


Introduction
Childhood adversity, including childhood trauma, abuse, and neglect, are established contributors to the risk for the development of mental health disorders, including posttraumatic stress disorder (PTSD; Kessler et al., Reference Kessler, Aguilar-Gaxiola, Alonso, Benjet, Bromet, Cardoso, Degenhardt, De Girolamo, Dinolova, Ferry, Florescu, Gureje, Haro, Huang, Karam, Kawakami, Lee, Lepine, Levinson and Koenen2017). Accumulating evidence suggests that unpredictability in the child’s caregiving and environment can also have long-term consequences for mental health (von Stumm, Reference von Stumm2024; Keen et al., Reference Keen, Chen, Slopen, Sandel, Copeland and Tiemeier2023; Spadoni et al., Reference Spadoni, Vinograd, Cuccurazzu, Torres, Glynn, Davis, Baram, Baker, Nievergelt and Risbrough2022; Aran et al., Reference Aran, Swales, Bailey, Korja, Holmberg, Eskola and Davis2024), independent of other forms of adversity (e.g. abuse, neglect, poverty, Spadoni et al., Reference Spadoni, Vinograd, Cuccurazzu, Torres, Glynn, Davis, Baram, Baker, Nievergelt and Risbrough2022; poverty: Keen et al., Reference Keen, Chen, Slopen, Sandel, Copeland and Tiemeier2023). Unpredictability of parental and environmental signals is characterized by lability of caregiver behavior and mood in addition to a disrupted home environment (e.g. frequent moves, lack of household routine). The notion that unpredictability acts as a potent form of ELA is grounded in various neurodevelopmental theories, including life-history theory (adaptation to developmental context; Ellis, Sheridan, Belsky, & McLaughlin, Reference Ellis, Sheridan, Belsky and McLaughlin2022), attachment theory (emphasizes a consistent and responsive caregiver; Sroufe, Reference Sroufe2005), theories related to household chaos/family routine (Marsh, Dobson, & Maddison, Reference Marsh, Dobson and Maddison2020), learning theory (predictability in sensory input and action consequences; Köster, Kayhan, Langeloh, & Hoehl, Reference Köster, Kayhan, Langeloh and Hoehl2020), as well as biological evidence that inconsistent patterns of caregiver signals can shape neural circuit formation and synaptic connectivity during development (Birnie & Baram, Reference Birnie and Baram2022). In the last decade, unpredictability in early life has emerged as a unique contributor to emotional and cognitive development, leading to a more comprehensive understanding of early-life adversity mechanisms, as well as policy and intervention strategies to mitigate its effects (Glynn, Reference Glynn2025; Baram et al., Reference Baram, Davis, Obenaus, Sandman, Small, Solodkin and Stern2012).
One mechanism through which early-life unpredictability may shape adult psychopathology is via modification of the reward system. In rodents, unpredictable maternal behaviors disrupt reward circuit connectivity and increase anhedonia-like phenotypes, operationalized by lowered reward sensitivity and reduced pleasure-seeking behavior (Birnie et al., Reference Birnie, Short, De Carvalho, Taniguchi, Gunn, Pham, Itoga, Xu, Chen, Mahler, Chen and Baram2023; Bolton et al., Reference Bolton, Molet, Regev, Chen, Rismanchi, Haddad, Yang, Obenaus and Baram2018; Kangas et al., Reference Kangas, Short, Luc, Stern, Baram and Pizzagalli2022; Levis et al., Reference Levis, Birnie, Bolton, Perrone, Montesinos, Baram and Mahler2022). In humans, unpredictability in early life is linked to aberrant connectivity and maturation in circuits related to reward processing and response (Glynn & Baram, Reference Glynn and Baram2019; Short & Baram, Reference Short and Baram2019; Granger et al., Reference Granger, Glynn, Sandman, Small, Obenaus, Keator and Davis2021; Wang et al., Reference Wang, Cao, Zheng, Chen and Zhu2024). Given this extensive cross-species evidence, it is reasonable to suspect that unpredictability in childhood might confer risk for psychiatric symptoms related to the reward function – such as anhedonia. Anhedonia (or hypohedonia) is the reduced capacity to experience pleasure or interest in typically rewarding experiences and often reflects disruptions in the brain’s reward systems (Der-Avakian & Markou, Reference Der-Avakian and Markou2012; Treadway & Zald, Reference Treadway and Zald2011). Rather than a simple absence of positive affect, anhedonia encompasses broader impairments in how rewards are processed, anticipated, and valued – processes that may be particularly sensitive to unpredictable sensory signals from the caregiver and environment (Pizzagalli, Reference Pizzagalli2014; Whitton, Treadway, & Pizzagalli, Reference Whitton, Treadway and Pizzagalli2015). Both cross-sectional and prospective studies have linked anhedonia symptoms in adulthood to childhood unpredictability (Spadoni et al., Reference Spadoni, Vinograd, Cuccurazzu, Torres, Glynn, Davis, Baram, Baker, Nievergelt and Risbrough2022; Null et al., Reference Null, Duda and Pizzagalli2024; Hunt et al., Reference Hunt, Vinograd, Glynn, Davis, Baram, Stern, Nievergelt, Cuccurazzu, Napan, Delmar, Baker and Risbrough2024); however, no prospective studies have shown if increased anhedonia symptoms mediate the contribution of early life unpredictability to adult neuropsychiatric disorders.
