


1. Introduction
In many countries, health care services are delivered through a mix of for-profit and non-profit providers. There are various rationales for having mixed markets. In theory, mixed markets can enhance welfare compared to either full public or full private provision (Le Grand, Reference Le Grand1991; Besley and Ghatak, Reference Besley and Ghatak2007; Barr, Reference Barr2012; Chalkley and Sussex, Reference Chalkley and Sussex2018). On the one hand, the public or non-profit sector serves as a way of guaranteeing access to a certain minimum quality of care (De Fraja, Reference De Fraja2009; Barr, Reference Barr2012). On the other hand, for-profit parties have an incentive to enhance efficiency since they directly benefit from cost savings. They typically implement changes more rapidly due to their greater willingness to take risks in pursuit of potential profits. In addition, they are likely to be more creative, which increases their chances of offering innovative care options and luxury services. They may also more easily attract motivated workers, allowing them to better address labor market issues (Besley and Ghatak, Reference Besley and Ghatak2005; Comondore et al., Reference Comondore, Devereaux, Zhou, Stone, Busse, Ravindran, Burns, Haines, Stringer, Cook, Walter, Sullivan, Berwanger, Bhandari, Banglawala, Lavis, Petrisor, Schünemann, Walsh, Bhatnagar and Guyatt2009; Chalkley and Sussex, Reference Chalkley and Sussex2018).
However, this welfare gain depends on the extent to which distortions exist. The theoretical literature on mixed markets discusses distortions created by government or non-profit care provision on market outcomes, such as crowding out (De Fraja, Reference De Fraja2009). A possible distortion caused by for-profit provision in the care sector is risk selection. For-profit entities might reduce costs by choosing clients based on their health status, commonly referred to as cherry picking (attract relatively healthy, and therefore cheaper individuals) or lemon dropping (redirect relatively unhealthy individuals to other providers) (Akerlof, Reference Akerlof1971; Newhouse, Reference Newhouse1996). Other possible distortions are upcoding (assigning patients to higher-level care codes to increase reimbursement rates) or delivering lower quality of care (Silverman and Skinner, Reference Silverman and Skinner2004; Steinbush et al., Reference Steinbusch, Oostenbrink, Zuurbier and Schaepkens2007).
In institutional long-term care (LTC), mixed markets typically involve a combination of non-profit and for-profit nursing homes. Our study explores potential distortions in the Dutch institutional LTC mixed market for dementia. While all Dutch residential nursing homes are non-profit, for-profit organisations, have increasingly entered the market, offering round-the-clock care provided in (clustered) home-like settings as an alternative to non-profit residential care.
Recent empirical literature reveals distortions in mixed institutional LTC markets worldwide, but the empirical evidence is mixed. For example, Gandhi (Reference Gandhi2023) identified evidence of risk selection in California nursing homes, which disproportionately disadvantaged Medicare patients during periods of bed scarcity. However, no significant differences were observed between non-profit and for-profit nursing homes. Bach-Mortensen et al. (Reference Bach-Mortensen, Goodair and Esposti2024) showed that, since 2011, for-profit nursing homes in England provided on average lower levels of care quality compared to public ones. Distortions can be especially problematic in LTC markets because of some unique characteristics. Individuals in nursing homes are generally not mobile and often unable or unwilling to move to another facility (Mukamel, Reference Mukamel, Ladd, Weimer, Spector and Zinn2009). Therefore, voting with your feet is not easy, and the incentives for risk selection or the provision of lower-quality care are difficult for clients to address or correct.
A potential reinforcing factor is that some for-profit nursing homes, often part of large nursing home chains, are owned by private equity (PE) companies. Those PE partners have entered the LTC markets of Organisation for Economic Co-operation and Development (OECD) countries during the last twenty years (Mattingly, Reference Mattingly2023). The rationale for this trend is that PE-owned organisations may implement more optimised business strategies than other for-profit nursing homes. These strategies can include adjustments in services offered, governance, diversification, separating property from operations, or expanding locations, all aimed at maximising profits (Pradhan et al., Reference Pradhan, Weech-Maldonado, Harman, Laberge and Hyer2013; Bos and Harrington, Reference Bos and Harrington2017; Harrington et al., Reference Harrington, Jacobsen, Panos, Pollock, Sutaria and Szebehely2017). PE companies are typically characterised by a stronger focus on short-term profitability and may plan to divest their assets after a certain period. Additionally, they are often responsible for the debt incurred through acquisitions financed with borrowed money to acquire these facilities. Dewatripont and Tirole (Reference Dewatripont and Tirole2024) showed that if the degree of greed among private parties (e.g., PE-owned companies) is high, problems are more likely to arise. The stronger the drive for profit, the higher the likelihood that all available legal loopholes will be exploited, especially in the absence of intrinsic motivation to restrain such practices (Stevenson and Grabowski, Reference Stevenson and Grabowski2008; Eghbali, Reference Eghbali2023; Dewatripoint and Tirole, Reference Dewatripont and Tirole2024). They also showed that mixed markets can work well under the right circumstances since the benefits of competition might outweigh the potential negative effects. Most of the available empirical research in LTC focusses on the role of PE-owned nursing homes on care quality (Lainoff, Reference Lainoff2020). Some studies show no significant differences in quality performance between PE-owned nursing homes and other nursing homes (Winblad et al., Reference Winblad, Blomqvist and Karlsson2017; Braun et al., Reference Braun, Yun, Casalino, Myslinski, Kuwonza, Jung and Unruh2020; Hussem et al., Reference Hussem, Tenand and Bakx2020; Kruse et al., Reference Kruse, Ligtenberg, Oerlemans, Groenewoud and Jeurissen2020). However, the profit motive of PE providers by cutting costs to increase revenues may also harm the quality of care (Pradhan et al., Reference Pradhan, Weech-Maldonado, Harman, Al-Amin and Hyer2014; Bos et al., Reference Bos, Kruse and Jeurissen2020; Hussem et al., Reference Hussem, Tenand and Bakx2020; Kruse et al., Reference Kruse, Ligtenberg, Oerlemans, Groenewoud and Jeurissen2020, Patwardhan et al., Reference Patwardhan, Sutton and Morciano2022). For instance, Gupta et al., (Reference Gupta, Howell, Yannelis and Gupta2021) examined the impact of PE buyouts in U.S. nursing homes on short-term mortality. Their findings revealed that frail (Medicare) individuals admitted to a PE-owned nursing home faced an elevated risk of short-term mortality. Braun et al., (Reference Braun, Jung, Casalino, Myslinski and Unruh2021) explicitly examined quality differences between PE-owned nursing homes and other for-profit nursing homes in the U.S. during Covid-19 pandemic, finding that PE-owned facilities had higher rates of emergency department visits, hospitalisations, and Medicare spending.
The Dutch institutional LTC market has some distinguishing features, which are i) access to this type of care needs to be approved by a government-run gatekeeping system (Bakx et al., Reference Bakx, Schut and Wouterse2021); ii) for those who qualify, the system is typically generous and the care is of relatively high quality (Bakx et al., Reference Bakx, Schut and Wouterse2021); iii) for-profit and not-for-profit organisations make use of the same public funding; iv) for-profit, including PE-owned organisations, are on the rise (Bos et al., Reference Bos, Kruse and Jeurissen2020), but the market shares are small relative to, e.g., the U.K. and U.S. As shown in the theoretical and international empirical literature, the introduction of for-profit (PE-owned) entities in the Dutch LTC system may entail some risks for market distortions. Our findings provide no strong evidence of such distortions and, therefore, no indication that for-profit organisations (including PE-owned ones) exhibit the same level of adversarial behaviour as observed in other parts of the world.
Our research focusses on individuals with dementia. First, the prevalence of dementia is steadily increasing worldwide due to aging populations, posing significant challenges for LTC systems (WHO, 2019). Second, individuals with dementia have unique and complex needs that go beyond standard medical care, including support with daily activities, behavioural management, and the provision of a safe and stimulating environment. As cognitive decline progresses, these individuals often require specialised, person-centred care that addresses both their physical and emotional well-being (Lee et al., Reference Lee, Lee and Kim2022). It is therefore paramount to better understand whether and how this growing demand for tailored LTC services can be effectively addressed by a more diverse range of care arrangements. Third, many PE-owned nursing homes focus on dementia care. One reason for this is that it may be easier to reduce care costs of patients with mild dementia without severe physical impairments, compared to individuals with significant physical disabilities who may require more intensive and specialised care. Moreover, concentrating on a specific type of disability allows for more streamlining of care processes and optimisation of resources, possibly leading to increased cost-efficiency and higher profitability.
1.1. The Dutch long-term dementia care market
In 2015, the Netherlands ranked as the highest spender on LTC among OECD countries while having an average percentage of older individuals (OECD, 2023). The increasing costs and the lack of incentives for efficiency raised concerns about the financial sustainability of the system (Schut and van den Berg, Reference Schut and Van den Berg2010). As a result, the Dutch LTC system was extensively reformed, and the Long-Term Care Act (LTCa) came into force in January 2015. The LTCa covers intensive forms of care for vulnerable people or people with severe mental or physical disabilities who need round-the-clock care. It does not include less intensive care alternatives such as formal home care provided through district nursing. The focus of our study is on LTCa care. Figure 1 shows the various steps that an individual with severe dementia might follow within the Dutch institutional LTC system.
Potential care pathway for a dementia patient in the Dutch institutional LTC system.

