and Bosy-Westphal5 observed that the mean BRI values increased with higher BMI but decreased when examined by specific BMI classifications. This suggests that while BRI and BMI are correlated, they provide distinct information and are not interchangeable metrics. Table 3 shows a pattern that reveals why BMI alone can be limited as a measure of body composition among the US Black population. Although the mean BRI increases steadily as BMI increases, which is expected, the wide overlap in BRI ranges across categories highlights an important limitation of BMI. For example: Some individuals classified as “Healthy Weight” by BMI (18.5–24.9) have BRI values as high as 6.42, which overlaps with the Overweight or even Obesity Class 1 range. Similarly, participants classified with Obesity Class 1 had BRIs ranging from 3.76–8.17, with the lower end of the range overlapping with the Healthy Weight and Overweight BMI categories. This overlap suggests that non-Hispanic Black people with similar BMI values can have very different body fat distributions or shapes, which BRI captures more directly than BMI. In other words, BMI may misclassify some individuals’ adiposity or health risk, especially among those with similar body weights but different body compositions. Additionally, we found that 49.45% of non-Hispanic Black participants were in an obese category (i.e., the 3 obese categories combined as shown in Table 3) when nativity was not considered.
In this study, BRI was significantly higher for US-born Black people than their foreign-born counterparts. These results are consistent with other research studies where differences in obesity rates between US-born and foreign-born Black people were found using BMI and BMI cut-offs. Horlyck-Romanovsky and her colleagues Reference Horlyck-Romanovsky, Wyka, Echeverria, Leung, Fuster and Huang13 sought to explore how the odds of obesity differed between US- and foreign-born Black persons in New York City. They found that foreign-born Black people had a lower average BMI compared to US-born Black people (27.7 vs 28.6 kg/m2; P < 0.001). The prevalence of obesity was also significantly lower among foreign-born Black people compared to US-born Black people (28.7% vs 35.3%; P < 0.001). However, foreign-born Black people showed a higher likelihood of being overweight relative to US-born Black people (37.7% vs 33.4%; P < 0.001). In another study by O’Connor et al., Reference O’Connor, Thoreson and Ricks14 BMI and waist circumference (WC) measurements were lower for foreign-born Black people compared to US-born Black people. However, after accounting for the differences in either BMI or WC, the foreign-born Black people had higher amounts of visceral fat tissue and lower levels of subcutaneous fat deposits compared to their counterparts (P < 0.01). Even though our results may also suggest that foreign-born Black people have an advantage over US-born Black people with lower BRI and higher HEI scores compared to their counterparts, a study by Commodore-Mensah et al., Reference Commodore-Mensah, Himmelfarb, Agyemang and Sumner15 calls for a need to re-examine research in populations of African descent as some African immigrants may be at higher risk for cardiometabolic disease compared to African Americans.
In contrast to previous research linking HEI with BMI and obesity, we found no significant association between HEI and BRI. A systematic review of 34 studies examined associations between dietary quality indices and abdominal obesity. Reference Asghari, Mirmiran, Yuzbashian and Azizi16 Thirteen of these studies specifically analyzed the HEI across its various editions. The review concluded that higher HEI scores strongly predict lower risks of overall obesity among men in particular. The HEI appears to be a useful diet metric in research and clinical practice to gauge and monitor eating patterns related to obesity outcomes; however, in the current study, the same relationship was not observed with BRI. Nevertheless, foreign-born participants had significantly higher levels of education and better diet quality scores (HEI), both of which are typically associated with healthier weight and lower central adiposity. Notably, the observed differences in diet quality between the two groups may reflect differences in food environments that shaped socialization in early life. A systematic review of 104 studies highlights ethnic and health disparities within US food environments, showing that Black communities experience profound disparities in both food accessibility and quality, resulting in limited access to healthy foods and greater exposure to processed and ultra-processed foods. Reference da Silva Magalhães, Schattschneider and de Vargas17 In contrast, evidence suggests that the traditional diets of immigrants, including those of African descent, are typically nutrient-dense and rich in fiber and whole foods, which confer protective health benefits. Reference Berggreen-Clausen, Hseing Pha, Mölsted Alvesson, Andersson and Daivadanam18 Additionally, a greater proportion of foreign-born Black people were married or living with a partner, a factor linked in multiple studies to better health behaviors and outcomes. Married or partnered adults tend to experience protective effects on physical and mental health, partly because partners often supply social support and shared resources that encourage healthier behaviors. Reference Robards, Evandrou, Falkingham and Vlachantoni19–Reference Wang, Pbert and Lemon21 Social support from household members has been associated with healthier eating patterns and greater involvement in meal planning and preparation, while single adults are more likely to purchase prepared meals or eat away from home. These group-level differences in adjusted variables could contribute to the lower BRI observed in the foreign-born group seen in our study.
