


Introduction
Persistent pulmonary hypertension of the newborn is defined by the failure of the normal postnatal decline in pulmonary vascular resistance, typically resulting in impaired oxygenation, right ventricular dysfunction, and pulmonary-to-systemic shunting through the arterial duct. The incidence of persistent pulmonary hypertension in neonates is estimated to be 1.9/1000 live births Reference Walsh-Sukys, Tyson and Wright1 and is linked to significant mortality and morbidity, with a 1-year survival rate of 90% and 15–25% of patients experiencing neurological impairments. Reference Clark, Huckaby and Kueser2,Reference Konduri, Vohr and Robertson3
Treatment of persistent pulmonary hypertension consists of managing hypoxaemia, supporting cardiac function, and treating possible underlying conditions. One of the most important treatments for severe cases is pulmonary vasodilation therapy with inhaled nitric oxide, which reduces smooth vascular muscle tone by activating guanylyl cyclase. Reference Bendapudi, Rao and Greenough4 Treatment with inhaled nitric oxide improves oxygenation and decreases the need for extracorporeal membrane oxygenation. Reference Fraisse, Geva, Gaudart and Wessel5 The most important indication for starting inhaled nitric oxide is extrapulmonary right-to-left shunting, evaluated with transthoracic echocardiography. Reference Abman, Hansmann and Archer6
Echocardiography is a valuable tool for differential diagnosis and in evaluating treatment response in neonatal pulmonary hypertension. Reference de Boode, Singh and Molnar7 Ruling out CHDs, such as total anomalous pulmonary venous drainage, ductal dependent systemic circulation, severe Ebstein’s anomaly, or transposition of great arteries, is essential before treatment decisions. Reference de Boode, Singh and Molnar7 Further evaluations should include assessment of both systolic and diastolic ventricular function, presence and direction of shunts, the severity of pulmonary hypertension and systemic cardiac output, as well as treatment outcomes and complications. Reference McNamara, Jain and El-Khuffash8 Repeated studies are recommended especially in infants who fail to respond to therapy Reference Abman, Hansmann and Archer6,Reference de Boode, Singh and Molnar7
The availability and use of echocardiography have significantly increased during the last decades in neonatal intensive care. Reference Abman, Hansmann and Archer6 Echocardiography performed by a neonatologist is widespread practice, and several recommendation papers have lately been published concerning targeted neonatal echocardiography and point of care ultrasound. Reference Abman, Hansmann and Archer6,Reference McNamara, Jain and El-Khuffash8–Reference Elsayed, Wahab and Mohamed12 It is generally agreed that the first echocardiography should be more comprehensive and rule out CHD. The study can be performed by a neonatologist with advanced experience but should be reviewed by a paediatric cardiologist in a reasonable time frame. Reference Mertens, Seri and Marek9 In general, it is important to distinguish between the comprehensive cardiac assessment performed by paediatric cardiologists and the targeted echocardiography conducted by other specialists as part of clinical decision-making in ICUs. Reference McNamara, Jain and El-Khuffash8,Reference Mertens, Seri and Marek9
Our aim in this study was to evaluate the role of echocardiography and quality of reporting cardiac findings during treatment of persistent pulmonary hypertension among newborn infants receiving inhaled nitric oxide treatment in a tertiary neonatal ICU (NICU).
Materials and method
All neonates who received inhaled nitric oxide for pulmonary hypertension at Oulu University Hospital from September 2016 to September 2021, identified from electronic patient records, were included in this study. Maternal, pregnancy- and birth-related factors (age, body mass index, diabetes, pre-eclampsia, substance use during pregnancy, antenatal steroid use, and the dosage, type of labour, pregnancy complications) were retrieved from patient records. Diabetes type 1 and 2 as well as gestational diabetes were grouped together as diabetes.
The following aspects of birth were collected: spontaneous birth, vaginal birth including vacuum delivery, and caesarean section, including elective, urgent, and emergency sections. Patient characteristics (gender, gestational age, birth weight, umbilical artery pH, Apgar score, medical diagnoses) and information of respiratory care in the NICU (fraction of inspired oxygen, intubation, mechanical ventilation, surfactant dosage, duration, and dosage of nitric oxide) were collected.
