

Introduction
Violence in educational or work environments is a behavior that has been increasing, and Mexico is no exception. The behavior seems more common among medical students than in other faculties, perhaps due to the stress of high levels of responsibility they carry for the health and lives of others, where a mistake is intolerable. Among the different forms of abuse of students (undergraduate and graduate), which includes verbal abuse, physical violence, and discrimination based on race, sexual harassment and gender discrimination stand out. In the medical profession, sexual abuse is experienced in a particular way. Medical work is often immersive, and the boundaries between work and social life are blurred. In addition, the risk of both types of mistreatment is higher in hierarchical environments, organizations tolerant of sexual harassment, and when people in authority perpetrate it. Examples of harassment experienced by female medical students worldwide include educational inequities, stereotypical and sexist comments (including sexual jokes), sexual harassment (with inappropriate verbal or physical advances) and inappropriate touching.
We have contact with students and professionals at various stages in the career of the medical surgeon, as well as specialties and subspecialties. We have heard firsthand stories of abuse of power and harassment by physicians towards physicians. Therefore, we are very interested in carrying out a more in-depth study that can substantially impact stopping these acts that have been normalized in teaching medicine and in the path that must be followed to achieve certain career goals.
Gender in Society
Mexico has a total of 126,014,024 inhabitants, of which 51.2% are women. In the case of Mexico City (CDMX), the population is 9,209,944 inhabitants, of which 52.2% are women. Furthermore, the adult population of CDMX between 25 and 69 years old is 5,516,642 inhabitants, 53% of whom are women. All the above data is reflected in the population census conducted by the National Institute of Statistics and Geography (INEGI). (1)
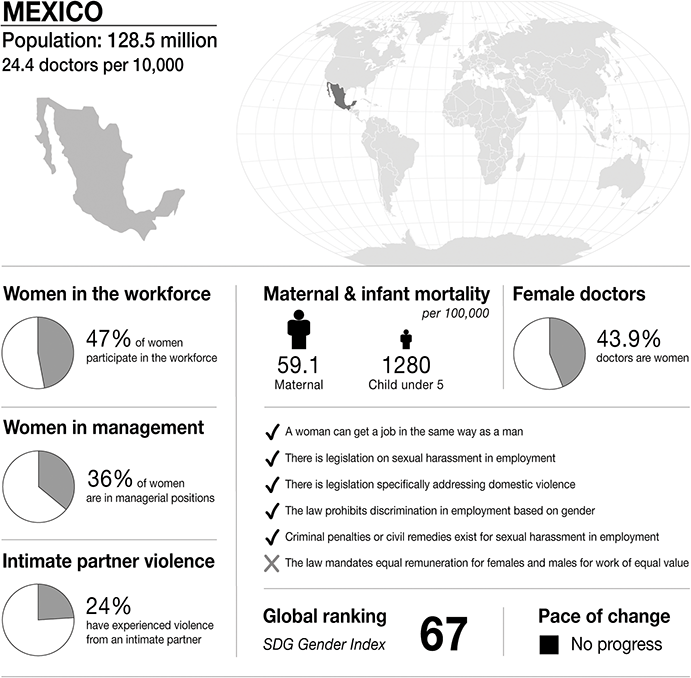
Infographic Mexico. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.