Extant hypotheses suggest that PTSD symptoms may partly stem from reduced motivation for reward, in addition to the threat hyperresponsiveness traditionally linked to the disorder. During motivational conflict, reduced reward processing and/or responses could bias behavioral decision-making toward avoidance, even at the risk of loss of reward (Akiki et al., Reference Akiki, Jubeir, Bertrand, Tozzi and Williams2025; Bennett, Davis, & Fitzgerald, Reference Bennett, Davis and Fitzgerald2023). PTSD is consistently associated with reward-system deficits, including disruption in reward processing/circuits and comorbid anhedonia symptoms, with recent evidence suggesting that these deficits contribute to both development and maintenance of PTSD (Risbrough et al., Reference Risbrough, Glynn, Davis, Sandman, Obenaus, Stern, Keator, Yassa, Baram, Baker, Vermetten, Baker and Risbrough2018; Admon et al., Reference Admon, Milad and Hendler2013). Acute reward disruption post-trauma is associated with risk for long-term PTSD (Stevens et al., Reference Stevens, Harnett, Lebois, Van Rooij, Ely, Roeckner and Ressler2021), while intact reward behavior may be a resiliency factor for fear-based disorders like PTSD (Kalisch, Russo, & Müller, Reference Kalisch, Russo and Müller2024). Reward circuit hyporesponsivity and self-reported anhedonia prior to trauma exposure also predict the development and maintenance of PTSD symptoms post-trauma (Acheson et al., Reference Acheson, Vinograd, Nievergelt, Yurgil, Moore, Risbrough and Baker2022; Admon et al., Reference Admon, Milad and Hendler2013). Cross-sectional analyses indicate that anhedonia mediates childhood trauma associations with PTSD (Haim-Nachum et al., Reference Haim-Nachum, Amsalem, Lazarov, Zabag, Neria and Sopp2024), supporting the idea that reward disruption, as measured by anhedonia, may mediate the increased risk for PTSD associated with ELA, including unpredictability. However, no prospective, longitudinal studies have investigated the effect of childhood unpredictability on the development of PTSD symptoms, nor the putative role of anhedonia symptoms as a mediating factor.
This study used a prospective, longitudinal design to test the hypotheses that (1) childhood unpredictability acts as a risk factor for adult PTSD symptoms, and (2) the risk associated with childhood unpredictability is conferred via decreased reward processes as measured by higher anhedonia symptoms. These hypotheses were investigated using longitudinal data on childhood unpredictability, anhedonia symptoms, and PTSD from three distinct cohorts: (1) Adult male service members, (2) adult females, and (3) male and female adolescents. As such, the present study sought to examine a mechanism through which childhood unpredictability might lead to adult PTSD symptoms and determine the extent to which this mechanism is generalizable across development and different populations. We hypothesized that the link between higher unpredictability during childhood and higher PTSD symptoms later in adulthood would be partially mediated by higher anhedonia symptoms earlier in life, and that both the main effect of unpredictability and the mediating effect of anhedonia symptoms would be present in each cohort. Overall, the present study should advance our understanding of early life risk factors for PTSD symptoms later in life.
Method
Participants and procedures
Male service member cohort
The service member cohort consisted of 314 active-duty service members or Veterans who had participated in the Marine Resiliency Study (Baker et al., Reference Baker, Nash, Litz, Geyer, Risbrough and Nievergelt2012), a longitudinal study of Marines and Navy Corpsman assessed prior to and following combat deployment. All study procedures were approved by the VA San Diego Healthcare System and the University of California, San Diego, Institutional Review Boards. Participants provided written informed consent.
Adult female cohort
The cohort of adult females consisted of a community sample of 170 women participating in an ongoing, longitudinal study of maternal and child health recruited from Southern California medical clinics. All study procedures were approved by the responsible Human Subjects Review Board, and participants provided written informed consent.
