


Introduction
Bicuspid aortic valve is one of the most common forms of CHD with an estimated prevalence of 1–2%. Reference Ward1 Although commonly asymptomatic in childhood, it can be associated with serious complications including aortic valve stenosis or regurgitation and ascending aortic dilation, aneurysm, and dissection. Reference Michelena, Desjardins and Avierinos2 Early diagnosis is important and allows for monitoring and, in some cases, intervention before potentially catastrophic complications develop. Given the inheritable nature of bicuspid aortic valve, screening of first-degree family members is recommended with each new diagnosis. Reference Jain, Ammar and Kalvin3 The gold standard for diagnosis is transthoracic echocardiography in children, which has an estimated sensitivity of 92% and specificity of 96%. Reference Chan, Stinson and Veinot4
Left ventricular hypertrophy is a common finding on paediatric electrocardiogram, especially in highly trained athletes. Reference Tague, Wiggs and Li5 This finding is nonspecific with diverse aetiologies including structural heart disease, cardiomyopathy, and non-cardiac causes. Echocardiogram, the gold standard for diagnosis, is often performed with this electrocardiogram finding. In a study analysing 4637 encounters of patients 0–18 years of age with left ventricular hypertrophy comparing electrocardiogram and echocardiogram performed within 24 hours, electrocardiogram had high sensitivity (≥ 90%) but poor specificity (43%), with low positive predictive value (< 20%). Reference Tague, Wiggs and Li5
Current standard of practice for initial echocardiographic assessment for all screening indications in paediatrics is comprehensive echocardiography. While comprehensive echocardiograms provide standardised and detailed information, targeted ultrasonography has been increasingly utilised in many healthcare settings with impressive efficiency and diagnostic results. Real-time cardiac point-of-care ultrasound interpretation performed by paediatric emergency medicine attendings had sensitivity and specificity of 100% and 99.5%, respectively, for both pericardial effusion and left ventricular systolic dysfunction in comparison to expert review. Reference Miller, Arichai and Gravel6 Cardiac point-of-care ultrasound has also been increasingly incorporated into neonatal practice with application in assessment of umbilical venous catheter placement, pericardial effusion, and cardiac tamponade. Reference Singh, Bhombal, Katheria, Tissot and Fraga7
Targeted echocardiogram may be a more cost-effective screening tool. A proof-of-concept pilot study performing cost-benefit analysis on 100 patients with increased cardiac risk showed that a targeted echocardiogram performed before elective non-cardiac surgery may be more cost-effective than conventional comprehensive echocardiogram. Reference Neale, Williams and Canty8 Targeted echocardiogram for low-yield screening indications may be more accessible and more cost-effective and may avoid identification of insignificant incidental findings that lead to costly follow-up visits, imaging studies, and potential stress for patients and their families.
Our study aims to explore the role of targeted echocardiography as a screening tool for bicuspid aortic valve and left ventricular hypertrophy in the paediatric age group. We specifically aim to assess the risk of missing significant cardiac diagnoses that would otherwise be identified by comprehensive echocardiograms.
Methods
Study design and patient selection. This retrospective observational study was approved by the Seattle Children’s Hospital Institutional Review Board. The Picture Archiving and Communication Systems imaging system was queried for echocardiogram studies meeting study criteria. Inclusion criteria were: 1) < 18 years of age at the time of initial screening echocardiogram; 2) comprehensive transthoracic screening echocardiogram was performed; 3) the screening echocardiogram was performed between 2011 and 2020; and 4) indication for screening echocardiogram was bicuspid aortic valve or left ventricular hypertrophy as indicated by the echo screening indication codes below:
-
1. The indication for screening for bicuspid aortic valve included “family history of bicuspid aortic valve.”
-
2. The indication for screening for left ventricular hypertrophy included “left ventricular hypertrophy on electrocardiogram” or “biventricular hypertrophy on electrocardiogram.”
Patients with additional history or exam findings documented in the cardiology visit note meeting the “appropriate” or “may be appropriate” criteria for performing a comprehensive echocardiogram according to the 2014 paediatric appropriate use criteria guidelines were excluded. Reference Campbell, Douglas, Eidem, Lai, Lopez and Sachdeva9 Patients with clinical histories or exam findings not specifically mentioned in the appropriate use criteria guidelines were reviewed by two independent reviewers and excluded from the study if full echocardiogram is deemed indicated by both reviewers.