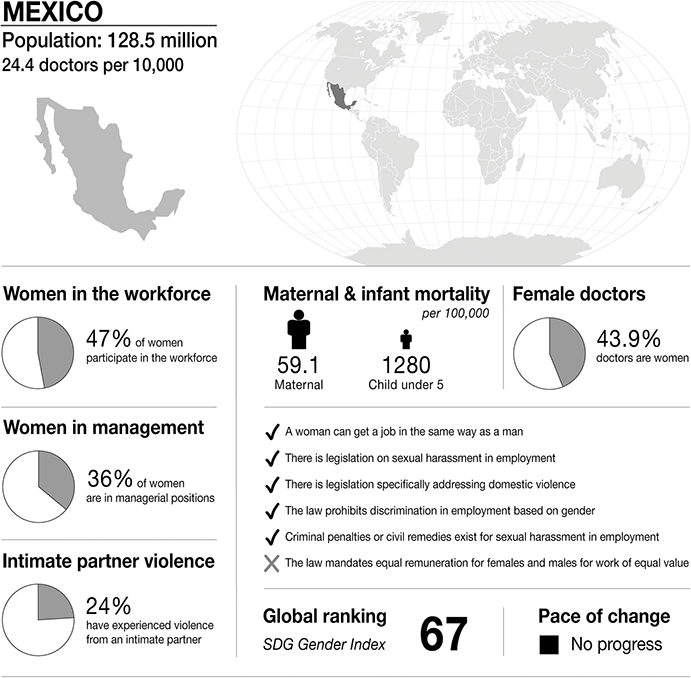
Figure 25.1 Long description
The infographic provides information about Mexico, with a population of 128.5 million and 24.4 doctors per 10,000 people. It highlights several gender-related statistics. 47 per cent of women participate in the workforce. 36 per cent of women are in managerial positions. 24 per cent of women have experienced intimate partner violence. Maternal mortality is 59.1 per 100,000. Infant mortality under 5 is 1280 per 100,000. 43.9 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Mexico:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– there is no law that mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 67, and is stable.
Considering the above data, we can affirm that there is a slight difference between the number of men and women in the country; however, this gap is exacerbated when we talk about the presence of women and men in positions of power and decision-making. A clear example of this difference and its prevalence was observed when, in 2014, the obligation of political parties to guarantee gender parity for the registration of candidacies to different elected positions was raised to Constitutional rank (INEGI-INMUJERES). (1) In Mexico City, the governor was appointed by the republic’s president, and the position had been assigned only to men. However, in 1999–2000, democratic election was established, and a woman was appointed interim governor. In the 2018 elections, Claudia Sheinbaum Pardo was elected as head of a government of science, and there was likewise a considerable increase in the participation and election of women for the mayoralties of the city. (Reference Fernández Poncela2)
According to INEGI 2020 statistics, 15.1% of the total population in Mexico is indigenous, and half are women. They are doubly discriminated against, first because of their indigenous status and second for gender reasons. Opportunities for indigenous women in labor, political participation, or schooling are very scarce and may even be non-existent in some ethnic groups. In the most challenging situations, some indigenous women who have not reached the age of majority are the object of transactions in exchange for some material good for their families. These acts are shielded using arguments about the uses and customs of various indigenous peoples. (Reference ChandomÍ3)
Gender in Medicine
In Mexico, there has been an increase in the number of women in the medical field. For example, in the last school year, 2019–20, the General Directorate of School Administration (DGAE) of the National Autonomous University of Mexico (UNAM) reported that 33% of the 1,930 students accepted for the career of a medical surgeon were women.
Since the 1990s, the gender breakdown in medical schools has been reversed, and to date, the female sex is predominant. This phenomenon has been dubbed the ‘feminization of medicine’. One projection suggests that by 2027 the percentage of women enrolled in medical schools will reach 60% nationally. (Reference Graue-Wiechers, Alarcón-Fuentes, Guevara-Guzman, Ostrosky-Wegman, T, 372ME, P, E and P4)
The presence of men stands out within management positions in health institutions and medical schools. However, the last decades have seen increased participation of women as leaders, mainly in medical education and some health institutions. Within medical education, the UNAM School of Medicine is one of the most representative of this change since more than half of the managerial positions, including secretaries and heads of academic departments, are held by women. In the research division, seven women head their departments, and the positron emission tomography/computed tomography (PET/CT) services, research, and teaching unit is headed by a woman.