Adolescent cohort
The adolescent cohort consisted of 137 male and female adolescents from an ongoing longitudinal study of early life influences on child and adolescent development. These adolescents have been followed prospectively from the prenatal period through adolescence (details described in Glynn et al., Reference Glynn, Stern, Howland, Risbrough, Baker, Nievergelt, Baram and Davis2019). All study procedures were approved by the responsible Human Subjects Review Board. Individuals over 18 provided consent for themselves, and mothers provided consent for their children if they were younger than 18; participants younger than 18 also provided assent to participate.
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Measures
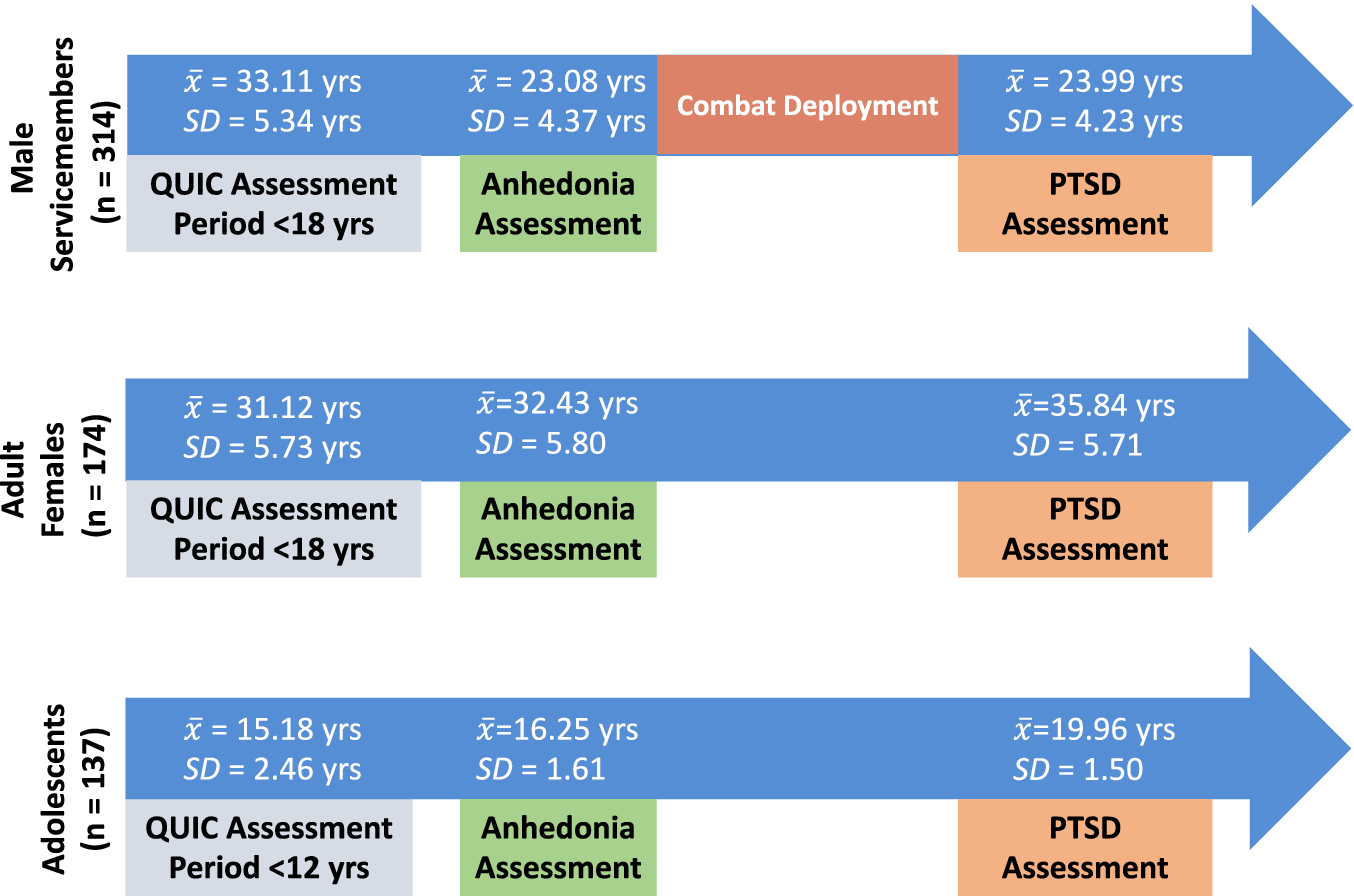
A timeline of childhood unpredictability, anhedonia symptoms, and PTSD assessments for each cohort, including the mean age of administration for each measure in each cohort, can be found in Figure 1. Gender, race, and ethnicity were self-reported by participants.