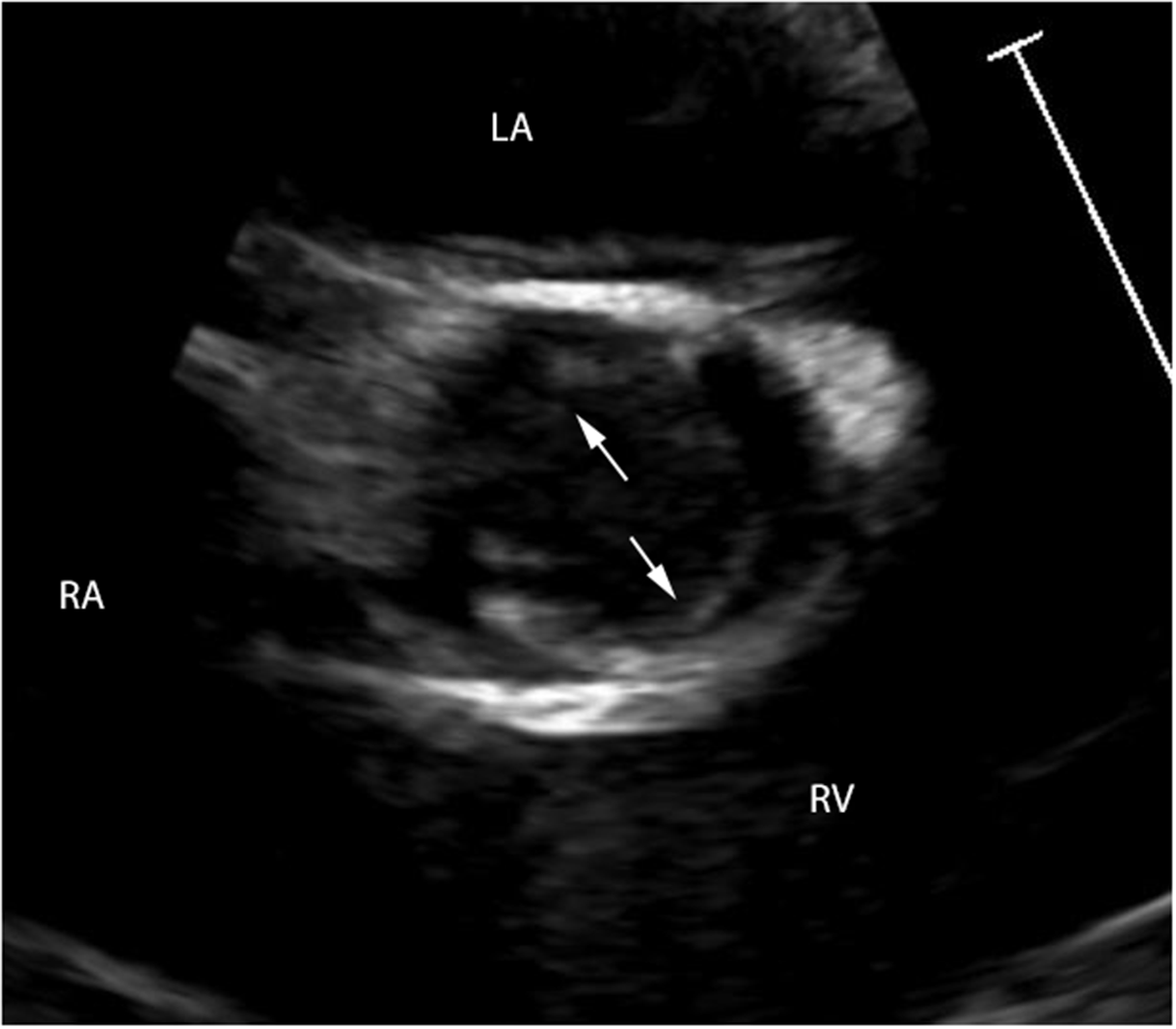
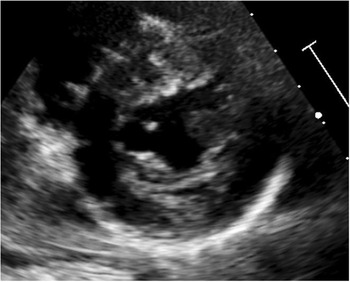
Targeted echocardiogram views. As per institutional protocol, the parasternal short-axis view at the aortic valve portion was routinely used to diagnose bicuspid aortic valve. This view demonstrates loss of normal triangular opening shape of aortic valve morphology in systole in the presence of a bicuspid valve (Figure 1). Similarly, parasternal short-axis view at the level of the papillary muscles was routinely used to diagnose left ventricular hypertrophy as per the American Society of Echocardiography 2024 guideline recommendations to assess wall thickness in short-axis view by 2D or M-mode (Figure 2). Reference Lopez, Saurers, Piers and Barker14
Parasternal short axis at the aortic valve view demonstrating loss of normal triangular opening shape in systole in patient with bicuspid aortic valve.