Information on the use of echocardiography in the NICU (number of studies, parameters reported in patient files, availability of images, performer) was collected. The performers were categorised as neonatologist, paediatric cardiologist, or paediatrician. When the echocardiography was performed under supervision by paediatric cardiologist, the operator was categorised as cardiologist. Indications for evaluations were divided into two categories: diagnostic and treatment follow-up. Additionally, Picture Archiving and Communication System was used to access archived images. All echocardiography variables in this study were collected retrospectively from the textual content of electronic medical records following the recommendation by de Boode et al. Reference de Boode, Singh and Molnar7
Statistical analysis
Data were analysed using IBM SPSS Statistics for Windows 10, version 29.0.1.0 (171) (SPSS Inc., Chicago, Ill., USA). Data are described as mean ± standard deviation (SD), median [range], and/or n (%). Comparison between the 1st, 2nd, and 3rd echocardiography, as well as comparison of reports between subspecialty groups, was carried out using the Pearson chi-square test. P-value less than 0.05 was considered statistically significant.
Results
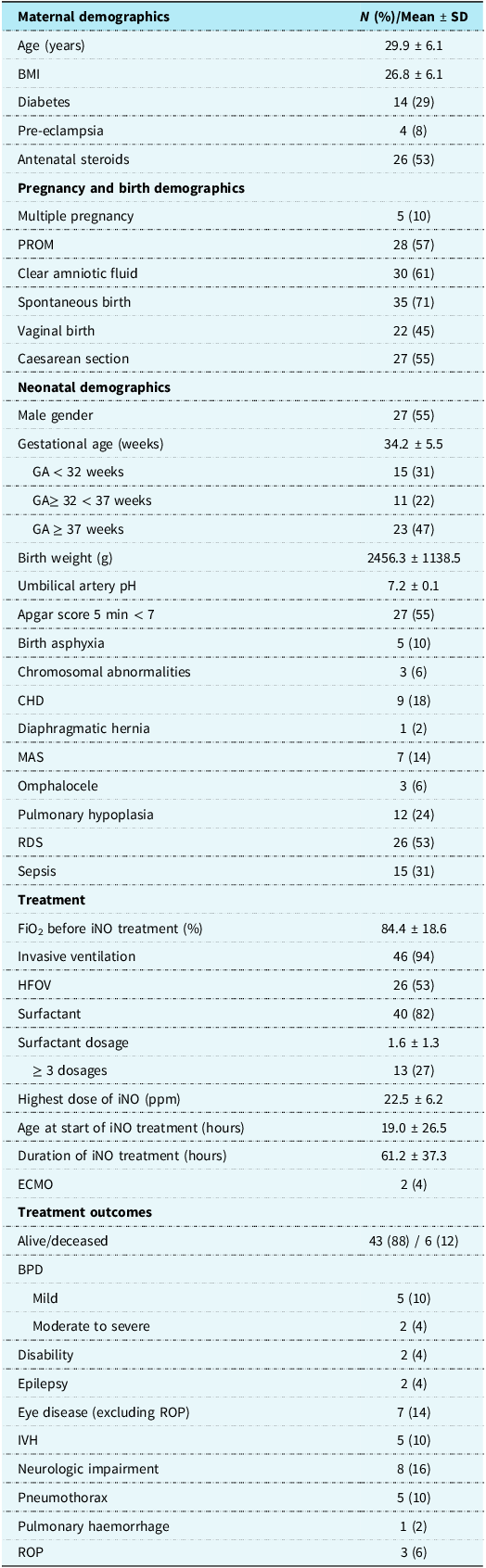
Forty-nine neonates received inhaled nitric oxide during the study period and were included in the analysis. Preterm infants accounted for 53% of the patients, and 31% of them were very preterm, born before 32 weeks of gestation. Detailed patient characteristics, treatment, and treatment outcomes are presented in Table 1.
Maternal and neonatal demographics, treatment and outcomes

Table 1 Long description
The table presents detailed characteristics, treatment, and outcomes for forty-nine neonates who received inhaled nitric oxide. It includes maternal demographics such as age, body mass index, diabetes prevalence, and antenatal steroid use. Pregnancy and birth demographics cover aspects like multiple pregnancies, premature rupture of membranes, mode of delivery, and gestational age. Neonatal demographics detail gender, birth weight, umbilical artery pH, Apgar scores, birth asphyxia, chromosomal abnormalities, and various neonatal conditions such as congenital heart disease, diaphragmatic hernia, and others. Treatment information includes the use of invasive ventilation, high-frequency oscillatory ventilation, surfactant, inhaled nitric oxide dosage and duration, and extracorporeal membrane oxygenation. Treatment outcomes cover survival rates, bronchopulmonary dysplasia, disabilities, epilepsy, intraventricular hemorrhage, neurologic impairment, pneumothorax, pulmonary hemorrhage, and retinopathy of prematurity.