Timeline of measure administrations across the male service member (top), adult female (middle), and adolescent (bottom) cohorts. The period for the QUIC refers to the time period respondents were asked to consider when answering questions about childhood unpredictability. Anhedonia symptoms and PTSD assessments pertained to current symptoms.
 $ \overline{x} $
and SD refer, respectively, to the mean age and standard deviation of age at the time of administration for each measure, both of which inquired about current symptoms. For the male service member cohort, all anhedonia assessments were given prior to combat deployment, and all PTSD assessments were given following combat deployment. Note: QUIC = Questionnaire of Unpredictability in Childhood.
$ \overline{x} $
and SD refer, respectively, to the mean age and standard deviation of age at the time of administration for each measure, both of which inquired about current symptoms. For the male service member cohort, all anhedonia assessments were given prior to combat deployment, and all PTSD assessments were given following combat deployment. Note: QUIC = Questionnaire of Unpredictability in Childhood.

Childhood unpredictability
Childhood unpredictability was assessed with the Questionnaire of Unpredictability in Childhood (QUIC; Glynn et al., Reference Glynn, Stern, Howland, Risbrough, Baker, Nievergelt, Baram and Davis2019), a 38-item retrospective self-report indexing social, emotional, and physical unpredictability during early life. Example items include ‘I experienced changes in my custody arrangement’ and ‘I usually knew when my parents were going to be home’. Nine items pertained to situations experienced prior to age 12, while 29 pertained to experiences prior to age 18. Higher scores indicated greater unpredictability during childhood. Across the three cohorts, the QUIC demonstrated excellent internal consistency (α ≈ .84–.92) and test–retest reliability (r ≈ .92). Evidence of construct validity includes prospective associations with objectively measured maternal unpredictability in infancy and concurrent associations with self-reported levels of household chaos, inconsistent discipline, and lax parental supervision during adolescence (Glynn et al., Reference Glynn, Stern, Howland, Risbrough, Baker, Nievergelt, Baram and Davis2019). Importantly, the QUIC demonstrates unique associations with mental health symptoms after controlling for other measures of childhood adversity, such as income-to-needs ratio and childhood trauma, suggesting it is a unique dimension of ELA (Glynn et al., Reference Glynn, Stern, Howland, Risbrough, Baker, Nievergelt, Baram and Davis2019). The QUIC is composed of five subscales: Parental Monitoring & Involvement, Parental Predictability, Parental Environment, Physical Environment, and Safety/Security. However, extant data do not support divergent associations with psychiatric symptoms for these subscales, and we had no specific hypotheses about subscales; therefore, only the total QUIC score was analyzed for this study.
Trauma exposure during childhood
The extent of childhood trauma was measured using the life events checklist (LEC; Weathers, Blake et al., Reference Weathers, Blake, Schnurr, Kaloupek, Marx and Keane2013), a self-report inventory cataloging 16 discrete categories of potentially traumatic events (e.g. serious accidents, physical assault, sexual assault) and one ‘other’ category. Respondents indicate whether: (a) the event happened directly to them; (b) they witnessed the event happen to someone else; (c) they learned about the event happening to someone else; (d) it does not apply; or (e) they are not sure. In addition, for each endorsed event, participants indicated the earliest age at which the event occurred. For the adult cohorts, LEC total score was defined as the number of events endorsed as having happened to them or witnessed prior to the age of 18. For the adolescent cohort, LEC total was computed in the same way, but only LEC events that occurred prior to or concurrent with the QUIC were included in the total score to help ensure the trauma was not the result of unpredictability.
Anhedonia
Service member cohort
Anhedonia symptoms in the servicemember cohort were assessed using the Beck Depression Inventory anhedonia item subset (BDI-A). The BDI-A is composed of the three anhedonia-related items taken from the 21-item Beck Depression Inventory II (BDI-II; Beck et al., Reference Beck, Steer and Brown1996), which is a self-report measure of depressive symptoms from the past 2 weeks. The BDI-A items on the BDI-II are: loss of pleasure, loss of interest, and loss of interest in sex. The ability of these three items to validly measure anhedonia symptoms was previously demonstrated in a principal component analysis using the same male service member cohort (see Acheson et al., Reference Acheson, Vinograd, Nievergelt, Yurgil, Moore, Risbrough and Baker2022). Additionally, the BDI-A exhibits evidence of very good internal consistency reliability in this cohort across multiple assessments (α ≈ .74–.84; Hunt et al., Reference Hunt, Vinograd, Glynn, Davis, Baram, Stern, Nievergelt, Cuccurazzu, Napan, Delmar, Baker and Risbrough2024). Higher scores on the BDI-A reflect higher anhedonia symptom severity.