Parasternal short-axis mid-cavity view allows for assessment of end-diastolic posterior and septal wall thicknesses and relative end-diastolic dimension.

Data collection: Echocardiogram reports were reviewed for findings. Findings other than bicuspid aortic valve or left ventricular hypertrophy were collected as they were likely to be missed if only the targeted echocardiogram view was performed. We recorded all abnormal findings for both groups documented by the contemporary reader in the echocardiogram reports. If follow-up was recommended for the finding, follow-up clinic visits and echocardiogram reports were reviewed to assess for any disease progression or additional findings. Clinical parameters recorded included symptoms, family history, cardiac medications, physical activity restrictions, need for subacute bacterial endocarditis prophylaxis, catheter-/surgery-based interventions, and/or ongoing cardiology follow-up.
Results
Bicuspid aortic valve group
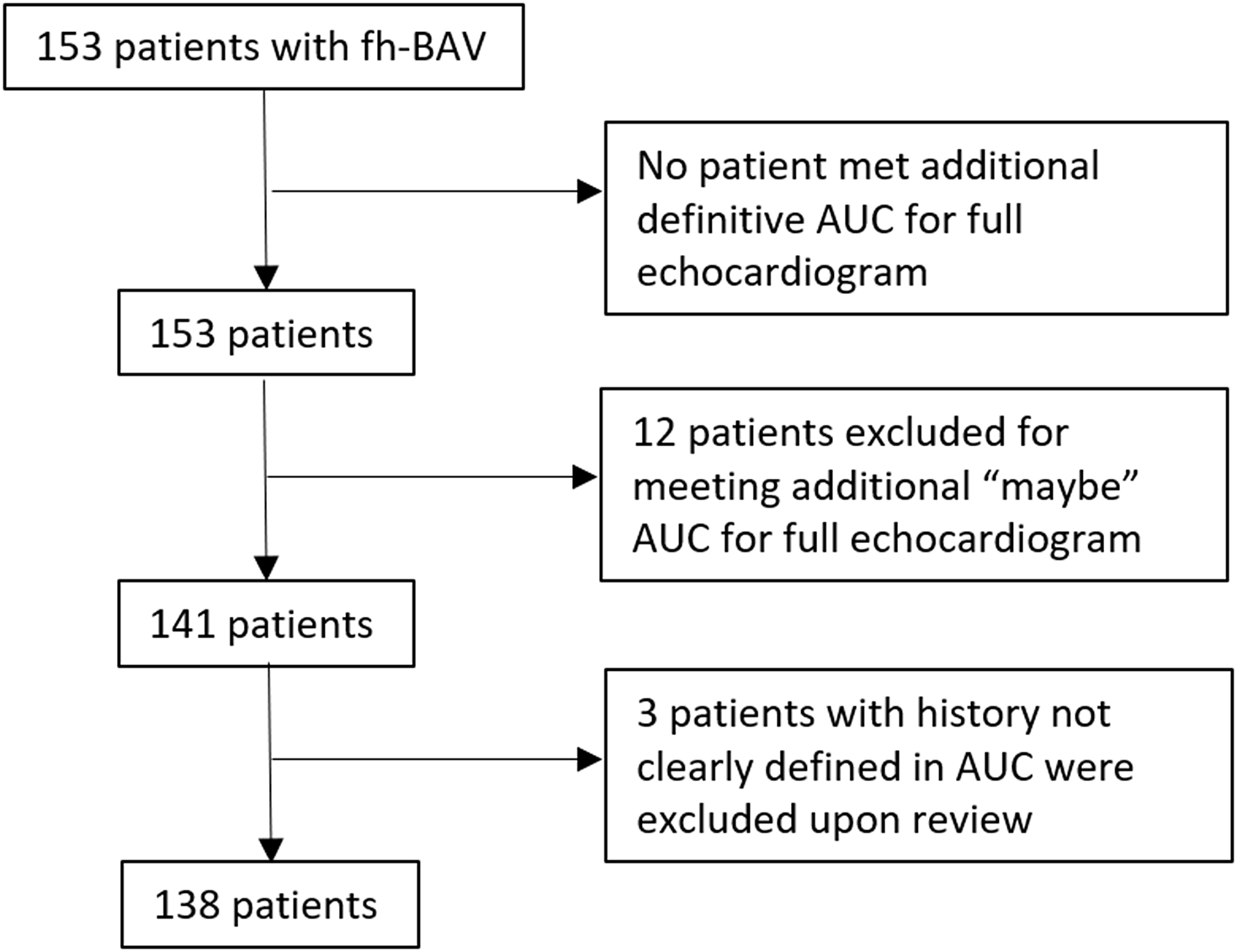
In the study period, 153 comprehensive screening echocardiograms for family history of bicuspid aortic valve were identified; 15 were excluded (Figure 3). Some common indications that met the “may be appropriate” criteria of the 2014 paediatric appropriate use criteria for a full echocardiogram and were hence excluded from this study were: family history of other CHD such as coarctation of the aorta; hypoplastic aortic arch; and hypoplastic left heart syndrome. Of note, presumptively innocent murmur with no symptoms, signs, or findings of cardiovascular disease and a benign family history was not an indication for an echocardiogram according to the appropriate use criteria, and of the 138 patients selected, 24 had documented innocent murmurs on exam. No pathologic murmurs were documented. Four of the 138 patients reported intermittent non-exertional chest pain.