Access to LTCa care is granted or rejected by the Care Needs Assessment Center (CNAC), based on detailed, nationwide, objective criteria. Entitlements for (dementia) LTCa care are expressed using care need packages where, overall, lower numbers stand for lower intensity of care and higher numbers for more intensive forms of care. Actual use of LTCa care is restricted to individuals who have been granted it, and they can only utilise the care outlined in the granted care needs package (Maarse and Jeurissen, Reference Maarse and Jeurissen2016).
Individuals with an LTCa entitlement can choose between residential care (care in non-profit nursing homes) or continuing living independently (i.e., in their own or rented accommodation) and getting all the support and care they need there. LTCa care in own accommodation or in home-like settings can be provided in three ways.Footnote 1 First, clients can opt for a ‘Full home care package’, which is typically provided in a clustered form in a home-like environment such as an apartment or on an estate. Care is then provided by one single provider. Second, clients can opt for a ‘Modular home care package’, but in this case, care is provided by multiple providers most often in the client’s own accommodation. Those care packages offer the same care individuals would receive if they were living in a residential nursing home. Most importantly, it includes nursing care and treatment and non-medical services like personal care, provision of food and drinks, transportation, cleaning of living space, and sometimes respite care. The care costs are covered by the LTCa (except for own contributions) but, unlike in residential nursing homes, the individual remains responsible for his or her own housing costs. Individuals can only opt for home care packages (instead of residential nursing home care) when care offices expect that living independently is still feasible and the required care can be provided in an efficient (clustered) way (Plaisier and Den Draak, Reference Plaisier and Den Draak2019; Bakx et al., Reference Bakx, Wouterse, Van Doorslaer and Wong2020). Third, clients can opt for a ‘Personal Budget’ with which he or she can make his or her own care arrangements.
Monthly out-of-pocket payments are required for each delivery method. The amounts individuals must pay depend on their financial resources (income and wealth), age, partner status, and type of received care. In the case of residential care in nursing homes, the monthly co-payment ranges between 0 to 2,887 euros. For those choosing to receive care in their own or rented accommodation, the monthly co-payment is significantly lower, ranging from 29 to 880 euros. Particularly for wealthier older individuals, a ‘Full Home Care Package’ may be more appealing due to their comparatively lower monthly co-payment (Tenand et al., Reference Tenand, Bakx and Wouterse2021).
The 2015 reform also created financial opportunities for for-profit providers, gradually transforming the Dutch institutional LTC sector into a mixed market.Footnote 2 Until 2015, the role of for-profit nursing homes in the Netherlands was minimal. This was largely due to the prevailing belief that the Dutch government was responsible for those in need of LTC, leading to public LTC insurance with extensive coverage since 1968 (Maarse and Jeurissen, Reference Maarse and Jeurissen2016). The number of for-profit nursing homes increased from about 120 locations in 2014 to 291 in 2018 and to 550 in 2023. This number remains modest compared to the 2,355 non-profit residential nursing home locations in 2023, which provide accommodations to approximately 122,000 individuals (Bos et al., Reference Bos, Kruse and Jeurissen2020; Zorgkaart Nederland, 2024; Actiz, 2024). In recent years, an increasing number of PE-owned companies have shown interest in the healthcare sector, leading to acquisitions of small healthcare providers. Currently, five large PE investors are active in the LTC sector.Footnote 3 These investors collectively own 253 for-profit nursing home locations distributed across 10 labels, encompassing approximately 6,000 rooms (Bos et al., Reference Bos, Kruse and Jeurissen2020). As shown in Figure 1, while residential care is only provided by non-profit organisations, round-the-clock care at home or in homelike settings is offered by non-profit and for-profit (PE-owned) organisations.
In the last decade, individuals entitled to LTCa care have faced increasing waiting times before receiving the care needed due to supply shortages (Actiz, 2024). Therefore, investments from PE-owned or other for-profit organisations might alleviate the escalating demand for residential care and offer more care options, such as the opportunity to live in more upscale apartments in care complexes and receiving round-the-clock care there. Care complexes may operate more efficiently when all clients reside together.
1.2. Potential distortions in the Dutch institutional LTC mixed market
The organisation and commercialisation of the Dutch institutional LTC system also entail some risks. First, profit payments to shareholders are prohibited by law (under the Care Institutions Admission Act). Given the increasing (unmet) demand for institutional care, growing preferences for ageing at home (Tenand et al., Reference Tenand, Bakx and Wouterse2021) and the relatively generous public coverage, offering LTCa care have become more financially attractive and for-profit organisations have found ways to circumvent the profit ban using home care packages provided in (clustered) home-like settings. The profit ban holds for the care component, but not for the housing component. Therefore, for-profit organisations rent apartments to individuals who have been granted LTCa care and offer them those packages. The living-related components such as rent, property, service costs, and catering are paid for by the clients themselves, and the providers may make profit on the housing component (Ministerie van Volksgezondheid Welzijn en Sport, 2022). In principle, profits are generated from (high) living expenses and service costs, but there is some evidence suggesting that profit is also being derived from the care component (Bos et al., Reference Bos, Kruse and Jeurissen2020).
Second, for-profit and non-profit facilities are both eligible for public LTCa funding. They are paid through the same reimbursement system and receive a government-regulated maximum daily rate for each care package provided.Footnote 4 The price of a care package also depends on where the care is provided, whether in a residential nursing home or in (clustered) home-like settings (e.g., full home care packages) (Bakx et al., Reference Bakx, Wouterse, Van Doorslaer and Wong2020). The reimbursement of a care package is based on a case payment model. The provider receives a fixed price based on average cost of care, which are independent from the actual delivered care. Therefore, some cost variations are possible within each care package which creates opportunities for risk selection and potential upcoding. The risk selection part comes from the incentive of for-profit players to target individuals within a care package with predictable lower costs. For-profit organisations also have an incentive for transferring patients to a residential nursing home as client’s (physical) health deteriorates over time and more extensive care is needed. Sometimes, this is already mentioned in the housing/care contract. This may also be accompanied by a change of entitlement based on the CNAC assessment, which may precede or follow the move. Although the nursing homes cannot influence the result of the CNAC assessment, they can decide when it is initiated. This leads to a potentially complex interplay between ‘upgrading’ an entitlement and moving. On the one hand, there is a financial incentive to upgrade the entitlement, and keep the client in the nursing home without providing adequately extensive care. On the other hand, as time elapses, this could lead to significantly degraded quality.
2. Methods
2.1 Datasets and study sample
We used two administrative individual-level datasets from Vektis, a business intelligence company for the Dutch healthcare sector that collects all health insurance claims data. The first dataset consists of all claims data for LTC from 2017–2021. Individual health information was derived from a dataset on secondary care use from 2016–2021. Selecting these years enabled us to use the most recent available data at the time of this study and to monitor the expansion of PE providers which started in 2017–2018. We merged the two datasets at the individual level using unique identifiers.
First, we selected all claims related to two specific care packages. These packages are for individuals who need protected living with intensive dementia care.Footnote 5 The first package is for individuals receiving care in a residential nursing home and the second one is for individuals with a full home care package.Footnote 6 All claims for modular home care packages were excluded as this type of care is mostly provided while waiting for the most preferred care option. We also excluded personal budget claims as no full care information was available for them. Second, individuals typically have more than one claim per care package. Multiple claims together describe the entire care use of the client over the observation window. To identify individuals who began their institutional LTC trajectory in 2017 or later, we excluded those who had a claim in 2016. Follow-up duration varied by start year: individuals with a first invoice in 2017 were followed for up to five years, those starting in 2018 for up to four years, and so on, with a one-year follow-up for individuals who initiated care in 2021. Finally, we only included individuals who were 70 years and older at the time of their first claim. The final study sample included 105,444 unique individuals.
The Vektis dataset also includes information on the unique identification codes of nursing homes, which are typically used for processing claims with health insurers. These codes allow us to link claims to the corresponding nursing homes. While the dataset does not contain ownership information, it does include a unique registration number from the Chamber of Commerce. To determine for each calendar year whether the facilities were for-profit or non-profit we use a two-step process. First, we checked the legal form of the organisation using the Chamber of Commerce website (kvk-number). Nursing homes that had a ‘foundation’ as a legal form were classified as non-profit institutions. Nursing homes with other legal forms, such as ‘private limited company’ were classified as for-profit institutions. Second, we compared the derived classification with the classification listed on the website ‘ZorgkaartNederland.’ This site divides nursing homes into private residential care centres (for-profit nursing homes) and non-profit nursing homes. In case of discrepancies between the two websites, we searched the website of the respective nursing homes. For-profit nursing homes that were owned by one of the five PE companies were classified as PE-owned facilities.
Individual health information was also derived from the Vektis data. For this, we used data on secondary care use from 2016 to 2021. We explain below how the health variables were constructed.
Finally, because the Vektis data does not include information on individual’s socio-economic status (SES), we used public data from Statistics Netherlands (CBS) at the postal code level as a proxy (Statistics Netherlands, 2024a). Data from the last postal code registered before admission were used in our analyses. More details on these variables are also provided below.
2.2 Analyses risk selection: Cherry picking
Outcome variable: To examine the extent of cherry picking, a categorical variable with four levels was constructed. This variable was based on the ownership of the care provider and on the type of care the individual received: (1) non-profit nursing homes providing residential care, (2) non-profit nursing homes providing round-the-clock care in the own home or home-like settings (i.e. full home care packages)Footnote 7 (3) PE-owned organisations providing full home care packages and (4) other for-profit entities providing full home care packages.
Main independent variables: Two variables were included to assess the extent of cherry picking. The first variable measures the level of comorbidity before admission. We calculated the Charlson comorbidity index for each individual. This index was constructed by identifying the presence of a diagnosis 365 days before admission (i.e., the first LTCa claim). The presence of a diagnosis was based on a selection of ICD-10 diagnoses using the definition of Bär et al. (Reference Bär, Bakx, Wouterse and Van Doorslaer2022). The second variable indicates whether the individual visited a hospital during the three months preceding admission (dummy = 1) or not (dummy = 0). No distinction was made between outpatient and inpatient visits.
Other independent variables: Besides age and gender, seven additional variables were used to characterise the client’s neighbourhood (based on the postal code of residence of the individual before admission). We selected: 1) the share of inhabitants with Dutch background (%) which is defined by the percentage of individuals born to parents, both of whom are natives of the Netherlands; 2) the percentage of owner-occupied homes defined as: number of houses owned by the (future) occupant(s) or used as a second residence divided by the total number of residences; 3) value homes defined as the average provisional value of all homes with a known property tax assessment; 4) the percentage of residents who receive unemployment benefits, social assistance or related benefits, as well as disability benefits; 5 & 6) the number of households belonging to the 40% lowest and 20% highest income group measured at national level and 7) the degree of urbanisation of the municipality of residence, determined by the number of addresses per km2 (from 1-very strongly urban to 5-rural). More details on these variables can be found in Statistics Netherlands (Statistics Netherlands, 2024b). The eighth variable ‘excess capacity’ indicates the difference between the maximum number of beds per institution and the number of filled beds 3 months before admission within a radius of 20 km, as measured from the previous postal code of the individual. This variable was included to some extent control for the likelihood of risk selection: the more excess capacity in the area is, the less likely firms are to select lower risks as they aim to fill all available beds. Our model was also corrected for the size of the nursing home provider: the variable takes the value ‘0’ for nursing home providers with more than 20 clients and ‘1’ otherwise. Finally, a set of four year dummies were included to control for potential contextual changes during the follow-up of our study. Those dummies also partially account for the Covid-19 pandemic.
Statistical analyses: Multinomial logit models were estimated to assess the probability of using a specific type of round-the-clock care (our categorical outcome variable). In the first set of analysis (Model I), we used the full sample and selected non-profit nursing homes providing residential care as the reference category, with parameters estimated for the other three categories.
Remind that, in the Dutch context, we cannot compare for-profit and non-profit residential nursing homes as all of them are non-profit. To better understand the differences in incentives between for-profit and non-profit firms, all analyses were also performed on a sample excluding all individuals receiving residential care (Model II). In those analyses, we used the non-profit nursing homes providing full home care packages as a reference category. A significance level of 5% was used in all statistical analyses.
2.3 Analyses care trajectories: lemon dropping and upgrading care entitlement
Outcome variables: Two variables were used to examine differences in care trajectories across care providers. We used times to (1) transfer from one LTC facility to anotherFootnote 8 and (2) change of care needs entitlement. These variables measure the time between getting the first invoice in a specific facility and the moment that an individual is observed to move to another LTC facility and the change of entitlement, respectively.
Main determinant: Dummies indicating the type of nursing home care were included in the models. In the analyses based on the full sample, we used non-profit residential nursing homes as the reference category (Model I), and in the analyses excluding individuals receiving care in residential nursing homes, we used non-profit nursing homes providing full home care packages as the reference category (Model II).
Control variables: We used the variables mentioned in 3.2 to control for potential population differences, supplemented by the number of hospital admissions with overnight stay during our follow-up. This may be an indication that the client’s health was deteriorating, which might have triggered a forced move.
Statistical analyses: Cox Proportional hazards models were used. Proportional hazards are an underlying assumption of the Cox model. However, the effect of the baseline control variables can change with time. For example, the effect of a previous hospitalisation may be very different on the day of admission and a year later. For this reason, we tested the proportional hazards assumption, and it failed in several baseline variables. Therefore, we included time-dependent coefficients when indicated by the proportional hazards test (Zhang et al., Reference Zhang, Reinikainen, Adeleke, Pieterse and Groothuis-Oudshoorn2018; Nahhas, 2023).Footnote 9 We also accounted for clustering of individuals within organisations. Hazard ratios, coefficients, standard errors and p-values were reported.
2.4 Analyses quality of care: mortality and avoidable hospitalisations
Outcome variables: We used two dependent variables to assess the relationship between types of nursing home care and quality of care. The first one is (1) mortality. This variable measured the duration between the first invoice in a specific facility and the moment that an individual dies. The second is (2) avoidable hospitalisations which was measured as the duration between the first invoice in a specific facility and all observed avoidable hospitalisations. We followed Bär et al. (Reference Bär, Bakx, Wouterse and Van Doorslaer2022) to define avoidable hospitalisations, except that we used claims diagnosis and ICD-10 instead of ICD-9. Bär et al. (Reference Bär, Bakx, Wouterse and Van Doorslaer2022) include rehabilitation as avoidable hospitalisations, and we included this from the LTC database using all claim codes for rehabilitation.Footnote 10
Main determinant and Control variables: We included dummies to indicate the type of care the individuals received and all variables mentioned in 3.3.
Statistical analyses: For the analyses of mortality, the same types of Cox models were used as for lemon-dropping. For avoidable hospitalisations, which can happen multiple times, the Andersen-Gill model was used (Andersen and Gill, Reference Andersen and Gill1982).
3. Results
3.1. Descriptives study sample
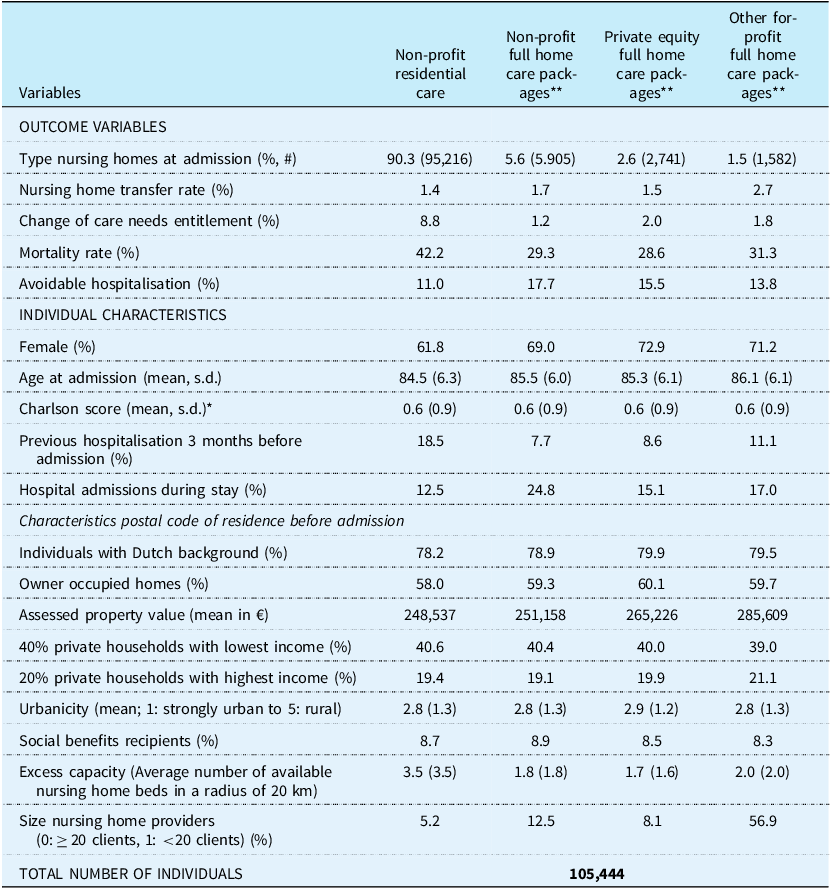
Table 1 reports the descriptive statistics of the study sample per type of nursing home care. The first part of Table 1 shows summary statistics of the outcome variables. Appendix A reports the Kaplan-Meier curves of the four duration variables, per type of nursing home care provided.
Descriptives study sample per type of round-the-clock care at admission