Adult female and adolescent cohorts
Anhedonia symptoms within the adult female and adolescent cohorts were assessed using the mood and anxiety symptom anhedonic-depression questionnaire (MASQ-AD; Clark & Watson, Reference Clark and Watson1991). The MASQ-AD is a 22-item self-report subscale of the MASQ that assesses anhedonic depression symptoms over the past week. The MASQ-AD has demonstrated excellent internal consistency reliability across multiple samples (α ≈ .88–.96; Buckby et al., Reference Buckby, Yung, Cosgrave and Killackey2007; Talkovsky & Norton, Reference Talkovsky and Norton2015) and construct validity as demonstrated by good utility for identifying depressive disorders distinct from anxiety disorders (Buckby et al., Reference Buckby, Yung, Cosgrave and Killackey2007). Factor-analytic studies indicate that the MASQ-AD captures two correlated facets – loss of interest and low positive affect (Naragon-Gainey et al., Reference Naragon-Gainey, Watson and Markon2009) – but given their conceptual overlap and the strong internal consistency of the total scale, we analyzed the composite score as a single indicator of anhedonia symptoms. Higher scores on this subscale indicate higher levels of anhedonia symptoms.
PTSD symptoms
Service member cohort
PTSD symptoms in service members were assessed using the Clinician Administered PTSD Scale for DSM-IV (CAPS-IV; Blake et al., Reference Blake, Weathers, Nagy, Kaloupek, Gusman, Charney and Keane1995). The CAPS-IV is a semi-structured interview assessing the severity and frequency of the 17 diagnostic criteria for PTSD from the DSM-IV. The CAPS-IV yields a current or lifetime PTSD diagnosis and a total PTSD severity score. The CAPS-IV has demonstrated excellent psychometric properties, including excellent convergent validity with other measures of PTSD (Blake et al., Reference Blake, Weathers, Nagy, Kaloupek, Gusman, Charney and Keane1995). A subset of the interviews was independently rerated by a second study clinician. Interrater reliability between interviewers for total CAPS-IV scores was excellent (ICC = 0.99) (Yurgil et al., Reference Yurgil, Barkauskas, Vasterling, Nievergelt, Larson, Schork, Litz, Nash and Baker2014). Of note, CAPS-IV was utilized in the service member cohort because the study predated the release of DSM-5.
Adult female and adolescent cohorts
PTSD symptoms in the adult female and adolescent cohorts were assessed using the PTSD Checklist for DSM-5 (PCL-5; Weathers, et al., Reference Weathers, Blake, Schnurr, Kaloupek, Marx and Keane2013), a 20-item self-report measure of PTSD symptoms that maps directly onto DSM-5 diagnostic criteria for PTSD. The PCL-5 has been shown to possess excellent psychometric properties across multiple populations (Blevins et al., Reference Blevins, Weathers, Davis, Witte and Domino2015), including excellent internal consistency (α ≈ .84–.92) and test–retest reliability (r = .82), as well as strong convergent validity as demonstrated by high positive correlations with PTSD interview measures (e.g. CAPS-5). Higher scores indicate greater severity of PTSD symptoms.
Analytical plan
Main analyses
Within each cohort, Pearson correlations tested associations among the main study variables. Correlations were used to confirm that (a) there was a zero-order relationship between QUIC and PTSD symptoms that mediation might explain and (b) the proposed mediator (anhedonia symptoms) is significantly associated with both the predictor (QUIC) and outcome (PTSD symptoms) variables, as is required by the selected mediation analysis approach (MacKinnon et al., Reference MacKinnon, Lockwood, Hoffman, West and Sheets2002). If correlations were demonstrated, we next ran a hierarchical regression model with PTSD symptoms as the outcome variable, QUIC as a predictor in the first step, and anhedonia symptoms as a predictor in the second step. These models tested if including anhedonia symptoms in the model led to a reduction in the QUIC effect size – evidence of mediation according to our selected approach (MacKinnon et al., Reference MacKinnon, Lockwood, Hoffman, West and Sheets2002). For models that met the above criteria, we then conducted a formal mediation analysis using model four of the SPSS PROCESS Macro (Preacher & Hayes, Reference Preacher and Hayes2004). This model estimates direct and indirect effects using ordinary least squares path analysis. Indirect effects were tested with 10,000 bootstrap resamples to generate bias-corrected 95% confidence intervals (95% CIs), which are considered significant when they do not contain zero. This approach allows for inference about mediation effects without assuming normality of the indirect path distribution.