BMI = body mass index; BPD = bronchopulmonary dysplasia; ECMO = extracorporeal membrane oxygenation; FiO2 = fraction of inspired oxygen; GA = gestational age; HFOV = high frequency oscillatory ventilation; iNO = inhaled nitric oxide; IVH = intraventricular haemorrhage; MAS = meconium aspiration syndrome; PROM = prelabour rupture of membranes; RDS = respiratory distress syndrome; ROP = retinopathy of prematurity.
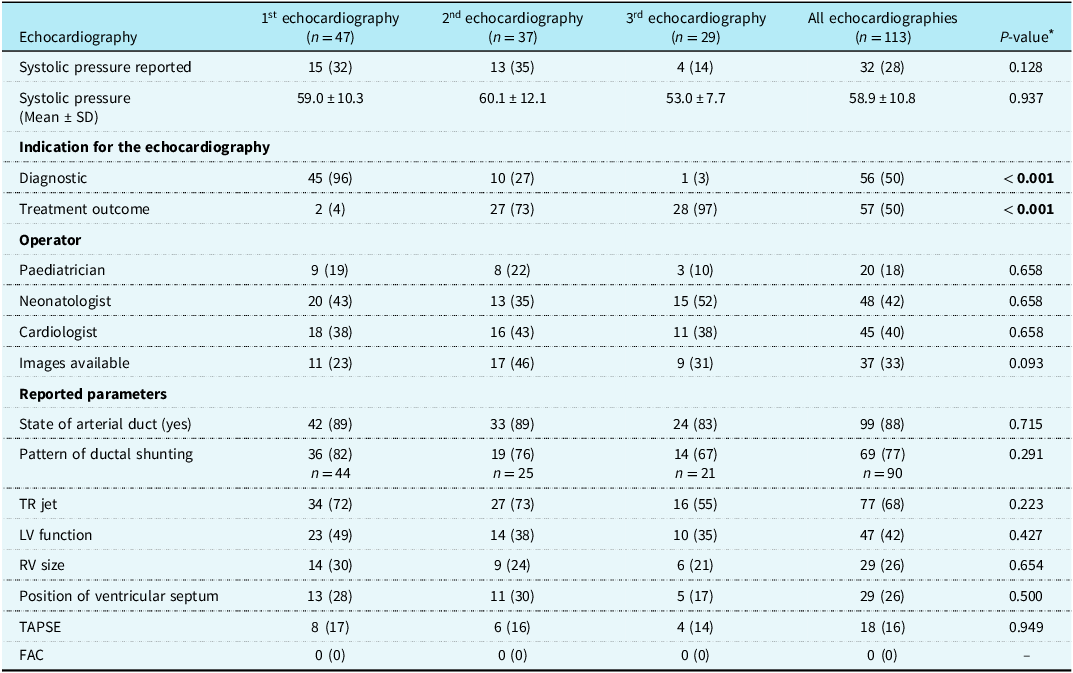
Altogether, 113 echocardiographs were performed on 47 patients during their stay in the NICU, with a median of three evaluations per patient, ranging from 0 to 9. All reports were included in the analysis. Two critically ill patients received inhaled nitric oxide as a rescue therapy without echocardiography but did not respond to treatment and died soon after. The causes of death were severe birth asphyxia and severe lung hypoplasia caused by extremely premature birth. The indication for echocardiography was diagnostic in the first imaging (96%) and treatment response in 97% of occasions for the third evaluation. Systolic blood pressure was mentioned in 28% of reports, with the median pressure being 59 mmHg. The most often reported parameters were presence and pattern of ductal shunting (88% and 75%, respectively). Fractional area change of right ventricle was not given in any of the reports, and images were archived only in 33% of occasions. Detailed echocardiography information is presented in Table 2.
Echocardiography results

Table 2 Long description
The table presents data from three echocardiography evaluations, showing systolic pressure reported in 28 percent of cases with a mean of 58.9 millimeters of mercury. Diagnostic indications dominate the first evaluation at 96 percent, while treatment outcomes are primary in the third at 97 percent. Various operators, including pediatricians, neonatologists, and cardiologists, conducted the evaluations. Reported parameters frequently include the state of arterial duct and pattern of ductal shunting, with images available in 33 percent of cases. The table highlights trends in reporting and operational practices across evaluations.