Table 1 Long description
The table compares various types of round-the-clock care at admission, focusing on outcome variables and individual characteristics. It has 20 rows and 5 columns. The columns are labeled as Non-profit residential care, Non-profit full home care packages, Private equity full home care packages, and Other for-profit full home care packages. The rows are grouped into outcome variables and individual characteristics. Outcome variables include type nursing homes at admission, nursing home transfer rate, change of care needs entitlement, mortality rate, and avoidable hospitalisation. Individual characteristics include female, age at admission, Charlson score, previous hospitalisation 3 months before admission, hospital admissions during stay, individuals with Dutch background, owner-occupied homes, assessed property value, 40 percent private households with lowest income, 20 percent private households with highest income, urbanicity, social benefits recipients, excess capacity, and size nursing home providers. Each cell contains specific percentages, mean values, or other relevant data points.
* Defined as Bär et al. (30), except based on claims diagnosis and ICD-10 instead of ICD-9. ** Round-the-clock care provided in home-like settings as an alternative to traditional residential care.
First, the vast majority of individuals received care in a residential nursing home. Second, few individuals were observed to be transferred to another facility or to get a new entitlement. The nursing home transfer rate did not vary a lot between the different ownership-care settings except for other for-profit full home care packages. In this setting the transfer rate was 2.7% and twice as high as in other settings. Furthermore, the descriptives show that both the avoidable hospitalisation rates varied more between types of care setting (residential or full home care package) than between ownership categories. The Kaplan-Meier curves in Appendix A show that the durations until obtaining a new care entitlement and the time to a first avoidable hospitalisation were shorter for those receiving a full home care package.
Table 1 also shows that for the characteristics measured at the level of the individual (female, age at admission, Charlson score, previous hospitalisation and hospitalisations during stay), the variation was mainly determined by where the care was provided (residential or in home-like settings). The percentage of females ranged from 61.8% in residential to 72.9% in PE-owned settings. Relatively more females received full home care packages comparing to residential care. The average age varied from 84.5 in residential care to 86.1 to for-profit home-like settings indicating that on average clients receiving round-the-clock care at home were slightly older. The mean Charlson score was comparable across all settings (0.6). The percentage of previous hospitalisations was much higher in residential settings (18.5%) compared to in home setting (ranging from 7.7% for non-profit full home care to 11.1% for other for-profit full home care). The number of hospitalisations during stay was much larger in home-like settings than in residential care.
The descriptives of the postal codes of residence before admission showed that the percentage of inhabitants with Dutch background was a bit higher for clients subsequently admitted to for-profit (PE-owned) settings. For-profit nursing homes also had more residents coming from postal codes with a higher home-ownership rate and fewer residents who received benefits. The percentage of inhabitants receiving social benefits was comparable for clients admitted to for PE-owned and other for-profit nursing homes. The percentage ‘high income private households’ was slightly higher in other for-profit organisations than PE-owned nursing homes. This may be possibly explained by one large PE provider targeting individuals receiving only a basic state pension or a small pension.
Finally, the variable ‘excess capacity’ (namely the average number of free beds per nursing home location within a radius of 20 km) was higher for residential care (3.5) compared to home-like settings (ranging from 1.7 for PE to 2.0 for other for-profit organisations).
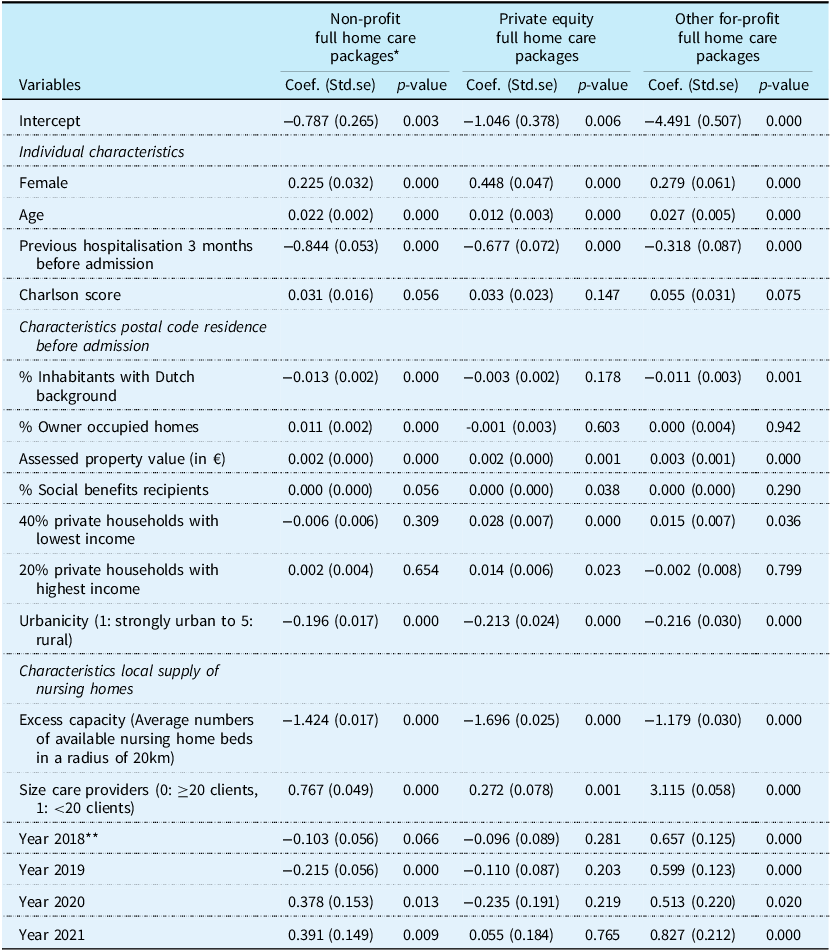
3.2 Results risk selection: cherry picking
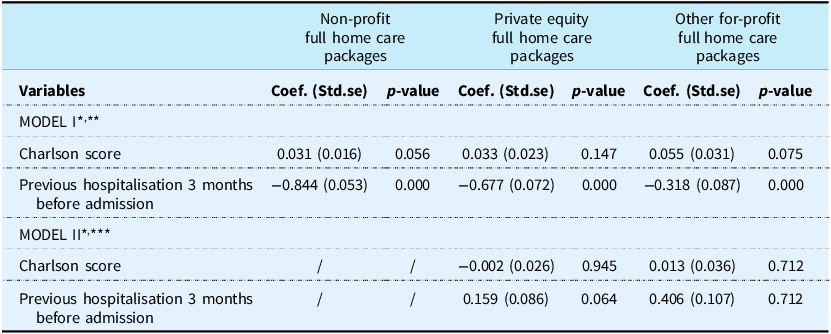
Table 2 shows the estimation results of the multinominal logit models exploring the extent of cherry picking.Footnote 11 In model I, estimated on the full sample, the variable ‘previous hospitalisation’ had significant negative coefficients for all types of home-like settings, indicating that individuals with higher levels of frailty were more likely to end up in residential care than others. Note also that the coefficients were less negative for the for-profit full home care-organisations than for the non-profit ones. Furthermore, the coefficient of the Charlson score was slightly higher for the home-like settings than in residential settings, but not significant at the 5%-level (p–values ≥ 0.056). Therefore, the selection of healthier clients seemed to be more related to the financing structure (i.e., the full home care packages versus residential care) and not to the type of ownership, as no strong differences in coefficients were observed between the organisations providing full home care packages. To further test this, we run analyses based on a sample only including individuals receiving full home care packages (Model II, reference category ‘non-profit full home care packages’). Those analyses confirmed the absence of significant differences between the for-profit and non-profit organisations providing round-the-clock care in home-like settings. On the contrary, individuals who had been hospitalised three months before admission were slightly more likely to be in PE-owned nursing homes, though the coefficient was only significant at a 10% significance level (p-value = 0.064).
Estimation results multinomial logit model risk selection (excerpt)