Sensitivity analyses
We ran three sensitivity analyses to address alternative explanations for study findings. First, we tested if effects of QUIC on PTSD and the mediating effect of anhedonia symptoms were independent of exposure to trauma in childhood. We tested this by including childhood LEC (first step) in a regression model in which QUIC (second step) was entered as a predictor of PTSD symptoms in each cohort and by rerunning the PROCESS mediation model, including childhood LEC as a covariate. Second, we reran all significant mediation models removing PTSD criterion D symptoms (i.e. seven items) from the PTSD total score, given that the content of criterion D overlaps significantly with anhedonia. Thus, this analysis was conducted to ensure that any mediating effect of anhedonia symptoms was not merely driven by symptom overlap with PTSD. Finally, for the service member cohort only, we reran the mediation controlling for PTSD symptoms at pre-deployment to verify that the mediating effect of anhedonia symptoms was not driven by pre-existing PTSD symptoms. Since PTSD symptoms were assessed at only one timepoint in the other two cohorts, this follow-up analysis could not be performed in those cohorts.
All analyses were conducted in SPSS version 28. Alpha was set at .05 (two-tailed) for all applicable tests.
Results
Sample characteristics
Demographic and clinical characteristics of each cohort can be found in Table 1.
Demographic and clinical characteristics of the study samples

Note: Ranges refer to the range of possible values for the measure. Childhood LEC refers only to traumatic events that were directly experienced or witnessed during childhood; for the adolescent cohort, childhood LEC events were only those that were concurrent with or prior to the QUIC. QUIC = Questionnaire of Unpredictability in Childhood; LEC = Life events checklist; BDI-A = Beck Depression Inventory Anhedonia Items; MASQ-AD = Mood and anxiety symptom questionnaire anhedonic-depression subscale; CAPS-IV = Clinician Administered PTSD Scale for DSM-IV; PCL-5 = PTSD Checklist for DSM-5.
Associations between primary study variables
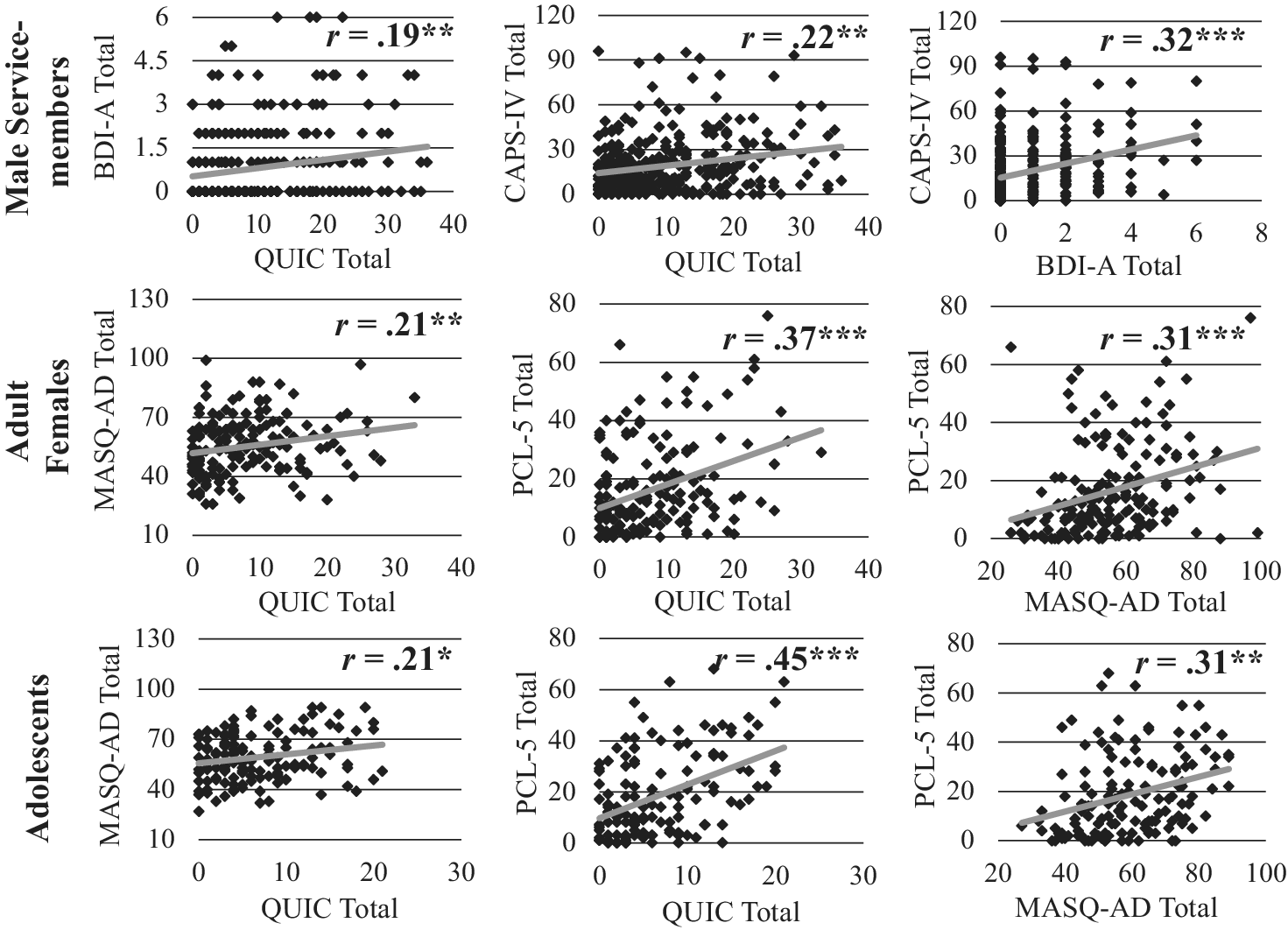
Scatterplots of Pearson correlations between childhood unpredictability, PTSD symptoms, and anhedonia symptoms for each cohort are shown in Figure 2. Significant positive associations were observed for each of the three pairs of variables across all three cohorts (rs > .19, ps < .016).
