


Introduction
Paediatric clinical research has yielded important breakthroughs, particularly in paediatric cancer, polio, and infectious diseases. Most parents agree clinical research advances treatment of paediatric diseases, yet only 25% of U.S. adults said they would allow their child to participate in a research study Reference Marceau, Welch, Pemberton and Pearson1 . Understanding parent and child perceptions is key to developing research studies and preparing for recruitment of paediatric populations, yet understanding what parents and children like or dislike about study participation is often not considered.
Studies have been conducted to learn why parents allow a child to participate in research and to identify differences between parents who consent and those who decline. These show helping others and helping one’s own child are powerful motivators for parents considering participation in research. Perceptions of risk, harm, inconvenience, and knowledge about clinical research processes highly influence parental decisions about participating. 2,Reference Caldwell, Butow and Craig3,Reference Hoehn, Wernovsky and Rychik4,Reference Tait, Voepel-Lewis and Malviya5,Reference Singhal, Oberle, Burgess and Huber-Okrainec6 The literature reveals that most parents who are asked to participate in research feel research is important and carefully balance their desire to benefit society and their child with the perceived risks of participation.
In studies of individuals with CHD, reasons for participation in research studies may differ from those with other less serious conditions or for healthy volunteers. CHD is the most common type of birth defect, with 1 in 4 babies born with a heart defect having a critical CHD. Reference Zupancic, Gillie, Streiner, Watts and Schmidt7 Infants with critical CHDs generally need one or more surgeries and other invasive procedures in their first year of life. Given the significant morbidity and mortality associated with critical CHDs, research is essential to learning new strategies for delivering optimal care. Reference Oster, Lee, Honein, Riehle-Colarusso, Shin and Correa8
The Pediatric Heart Network, a collaboration of children’s hospitals in the United States and Canada, conducts research with children who acquire heart disease and individuals born with a heart defect. Similar to many other diseases and conditions, participation of parents and their children in Pediatric Heart Network research is vital to answering important scientific questions. Little is known about parental and adolescent perceptions after participation in paediatric cardiology research. Therefore, we developed an ancillary study to the Fontan Udenafil Exercise Longitudinal Assessment (FUEL) Randomised Controlled Trial and its Open-Label Extension study. The FUEL Trial focused specifically on children with single ventricle who had undergone a Fontan procedure. It was a randomised, double-blind, placebo-controlled clinical trial of twice-daily medication over a 6-month period. The study included two in-person visits and 12 phone calls over 26 weeks. Included were a blood draw, echocardiogram, exercise test, questionnaires, and an endothelial peripheral Arterial Tonometry (EndoPAT ®) at the in-person visits. In the open-label extension trial of the FUEL Trial, all participants received Udenafil twice daily and underwent the same testing at baseline and week 52, with two in-person visits and 14 phone calls. The purpose of this study was to understand research participant and parental perceptions of study communication, study team, medical care, study procedures, and study expectations. Additionally, we wanted to learn what would compel individuals to participate in future studies.
The use of surveys has become common practice in both the clinical and research settings. Combining qualitative research to develop the survey and quantitative research to analyse the responses helps answer questions that cannot be addressed by one method alone. Although it is not mandatory that a survey be validated, it is important to validate survey questions to ensure they measure what they are intended to and produce reliable results.
The surveys (See Appendices 1 for the parent survey and 2 for the adolescent survey) were designed to capture and evaluate how adolescents and their parents viewed their participation in a research study, what would compel them to participate in future studies, and what researchers could do to enhance a research participant’s experience. We asked questions related to how they perceived the study procedures, the study team, medical care, and study expectations. The specific aims were Reference Marceau, Welch, Pemberton and Pearson1 to describe participant and parent/guardian perceptions of their participation in the Pediatric Heart Network FUEL trial and during the follow-up in the FUEL open-label extension study based on responses to a survey, 2 to identify changes in participant and parental responses between the final trial visit (6 months post-randomisation) and the final open-label (non-randomised) extension study visit roughly 12 months later, Reference Caldwell, Butow and Craig3 to compare responses from parents to responses from adolescent participants, and Reference Hoehn, Wernovsky and Rychik4 to identify factors associated with participant and parental experience that could positively affect participation in future paediatric research studies. Insights gained from this survey may enhance our understanding of factors that contribute to participant’s satisfaction and identify ways to improve experiences in future studies of children with serious medical conditions and their parents.
Methods
Participants
From 2017 to 2020, a validated survey was offered to all adolescent participants (12–19 years) and their mothers, fathers, and legal guardians at the FUEL final study visit (T1 or approximately 6 months post-randomisation) and again at the open-label extension final study visit (T2 or approximately 18 months post-randomisation).