Our results also showed that non-Hispanic Black women were more likely to have a higher BRI than men. The study by Liu et al. Reference Liu, Liu and Guan22 found that the optimal BRI cut-off point for higher risk of hypertension was 4.62 across the general hypertensive population. However, this threshold differed by gender, with a lower cut-off of 3.86 in men and higher cut-offs of 4.01 and 5.08 in pre-menopausal and post-menopausal women, respectively. This suggests that typical BRI values tend to be lower in men compared to women, but more importantly, hypertension risk increases at lower BRI among men and higher BRI among women. Additionally, the study by Endukuru et al. Reference Endukuru, Gaur, Dhanalakshmi, Sahoo and Vairappan23 noted that the efficacy of BRI and other anthropometric measures in identifying metabolic syndrome varied between genders.
In this study, there was a positive relationship between age and BRI which suggests that as age increases, there is also an increase in body roundness. Other research studies have shown that increasing visceral fat positively correlates with increasing age, with this relationship being stronger in men than in women. Reference Hunter, Gower and Kane24,Reference Baarts, Jensen and Hansen25 The increased risk of visceral fat with aging may explain the increased risk of metabolic disease occurrence seen in the aging population. In a review paper, Hunter et al. Reference Hunter, Gower and Kane24 argued that the relationship between aging and increasing visceral fat is a result of an overlap in weight gain, muscle loss, and shift in fat distribution, occurring mostly in adults between 20 and 70 years.
Strengths
As the BRI is relatively new in US research, this is one of very few studies examining this measure, especially as it relates to Black Americans. Indeed, this study may be the first analysis solely investigating correlations of BRI across US-born and foreign-born Black people. Also, the dataset and the range of the timeline selected in this study is recent and nationally-representative of Black people in the US.
Limitations
As this was a secondary analysis of cross-sectional data, there are inherent limitations. The single-timepoint design prevents determining if observed associations are causal. Secondly, selection biases, information inaccuracies, or inadequate confounder adjustments may persist. BRI is more difficult to compute and interpret than BMI. Also, it is worth noting that to date, there are no set cut-offs for BRI that identify illness. Furthermore, in this study, while covariates were included and adjusted for, other unmeasured factors could still influence findings. Ultimately, the results should be interpreted prudently. Thus, while we adjusted for key sociodemographic factors and diet quality, other confounders such as cultural differences, physical activity, and healthcare access, which were not measured in this study, may also influence central adiposity and could explain some of the observed differences between the participant groups. Additionally, a key limitation is that NHANES identifies foreign-born status but does not specify country of origin, grouping individuals from diverse regions such as the Caribbean and Africa. This lack of detail may limit interpretation and generalizability of BRI differences by nativity. Lastly, this study could not account for the exact duration of residence in the US because the question on length of stay used categorical responses, such as 1–5 years or more than 50 years, rather than years in residence. This limited the ability to calculate a precise measure of time since migration or to refine the nativity variable without substantially reducing the sample size among foreign-born participants.
Future directions
For now, these exploratory findings warrant replication through more controlled research before conclusions are solidified. Further research can confirm if dietary factors directly mediate the relationship between nativity status and BRI. Also, future research should explore foreign-born subgroups where possible to deepen understanding of differences in the group. Furthermore, future waves of NHANES should attempt to collect data on a larger sample of foreign-born individuals.
Conclusion
The findings suggest that nativity could play a significant role in the occurrence of central adiposity in the non-Hispanic Black population, which could result in the development of cardiometabolic diseases in later life. In this study, while obesity rates were high among both US-born and foreign-born Black people, US-born Black people had greater central adiposity, measured by BRI, than their foreign-born counterparts. The available evidence also indicates that BRI increases with age, and BRI values were generally higher in women compared to men. These findings underscore the potential screening utility of BRI as an alternative tool or used in tandem with BMI to enable preliminary determination of centralized obesity in the Black population. Also, although these findings are preliminary and more research is needed, they highlight a potential opportunity for researchers and healthcare professionals to cultivate targeted health promotion strategies with a dual emphasis on sustainability and outreach. Specifically, efforts could focus on maintaining positive health behaviors to maintain low central adiposity among foreign-born Black people who may lose precedence for health due to acculturation. Concurrently, improving engagement in physical activity and building awareness of obesity-related risks should be prioritized among US-born Black people.
Acknowledgments
None.
Author contribution
The first author (DG) conceptualized the research topic, conducted most of the statistical analyses, took the lead on drafting and revising the full manuscript while integrating co-authors’ feedback, and submitted the manuscript for publication. The second author (LK) contributed substantially to the data analysis and the interpretation of results. LK provided feedback on the manuscript and supervised the first author throughout the research process. The third author (JL) was key in conceptualizing the research topic, including research questions, and refining the full manuscript. JL offered critical feedback throughout the research process and mentored and supervised the first author.
Financial support
The authors did not receive any financial support from a funding agency, commercial sector, or non-profit organization.
Competing interests
None
Ethical standard
Ethical approval was not required for this study, as it involved secondary analysis of publicly available, de-identified data from the National Health and Nutrition Examination Survey (NHANES). The dataset was accessed through the Centers for Disease Control and Prevention (CDC) website (https://www.cdc.gov/nchs/nhanes/) and all analyses were conducted in accordance with relevant guidelines and regulations.

 Open access
Open access