


Introduction
Residency is a critical time in developing skills and knowledge during medical training. Many practices are acquired through apprenticeship and modeling, with new experiences in team dynamics, shared decision-making, end-of-life care, life-altering discussions, and the interpersonal conflict that can develop from this interplay. The core of residency training focuses on medical knowledge and practice, wherein ethics discussions are often considered a complimentary tenet of learning but not central to residency education. The Accreditation Council of Graduate Medical Education (ACGME) requires that pediatric residency programs provide professionalism and ethics education during trainingFootnote 1; however, there is wide variation among programs in how that education is delivered, as there are no standardized ethics curricula for pediatrics residents. Ethical climate and moral distress are interrelated in the medical workplace,Footnote 2 and this has been particularly so in medical training.Footnote 3 “Moral distress” was first coined by Andrew Jameton in 1984 and described as the psychological distressed caused by knowing the right thing to do but being unable to do the right thing.Footnote 4 In 2012, Wendy Austin described moral distress in healthcare professionals as “experiences of frustration and failure in fulfilling moral obligations inherent to their fiduciary relationship with the public.”Footnote 5 For resident trainees, there is an added potential for conflict as a trainee’s decisions are guided by attendings, while they are still developing a framework for approaching both moral distress and ethical conflicts independently and as part of a healthcare team. Developing this framework is essential for trainees to navigate and maintain their relationship with their patients and the public, as this relationship is crucial to effective care and to supporting a provider’s sense of duty and fulfillment.
There are several studies that illustrate moral distress is prevalent in residency. As Ross Hilliard et al. state, “the ethical conflicts [pediatric residents] face more often relate to their training, their inexperience and the hierarchical structure of the medical education program.”Footnote 6 Studies have shown that moral distress in residents not only persists but is higher than that measured in their counterpart attendings.Footnote 7 Jeffrey T. Berger emphasizes the importance of addressing moral distress in medical education and training, stating “moral distress is a silent epidemic that undercuts efforts to promote professionalism and to sustain empathetic physicians.”Footnote 8 Despite Berger’s warning, few studies have shown meaningful methods for reducing moral distress in residents. In conducting this pilot study, we hypothesized that pediatrics residents would experience reduced moral distress through discussion of ethics cases, they developed, and presented in a peer-group setting with multidisciplinary expert contributions. This format would enable residents to develop the tools and processes necessary to successfully address challenging situations that often lead to moral distress.
Approach/intervention
Curriculum development
Following a framework described by Paul Helft et al. for facilitated ethics conversations for bedside nursing staff,Footnote 9 we proposed a novel case-based ethics curriculum to be presented at residency program-sponsored weekly noon conference-style educational conferences led by a pediatrics resident and mediated by a member of the hospital ethics committee. Each case consisted of a case description, an outline of ethical concerns in the case, points and counterpoints by multidisciplinary consults involved in the case, a discussion of ethical frameworks to address the issues, a conclusion, and concluded with an American Board of Pediatrics-style question to test comprehension. By having residents bring forward cases they had personally experienced, we hoped to create a sense of community and shared experience among the session “leaders” and “learners,” as well as ensure that we were not only addressing objective ethical conflicts but also exploring the resident experience in their unique role as part of the healthcare team. We emphasized and incorporated an interdisciplinary approach to each case by inviting nonmedical professionals to participate and share their expertise and perspectives: for example, for a case regarding underage sexual activity, we invited social workers employed by the Department of Child Services; for a case regarding financial stewardship, we discussed the case with the hospital Chief Financial Officer. Five of these live, in-person 1-hour case discussion sessions were presented over 5 months in the 2018–2019 academic year.
There are several unique factors that must be considered in teaching residents, which had previously been well-described by Douglas Diekema.Footnote 10 The sessions were made more accessible to residents by incorporating them into daily existing educational conferences and did not require prereading. Each session was self-contained, and attendance at other sessions was not required to be beneficial.
With institutional review board approval, a total of 140 pediatrics and combined pediatrics (medicine-pediatrics, emergency medicine-pediatrics, triple board, child neurology) residents at Indiana University that attend a daily educational conference were invited to participate in the study. Residents were encouraged to submit de-identified cases they have personally experienced and would like to discuss. The case and discussion were developed by the resident under the guidance of an ethicist and included a brief overview of an ethics topic to provide a framework for approaching the case. Though each case was unique, the goal was to cover basic concepts in biomedical ethics including autonomy, beneficence, nonmaleficence, and justice, as well as topics unique to pediatrics including periviability, parental duties and rights, informed consent, and transplant. A total of five sessions were completed as part of our intervention. Each discussion included 1–3 American Board of Pediatrics board-style questions related to ethics.
We aimed to determine (1) how ethics case discussions and guidance are valued by residents, (2) whether such a program affects ethics knowledge and perceived moral distress, and (3) to evaluate residents’ perceived moral distress before, during, and after a 5-session case-based ethics discussion series.
Evaluation
We performed baseline (“Baseline”), peri- (“Session”) and postintervention (“Final”) survey measurements. The Baseline and Final survey measures included the previously validated Test of Residents Ethics Knowledge, specifically Pediatrics (TREK-P, Supplement 1),Footnote 11 as well as a rating on the Moral Distress Thermometer (MDT) (Supplement 2)Footnote 12 related to experiences over the prior three months, and a Likert-scale question set that covered subjective ethics experiences by the residents (Supplement 3). With each session, participating residents were asked to complete an MDT related to their current experience, as well as a session evaluation (Supplement 4). Open-ended responses for session improvement were also recorded.