Perceptions Survey
The Perceptions Surveys were developed to capture and evaluate adolescent participant and parental perceptions of research participation and understand how participants and parents perceived the study procedures, the study team, medical care, and study expectations.
Questions were asked on a 5-point Likert scale from strongly disagree to strongly agree and scored by averaging an ordinal scale from –2 to + 2, with higher scores indicating more positive perceptions. Open-ended questions queried the most/least appealing aspects of study participation and whether respondents would consider future research participation. Respondent and family characteristics were also assessed on the surveys and included relationship to the adolescent and parent’s education. We also asked whether the family had participated in or worked on other research studies.
The validated survey was originally developed using focus groups consisting only of parents. Subsequently, a subgroup of the first 12 consenting participants in our study (one each in age groups 12–13, 14–15, and 16–19 at four sites) participated in an interview to further validate the survey content in the adolescent population. Using an interview guide, the interviewer asked each participant questions to better understand the adolescent’s viewpoints and experiences and to identify any potential content changes required for this population. There were no changes to the survey content made following these focused interviews (cognitive debriefing).
Study design
This protocol was developed by the Nursing Research Committee of the Pediatric Heart Network as an ancillary study to the FUEL Trial. The Perceptions Surveys were an optional component administered to the adolescent study participants and/or their parent(s) at 2 time points (T1 and T2) corresponding to the end of the FUEL and open-label extension studies. The study was approved by the Institutional Review Boards at each of the 14 participating sites. Parental consent as well as participant assent was obtained.
Statistical analysis
Each question was coded into one of five possible ordinal scores ranging from −2 to + 2. Positive scores represent more positive perceptions; some scales were flipped for scoring purposes. Prior to averaging responses across questions, a confirmatory factor analysis was performed to assess whether the survey questions loaded into the four domains from the sections within the survey (i.e., each section should be scored separately): Study Communications and Activities, Study Team, Medical Care, Study Expectations. For both the parent and participant surveys, results suggested the survey responses did not divide into those four separate domains. Therefore, a principal components analysis was performed to determine whether the survey items loaded into any latent factors. Only a single factor (i.e., all survey questions) was identified, with a Cronbach’s alpha of 0.94 for both participants and parents. Therefore, scores (on the −2 to + 2 scale) for each question were averaged to form a single summary score.
T-tests were used to compare adolescent participants versus parents, girls versus boys, and mothers versus fathers at both time points; paired t-tests assessed change over time in adolescent and parental perceptions. Correlations and generalised linear models were used to identify factors associated with baseline perceptions, separately for adolescent participants and parents.
There were three open-ended questions asking what the participants liked best and least about participation in this study and whether they would consider future participation in another study. Responses were categorised into several common themes (see Table 1).
Responses to open-ended questions regarding likes, dislikes, and future participation at time points 1 and 2 (T1, T2)

Results
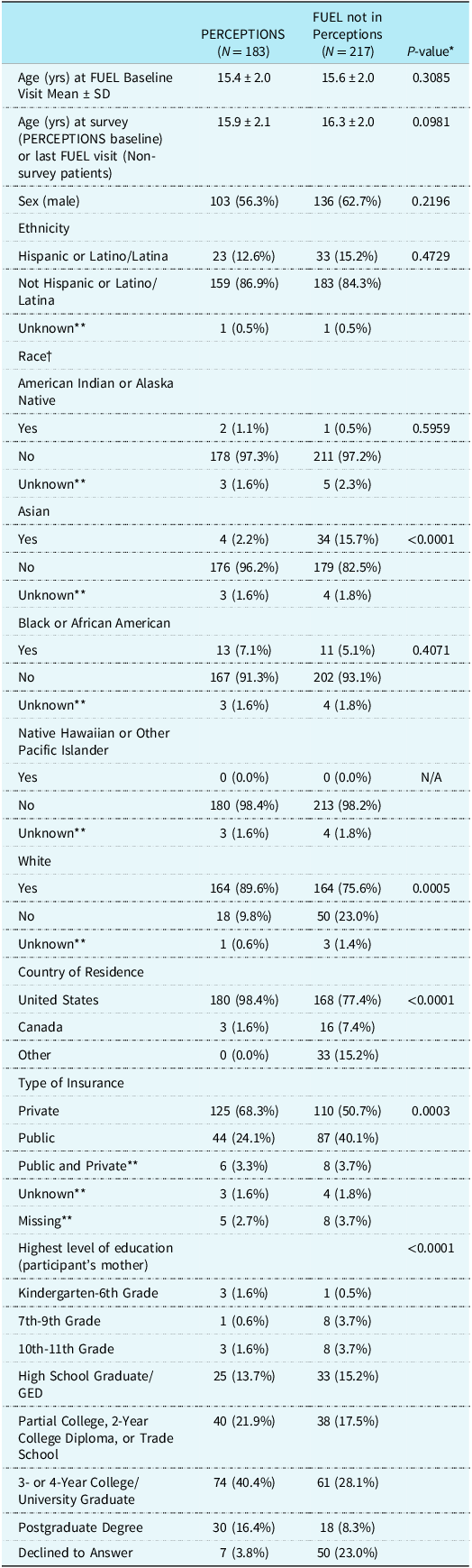
At T1 (6 months after randomisation), among 250 FUEL participants at 14 participating centres, we received 179 adolescent (56% male) and 183 parent surveys (85% mothers), including 170 child-parent paired responses. The participants were aged 15.9 ± 2.1 at enrolment into the Perceptions Study. The majority were white (89.6%) and 12.6% were of Hispanic or Latino/Latina ethnicity. Most were privately insured (68.3%) with the mothers having obtained at least a 3- or 4-year college/ University degree (56.8%) (Table 2). Compared to those eligible but not enrolled, participants were more likely to reside in the United States and have private health insurance, but no other significant differences were noted.
