


Introduction
Ketamine is a dissociative anaesthetic, derived from phenylcyclohexylamine, that exerts analgesic, anti-inflammatory, and anti-depressant actions. The anaesthetic and analgesic properties of ketamine correlate to its main mechanism of action as a non-competitive antagonist of the N-methyl-D-aspartate receptor, a subtype of glutamate receptor involved in pain transmission, mood regulation, and consciousness. Antagonism of these receptors increases glutamate levels in the brain, which promotes the release of brain-derived neurotrophic factor and supports synaptogenesis. Reference Domino1–Reference Dasari and Ninave5
Additional pharmacological targets of ketamine include dopamine, serotonin, γ-aminobutyric acid, opioid, and cholinergic receptors and hyperpolarisation-activated cyclic nucleotide-gated and voltage-gated sodium channels. Ketamine prevents the reuptake of catecholamines like norepinephrine and epinephrine, producing a hyperadrenergic state including elevated heart rate and blood pressure. Interaction with serotonin transporters increases extracellular serotonin and dopamine levels by inhibiting their reuptake. Inhibition of M1 muscarinic acetylcholine receptors results in central and peripheral anticholinergic adverse effects associated with ketamine, such as drowsiness and increased sympathetic tone. Ketamine also interacts with opioid receptors (mu, delta, and kappa), which contributes to its analgesic and psychoactive properties. Reference Domino1–Reference Dasari and Ninave5
Due to its multifaceted pharmacological profile with the potential to stimulate sympathetic activity and produce negative inotropic effects, ketamine raises concern for haemodynamically significant alterations. Reference Dasari and Ninave5 For patients in the cardiac intensive care unit, haemodynamic stability is often tenuous, and thus finding an anaesthetic that limits these changes is paramount. Reference Williams and Friesen6–Reference Loomba, Gray and Flores13 The primary aim of this study was to characterise the effect of a single dose of intravenous ketamine on heart rate, arterial saturation, respiratory rate, mean arterial blood pressure, central venous pressure, and renal near infrared spectroscopy.
Methods
Study design
This study was a single-centre, retrospective study utilising high-fidelity physiologic data aggregated using the Sickbay platform (Medical Informatics Company, Houston, TX). The primary aim of this study was to characterise the effect of a single dose of intravenous ketamine on heart rate, arterial saturation, respiratory rate, mean arterial blood pressure, central venous pressure, and renal near infrared spectroscopy. Secondary aims of this study were to quantify the occurrence of unexpected apnoea within 30 min of ketamine administration and the need for cardiopulmonary resuscitation, bolus vasoactive medication, or bolus intravenous fluids within 30 min of ketamine administration.
Patient and administration selection
Patients cared for in the paediatric cardiac intensive care unit who received a dose of intravenous ketamine were identified between January 1, 2022, and May 1, 2025. The year 2022 was utilised as the initial year as it was the year that haemodynamic data routinely began being captured by Sickbay at the institution. Patients without data captured in Sickbay and those on mechanical circulatory support (ventricular assist device or extracorporeal membrane oxygenation) were excluded from the study. Administrations without an arterial line in place during the study period were also excluded. As the aim was to identify the effect associated with a single dose, only ketamine administrations without a ketamine administration in the preceding 30 min were included. This interval was selected as paediatric data demonstrates that intravenous ketamine’s physiologic effects last 10 to 20 min.
Clinical practice
At Ann & Robert H. Lurie Children’s Hospital, ketamine is used in the cardiac intensive care unit for analgesia in acute situations of patient discomfort as well as for procedural sedation. Intravenous dosing is generally either 0.5 mg/kg or 1 mg/kg per dose in this specific unit dependent on clinical indication.
Variables of interest
Data for the following physiologic variables were collected: heart rate, arterial saturation, respiratory rate, mean arterial blood pressure, and renal near infrared spectroscopy. All datapoints were captured and recorded by Sickbay. The data were retrieved from Sickbay with a 1-s temporal resolution.
The following are the units and devices from which these data were captured and sent to Sickbay: heart rate was captured as beats per minute from telemetry; arterial saturation was captured in percent via a pulse oximeter; respiratory rate was captured in respirations per minute via a pulse oximeter; mean arterial blood pressure was collected in mmHg via an arterial line; renal near infrared spectroscopy was captured in percent via the INVOS 5100 system (Medtronic, Boston, MA).