Table 2 Long description
The table presents estimation results of multinomial logit models exploring the extent of cherry picking in different home care settings. It has two models, Model I and Model II, each with three columns for different types of home care packages: Non-profit full home care packages, Private equity full home care packages, and Other for-profit full home care packages. Each column includes coefficients, standard errors, and p-values for the variables Charlson score and Previous hospitalisation 3 months before admission. Model I is estimated on the full sample, while Model II is based on a sample including only individuals receiving full home care packages. Row 1: Model I. Row 2: Charlson score, Coef. (Std.se), p-value, 0.031 (0.016), 0.056, 0.033 (0.023), 0.147, 0.055 (0.031), 0.075. Row 3: Previous hospitalisation 3 months before admission, Coef. (Std.se), p-value, -0.844 (0.053), 0.000, -0.677 (0.072), 0.000, -0.318 (0.087), 0.000. Row 4: Model II. Row 5: Charlson score, Coef. (Std.se), p-value, /, /, -0.002 (0.026), 0.945, 0.013 (0.036), 0.712. Row 6: Previous hospitalisation 3 months before admission, Coef. (Std.se), p-value, /, /, 0.159 (0.086), 0.064, 0.406 (0.107), 0.712.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds), the
size of the nursing home provider and four year dummies. Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
*** Reference category: non-profit full home care package.
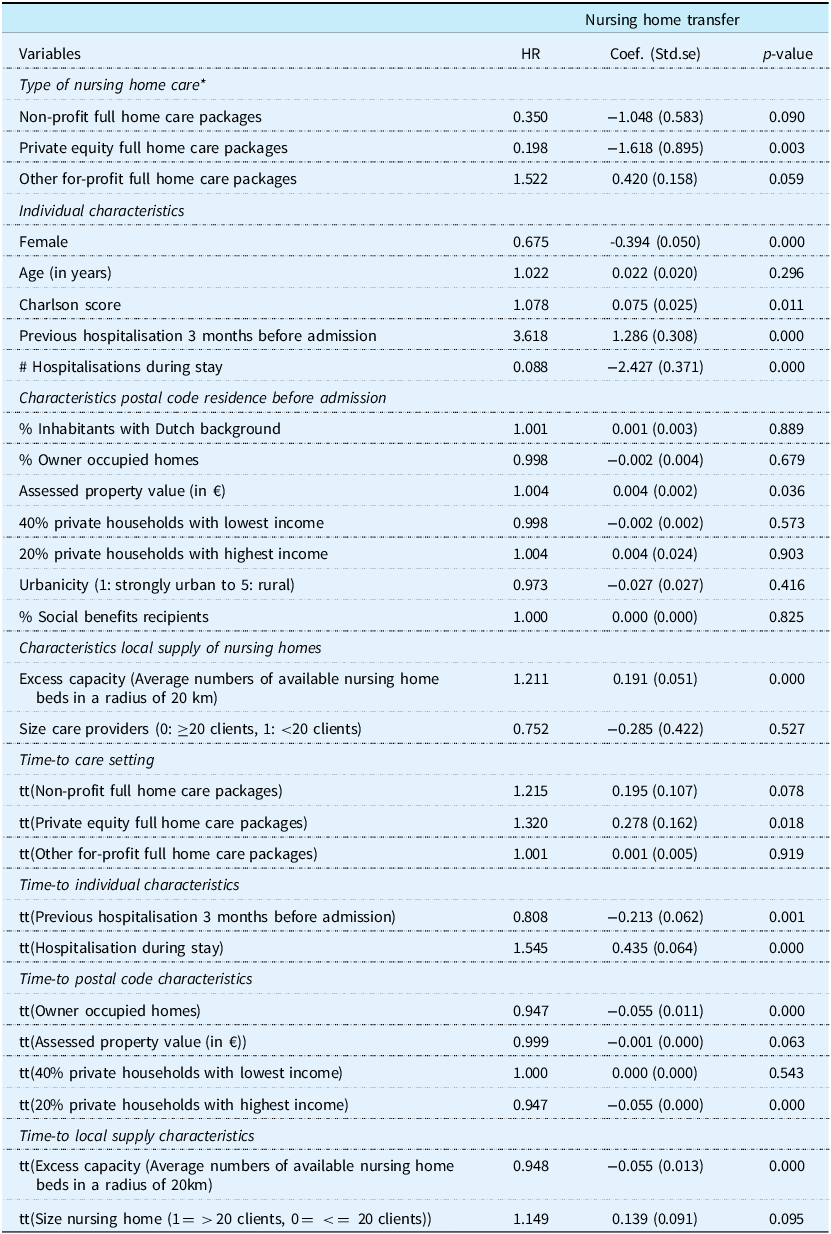
3.3 Results care trajectory: nursing home transfer and change of care entitlement
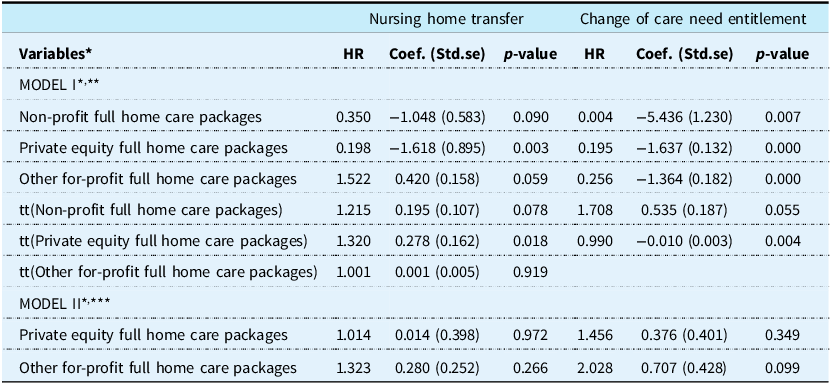
Table 3 shows the estimation results of a Cox model with time-varying coefficients assessing the relationship between the type of nursing home care at admission and the duration to a transfer to another nursing home setting and to a new care need entitlement.
Estimation results time-varying cox models changes in care trajectories (excerpt)