Data are presented as N (%) if not otherwise mentioned. Significant p-values are bolded. FAC = fractional area change; LV = left ventricle; PFO = patent foramen ovale; RV = right ventricle; SRT = surfactant replacement therapy; TAPSE = tricuspid annular plane systolic excursion; TR peak velocity of tricuspid regurgitation.
* Pearson’s chi-square test was used for comparison between the groups.
Echocardiographs were mostly performed by neonatologists (42%) and cardiologists (40%). Comprehensive evaluation to rule out CHD was done by paediatric cardiologist in 56% of cases, and cardiologists archived images more often than neonatologists (53% and 6%, respectively, P < 0.001). They also more frequently reported findings systematically compared to neonatologists and paediatricians (Figure 1). Systolic blood pressure, left ventricular function, size or function of right ventricle, septum deviation, and tricuspid regurgitation jet velocity were commonly reported by cardiologists and less often by neonatologists. Paediatricians often mentioned systolic blood pressure and patency of arterial duct and described ductal shunting, but paid less attention to the ventricular function (Figure 1).
Comparison of reported echocardiography parameters based on performers’ background. Pearson’s chi-square test revealed statistically significant differences between neonatologists and cardiologists in every parameter; between neonatologists and paediatricians in systolic blood pressure, RV size, septum deviation, TAPSE and TR jet; between paediatricians and cardiologists in LV function, patency of the arterial duct and shunt direction. LV = left ventricle; PFO = patent foramen ovale; RV = right ventricle; SRT = surfactant replacement therapy; TAPSE = tricuspid annular plane systolic excursion; TR peak velocity of tricuspid regurgitation.

Figure 1 Long description
The bar graph compares echocardiography parameters based on performers' background, showing percentage values for pediatricians, neonatologists, and cardiologists. The x-axis lists parameters: systolic blood pressure, ductus open, ductal pattern, TR jet, LV function, RV size, septum position, and TAPSE. The y-axis represents percentage values ranging from 0 to 100. Each parameter has three bars representing pediatricians, neonatologists, and cardiologists, with different heights indicating varying percentage values. The color scheme includes black for pediatricians, dark gray for neonatologists, and light gray for cardiologists. Notable trends include higher percentages for cardiologists in most parameters. Annotations indicate statistical significance with P-values for each comparison. All values are approximated.
Six patients (12%) died, and two patients required extracorporeal membrane oxygenation and thus were transferred to the national paediatric extracorporeal membrane oxygenation centre in Helsinki. Invasive ventilation was needed in 94% of patients and high frequency oscillatory ventilation as a rescue mode of ventilation in 53% of cases. Three patients, who did not require intubation or surfactant treatment, received oxygen and inhaled nitric oxide via nasal cannulae. The median fraction of inspired oxygen was 0.9 before starting inhaled nitric oxide and time from birth to treatment 10 hours. Detailed information on treatment and outcomes is presented in Table 1.
Discussion
In our unit, echocardiography performed by both neonatologists and paediatric cardiologists was frequently used in diagnosing and monitoring treatment response in neonates suffering persistent pulmonary hypertension. However, a systematic approach to assessment, reporting, and saving images is yet to be established. It appears that current clinical practice is still relatively far from recently published detailed guidelines, Reference McNamara, Jain and El-Khuffash8,Reference Singh, Bhombal and Katheria13 when evaluated retrospectively in light of documentation from patient files.