Patient age at the time of ketamine administration was captured in months with weight captured in kilograms. The patient’s primary circulatory physiology was categorised as one of the following: fully septated biventricular, left to right shunt, limitation to systemic flow, limitation to pulmonary flow, pre-operative transposition, functionally univentricular multidistributive, functionally univentricular Glenn, functionally univentricular Fontan, or ventricular dysfunction. Patients may certainly exist in multiple circulatory physiologies and thus what was considered the primary circulatory physiology was utilised. Data on patient orthotopic heart transplant status was recorded and captured as well. The presence or absence of mechanical ventilation at the time of ketamine administration was recorded as well. This reflected if the patient was intubated prior to the ketamine administration of interest. Concurrent usage of bolus opioids, benzodiazepines, and paralytics administered during the period of interest were also captured.
Vasoactive inotrope score was also collected. Apnoea during the study period and need for a fluid bolus, vasoactive bolus, or cardiopulmonary resuscitation were also recorded.
Time period
The study period selected was 30 min prior to the administration of ketamine and 30 min after administration. Any time prior to administration was assigned a phase of “pre” while any time after administration was assigned a phase of “post”. Relative time was calculated in relation to the time of administration in seconds.
Statistical analyses
Continuous variables are presented as mean and standard deviation while categorical variables are presented as an absolute count and percent.
Multivariable linear regression modelling was utilised to evaluate the association between ketamine administration and changes in the tracked haemodynamic parameters while incorporating covariates that could influence physiologic response. The dependent variables modelled included heart rate, arterial saturation, respiratory rate, mean arterial blood pressure, central venous pressure, and renal near infrared spectroscopy. Each model was constructed using an ordinary least squares approach. Independent variables included in the model were the following: ketamine dose (mg/kg), circulatory physiology, opioid administration, benzodiazepine administration, paralytic administration, and time phase. A separate model was created for each dependent variable.
For each physiologic variable, missing data was imputed. This imputation was done using median imputation as this smooths over short periods of time without altering the overall trajectory of the data. Because these analyses pooled all time-aligned values into a regression model rather than applying time-series forecasting for each individual, this framework functioned analogously to an autoregressive integrated moving average with exogenous covariates model, albeit implemented through cross-sectional regression conditioned on pre/post time phase and covariates.
It is important to note that the statistical methodology uses data from before and after the administration and the data from before serves as the control. Thus, while there isn’t a traditional control arm, this methodology utilised with time-series data does have control data, allowing for the effect of ketamine to be estimated. Detailed discussion of the statistical methods is beyond the scope of this manuscript but the control data in time-series regressions and the strong correlation of results from such analyses when compared to randomised controlled trials are described in the literature.
An unsupervised cluster analysis was performed to help identify naturally occurring clusters using a machine learning approach. This was done utilising an agglomerative hierarchical clustering using Ward’s linkage method. The pairwise Euclidean distances between standardised physiologic change vectors were computed, and cluster linkage was performed. Ideal cluster number was determined using calculated silhouette scores.
All models were implemented in Python using the statsmodels package.
Results
Cohort characteristics
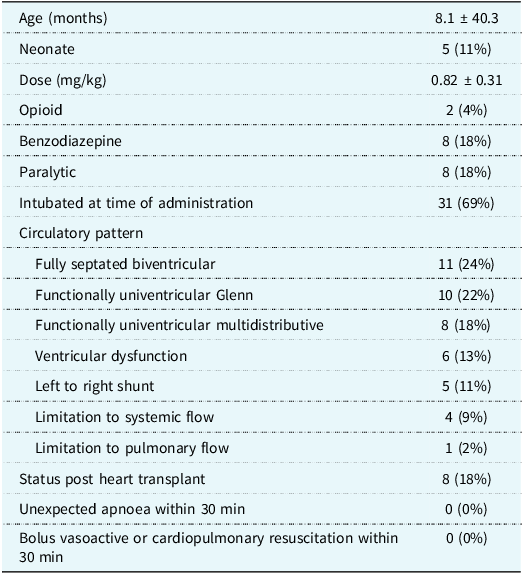
A total of 45 administrations were included in the final analyses. The average age was 8.1 months and the average weight was 9.3 kg. The most frequent circulatory physiologies were fully septated biventricular (24%) and functionally univentricular Glenn (22%). Of all patients, 18% were status post orthotopic heart transplant. A bolus opioid was administered during the study period in 4%, a bolus benzodiazepine was administered during the study period in 18%, and a bolus paralytic was administered during the study period in 18% (Table 1).
Cohort characteristics