Table 3 Long description
A table with two main models comparing nursing home transfer and change of care need entitlement for different home care packages. The table has 12 rows and 10 columns. Column headers are Variables, HR, Coef. (Std.se), and p-value for both Nursing home transfer and Change of care need entitlement. Row labels include different types of home care packages and their time trends. Row 1: Non-profit full home care packages, HR 0.350, Coef. -1.048 (0.583), p-value 0.090, HR 0.004, Coef. -5.436 (1.230), p-value 0.007. Row 2: Private equity full home care packages, HR 0.198, Coef. -1.618 (0.895), p-value 0.003, HR 0.195, Coef. -1.637 (0.132), p-value 0.000. Row 3: Other for-profit full home care packages, HR 1.522, Coef. 0.420 (0.158), p-value 0.059, HR 0.256, Coef. -1.364 (0.182), p-value 0.000. Row 4: tt(Non-profit full home care packages), HR 1.215, Coef. 0.195 (0.107), p-value 0.078, HR 1.708, Coef. 0.535 (0.187), p-value 0.055. Row 5: tt(Private equity full home care packages), HR 1.320, Coef. 0.278 (0.162), p-value 0.018, HR 0.990, Coef. -0.010 (0.003), p-value 0.004. Row 6: tt(Other for-profit full home care packages), HR 1.001, Coef. 0.001 (0.005), p-value 0.919. Row 7: Private equity full home care packages, HR 1.014, Coef. 0.014 (0.398), p-value 0.972, HR 1.456, Coef. 0.376 (0.401), p-value 0.349. Row 8: Other for-profit full home care packages, HR 1.323, Coef. 0.280 (0.252), p-value 0.266, HR 2.028, Coef. 0.707 (0.428), p-value 0.099.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds),
the size of the nursing home provider, the observed total number of hospital admissions and four year dummies.
Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
*** Reference category: non-profit full home care package.
The estimation results on the full sample (Model I) show that, after correction for differences in health status at admission and during follow-up, the coefficients of the time-constant and time-varying components of non-profit and (PE-owned) home-like settings were borderline significant (at 10% level), implying that the relationship between those variables and nursing home transfers varied over time. Contrarily, the coefficient of other for-profit entities remained constant over time and was positive, suggesting that their clients were more likely to be transferred than those in residential homes. The coefficients of both the non-profit and the PE-owned organisations remained negative during the whole observation period (though slightly increasing). This translates in lower probability of being transferred in those organisations than in residential settings. Model II shows the results of the same analysis on a sample only including full home care package clients. None of the coefficients were significant, demonstrating the absence of difference in transfers between the three types of firms providing round-the-clock care in home-like settings.
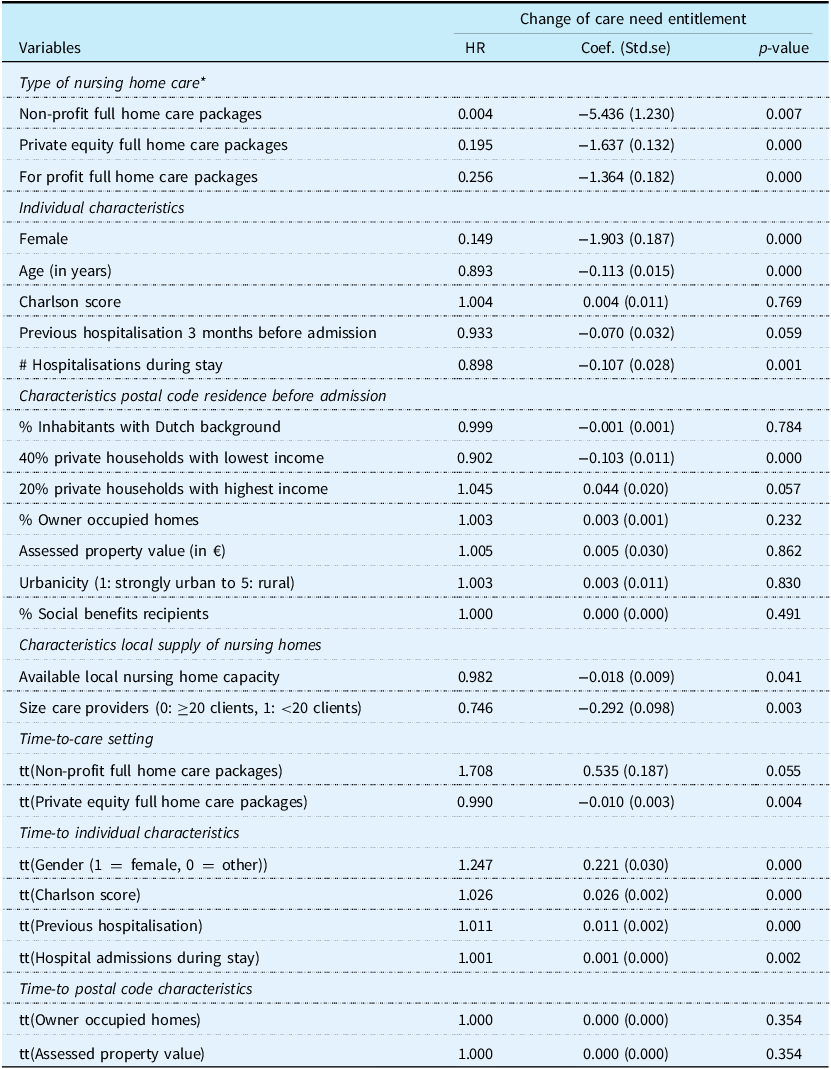
Table 3 also shows the estimation results of Cox models assessing the relationship between the type of nursing home care at admission and the duration to a change of care needs entitlement. For model I, after correction for differences in health status at admission and during follow-up, the time-constant coefficients of all (clustered) full home care settings entities were negative and strongly significant. Even after taking into account the significant time-varying coefficients, the association remained negative during the full observation period. This suggests that the probability of changing entitlement by (clustered) full home care firms was lower than in residential nursing homes. The estimation results of Model II demonstrated no strong differences in upgrading between non-profit and for-profit firms (coef. >0 & p–values ≥ 0.099) providing round-the-lock dementia care in home-like settings. This also agreed with findings based on Kaplan-Meier curves ‘Transfer to another organisation’ and ‘Change of care need assessment’ in Appendix A.
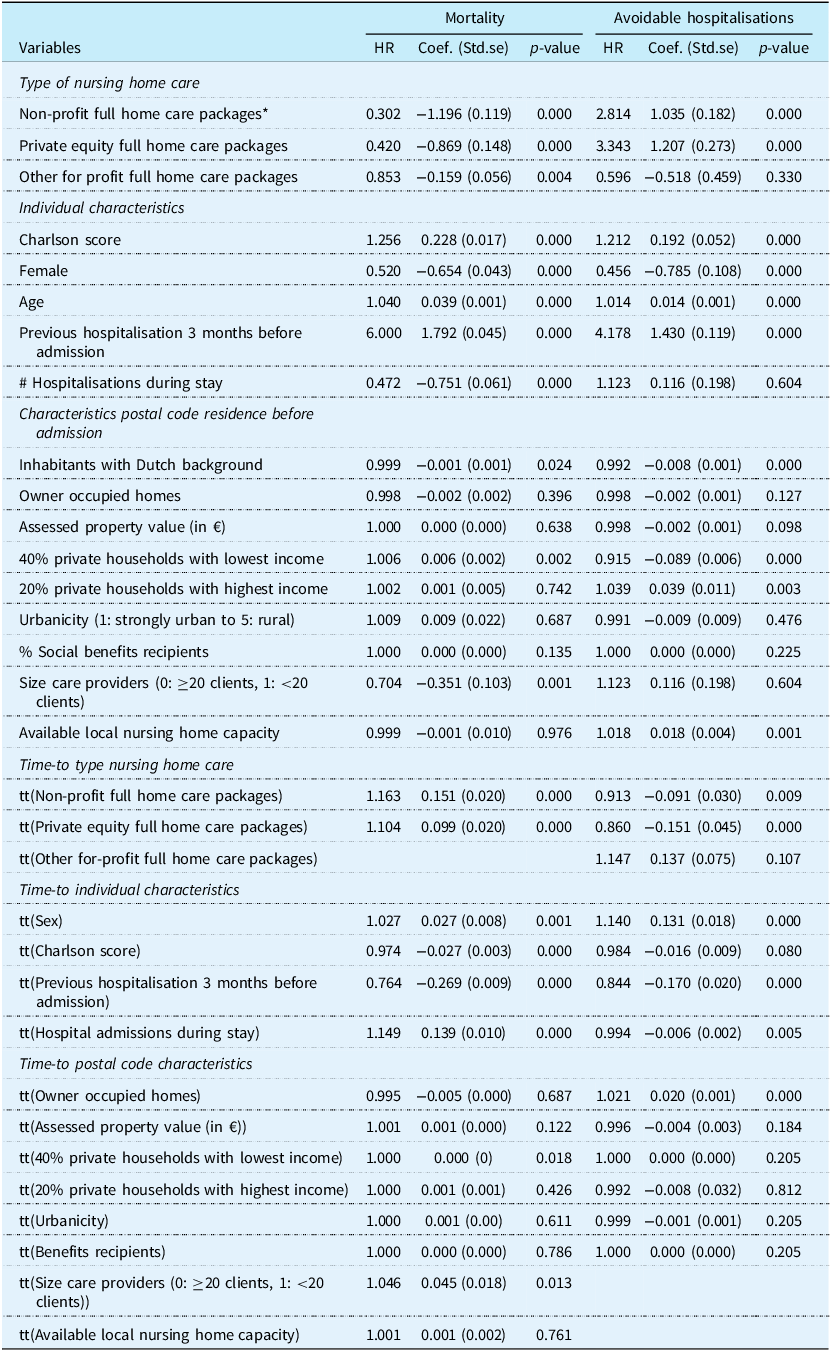
3.4 Results quality of care: avoidable hospitalisations and mortality
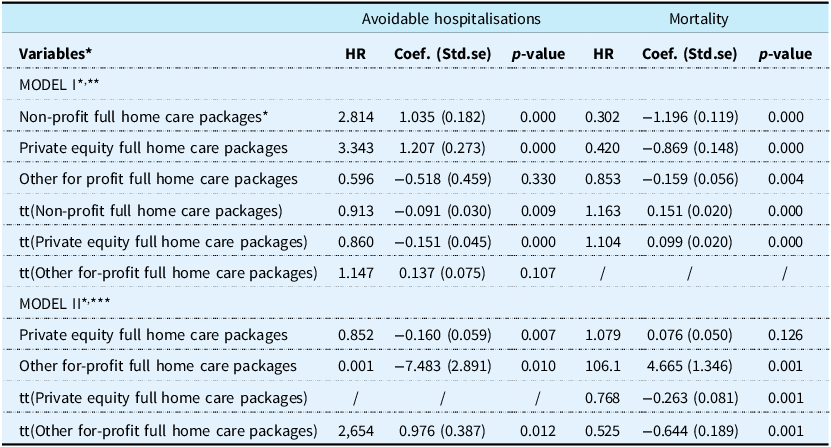
Table 4 shows the estimation results of (time-varying) Cox models assessing the relation between type of nursing home care, avoidable hospitalisations, and mortality. In both models, adjustments were made for differences in health status at admission and during follow-up and for neighbourhood characteristics.
Estimation results time-varying cox models quality of care (excerpt)