Residents were compensated with a $5 gift card for completion of each session survey and an additional gift card for completing Baseline and Final surveys. To encourage data completion by as many participants as possible, anyone who completed all session surveys as well as Baseline and Final surveys was entered into a raffle for an additional gift card.
Outcomes
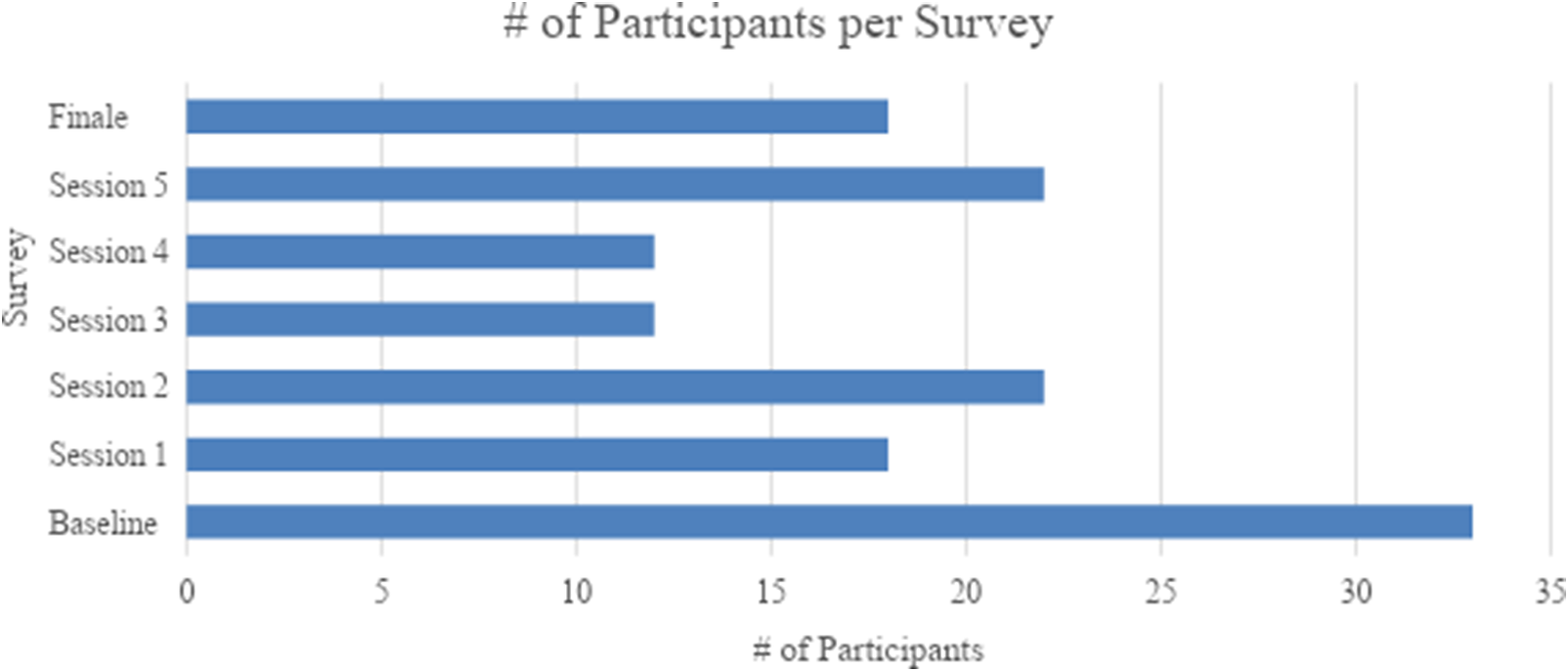
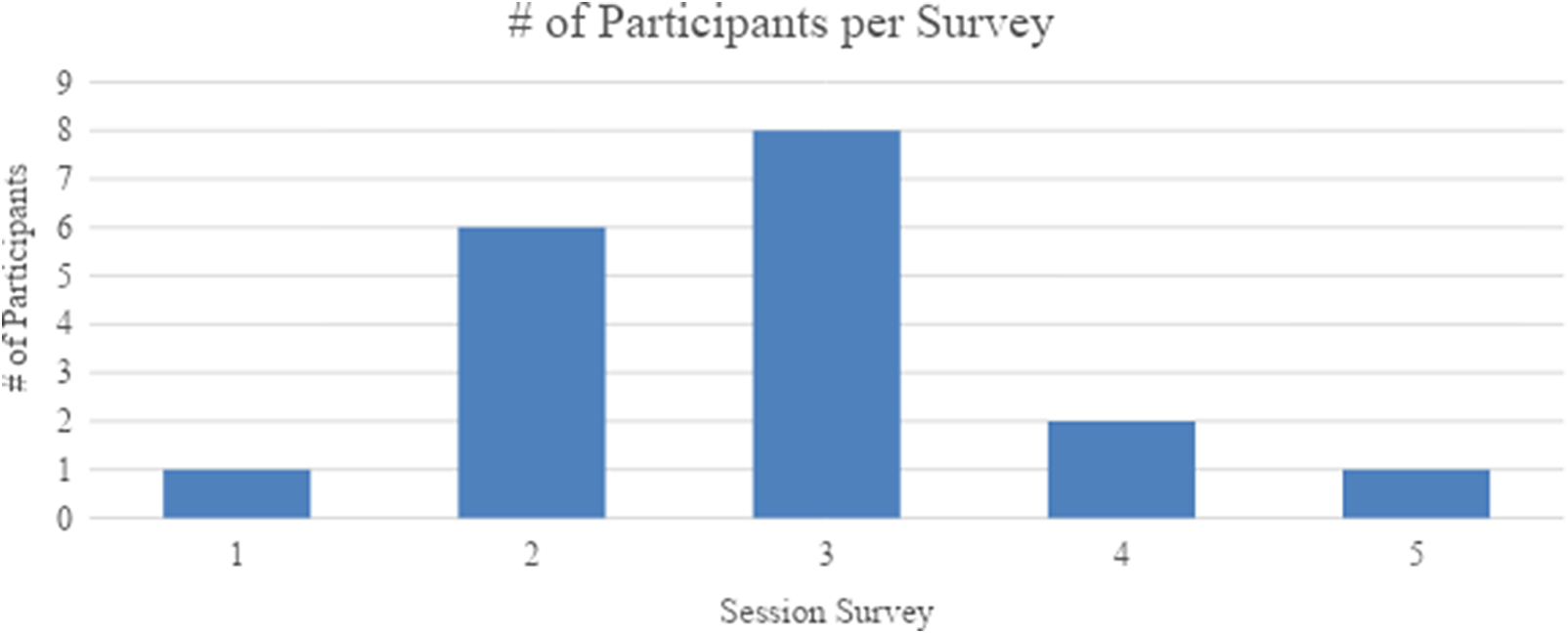
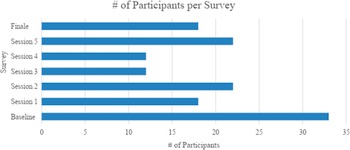
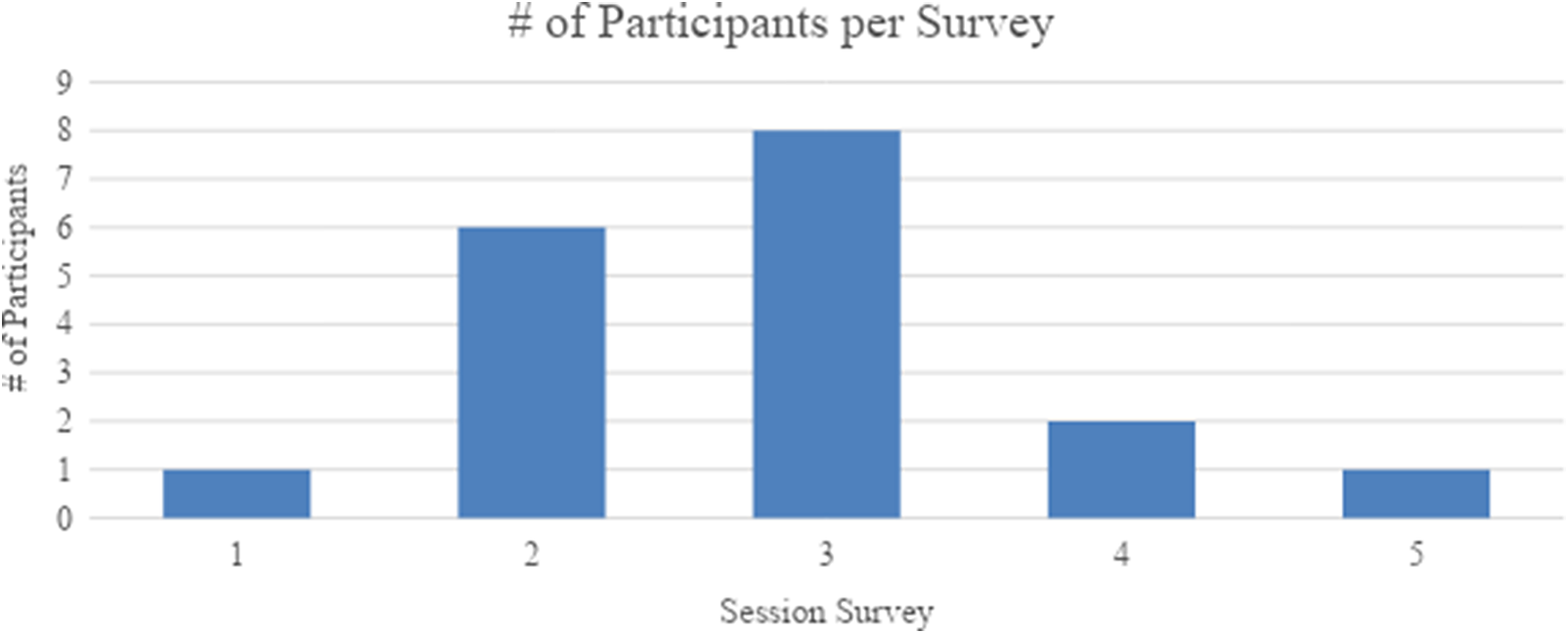
A total of seven surveys were distributed. The Baseline survey was distributed prior to any session. Each Session survey was distributed after the respective session was conducted. The Final survey was distributed once an ample amount of time was given for session five participants to complete the questionnaire. A total of 137 survey responses were received from all questionnaires. The number of participants per survey is displayed in Figure 1. Of a total of 60 unique participants, 11 participants completed the Baseline and Final survey along with three or more individual session surveys. These participants’ survey completion rate is displayed in Figure 2.