Patient demographics (PERCEPTIONS vs. FUEL not in perceptions)

* T-test for continuous variables, Fisher’s exact test for categorical variables.
** Parameter not utilised in statistical test.
† Race was asked separately for each category. Patients may have no race indicated, or multiple races indicated.
There were generally positive perceptions of participation in research, with the study team receiving the highest scores and medical care the lowest scores (but still positive) (Supplemental Table 2). Perceptions scored on the −2 to 2 scale demonstrated high perceptions of 1.35 ± 0.45 for adolescent participants and 1.56 ± 0.38 for parents at T1 (Figure 1). There were no significant differences in perceptions between adolescent females versus males (1.37 ± 0.46 vs. 1.33 ± 0.45; p = 0.59) or between mothers versus fathers (1.58 ± 0.38 vs. 1.43 ± 0.50; p = 0.15), but parents/guardians had slightly better perceptions than participants (p < 0.001). Bivariate analyses of covariates to summary scores for adolescents and parents revealed few significant predictors for parents (Supplemental Table 1). Older age of the child was associated with lower parental perceptions (correlation = -0.16, p = 0.03). Consenting to open-label extension was associated with slightly higher perceptions (1.40 vs. 1.18, p = 0.005 for adolescents; 1.62 vs. 1.42, p = 0.015 for parents).
Perceptions were averaged over survey questions on a scale of −2 to 2, with higher numbers indicating higher/more favourable perceptions. Both groups had high perceptions of study participation, with slightly higher perceptions for parents (p = 0.001 at both time points).

At T2 (18 months post-randomisation), survey responses were received from 121 adolescents and 114 parents. There were 112 child-parent paired responses demonstrating generally positive perceptions of participation in research: 1.39 ± 0.51 for participants and 1.58 ± 0.37 for parents (Supplemental Table 3) There were no significant differences in perceptions between adolescent females versus males (1.40 ± 0.54 vs. 1.38 ± 0.50; p = 0.85). However, there were differences between mothers (1.62 ± 0.35) and fathers (1.36 ± 0.43; p = 0.004). Among adolescents (N = 120) and parents (N = 102) who completed both T1 and T2 surveys, overall perceptions dropped very slightly from FUEL to open-label extension for parents (p = 0.03) but not for adolescents (p = 0.71). Parents had a 0.06-point drop which was statistically significant (p = 0.03), yet the overall score remained high (1.66 at T1 vs. 1.61 at T2). Furthermore, we found slightly higher perceptions among those who completed surveys at both time points compared to those only completing surveys at a single time point.
Common themes from open-ended responses at both T1 and T2 (Table 1) included liking to help others and themselves, liking the study team, and disliking study burden. Adolescents also commonly liked the compensation and disliked study-related test.
Discussion
Overall, the perception of participation in the FUEL/FUEL open-label extension Trials was positive and participants believed the study to be important to them and other families in the future who face a diagnosis of CHD. The study identified specific activities that participants particularly liked (helping others and the study team) and did not like (study testing).
Study communication
Communication plays an important role in research. Our survey was designed to assess communication between the study team, participants, and their parents by asking questions such as, “Before the study started, I felt the study team gave me enough information” and “I knew who to talk to if I had a question.” Both participants and parents responded with over 90% agreeing the study team had communicated well. However, when asked, “I knew I could leave the study at any time,” 10% of participants were not aware they could leave the study, while parents clearly understood (96%). This points out the importance of clear communication and understanding for both the participant and parent. Marceau and colleagues point out in their study that parents “thought it important to know that they can withdraw from a study any time.” Likewise, it would be equally important for the participant.