Cardiologists demonstrated a more structured approach to echocardiography compared with neonatologists and paediatricians, likely reflecting differences in training and their distinct roles within multidisciplinary teams. Reference Noori, Ramanathan, Lakshminrusimha and Singh14 Neonatologists appeared primarily focusing on excluding major heart defects and contraindications prior to initiating treatment, whereas cardiologists conducted a more comprehensive evaluation during regular office hours. Thereafter, neonatologists continued to evaluate treatment response at bedside. Similar workflow has previously been reported from Italian NICUs. Reference Corsini, Ficial and Fiocchi15,Reference Casani, Tozzi and Cocca16 Targeted neonatal echocardiography has become an important part of assessing critically ill neonates in NICU, and neonatology trainees are increasingly motivated to pursue formal training. Reference Cleator and Subhedar17
Systematic approach to echocardiography would help in building routines that support clinical decisions in timely manner, but insufficient time and limited supervision constitute the principal barriers to implementation in the current era across many units, including our own. Reference Corsini, Ficial and Fiocchi15,Reference Cleator and Subhedar17 De Boode et al. proposed a practical echocardiographic protocol for persistent pulmonary hypertension and suggested that initial assessment should include structural evaluation of the heart to rule out CHD, assessment of pulmonary artery pressure measured from the tricuspid regurgitation, shunt direction from patent ductus arteriosus and patent foramen ovale, interventricular septum position, subjectively assessed right ventricular size, and objective assessment of ventricular function. Reference de Boode, Singh and Molnar7 Current guidelines often enumerate a broad range of parameters for assessment, yet provide limited clarification regarding their relative clinical relevance or association with patient outcomes. Reference McNamara, Jain and El-Khuffash8,Reference Elsayed, Wahab and Mohamed12,Reference Singh, Tissot and Fraga18 In a relatively busy clinical environment, where the same personnel are responsible for both echocardiographic assessment and direct patient care, it would be helpful if the guidelines highlighted clear and reproducible core measurements that are valuable for clinical decision-making and patient prognosis in a given disease condition, with more detailed supplementary parameters presented separately. Reference Bunting, Steeds and Slater19,Reference Breinig, Dicky and Ehlinger20
Our study showed that neonatologists tend to rely on ductal shunting and tricuspid regurgitation when evaluating the severity of pulmonary hypertension. Only few reported other than eyeballing on ventricular function, even though more detailed evaluation of right ventricular function in this patient population might help in identifying those at higher risk for needing extracorporeal membrane oxygenation. Reference Aggarwal, Agarwal and Natarajan21 This would be important especially in NICUs, such as ours, that are located far from these services.
Image archiving was unexpectedly infrequent in our study cohort, likely reflecting several contributing factors, most notably operator behaviour, as earlier limitations in data management and transfer may have influenced image acquisition practices. As modern systems no longer impose such technical constraints, routine archiving of echocardiography images is now both feasible and advisable. Reference McNamara, Jain and El-Khuffash8 Establishing systematic image archiving and documentation should constitute the initial step toward enhancing the quality of image acquisition, the consistency of reporting, and the structure of fellow training. Image archiving is essential for evaluating hemodynamic changes during serial assessments in the NICU and perhaps even more importantly would facilitate e-consultations between specialists across centres for the most critically ill neonates. Reference Padovani, Singh and Pass22
Strengths and limitations
This is one of the few studies evaluating the clinical imaging practices in the era of increased availability of echocardiography and updated guidelines for different subspecialties. We had comprehensive data collection, and all neonates who had received inhaled nitric oxide in our NICU were included in this study without dropouts.
The most important limitation of our study arises from the retrospective design and constraints in the data availability. These factors limit our ability to determine whether, or to what extent, the quality of echocardiography reports influenced clinical decision-making or treatment outcomes. Furthermore, all patients with mild pulmonary hypertension who did not require vasodilator therapy were excluded from our study, and thus, the role of echocardiography in managing less severely ill neonates could not be assessed.
Conclusion
Transthoracic echocardiography is widely used by all specialists involved in the treatment of persistent pulmonary hypertension of neonate. There is considerable variation in reporting the study findings, and clinical imaging practices seem to diverge substantially from the published guidelines. We suggest addressing this gap through structured training and by providing simple guidelines that rank the parameters by importance, prioritising those that clearly guide treatment decisions and correlate with patient outcomes. A template for documenting the parameters, together with guidance on how to perform a brief but systematic assessment of the key points in each clinical setting, would be beneficial.
Acknowledgements
None.
Financial support
The Finnish Foundation for Pediatric Research supported Dr Kallio. The funder had no role in this study’s design, data collection and analysis, or reporting. Other authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests
None.
Ethical standard
This study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments and comparable ethical standards. The study protocol was approved by the Oulu University Hospital with registration number 80/2022. The ethical committee of the Northern Ostrobothnia Health Care District was consulted on ethical aspects, and, due to the quality control nature of the retrospective data evaluation, there was no need for informed consent.
Tweet
“Clinical echocardiography use in NICU often diverges from guidelines—revealing a gap between recommendations and daily practice.”


 Open access
Open access