Number of participants per survey. Baseline survey received a total of 33 responses. Session 1 and final surveys received 18 responses each. Session 2 and 5 surveys received 22 responses each. Session 3 and 4 surveys received 12 responses each.
Number of completed session survey responses per survey. Eleven participants completed both Baseline and Final surveys and participated in at least three or more sessions. These 11 participant survey responses per survey are scattered throughout session occurrences but are particularly high for sessions 2 and 3.
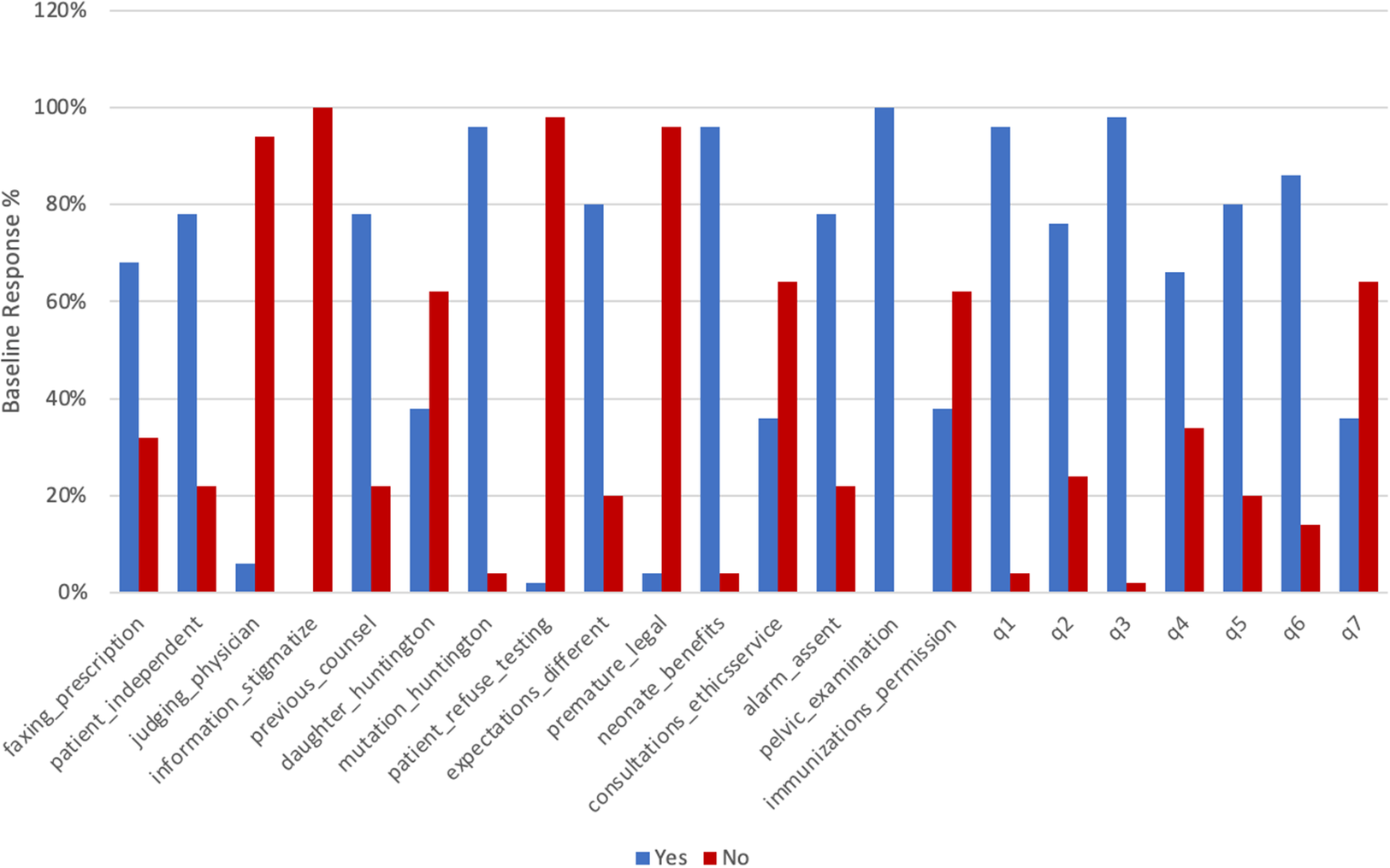
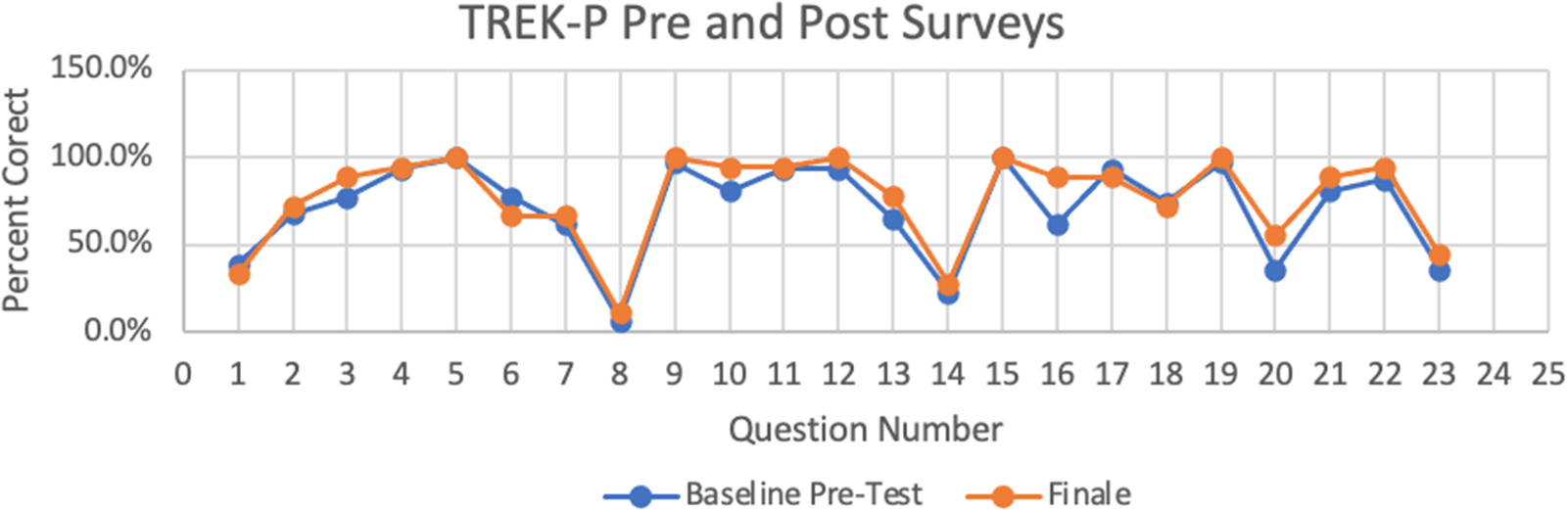