Table 4 Long description
A table with two models comparing the estimation results of time-varying Cox models assessing the relation between type of nursing home care, avoidable hospitalizations, and mortality. The table has 12 rows and 8 columns. Column headers are Variables, HR, Coef. (Std.se), p-value for Avoidable hospitalizations, and HR, Coef. (Std.se), p-value for Mortality. Row labels include different types of full home care packages and their time trends. Model I includes Non-profit full home care packages, Private equity full home care packages, Other for-profit full home care packages, and their time trends. Model II includes Private equity full home care packages, Other for-profit full home care packages, and their time trends. Each row provides specific values for HR, Coef. (Std.se), and p-value for both Avoidable hospitalizations and Mortality.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds), the size of the nursing home provider, the observed total number of hospital admissions and four year dummies. Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
*** Reference category: non-profit full home care package.
In model I, avoidable hospitalisations were more likely for both non-profit (coef.: 1.035, p–value = 0.000) and PE-owned full home care packages (coef. = 1.207, p–value = 0.000) than in residential nursing homes. The coefficient over time showed that, though the difference became smaller, this result remained during the whole observation period. For-profit full home care packages showed no significant relationships. At the other side, analyses in model II demonstrated a decreased probability of having avoidable hospitalisations in for-profit firms compared to non-profit firms. This was also consistent with findings based on the Kaplan-Meier curve ‘Avoidable hospitalisations’ in Appendix A. Regarding mortality, in model I, individuals were much less likely to die soon than in residential nursing homes. In model II, individuals in other for-profit firms faced higher mortality rates than in non-profit firms (p–value = 0.001).Footnote 12
4. Discussion
The introduction of for-profit (PE-owned) entities in LTC systems has the potential to enhance efficiency, reduce bureaucracy, and offer more choices for consumers. However, there is a risk of market distortions. The literature on for-profit nursing homes is dominated by experiences in the U.S. and the U.K. and demonstrates on average distortions in mixed markets (Pradhan et al., Reference Pradhan, Weech-Maldonado, Harman, Al-Amin and Hyer2014; Bos et al., Reference Bos, Kruse and Jeurissen2020; Hussem et al., Reference Hussem, Tenand and Bakx2020; Kruse et al., Reference Kruse, Ligtenberg, Oerlemans, Groenewoud and Jeurissen2020; Gupta et al., Reference Gupta, Howell, Yannelis and Gupta2021; Patwardhan et al., Reference Patwardhan, Sutton and Morciano2022).
The Netherlands has a system of organising and financing LTC that is substantially different from the ones in the U.S. and U.K. Care provision for severely disabled individuals aligns closely with the principles of universal health care, the quality of and access to institutional LTC are highly regulated, and financing is largely public with maximum prices and relatively low out-of-pockets payments (Maarse and Jeurissen, Reference Maarse and Jeurissen2016; Bos et al., Reference Bos, Kruse and Jeurissen2020; Bakx et al., Reference Bakx, Schut and Wouterse2021). This may imply that the potential for gaming is more limited compared to other countries.
Our paper suggests no significant market distortions in the Dutch institutional LTC care market. More specifically, we did not find any evidence of risk selection by for-profit (PE-owned) firms. First, we were not able to find any significant relationship between type of ownership and Charlson score. Second, individuals hospitalised in the past three months were more likely to receive care from non-profit residential care facility (care in kind or full home care package) rather than receiving a full home care package in a home-like setting. However, this was possibly due to the urgency following hospitalisation and the availability of crisis spots in these facilities, and not due to risk selection. Similar results hold with regards to other behavioural aspects. In all analyses, we found no evidence of increased probability of nursing home transfers by for-profit (PE-owned) organisations. This finding contradicts the hypothesis that for-profits firms are more likely to discharge unhealthier individuals compared to their (non-profit) counterparts. However, this result should be considered with some caution. First, Dutch nursing home care often involves long waiting lists, making it difficult to transfer to another facility (i.e. the observed number of transfers is low). Second, for the group we studied, the challenge is even greater, as relocation can be particularly stressful for individuals with dementia.
Furthermore, we did not find evidence of more frequent upgrading by for-profit (PE-owned) organisations. The occurrence of upgrading seems to be driven more by the financing structure (i.e., the full home care packages versus residential care) than by whether the organisation is for-profit or non-profit. This finding may partly be explained by the centralised assessment process of the CNAC, which makes it difficult to obtain a higher care entitlement. Finally, although our results indicated lower rates of avoidable hospitalisations in residential care overall, within the subgroup of providers offering care in home-like settings, for-profit firms – particularly those owned by PE – had lower rates of avoidable hospitalisations compared to non-profit firms. The question is why we find results that seem at odds with what other authors find in other countries (Gandhi, Reference Gandhi2023). There are several possible explanations. First, only individuals with an entitlement of the gatekeeper, namely the CNAC, have access to nationally-insured institutional LTC. As a result, the pool of potential clients is likely to be much smaller and more homogeneous than in other countries. Therefore, the profit margin on the care component may be relatively smaller than in other countries. This does not rule out the possibility that for-profit organisations employ better strategies, e.g., to substitute formal care with informal care compared to non-profit organisations, and as such make the provided care cheaper. Second, the market share of for-profits is (much) lower than elsewhere, reducing the scope for (abuse of) market power. Third, the Dutch LTC system is relatively generous and the quality of residential nursing homes is high, making it difficult for for-profit firms to engage in short-termist behaviour, since this would run them out of business.
There are several limitations to our research. First, it is challenging to draw a clear distinction between risk selection and self-selection. While the business strategies of for-profit (PE-owned) nursing homes might be aimed at attracting affluent (healthier) older individuals, only individuals who are expected to have lower levels of care costs are allowed by law to receive care in home-like settings. In addition, some facilities may attract different types of clients, and some clients may be willing to wait until their most preferred option becomes available. For our analysis this distinction does not have policy consequences since we did not find evidence of selection. However in other contexts it may be worthwhile to dig deeper into the distinction. Second, all analyses were performed at the corporate level. For larger chains, particularly those operating within the non-profit nursing home sector and PE-owned nursing homes, there may be unobserved variation in results of the different locations within individual corporations. Third, although we had access to a rich database, we had no access to all potentially relevant outcomes, like more detailed measures of quality of care, clients’ experience, or use of informal care. Some of our results could also have been affected by unmeasured differences in (cognitive or emotional) health or frailty. For instance, cherry picking could still take place based on unobserved behaviour precipitated by mental health decline. Finally, we refrained from examining differences in curative care (e.g., general practitioners (GP) care) between non-profit and for-profit facilities. Notably, the geriatrician employed at the nursing home often serves as the primary care provider within residential settings. Conversely, some evidence shows that clients receiving full care home packages rely more on GP, geriatric, physiotherapy, and hospital care (Aarnink, Reference Aarnink2017; Bakx et al, Reference Bakx, Schut and Wouterse2021). This type of care is not financed through the LTCa but via the Health Insurance Act, and some is voluntarily insured or out of pocket (such as physiotherapy). Additionally, several Dutch stakeholders recently signed a manifesto expressing concern about the quality and accessibility of care for older adults. Based on their observations, clients receiving full care packages in clustered, home-like residential settings were more frequently referred to outpatient clinics and emergency care, had longer hospital stays, and experienced more relocations than those in residential care – particularly when dementia lead to increased care dependency (Landelijke Huisartsenvereniging, 2023). However, their conclusions were mostly based on anecdotical information. While it is already known that clients with full home care packages make use of services covered under the Health Insurance Act, it remains unclear to what extent this results in higher or lower costs compared to residential institutional LTC. Therefore, future research should evaluate the implications for overall care quality and care expenditures of the introduction of full home care packages in the Dutch institutional LTC system. An additional avenue for future research would be to investigate and quantify the potential advantages that for-profit organisations in the Dutch institutional LTC system may have over their non-profit counterparts.
Whilst our results sketch a fairly rosy picture on the current behaviour of for-profit organisations in the institutional LTC market in the Netherlands, there is a word of caution. If scarcity increases and market shares and/or local market power increase, the adversarial incentives may materialise. Examples in various countries as well as other sectors within the Netherlands have shown that one cannot be too careful about this risk. To prevent provider misconduct, several measures can be implemented. We briefly mention three of such measures. First, we could adjust financing schemes to protect residential nursing homes from disadvantages in the face of risk selection. In the current system, not-for-profit organisations receive some compensation for the fact that they have less healthy clients, but one might argue that the compensation does not fully cover the difference in costs. Second, one can levy direct payments in case of transfers from for-profit to the non-profit sector. Whilst we did not find that such transfers took place on a larger scale, this may change in the future. Finally, a code of conduct for the sector can be a light weight ‘soft law- instrument to codify good behaviour. By taking these steps, the benefits of for-profit provision can be harmonised with public interests, thus preventing potential harm.
Acknowledgements
Three authors are affiliated with the Dutch Authority Consumer and Market. However, it is important to note that the views expressed in this paper do not necessarily represent the official position of this Authority. We would like to thank Niek Stadhouders for his valuable feedback and insightful comments, which greatly contributed to improving this manuscript.
Financial support
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Competing interests
The author(s) declare no conflict of interest.
Appendix A.
![]() Non-profit residential
Non-profit residential ![]() Non-profit full home care packages
Non-profit full home care packages ![]() Private-Equity owned full home care packages
Private-Equity owned full home care packages ![]() For-profit full home care packages.
For-profit full home care packages.