Regarding medical specialties, a report published in 2022 found that from 2006 to 2015, the surgical specialties that showed an increase in female students graduating were otolaryngology (55%), cardiothoracic surgery (23%), coloproctology (21%) and pediatric surgery (17%). Regarding clinical specialties, those with an increase were pediatric cardiology (52%), allergy/clinical immunology (30%), pediatric neurology (28%), genetics (25%), and pediatric endocrinology (23%). (Reference Sepúlveda-Vildósola, González, López-Sepúlveda and Martínez-Escobar5) For instance, only three of the thirteen institutes that make up the National Institutes of Health have had or now have female medical directors. However, the remaining institutes’ general directorates have never been led by a woman. (Reference Rivera-Romano, Fresno, Hernández-Lemus, Martínez-García and Vallejo6) In our country, data regarding gender violence in medical students has been reported from 15.5–69%, more towards women than men. To mention a couple of examples, it was reported to have been performed through sexist insults (F: 11.5%; M: 3.4%) and personal academic favoritism (F: 9.0%, M: 2.9%). (7)
Sexual harassment has been reported to occur more frequently in clinical cycles (73.66%) than in primary cycles (26.34%). In both, women are the most affected, and occurrence increases with the number of years of study, being significantly higher during the fourth and fifth years of the degree course. Harassment manifests as unwanted invitations to go out on a date, inappropriate jokes, leering, questions to female students about their sexual habits, unwanted sexual conversations, obscene flirtatious comments, insinuations of sexual relations, unwanted sexual attentions, or academic blackmail. Sexual abuse affects 7–28% of students; 46–54% are women and 19–39% are men. The forms of abuse include being spied on in bathrooms, being forced to undress, showing sexual organs, observing masturbation, being pressured to perform oral sex, and fondling, among others. (7)
Medical Education
In Mexico, the body in charge of evaluating and certifying the quality of medical education is the Mexican Council for the Accreditation of Medical Education, (8) which establishes the standards to evaluate the quality of education. (Reference Salud9) The figures reported by COMAEM for the second semester of 2022 are ninety-one accredited programs, eleven with expired accreditation, one without accreditation, twenty-five in self-assessment, two unfavorable opinions, and twenty-four without the accreditation process. (Reference Salud9)
The accreditation considers standards from the administrative process to the evaluation of the students and the monitoring of graduates. COMAEM’s challenge is to certify medical education because of the increase in medical schools and students in the country (133,000 students in 2018). (Reference Rillo, Martínez-Carrillo, Conteras-Mayén, Valdéz-Ramos and Castillo-Cardiel10) On the other hand, medical education in Mexico is heterogeneous; there are more than 140 public and private medical schools with different programs and characteristics. (Reference Blancas and Bárcena11) In addition, about 50% of specialty students are enrolled in postgraduate training at UNAM. Although the school environment seeks to be free of violence, a factor that can substantially increase the risk of violence is social service. The social service component is integrated into the program to ensure students gain practical experience and develop a sense of social responsibility before becoming practicing physicians. However, it is unpaid and unregulated and the government does not offer safeguards for physicians. (Reference Blancas and Bárcena11)
Resident doctors do not have labor rights since their professional activity is considered a postgraduate scholarship. These factors increase the susceptibility of physicians to unsafe and violent environments. (Reference Machado, Ramírez, Sepúlveda and Márquez12) A resident physician in Mexico is a medical professional who enters a receiving medical unit to perform a specialty characterized by academic, assistance, and research activities that must be carried out during the time stipulated in the related academic and operative programs. In addition, these must be endorsed and supervised by a university institution.