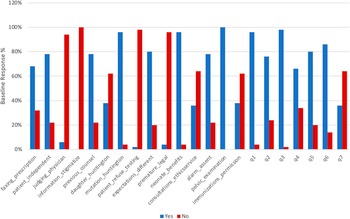
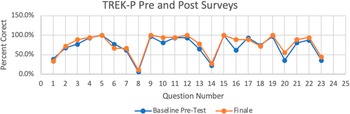
By comparing Baseline responses (Figure 3) to Final responses (Figure 4) of the TREK-P, response rates for each question in Supplement 1 can be compared. From the Baseline survey to Final survey, frequency of the majority response increased. After attending at least one ethics case discussion session, the answer in the majority increased as if confidence in responses increased. After the Fisher exact test, the only question that approaches significance is “immunizations_permission” as its p-value approaches 0.05 (Figure 5.) The rest of the data’s p-values are larger than 0.05, yielding no significant difference between the two datasets.
Baseline TREK-P response rates.
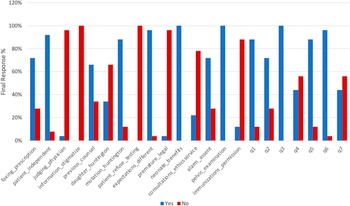
Final survey response rates.

Comparison of Baseline and Final TREK-P surveys. Ethics knowledge among this cohort was similar before and after the 5-session series. The only question approaching significance was question 16 (parental refusal of vaccination).
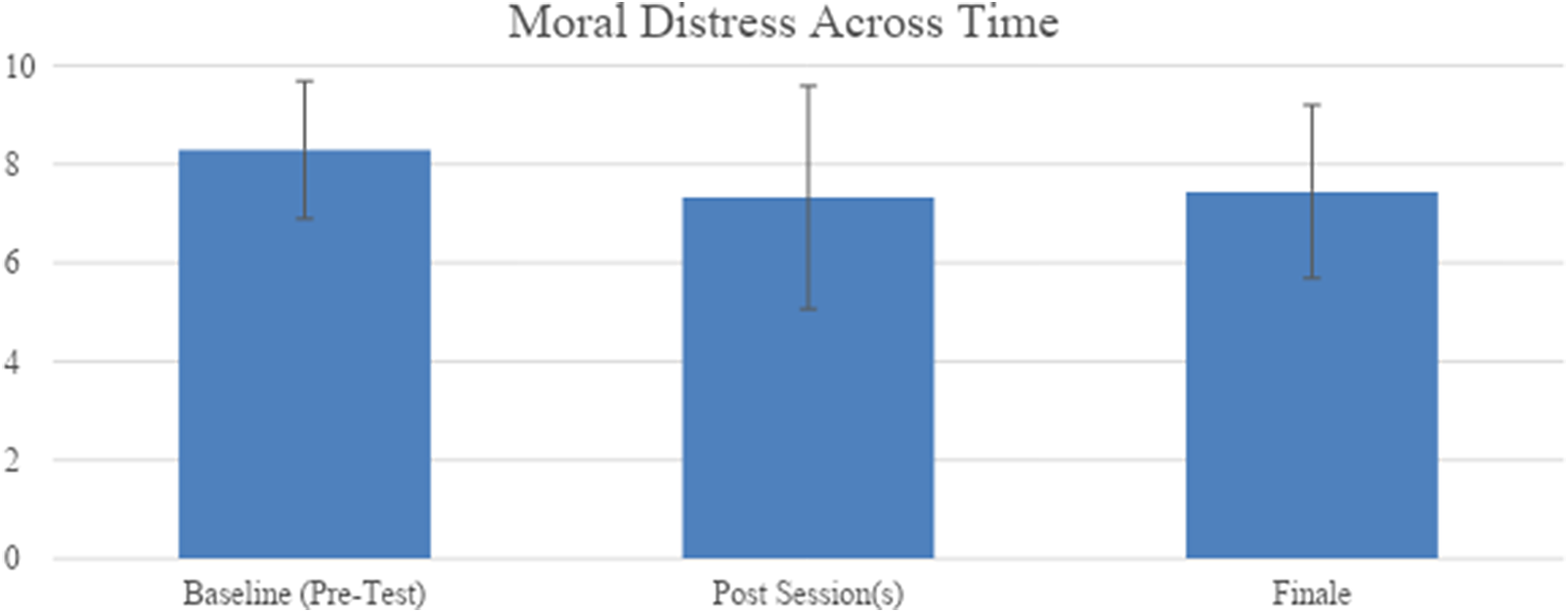
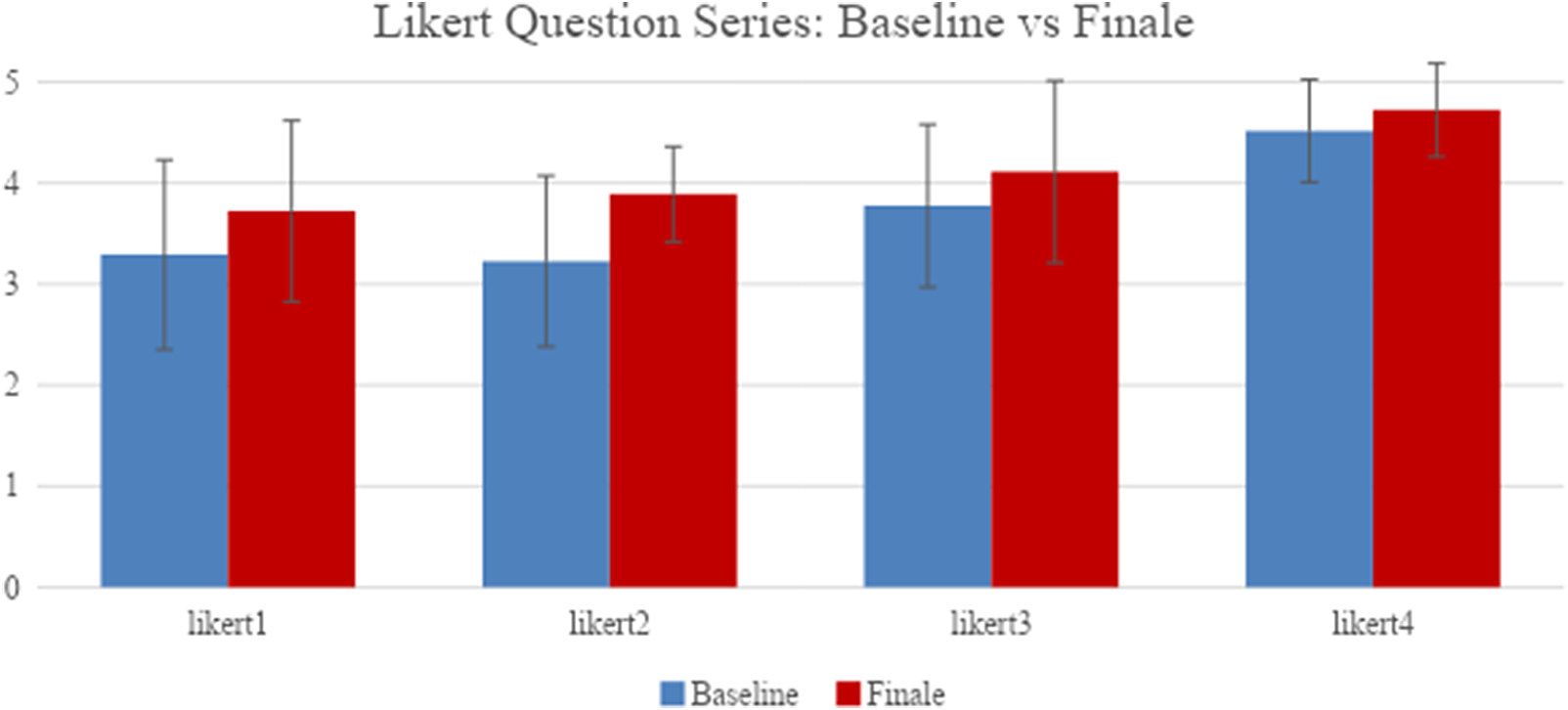
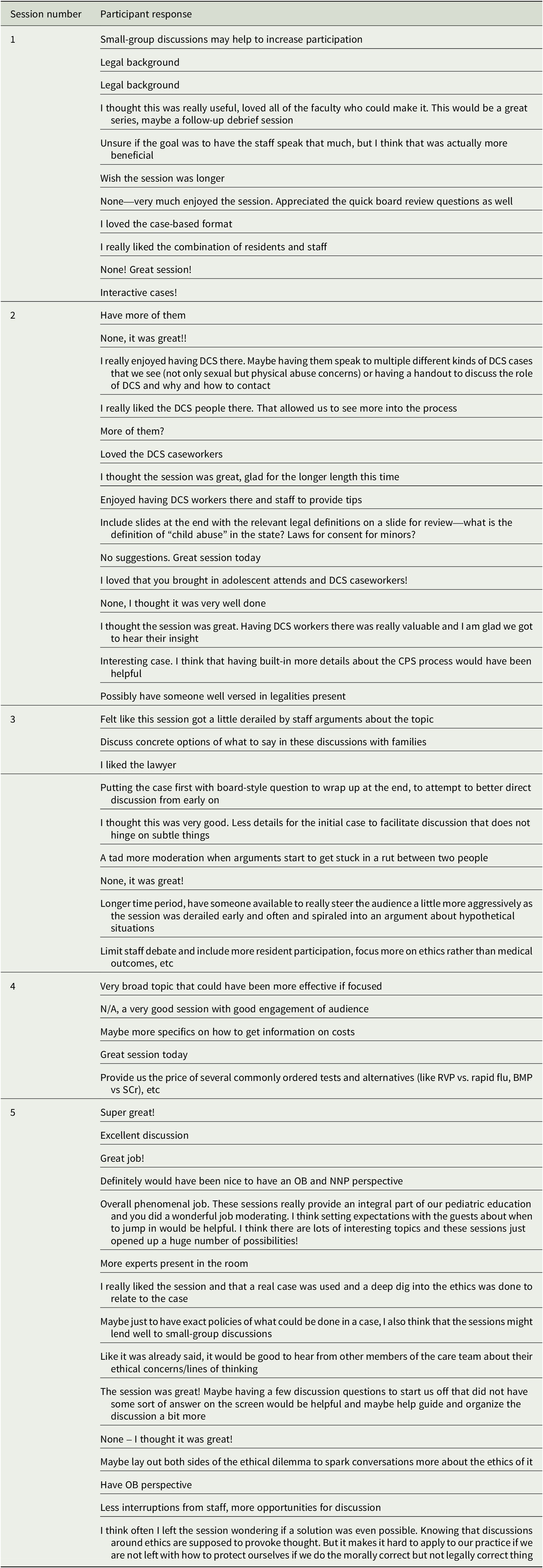
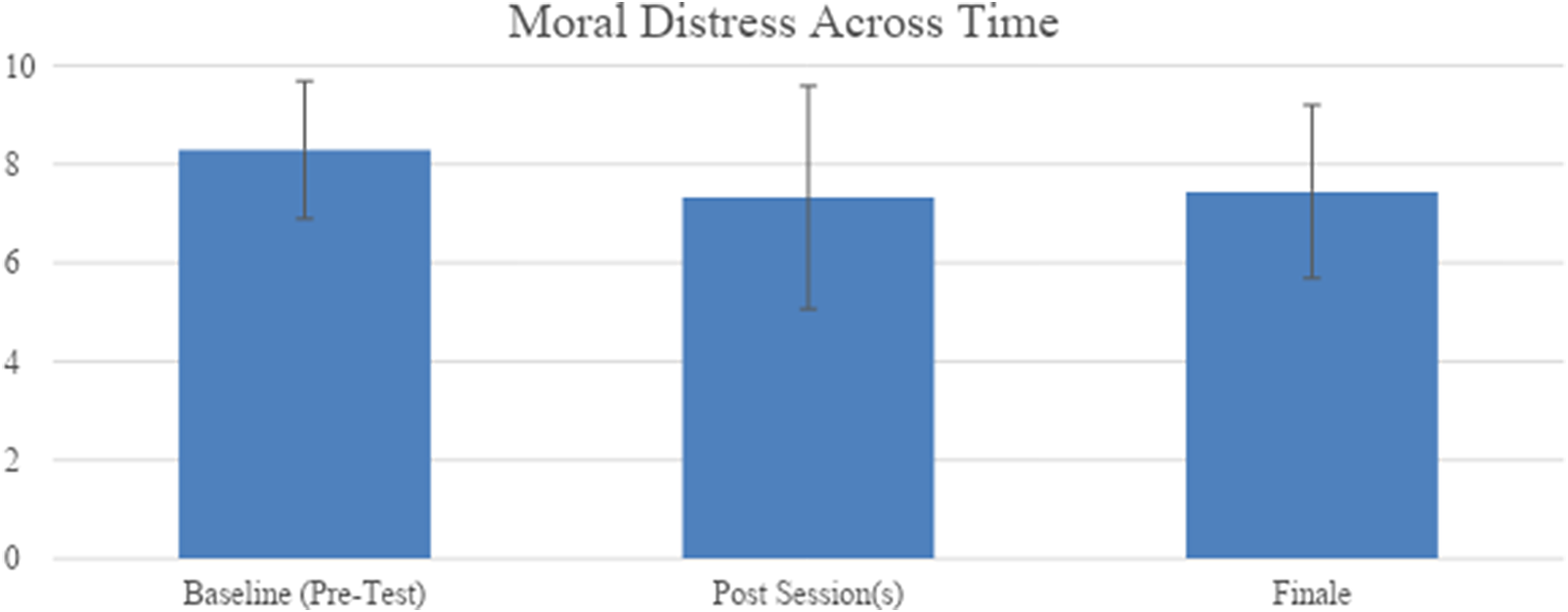
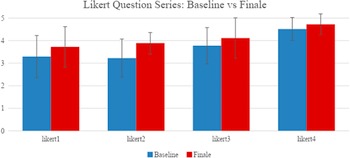
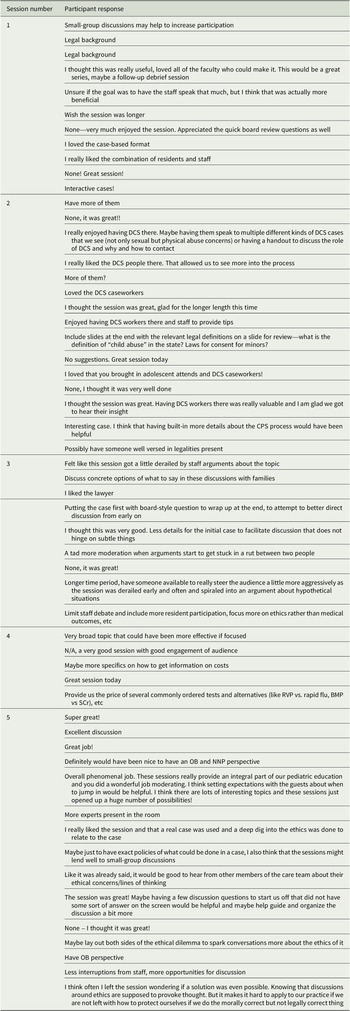
While not significant, a 10.2% decline was observed in resident moral distress (Figure 6). When comparing Baseline and Final responses, the only significance was increased preparedness to navigate ethical decisions (p = 0.004). (Figure 7). An increase in ethics knowledge was observed but was not significant. There were 86 total free-text submissions demonstrating a preference for case-based discussions and multidisciplinary input (Table 1). Residents expressed a desire for more sessions, time for small-group discussions, and legal insight (Table 1). Satisfaction was high overall with 90.7% of respondents feeling better prepared to address ethical concerns.