Of the 45 administrations, 26 (58%) were receiving vasoactive support. In these 26 administrations, milrinone was being utilised in 20 of these and epinephrine in 11 of these. The vasoactive inotrope score did not statistically significantly change over the study period.
No unexpected apnoea was noted following ketamine administration. While some doses of ketamine included were used intentionally for intubation, there were no unexpected intubations. No cardiopulmonary resuscitation, fluid bolus, or bolus vasoactives were required after ketamine administration. A change in vasoactive score occurred in 2 patients, with 1 patient having an increase of 2 and the other an increase of 1.
The average ketamine dose was 0.8 mg/kg/dose.
Heart rate
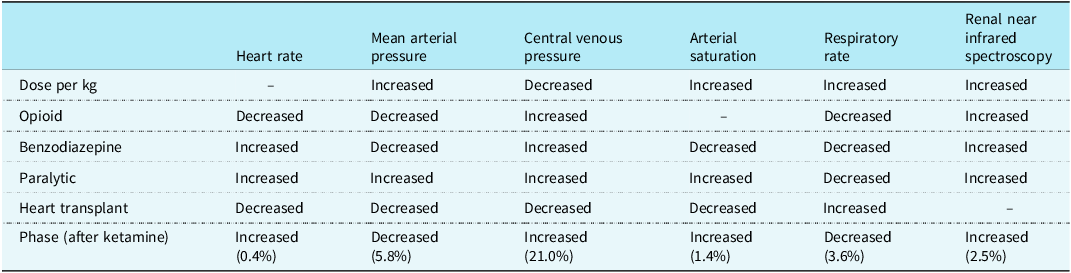
Ketamine administration was independently associated with an increase in heart rate (Figure 1). There was approximately a 0.4% increase in the 30 min following administration. Opioid, benzodiazepine, paralytic, and presence of heart transplant were independently associated with a decrease in heart rate (Table 2).
Graph of percent change in heart rate over time. The shaded area is the 95% confidence interval.

Effects by regression

Arterial saturation
Ketamine administration was independently associated with an increase in arterial saturation (Figure 2). There was approximately a 1.4% increase in the 30 min following administration. Paralytic was also independently associated with an increase in arterial saturation. Benzodiazepine and heart transplant were independently associated with a decrease in arterial saturation (Table 2).
Graph of percent change in arterial saturation over time. The shaded area is the 95% confidence interval.

Respiratory rate
Ketamine administration was independently associated with a decrease in respiratory rate (Figure 3). There was approximately a 3.6% decrease in the 30 min following administration. Opioid, benzodiazepine, and paralytic were all independently associated with a decrease in respiratory rate. Heart transplant was independently associated with an increase in respiratory rate (Table 2).
Graph of percent change in respiratory rate over time. The shaded area is the 95% confidence interval.

Mean arterial blood pressure
Ketamine administration was independently associated with a decrease in mean arterial blood pressure (Figure 4). There was approximately a 5.8% decrease in the 30 min following administration. Opioid, benzodiazepine, and heart transplant were independently associated with a decrease in mean arterial blood pressure. Paralytic was independently associated with an increase in mean arterial blood pressure (Table 2).
Graph of percent change in mean arterial pressure over time. The shaded area is the 95% confidence interval.

Central venous pressure
Ketamine was independently associated with an increase in central venous pressure (Figure 5). There was approximately a 21% increase in the 30 min following administration. Opioid, benzodiazepine, and paralytic were independently associated with an increase in central venous pressure (Table 2).
Graph of percent change in central venous pressure over time. The shaded area is the 95% confidence interval.