Law
The Federal Labor Law, in article 133, states that ‘Employers or their representatives are prohibited from carrying out acts of harassment and sexual harassment against any person in the workplace or allowing or tolerating such acts.’ (13)
Public hospitals and clinics received at least 118 complaints of acts of harassment and sexual and labor harassment from workers, residents and intern medical students, and beneficiaries, from December 1, 2018 to June 2019. The complaints range from acts of workplace harassment (unjustified workload, mistreatment, threats, and physical aggression) to sexual aggression (verbal and physical). Some women even report having been drugged to be later sexually abused by medical personnel. (Reference Universal14) Workplace harassment in the hospital environment occurs mainly in administrative areas; in the medical area, it is little reported. (Reference Aldave, Hernandez-Garnica and Puga-Murgia15) In a study of professional burnout in the hospital environment, psychological harassment, the medical specialty area of participants and the year of residency contributed to professional burnout by 23%, while the gender of participants and the intensity of harassment did not. (Reference Tafoya, Jaimes-Medrano, Carrasco-Rojas, Rodríguez-Machain and Ortiz-León16)
Medical Regulation
The General Law for Equality between Women and Men (2006), the General Law for Women’s Access to a Life Free of Violence (2007), and the Regulation of the General Law for Women’s Access to a Life Free of Violence, to name a few, stipulate rules on sexual harassment and gender violence in the workplace in Mexico. However, unfortunately, the applicability depends on the institution. Since so few institutions have a Gender-Based Violence Committee, there is currently little control over cases of gender-based violence in hospitals. One example is the Mexican Institute of Social Security (IMSS). In its ‘Code of Conduct and Prevention of Conflicts of Interest of Public Servants of the IMSS’, section 7.2 calls for respecting human rights, equality, and non-discrimination and enforcing measures to stop any form of violence, harassment, or sexual or labor harassment towards any person in the workplace. (17) On the other hand, during their training as medical specialists, university students can be encouraged to learn about the various forms of violence and, more importantly, reliable reporting channels. (Reference Olivares Olivares, Gómez Zapata, Flores Félix, Castañeda Prado, Turrubiates Corolla, Esperón Hernández and Valdez-García18)
Case Study
Prelude
The isolation experienced by medical students occurs from the moment they enter medical school, as educational demands prevent them from maintaining the family, social roles, and social relationships they had outside of medicine up to that point. Then they are cut off from university life. From the third year of studies, they are sent to a hospital where they take classes and begin to get involved in hospital medical care activities, especially in the morning but also in the afternoon and at night with ‘on-call’ hours. This isolation takes the form of long days of study-work inside the hospital from the fifth year of the career, called Medical Internship, and reaches its maximum during the specialty studies, called Medical Residency, where the short time outside the hospital is used to sleep and study.
The so-called ‘teaching hospitals’ have in common a hierarchical structural design characterized by the isolation of their doctors in training, who have little or no contact with the outside world. This strips them of their belongings, roles, and social positions before entering. Isolation is reinforced by impersonal treatment such as calling them by their grade of training instead of by name: the students, the MIPS (medical interns in the fifth or sixth year of their career), the interns, the R1, 2, 3 (first, second, third or subsequent resident physicians).
Doctors in training also break with the ordinary spheres of life – sleep, work, and recreation – and everything converges in the same physical space, always in the company of the same people and under a hierarchical organization that imposes rigid schedules and plans. Moreover, the work assigned to students (undergraduate and graduate) tends to be alienating, as they receive minimal payments in exchange for long and exhausting workdays laden with high professional responsibility and sometimes without the necessary inputs. The medical profession’s isolation and inflexible hierarchical order place students under a strict surveillance system designed to ensure their cooperation and obedience, through systematic harassment and the imposition of rules that endorse their subordinate role (the MIP cannot speak directly with the person on secondment but only with R1 and the latter with R2 and so on), or through the imposition of diffuse and changing rules whose purpose is to endorse the power of authority over students. Some laws violate their autonomy by forcing them to ask permission to carry out basic activities such as going to the bathroom or eating. Or through the systematic application of punishments, which include verbal aggressions such as obscene nicknames or swearing, cursing or humiliating them by highlighting their mistakes, making fun of them or talking about them as if they were not present, and forcing them to participate in activities that disqualify them, such as performing unnecessary, meaningless or menial tasks (e.g. mopping the office, buying dinner in the early morning). In turn, it is common for interns or residents also to receive ‘punishment guards’, which prolongs their confinement and isolation within the hospital.
On the other hand, a system of privileges is also included. Their obedience is rewarded with a degree of restitution for what is lost within the hospital; therefore, students adapt to the extent that they obey the rules, avoid punishment, and accept the privileges granted. The differential treatment that female medical students receive protects them from the mistreatment and abuse to which their male colleagues are subjected. This apparent protection enables male students to achieve triumphs in the competitive world of medical training, because they can’t earn the same privileges if they do not endure the same ‘punishment’.