Perceived resident moral distress over time. Participants report experiencing an average rate of 8.29 ± 1.40 during the time of completing the Baseline test, 7.33 ± 2.26 postsession 1, 2, 3, 4, or 5, and 7.44 ± 1.76 during the time of completing the Final survey.
Comparison of Baseline to Final responses to addendum 3. A Wilcoxon rank sum test (two-sided) was used to compare the Baseline to Final survey responses. Question Likert 2’s p-value is less than 0.05, which means the difference between the baseline and finale is significant for this individual question. The other three questions do not have significant differences as the p-values are bigger than 0.05.
Participant responses after individual sessions. A total of 86 free-text participant responses were collected from five surveys distributed after each individual case discussion session. Responses that were blank or consisted of “None” or “N/A” have been removed, including seven from session 1, seven from session 2, three from session 3, seven from session 4, and seven from session 5. The remaining 55 responses are included here.
Discussion
Our findings showed an increase but not a significant change in ethics knowledge related to our sessions but did show a significant increase in resident’s sense of preparedness for dealing with ethical conflicts. Though not statistically significant, a 10.2% reduction in moral distress was observed from Baseline to Final (Figure 6). Though this is likely multifactorial, including progression through residency, clinical volume, rotation intensity, and personal factors, we postulate that the combination of increased ethical preparedness and decreased moral distress is consistent with our hypothesis.
In addition to the importance of ethical discussions in developing a framework for future clinical practice, we felt that the types of cases discussed were essential to successful participant engagement and learning. To this end, we only discussed cases that were personally experienced by the resident presenting the case and provided a personal connection to the audience. Our goal was to establish a sense of community among residents in that we all experienced and struggled with these cases, but also to identify ethical conflicts in our daily practice, and relevant to our training and well-being as providers. We felt that this structure was unique and essential to the structure of our pilot project. The project was well-received by most participants and requested to be an ongoing part of training at the program. By commentary, one of the most favorable aspects of the curriculum was the involvement of nonmedical personnel, including hospital social workers and DCS case workers, a lawyer, the hospital CFO, and ethicists with a variety of clinical background training (adult pulmonary critical care medicine, neonatology, palliative care, pediatric pulmonology).
Strengths of our single-center pilot study included buy-in and encouragement from the Pediatric Residency Program leadership, enthusiasm from current pediatrics residents and involvement of residents in self-directed learning from cases with ethical dilemmas.
Our study faced several limitations and challenges. To make our curriculum as accessible as possible to our participants, we were only able to conduct a limited number of sessions during the academic year, competing with other didactic lectures for convenient scheduling. Additionally, conference attendance can be affected by changes in monthly rotation expectations and clinical volume; therefore, consistent attendance at all sessions was challenging. Together, these likely contributed to our overall low number of survey responses, limiting our effect size and statistical significance. All cases had a more robust attendance (estimated at about 20 participants each) regardless of the number of surveys completed, although this was not directly measured as part of the study. The lack of statistical significance could have been due to a low number of participants since this was a pilot project. It would be important to see whether a higher number of participants would yield a different result.
Conclusion and next steps
Pediatric trainees face ethical dilemmas during training that cause moral distress. Residents feel that understanding ethics is relevant to their practice. While residents desire case-based ethical discussions, this format does not by itself decrease moral distress in this pilot study. This study highlighted ethical concepts where residents desired further education. This curriculum is ongoing, as cases continue to be developed by pediatric residents in this format. Case presentations are stored in a central repository for future use. As the curriculum grows, we plan to map the cases to specific American Board of Pediatrics board examination topics. More data are needed to learn how this approach fits with the larger goal of increasing pediatric resident ethics knowledge and decreasing perceived resident moral distress during training.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0963180124000355.
Acknowledgments
None
Competing interest
The authors declare no conflicts of interest.



 Open access
Open access