Flow chart of patient selection in the bicuspid aortic valve group. Patients with family history of bicuspid aortic valve who met the 2014 paediatric appropriate use criteria guidelines for a full echocardiogram based on other indications were excluded.

Of the final 138 included in the study, 71 (51%) were males and mean age at echo was 8.4 ± 4.8 years. Bicuspid aortic valve was diagnosed by comprehensive echocardiogram in 5 patients (3.6%).
Incidental findings were noted in 15 (11%) of this group, with four of the 15 patients already diagnosed with bicuspid aortic valve. Of the 11 patients without the diagnosis of bicuspid aortic valve, seven had findings that were determined to be clinically insignificant during their cardiology visit, and follow-up was not recommended (Appendix Table A). Follow-up clinic visit and echocardiogram were recommended for the remaining four; findings and management are shown in Table 1.
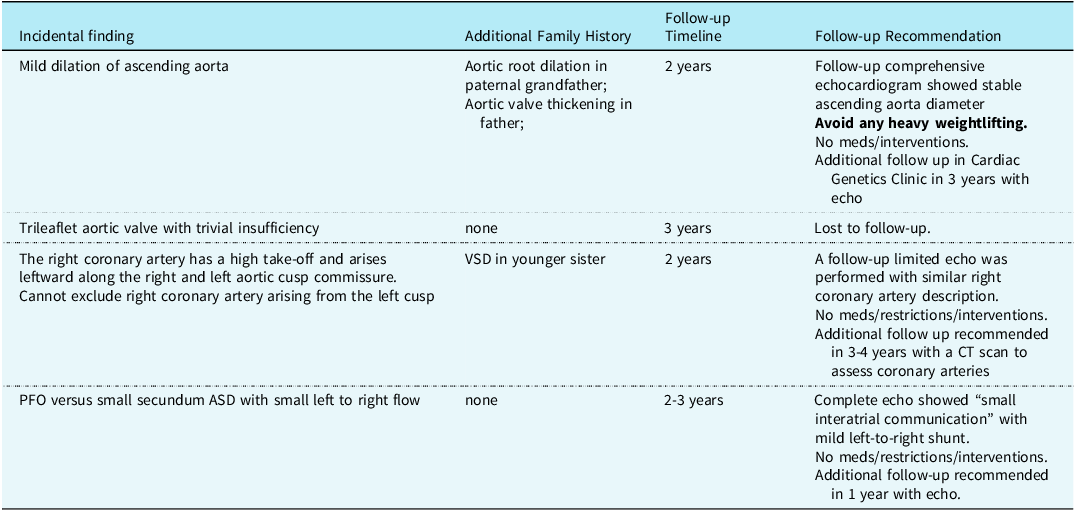
Actionable incidental findings on comprehensive echocardiogram in patients who screened negative for bicuspid aortic valve

These incidental findings include mild aortic root or ascending aorta dilation, trivial insufficiency of aortic valve, high and leftward take-off of the right coronary artery, and one case of patent foramen ovale vs. small secundum atrial septal defect. One patient was lost to follow up but three were seen back at clinic and received either comprehensive or limited follow-up echocardiograms.