In addition to the above, gender-based violence among medical students is also manifested by the following:
1) Gender discrimination. Physicians and residents often target female medical students based on their physical attractiveness. As a result, their teaching responsibilities are often skewed towards flirtation or condescending protection of female students, stripping them of their role as students and thus excluding them from intellectual competence within the field.
2) Sexual harassment. The intensity of harassment experienced by female medical students ranges from subtle advances to explicit sexual harassment. It is thus a known pattern within the medical profession that operates with impunity and gives rise to a culture of sexual harassment within teaching hospitals.
Assault
When Sara was a MIP, she attended to a patient with a periodontal abscess during a night shift. In her hospital, an otolaryngologist would typically handle such a procedure, so Sara called the doctor. However, while the doctor was on the way, she left the patient and a family member in front of the office and went to see another consultation because the emergency room was overfull with patients that day.
I remember the call from the otolaryngologist, who shouted at me, asking where I was, that he was not going to pass the patient by himself, that I was not his employee. I ran out, and throughout the consultation, he kept asking me and evidencing the questions he did not know in front of the patient … I felt very humiliated. At the end of the consultation, he told me not to accompany the patient, you left her here alone, she can go out alone, and I need to talk to you … at that moment, I thought he was going to scold me. However, he began to take my hand; meanwhile, he asked me, ‘What are you going to do now to make up for your mistake?’ I gave answers like ‘I’ll buy him a coffee’, which we used to do when we messed up, but he caressed my hand and face and said, ‘But come on, think about it a little more; what can you offer me?’ At that moment, I was paralyzed; he put his arms around me and pulled/brought me closer to him; when he was about to kiss me, a classmate knocked on the door, and I ran out of that office …. I don’t remember being so scared.
Following the incident, the student said that the doctor would make remarks in the corridors:
if there were people around, he would only tell me ‘Dr you owe me something’; if there were no people around, he would come close to my ear and tell me ‘how much for oral sex? have you ever made love to me in a van?’ During surgeries, he would grab me by the waist and laugh; he would say it was to see how concentrated you were, doctor. At some point, I realized that I began to dress differently; I looked for the least provocative … I guess I felt somehow guilty as if I had provoked him. I felt guilty in some way, as if I had provoked it. When I talked about it with other colleagues, each one told her experience, and we said that’s why we shouldn’t be alone, or even someone mentioned that we should see the benefit of it.
Exposure
Sara remembers commenting with her classmates that they should report the aggressors but that many of them mentioned several cases where negative consequences ensued for the students and not the aggressors. Some minimized the abuse or blamed the victims: ‘it is also your fault, you are always smiling, and they see it as an invitation, they are men, they like to compete for attention, you should feel flattered to have the attention of the handsome and successful doctor [aggressor otolaryngologist]’ (Sara recalls).
In the case of the male colleagues, they often argued errors in the interpretation on the part of the female doctors:
it is that you also exaggerate, as a man you tell them something nice, you flatter them, or you invite them to go out, and they already feel that we are harassing them, they can no longer hug anyone, besides they wanted to be in a man’s place, right? Well, they have to tolerate our jokes.
According to Sara, she once saw how they ‘punished’ an inmate who complained about verbal abuse from the doctor. ‘They had a dilator that they used to call it (the “Oh my god”), and they made the joke of raping him with this object in the doctors’ office while they told us that this happens to those who gossip; that dog does not eat dog, and that we are their pets and we owe them obedience’, she says.
You don’t feel inclined to report it in this situation since you can see how these doctors and the hospital administration are friendly. You seek assistance at the institution, but there are no avenues for complaint or accompaniment.
Aftermath
Sara says that these experiences throughout her professional training modified her way of addressing patients and the concept she had of certain health professionals.
I stopped smiling all the time, I became drier, curter, more distant, I changed the way I dressed, I tried to keep a low profile. … I remember following the advice of a friend, it worked for me to go with an angry face as if I was going to kill them all, the tone of my voice was forced to be more serious and I started to make sexist and sexual jokes in an attempt to belong, although I still don’t feel comfortable with them.
Currently, Sara belongs to a gender commission of her university to generate a change and propose ways to support the doctors to report and accompanies them during the process of avoiding revictimization.