Renal near infrared spectroscopy
Ketamine was independently associated with an increase in renal near infrared spectroscopy (Figure 6). There was approximately a 2.5% increase in the 30 min following administration. Opioid, benzodiazepine, and paralytic were also independently associated with an increase in renal near infrared spectroscopy (Table 2).
Graph of percent change in renal near infrared spectroscopy over time. The shaded area is the 95% confidence interval.

Summary of ketamine findings
Ketamine administration was independently associated with a 0.4% increase in heart rate, a 1.4% increase in arterial saturation, a 3.6% decrease in respiratory rate, a 5.8% decrease in mean arterial blood pressure, a 21% increase in central venous pressure, and a 2.5% increase in renal near infrared spectroscopy.
Cluster analysis
Unsupervised cluster analysis demonstrated that the optimal cluster number was 2. The silhouette score for a 2-cluster model as 0.39, demonstrating moderate separation between clusters.
Cluster 1 contained 2 patients. These patients demonstrated a 27.6% increase in heart rate, 10.7% increase in respiratory rate, 5.9% decrease in arterial saturation, 62% increase in mean arterial blood pressure, a 174% increase in central venous pressure and a 54.2% decrease in renal near infrared spectroscopy. Average weight in this cluster was 4.5 kg and 1 patient had a left to right shunt and the other had fully septated biventricular physiology. Neither patient received any opioid, benzodiazepine, or paralytic during the study period.
Cluster 2 contained 43 administrations. These patients demonstrated a 2.3% increase in heart rate, a 5.5% decrease in respiratory rate, a 0.3% increase in arterial saturation, 30.6% increase in mean arterial pressure, a 4.0% increase in central venous pressure, and a 2.6% increase in renal near infrared spectroscopy. Average weight in this cluster was 6.9 kg and all circulatory physiologies were present in this cluster.
Discussion
The findings of this study demonstrate that intravenous ketamine administration is statistically significantly associated with an increase in heart rate, increase in arterial saturation, decrease in respiratory rate, decrease in mean arterial blood pressure, increase in central venous pressure, and an increase in renal near infrared spectroscopy.
While many of these findings are statistically significant, they may not be clinically significant. For instance, even a 21% increase in central venous pressure represents a change from an average central venous pressure of 10 to 12 mmHg in this cohort. The magnitude of change in the other haemodynamic parameters is even less. The statistical methodology utilised combined with the presence of a large amount of data with high temporal resolution leads to analyses that are adequately powered to detect even small changes over the study period.
As the human body and its constituent organs require oxygen, it is important to put the haemodynamic effects of ketamine into the oximetric context. Systemic oxygen delivery is the product of oxygen content and cardiac output. Oxygen content further breaks down into the sum of the bound and dissolved oxygen. Cardiac output is best quantified by the Fick principle, which informs that cardiac output is equal to the oxygen consumption divided by the arteriovenous oxygen content difference. Reference Loomba14,Reference Loomba and Flores15
An increase in arterial saturation after ketamine administration indicates that oxygen content increases while the increase in renal near infrared spectroscopy (surrogate for venous saturation in the Fick principle) indicates that cardiac output also increases, regardless of cardiac lesion or underlying physiology. Cardiac output can be broken into further components of heart rate and stroke volume. Heart rate increased minimally with ketamine administration, implying that stroke volume must have also increased. Because the magnitude of change for all measured parameters is relatively small, the overall increase in systemic oxygen delivery may not be clinically significant. Regardless, what is of most importance is that systemic oxygen delivery does not decrease when ketamine is administered. Reference Loomba14,Reference Loomba and Flores15
Interestingly, 72% of the ketamine administrations were without any opioid or paralytic, meaning that an adequate therapeutic effect likely was achieved with the ketamine alone in order to accomplish the planned procedure or endpoint. The effect of opioid or paralytic was adjusted for in the analyses.
Unsupervised cluster analysis resulted in two clusters with moderate model quality. One cluster was quite small, containing 4.4% of administrations. This cluster demonstrated a large increase in mean arterial pressure, central venous pressure, and a decrease in renal near infrared spectroscopy. These patients were under 5 kg and received no opioid, benzodiazepine. These administrations may represent an exaggerated catecholamine response with increase in arterial and venous resistances. Increase venous resistance can impair venous return and cardiac output as per Guyton’s construct of the venous system. It is important to note that not all patients under 5 kg had this response. Thus, this cluster may be a result of adverse effects of ketamine. The patients in this cluster had fully septated biventricular circulation or a left to right shunt. The remainder of patients were in cluster 2 which seems to represent the more usual physiologic response.