One patient without bicuspid aortic valve but with incidental finding of mild dilation of ascending aorta was restricted from heavy weightlifting. This patient had family history of paternal grandfather with aortic root dilation in addition to bicuspid aortic valve; there was a lack of clear family history of presence or absence of connective tissue disorder. The rest of the patients without bicuspid aortic valve who required follow up due to incidental findings resulted in no change in management at their follow up visits, including cardiac medications, physical activity restrictions, need for subacute bacterial endocarditis prophylaxis, and catheter-/surgery-based interventions.
Left ventricular hypertrophy group
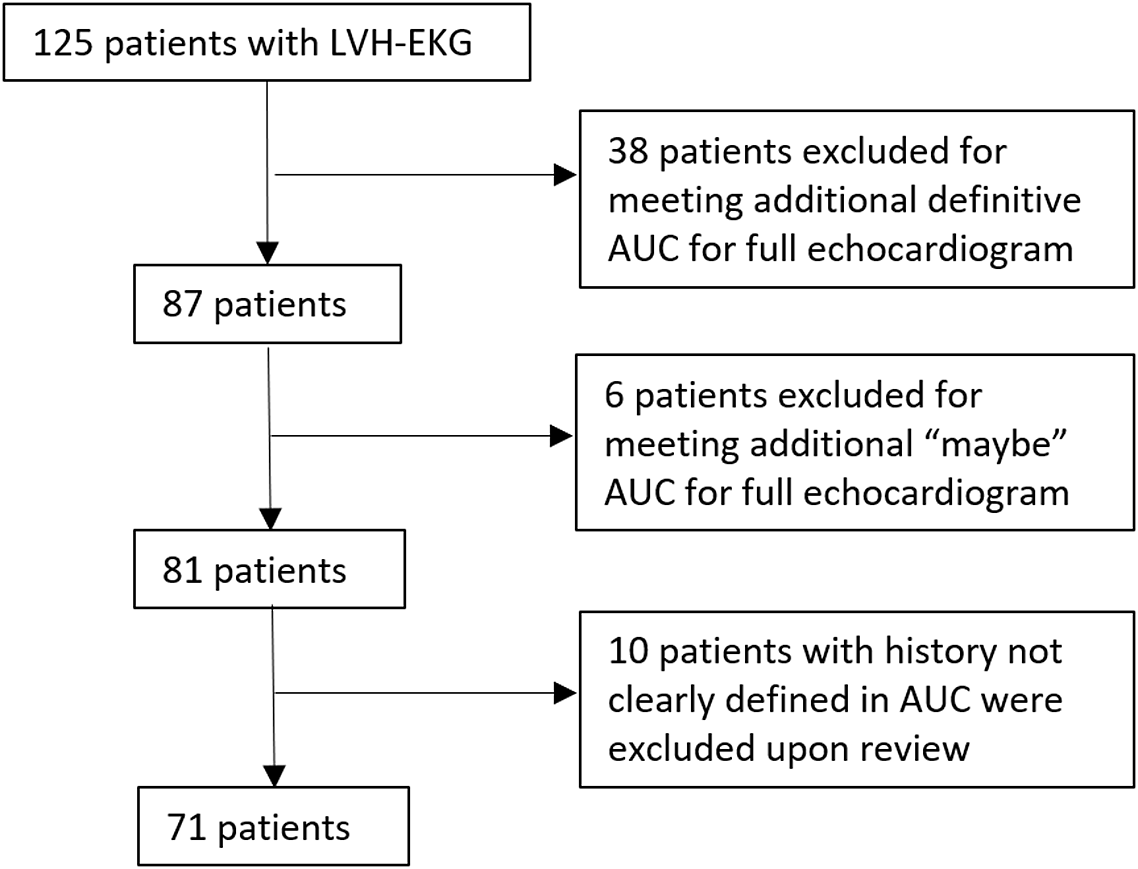
In the study period, 125 comprehensive screening echocardiograms for left ventricular hypertrophy on electrocardiogram were identified; 54 were excluded (Figure 4). Some indications that met the definitive criteria of the 2014 paediatric appropriate use criteria for a full echocardiogram and were hence excluded from this study were: family history of hypertrophic cardiomyopathy; exertional chest pain or non-exertional chest pain with abnormal electrocardiogram; palpitations with abnormal electrocardiogram; systemic hypertension; marfanoid body habitus on exam; and family history of cardiac death before age 50. Of the 71 patients selected, 17 had documented innocent heart murmurs on exam. Of the final 71 included in the study, 58 (83%) were males and mean age at echo was 10.9 ± 4.7 years. Left ventricular hypertrophy was diagnosed in two patients (2.8%) in this screening group by comprehensive echocardiogram.