It took me years in psychotherapy to understand that it was not my fault, to begin to team up with other doctors who had reported and that despite going through similar or stronger experiences than mine, they still keep their essence and a deep desire to make changes, some of them today in positions of power making changes in their work areas.
Discussion
The number of women in medical schools has not significantly improved their position, which can be attributed to the medical environment’s highly hierarchical and androcentric nature. (Reference Llenas-García, Masiá, Pascual Perez, González-Cuello, Agulló Re, Romero Nieto, Amat Díaz, Padilla Urrea, Rodríguez Lucena and Wikman-Jorgensen19) Gender-based violence, understood as an act of power and force exerted on women and men based on social and cultural constructs and belonging to a specific sex, persists in several areas. (Reference Çinaroğlu, Efgan and Payza20) Thus, it is a structural process sedimented in a sociocultural order that legitimizes it and provides people with the conditions and skills to exercise it. This reinforces and qualifies sexual harassment as a desirable behavior; that is, it is a means of control and not an end. Power relationships, constructed at the macro level, are expressed at the micro level in relationships and power dynamics established in the school environment between peers, teachers, and students. (Reference Chinichian, Aghabiklooei, Mehrdad, Pouryaghoub and Orouji21)
An in-depth analysis of how social systems and institutions affect interpersonal violence that disproportionately harms women must be carried out. (Reference Jenner, Djermester and Oertelt-Prigione22) In the medical profession, the symbolic structure of power is reflected through the hierarchical systems of teaching, learning and practice. These hierarchies are permeated by the androcentric characteristics of our current society. Therefore, the medical community reproduces and transmits, through the hidden curriculum, forms of perception, thought, and action that keep women and men (who do not meet the social standards of masculinity) in an undervalued space of powerlessness. (Reference Wheatley, McKeon, Pebole, Wells, Rees, Ward and Rosenbaum23) For example, sexual violence is considered a device of corporeality whose existence obeys a strategic need to control female bodies and is exercised against women for being women because their aggressors think them to lack the minimum rights of respect. (Reference Rolland, Hadouiri, Haas-Jordache, Gouy, Mathieu, Goulard, Morvan and Frajerman24) In its exercise, the socially structured male subjectivity intervenes to desire and possess women at any cost. In its activity, the socially structured male subjectivity intervenes to choose and include women at any cost. This sociological subjectivity, in turn, causes women to perceive violence less, because they conceive many of these acts as standard within their culture, that is, socially legitimized behaviors that are not considered incorrect. (Reference Berbegal-Bolsas, Gasch-Gallén, Oliván-Blázquez, Sánchez Calavera, García-Arcega and Magallón-Botaya25)
Violence in the medical environment creates human rights, public health, and academic problems due to its effects on physicians’ physical and mental health and its extensive negative consequences on the health system. (Reference Sammut, Ferrer, Gorham, Hegarty, Kuruppu, Salvo and Bradbury-Jones26) Gendered patterns of interaction during medical specialty training play a decisive role in the constitution of medical culture. Medical culture impacts specialty choices but also interferes with learning and the ability to perform as professionals. This also includes worse interactions with patients because they function as a reproduction of the same gender structures that originated it. Female medical specialists are deprived of performing procedures essential to their specialty and subsequently will probably practice that specialty with insecurity and have to make up for deficiencies during their training.
Identifying gender violence will make it possible to deduce that it is an inherent and incorporated problem in the daily work of school hospitals. This practice is rooted in the hegemonic medical knowledge and bearers of hierarchical power, without any questioning, masculinized, naturalized, and normalized in daily practice through routines, attitudes, language, and management of this knowledge, which is legitimized by the hospital institution from the very organization of the services. (Reference Sammut, Ferrer, Gorham, Hegarty, Kuruppu, Salvo and Bradbury-Jones26) Therefore, the education and training of medical specialists ritualize the difference and the gap between male and female health personnel. Biological, social, and cultural differences are not considered to improve care but rather to justify the differences and naturalize the use of power and the forms of daily violence exercised in the institution, between male and female coworkers.

 Open access
Open access