Appendix B.
Estimation results multinomial logit model cherry picking

Table B1 Long description
The table presents estimation results of a multinomial logit model for cherry picking among non-profit full home care packages, private equity full home care packages, and other for-profit full home care packages. It includes coefficients, standard errors, and p-values for various variables. The table has 30 rows and 7 columns. Column headers are Variables, Coef. (Std.se) for Non-profit full home care packages, p-value for Non-profit full home care packages, Coef. (Std.se) for Private equity full home care packages, p-value for Private equity full home care packages, Coef. (Std.se) for Other for-profit full home care packages, and p-value for Other for-profit full home care packages. Row labels include Intercept, Individual characteristics (Female, Age, Previous hospitalisation 3 months before admission, Charlson score), Characteristics postal code residence before admission (% Inhabitants with Dutch background, % Owner occupied homes, Assessed property value (in €), % Social benefits recipients, 40% private households with lowest income, 20% private households with highest income, Urbanicity (1: strongly urban to 5: rural)), and Characteristics local supply of nursing homes (Excess capacity (Average numbers of available nursing home beds in a radius of 20km), Size care providers (0: ≥20 clients, 1: <20 clients)). Year 2018, Year 2019, Year 2020, and Year 2021 are also included as variables. Notable trends include significant p-values for most variables across all types of home care packages, indicating strong statistical significance. The coefficients vary widely, reflecting different impacts of the variables on the likelihood of choosing each type of home care package.
* Reference category: non-profit residential
** Reference category: year 2017
Estimation results time-varying cox model lemon-dropping: nursing home transfer