Flow chart of patient selection in the left ventricular hypertrophy group. Patients with left ventricular hypertrophy on electrocardiograms but who met the 2014 paediatric appropriate use criteria guidelines for a full echocardiogram based on other indications were excluded.

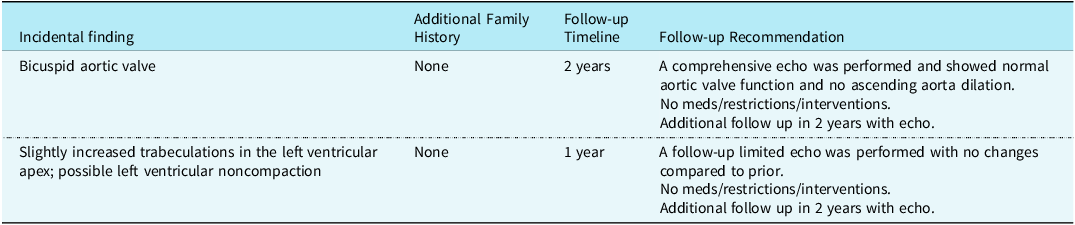
Incidental findings were noted in nine (13%) of this group, with two of the nine patients already diagnosed with left ventricular hypertrophy. Of the seven patients without the diagnosis of left ventricular hypertrophy, five had findings that were determined to be clinically insignificant during their cardiology visit, and follow-up was not recommended (Appendix Table B). Follow-up clinic visit and echocardiogram was recommended for the remaining two; findings and management are shown in Table 2.
Actionable incidental findings in patients who screened negative for left ventricular hypertrophy

These echo findings included one incidental finding of bicuspid aortic valve without family history, another with slightly increased trabeculations in the left ventricular apex, and possible left ventricular noncompaction. Both patients followed up in clinic and had a repeat echo, which resulted in no change in management, including cardiac medications, physical activity restrictions, need for subacute bacterial endocarditis prophylaxis, or catheter-/surgery-based interventions.
Discussion
Targeted echocardiography is a potentially effective screening tool for identifying bicuspid aortic valve and left ventricular hypertrophy in select indications. Most importantly, our study shows only a minor percent (2.8% for both groups) had incidental findings that prompted additional follow-up after the initial screening. Only one patient was found to have mild ascending aorta dilation and was recommended exercise restriction in the bicuspid aortic valve group. The rest of the follow-up group had insignificant incidental findings. Overall, our findings suggest that targeted single-view echocardiographic screening for patients for isolated indication of bicuspid aortic valve and left ventricular hypertrophy is unlikely to result in missed significant forms of heart disease.