Scatterplots of associations between childhood unpredictability and anhedonia symptoms (left), childhood unpredictability and PTSD symptoms (middle), and anhedonia symptoms and PTSD symptoms (right) across cohorts of service members (top), adult females (middle), and adolescents (bottom). Note: QUIC = Questionnaire of Unpredictability in Childhood; BDI-A = Beck Depression Inventory Anhedonia Items; MASQ-AD = Mood and anxiety symptom questionnaire anhedonia subscale; CAPS-IV = Clinician Administered PTSD Scale for DSM-IV; PCL-5 = PTSD Checklist for DSM-5. ***p < .001; **p < .01; *p < .05.

Testing anhedonia symptoms as a mediator of the longitudinal relationship between childhood unpredictability and PTSD symptoms
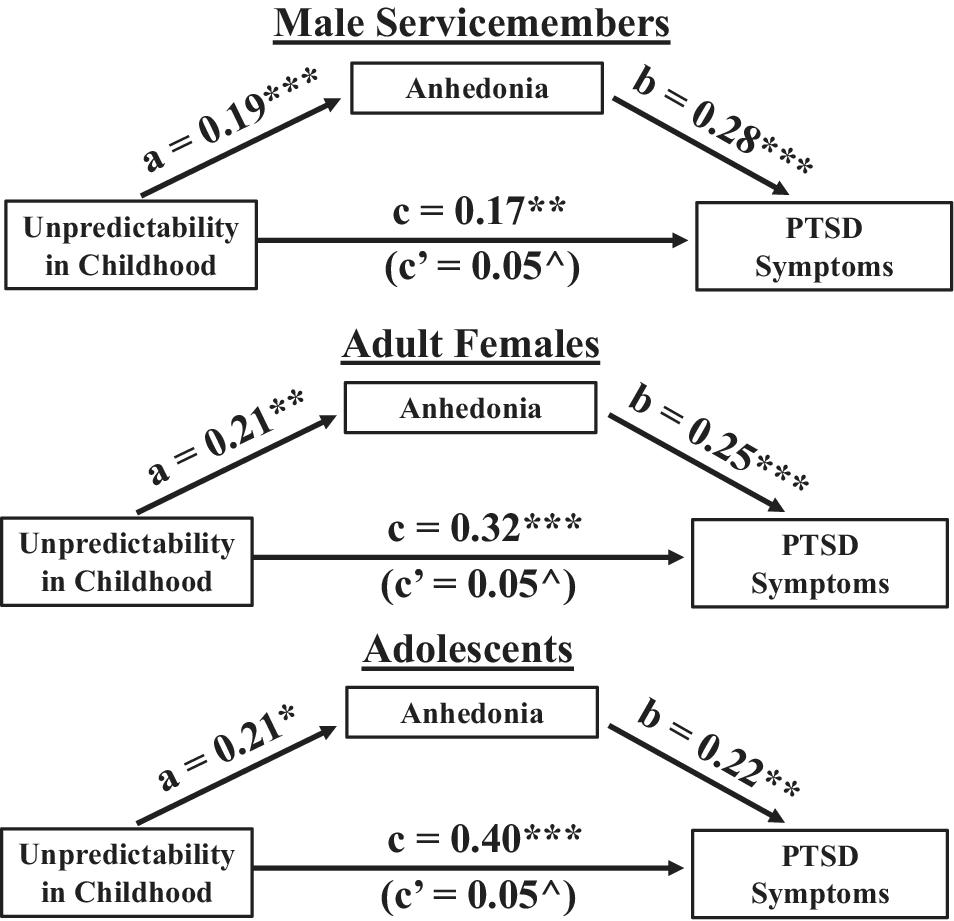
Mediational analyses revealed an indirect effect of childhood unpredictability on PTSD symptoms via higher anhedonia symptoms, which was significant in the male service member cohort (b = 0.055, 95% CI [0.02, 0.11]), the adult female cohort (b = 0.052, 95% CI [0.01, 0.13]), and the adolescent cohort (b = 0.046, 95% CI [0.01, 0.12]). Thus, in each cohort, a significant portion of the effect of childhood unpredictability on later PTSD symptoms was accounted for by higher anhedonia symptoms prior to the PTSD assessment. An illustration of the direct and indirect paths from unpredictability to PTSD symptoms for each cohort can be found in Figure 3.