A prior meta-analysis of 139 paediatric patients with congenital heart disease or pulmonary hypertension who received ketamine demonstrated no significant change in pulmonary vascular resistance, systemic vascular resistance, mean arterial blood pressure, cardiac index, heart rate, pH, partial pressure of carbon dioxide, or partial pressure of oxygen. None of the source studies utilised high fidelity data and thus had lower power to detect statistical differences even if present. Nonetheless, differences detected in the parameters-in-common were small, and even if found to be statistically significant were unlikely to be clinically significant. Reference Loomba, Gray and Flores13
Thus, it appears that ketamine at an average dose of 0.8 mg/kg per administration in children with a variety of circulatory physiologies is associated with minimal change in haemodynamic parameters and systemic oxygen delivery while providing adequate anaesthetic effect. These findings are similar to previous published studies. These are important data given the clinical concerns that many still hold with respect to the potentially deleterious effects of ketamine on heart rate and systemic vascular resistance, particularly in those with ventricular dysfunction. Previous data and the current study do not demonstrate significant changes in systemic vascular resistance or haemodynamic collapse.
These data are novel in the sense that previous studies of ketamine’s physiologic effects have not used data with such high temporal resolution. Data was collected at a resolution of 1 Hz, which shows that there could be 3,600 data points per variable during the 60-min study period (30 min before and after administration). This large amount of high-fidelity data allows for amply powered analyses. The time-series analyses utilised here are powered by the number of data points—not the number of patients—as the pre-ketamine data serves as the control data for each patient.
It is important to note that the pre-ketamine data function as the control in these time-series analyses. While a conventional control group is not present, control data is still incorporated for comparative analysis. This methodological approach has been described in the literature and its application in causal inference, with findings that have demonstrated strong correlation to randomised controlled trials(citations). The cohort encompasses a diverse patient population in terms of age, weight, and circulatory physiology with regression analyses performed allowing for assessment of the effect of these many factors.
Although there are strengths to this study, it is not without limitations. Due to the fairly routine weight-based dosing of ketamine at our institution, there was not a wide variety of doses observed, perhaps limiting the ability to discern the precise effect of dosing. Nonetheless, dose effect was not the primary focus of this study. The study also excluded patients who were receiving mechanical circulatory support during ketamine administration, and the results are thus not generalisable to this patient population. It is possible that the increase in central venous pressure is in fact artificial. It is possible that some of the increase in central venous pressure occurs due to the actual infusion of the medication itself. But it seems unlikely that the administration of the medication would lead to a sustained increase in central venous pressure as the ketamine administration takes less than 60 s. Administration of opioids or paralytic would take a similar amount of time. All medication administrations are low volume on a ml/kg basis. Additionally, we did not collect fraction of inspired oxygen. This was done purposely for a few reasons. First, this data is not well charted in acute situations and changes are often uncharted. Second, no patients required unexpected intubation due to the ketamine administration. Thus, it was felt a change in noninvasive fraction of inspired oxygen was unlikely modulating very large changes as there are pragmatic limitations to the augmentation of airway oxygen with noninvasive support modalities. Additionally, while there were no significant adverse events observed related to ketamine that some circulatory physiologies did not have a large number of patients so lesser frequent events may not be captured in the current study. Doses of ketamine can be variable, and larger doses may be used by some and the effects related to such doses may differ.
It should be noted that while the study utilises high fidelity data to characterise the effects of ketamine that the use of ketamine does not require such high fidelity data. This study is not to imply that ketamine can only safely be used when coupled with such high-fidelity physiologic data streaming and aggregation platforms.
Conclusion
The use of intravenous ketamine dosed from 0.5 to 1 mg/kg per dose in the paediatric cardiac intensive care unit appears safe and is associated with minimal haemodynamic change, apnoea, or haemodynamic collapse. This study represents the first data detailing the haemodynamic effects of ketamine captured with a 1-s temporal resolution.







 Open access
Open access