We demonstrated a low prevalence of bicuspid aortic valve (3.6%) and left ventricular hypertrophy (2.8%) amongst those referred for isolated family history of bicuspid aortic valve and left ventricular hypertrophy on electrocardiogram, respectively. This estimate in the population we studied is slightly lower than reported by some other studies. Reference Tague, Wiggs and Li5
Screening for bicuspid aortic valve is clinically important and highly cost-effective. In a study utilising an economic evaluation model performing a cost-effectiveness analysis of screening for first-degree relatives of patients with bicuspid aortic valve, it was found that screening with echocardiogram was less costly than no screening, leading to savings of 208 euros and gain of quality-adjusted life years. Reference Tessler, Leshno, Shmueli, Shpitzen, Durst and Gilon15 The average cost of a comprehensive echocardiogram is much higher compared to a point-of-care cardiac ultrasound. For example, a complete transthoracic echocardiogram at some institutions is billed for $1952.2 compared to a limited echocardiogram that is billed for $722.5. 16 Targeted echocardiography could be billed as a limited echocardiogram or point-of-care cardiac ultrasound. In addition to healthcare cost burden of initial screening, incidental findings leading to follow up clinic visits and echocardiograms add to the cost burden of comprehensive screening echocardiograms. Thus, targeted echocardiography may significantly reduce healthcare costs for the screening indications such as bicuspid aortic valve and left ventricular hypertrophy.
Targeted echocardiography may improve availability of care in resource-limited settings as this diagnosis can be mostly made in a single short-axis view image. There is growing evidence suggesting that point-of-care cardiac ultrasound can be learned quickly and performed effectively by non-cardiology medical professionals. Hellmann et al. demonstrated that medical residents learned to perform handheld cardiac ultrasonography at a reasonable rate with minimal formal training followed by one-on-one instruction by a certified technician. Reference Hellmann, Whiting-O’Keefe, Shapiro, Martin, Martire and Ziegelstein10 Engelman et al found that the quality of targeted cardiac ultrasound performed by a briefly trained health worker is adequate for diagnosis of rheumatic heart disease 96.6% of the time. Reference Engelman, Kado and Reményi11 If targeted single-view could be successfully performed by nonexpert scanners with hand-held ultrasound and remote cardiology interpretation, this may greatly improve accessibility for screening echocardiography in low-resource settings. If coupled with artificial intelligence, an emerging tool for disease diagnosis in cardiac imaging, it has the potential to lead to instantaneous, automated diagnosis. Reference Barry, Farina and Chao12
In our study, incidental findings on comprehensive echocardiograms performed for screening for isolated indications of bicuspid aortic valve or left ventricular hypertrophy triggered recommendation for additional cardiology follow-up and testing without a change in management in 93 and 100% of patients with incidental findings in respective groups. While an overall low percentage of clinical significance, these patients may experience anxiety while awaiting results or during observation periods and incur the cost associated with follow-up visits and testing. In a 2019 study on “cascades of care” in adult patients after incidental findings, 99.4% of physicians reported experiencing cascades with resultant patient psychological harm (68.4%), physical harm (15.6%), financial burden (57.5%), frustration (52.5%), and anxiety (45.4%). Reference Ganguli, Simpkin and Lupo13 Performing targeted single-view for specified indications may decrease both financial and non-financial costs associated with incidental findings on standard echocardiography.
One of the limitations of the study is that we did not examine the specific diagnostic accuracy, specificity, sensitivity, and predictive value of targeted single-view echocardiography for screening for bicuspid aortic valve and left ventricular hypertrophy. In future studies, we recommend assessing the diagnostic accuracy by comparing diagnostic accuracy using single echocardiographic views to the gold standard of complete echocardiograms by expert review.
Conclusion
Our study suggests that the risk of missing clinically important incidental findings identifiable with comprehensive echocardiography is extremely low for screening indications of isolated family history such as bicuspid aortic valve or left ventricular hypertrophy on electrocardiogram. Hence, targeted echocardiography focused on short-axis view is potentially an effective screening tool for those with isolated screening indications. Targeted echocardiography would likely reduce the rate of minor clinically insignificant incidental findings, potentially resulting in reduced financial and non-financial healthcare costs. With established appropriate use criteria, it may improve access to screening in remote and resource-limited areas.
Future studies should focus on prospectively evaluating targeted single-view echocardiography sensitivity amongst various echocardiogram screening indications. Efficacy of protocols with hand-held device for screening for bicuspid aortic valve and left ventricular hypertrophy as well as other indications should be explored. This study should serve as a stepping stone for further development of Artificial Intelligence driven automated and hand-held device technology for cardiac screening.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
The author(s) declare none.
Ethical standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committees Institutional Review Boards at the Seattle Children’s Hospital.

 Open access
Open access