Study team
Both parents and participants reported “liking” the study team. In the open-ended questions, comments were made in direct relationship to specific research coordinators and/or physicians. Comments such as “the coordinator was excellent at explaining things to us,” “they made me feel like my opinions mattered” and “the team was very kind and organised” were seen frequently. In a qualitative study, Luchtenberg and colleagues explored the child-doctor relationship in research. “Trust and familiarity seemed to be particularly important for supporting children whose treatment intersected with the research they were invited for, especially in situations where the consequences were not always foreseeable, such as when children were overwhelmed because they had recently been diagnosed, or when children were to be randomised to receive a specific drug.” Reference Stallings, Isenburg and Aggarwal9 The relationship between the participant and the research team is key, particularly in studies with prolonged duration.
Helping the participant and others
Our study revealed that helping others or helping the participant was the most liked aspect of the study. Many of the participants described wanting to help other children with CHD or help research in general referring to “knowing that I was contributing to a better understanding for future patients” or “knowing that our participation helps advance the research study for a better future that will impact/improve the care for Fontan patients.” Individuals participate in research for a variety of reasons, but our study aligns with several other studies supporting personal benefit or helping others Reference Marceau, Welch, Pemberton and Pearson1,Reference Stallings, Isenburg and Aggarwal9,Reference Luchtenberg, Maeckelberghe, Locock and Verhagen10 as the most common rationale for participating.
Study burden and tests
Study-related testing and burden were the most disliked part of the study by participants and parents, respectively. Engaging participants from the onset in study planning may help to provide valuable input and increase study success. Adolescents with CHD and their families can find it difficult to engage in research perceived to be demanding or requiring significant testing, but research is essential to learning new strategies and to providing optimal care. Hawke, et. al suggest that engaging youth as partners in research may offer benefits for not only the youth but also the research team and that “authentic youth feedback can make many contributions to a research project, notably ensuring a youth-friendly approach to a study, feasibility of recruitment and data collection, the meaningfulness of the results and ultimately project success as a whole.” Reference Crane and Broome11
The Pediatric Heart Network has engaged parent advocacy groups in the development of patient-facing research materials and promoting research studies after development. Engaging participants is not something the Pediatric Heart Network has traditionally done, despite the likelihood that participants could be highly instrumental in the development of protocols to promote the success of clinical trials where enrolment can often be challenging. The Neurodevelopmental and Psychosocial Interventions Working Group of the Cardiac Neurodevelopmental Outcome Collaborative suggests that including stakeholders as partners or advisors can help to ensure that stakeholder perspectives are incorporated into all phases of research. Reference Hawke, Relihan and Miller12 They emphasise that to promote inclusive research, “it is critical to involve community stakeholders in research design and recruitment” Reference Hawke, Relihan and Miller12 In a case study by Orellana and colleagues, they describe the formation of a paediatric advisory board. The committee members participated in quarterly meetings where they provided feedback to researchers on recruitment strategies, study materials, and procedures (14).
Compensation
A common positive aspect of participating in research given by adolescents was the compensation they received. Participants received a welcome gift bag containing items such as a water bottle, pen, T-shirt, and an iPod touch® after randomisation. Parents and participants were compensated for their time and effort after each study visit was completed. Compensation was either by gift card or cash, dependent on what was allowable at each site. They were also compensated for the return of the study medication bottles. In a systematic review of 23 studies, Crane and colleagues found in five of the studies, at least some of the participants thought cash incentives were a preferred form of incentive with rationale being: justice, pleasure associated with receiving cash, and compensation for time spent, discomfort experienced, and effort expended. Reference Luchtenberg, Maeckelberghe, Locock and Verhagen10
Limitations
This study has several limitations. Families were largely a white educated population, although those eligible and not enrolled were similar. The participants in this study are likely not representative of the Fontan population as a whole, but only those who were willing to consent to participate in a randomised clinical trial in the first place, thus the study findings should be interpreted cautiously. Those with more positive perceptions may have been more likely to choose to participate in the survey and those with better perceptions of FUEL may have been more likely to continue into the extension study. Statistical significance may not mean clinical significance, given the small magnitude of the differences. Perceptions were evaluated over an 18-month period and may be confounded due to participants being in a randomised clinical trial and subsequently in an open-label drug trial.
Conclusions
Perceptions of research were positive for both adolescents and parents, but slightly better for parents. Both reported they would consider participation in future research and outlined specific details about the barriers and facilitators to participation. Understanding what participants value and dislike can help to frame future research protocols with similar age groups. Engaging participants from the onset in study planning may help to provide valuable input and increase study success in not only future research design but clinical practice.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951125001702.
Financial support
Disclaimer: This study is supported by grants (HL135680, HL135685, HL135683, HL135689, HL135646, HL135665, HL135678, HL135682, HL135666, HL135691, HL068270) from the NHLBI, NIH. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the paper and its final contents. The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the U.S. Department of Health and Human Services.
Competing interests
NONE.





 Open access
Open access