Table B2 Long description
The table presents estimation results of a time-varying cox model for nursing home transfer. It has 28 rows and 4 columns. The columns are labeled as Variables, HR, Coef. (Std.se), and p-value. The table is divided into several groups of variables: Type of nursing home care, Individual characteristics, Characteristics postal code residence before admission, Characteristics local supply of nursing homes, Time-to care setting, Time-to individual characteristics, Time-to postal code characteristics, and Time-to local supply characteristics. Each row lists a specific variable along with its corresponding HR, Coef. (Std.se), and p-value. For example, the first row under Type of nursing home care shows Non-profit full home care packages with HR 0.350, Coef. 1.048 (0.583), and p-value 0.090. The table provides detailed statistical data relevant to nursing home transfers.
Estimation results time-varying cox model upcoding: change of care need entitlement

Table B3 Long description
The table presents estimation results from a time-varying cox model focusing on the change of care need entitlement. It includes variables such as type of nursing home care, individual characteristics, characteristics of postal code residence before admission, characteristics of local supply of nursing homes, time-to-care setting, time-to individual characteristics, and time-to postal code characteristics. The table has 31 rows and 4 columns. Column headers are Variables, HR, Coef. (Std.se), and p-value. Row labels include different variables like Type of nursing home care, Individual characteristics, Characteristics postal code residence before admission, Characteristics local supply of nursing homes, Time-to-care setting, Time-to individual characteristics, and Time-to postal code characteristics. Each row provides specific values for HR, Coef. (Std.se), and p-value. Notable trends include significant p-values for various variables indicating their impact on the change of care need entitlement.
* Reference category: non-profit residential care
Estimation results time-varying cox model quality of care: avoidable hospitalisations

Table B4 Long description
A table with 38 rows and 7 columns comparing mortality and avoidable hospitalizations. Columns are labeled HR, Coef. (Std.se), p-value for Mortality, and HR, Coef. (Std.se), p-value for Avoidable hospitalisations. Row labels include Type of nursing home care, Individual characteristics, Characteristics postal code residence before admission, Time-to type nursing home care, Time-to individual characteristics, and Time-to postal code characteristics. Each row provides specific data points for each column, detailing the impact of various factors on mortality and avoidable hospitalizations.
* Reference category: non-profit residential care
Appendix C:
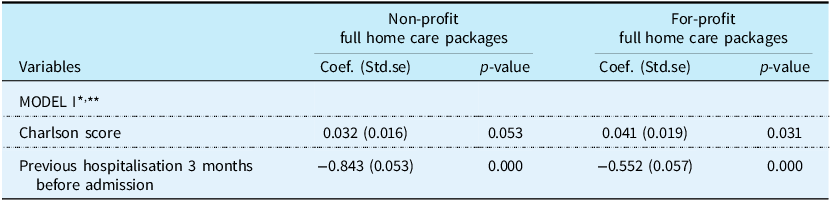
Given the limited understanding of how incentives differ between large PE-owned chains and smaller for-profit long-term care providers in empirical studies, we conducted new sensitivity analyses in which we grouped the PE-owned with the other for-profit entities. Tables 2R, 3R and 4R below report the results of those analyses.
Estimation results risk selection (excerpt)

Table 2R Long description
A table comparing the impact of variables on non-profit and for-profit full home care packages. The table has four rows and three columns. The columns are labeled Non-profit full home care packages and For-profit full home care packages, each with sub-columns for Coefficient (Coef.), Standard Error (Std.se), and p-value. The rows are labeled with the variables: Model 1, Charlson score, and Previous hospitalisation 3 months before admission. Row 1: Model 1, Coef. (Std.se), p-value. Row 2: Charlson score, 0.032 (0.016), 0.053, 0.041 (0.019), 0.031. Row 3: Previous hospitalisation 3 months before admission, -0.843 (0.053), 0.000, -0.552 (0.057), 0.000.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds), the size of the nursing home provider and four year dummies. Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
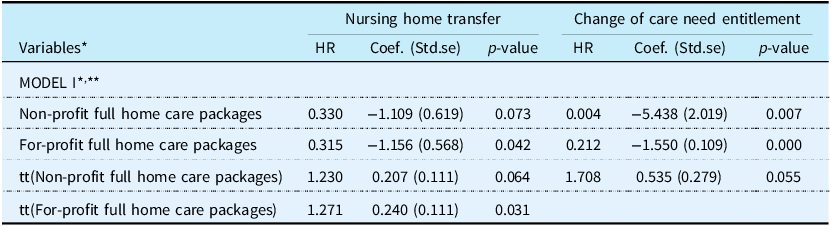
Estimation results Time-varying Cox models Changes in care trajectories (excerpt)

Table 3R Long description
The table presents estimation results from Time-varying Cox models, focusing on changes in care trajectories. It has four rows and three columns. The columns are labeled 'Variables', 'Nursing home transfer', and 'Change of care need entitlement'. The 'Nursing home transfer' column includes sub-columns for 'HR', 'Coef. (Std.se)', and 'p-value'. Similarly, the 'Change of care need entitlement' column includes sub-columns for 'HR', 'Coef. (Std.se)', and 'p-value'. The variables analyzed include 'Non-profit full home care packages', 'For-profit full home care packages', 'tt(Non-profit full home care packages)', and 'tt(For-profit full home care packages)'. Each row provides specific values for these sub-columns. Notable trends include the impact of non-profit and for-profit full home care packages on both nursing home transfer and change of care need entitlement, with varying hazard ratios, coefficients, and p-values indicating the significance of these impacts.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds), the size of the nursing home provider, the observed total number of hospital admissions and four year dummies.
Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
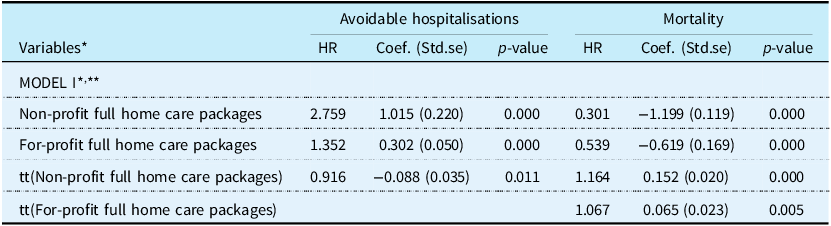
Estimation results Time-varying Cox models Quality of care (excerpt)

Table 4R Long description
A table with four rows and three columns comparing avoidable hospitalizations and mortality rates for different home care packages. The columns are labeled as Avoidable hospitalisations and Mortality. The rows are labeled as Non-profit full home care packages, For-profit full home care packages, tt(Non-profit full home care packages), and tt(For-profit full home care packages). Each column contains values for HR, Coef. (Std.se), and p-value. Row 1: Non-profit full home care packages, HR 2.759, Coef. 1.015 (0.220), p-value 0.000, HR 0.301, Coef. -1.199 (0.119), p-value 0.000. Row 2: For-profit full home care packages, HR 1.352, Coef. 0.302 (0.050), p-value 0.000, HR 0.539, Coef. -0.619 (0.169), p-value 0.000. Row 3: tt(Non-profit full home care packages), HR 0.916, Coef. -0.088 (0.035), p-value 0.011, HR 1.164, Coef. 0.152 (0.020), p-value 0.000. Row 4: tt(For-profit full home care packages), HR 1.067, Coef. 0.065 (0.023), p-value 0.005.
* Corrected for differences in age, gender, characteristics of postal code of residence (including excess capacity of nursing home beds), the size of the nursing home provider, the observed total number of hospital admissions and four year dummies. Estimation results not shown for the sake of brevity.
** Reference category: non-profit residential care.
The additional sensitivity analyses suggest slight differences in incentives between the PE-owned and the other for-profit organisations.
Table 2R (risk selection) shows that the for-profits organisations are more likely to have clients with significantly higher Charlson scores and less likely to have clients who have been hospitalised in the three months before admission. Those results are largely similar to the ones in Table 2 of the manuscript (though the results were not significant for the Charlson score index).
Table 3R (change in care trajectory) shows that the for-profits organisations in general are less likely to transfer clients (whereas the other for-profits organisations in Table 3 were more likely to transfer them (p-value = 0.059)). The results for change of care entitlement are very similar in Table 3 and Table 3R.
Table 4R shows that, in general, for-profit organisations are more likely to have avoidable hospitalisations (although that was only true for the PE-owned organisations in Table 4). The results on mortality are very similar in Table 4 and Table 4R.


 Open access
Open access