Mediation models depicting the effect of childhood unpredictability on later PTSD symptoms as mediated by anhedonia symptoms in service members (top), adult females (middle), and adolescents (bottom). Anhedonia symptoms were measured using the BDI-A for the service member cohort and using the MASQ-AD in the adult female and adolescent cohorts. PTSD symptoms were measured with the CAPS-IV in the service member cohort and with the PCL-5 in the adult females and adolescent cohorts. Unpredictability in childhood was measured with the QUIC for all three cohorts. C (direct effect) is the effect of childhood unpredictability on later PTSD symptoms not mediated by anhedonia symptoms, while c’ (indirect effect) is the effect of childhood unpredictability on later PTSD that is mediated by anhedonia symptoms. Note: QUIC = Questionnaire of Unpredictability in Childhood; BDI-A = Beck Depression Inventory Anhedonia Items; MASQ-AD = Mood and anxiety symptom questionnaire anhedonia subscale; CAPS-IV = Clinician Administered PTSD Scale for DSM-IV; PCL-5 = PTSD Checklist for DSM-5. ^bootstrapped 95% confidence interval does not contain zero; *p < .05; **p < .01; ***p < .001.

Sensitivity analyses
Consideration of childhood trauma
Results of regression models used to predict adult PTSD symptoms from QUIC and childhood LEC are shown in Table 2. In each cohort, higher childhood trauma was predictive of greater PTSD symptoms in adulthood (ps < .041). Critically, higher QUIC scores predicted higher PTSD symptoms even after covarying the effects of childhood trauma (ps < .001). After adjusting for childhood trauma, the indirect effect of QUIC on PTSD symptoms as mediated by anhedonia symptoms also remained significant in the male service member cohort (b = 0.052, 95% CI [0.020, 0.10]), the adult female cohort (b = 0.046, 95% CI = [0.007, 0.12]), and the adolescent cohort (b = 0.048, 95% CI [0.005, 0.12]). Thus, the relationship between childhood unpredictability and adult PTSD, as well as the mediating effect of anhedonia symptoms on this relationship, appeared to be unique from the effects of childhood trauma.
Hierarchical regression models of childhood unpredictability predicting adult PTSD symptoms, controlling for childhood trauma

Note: Childhood LEC was defined as the number of traumatic events endorsed as having directly experienced or witnessed prior to age 18 for the adult cohorts and as the number having directly experienced or witnessed concurrent with or prior to the age of QUIC administration for the adolescent cohort. QUIC = Questionnaire of Unpredictability in Childhood; LEC = Life events checklist; CAPS-IV = Clinician Administered PTSD Scale for DSM-IV; PCL-5 = PTSD Checklist for DSM-5.
Removing anhedonia-related symptoms from PTSD assessments
Removing anhedonia-related items from the PTSD symptom score did not alter the mediating effect of anhedonia symptoms, as its indirect effect remained significant in the male service member cohort (b = 0.047, 95% CI = [0.02, 0.10]), the adult female cohort (b = 0.055, 95% CI [0.01, 0.14]), and the adolescent cohort (b = 0.04, 95% CI [0.002, 0.09]). Thus, the mediating effect of anhedonia symptoms on the relationship between childhood unpredictability and PTSD symptoms did not appear to be driven by overlap with anhedonia-related content in PTSD assessment instruments.
Pre-deployment PTSD symptoms
Finally, within the male servicemember cohort, we reran the original mediation model including pre-deployment PTSD symptoms as a covariate. The indirect effect of QUIC via anhedonia symptoms remained significant, b = 0.019, 95% CI [0.0025, 0.048], suggesting that it was not an artifact of pre-existing PTSD symptoms.
Discussion
The present study tested two hypotheses: (1) that childhood unpredictability acts as a risk factor for adult PTSD symptoms, and (2) that childhood unpredictability confers risk for adult PTSD in part via increased anhedonia symptoms. Overall, our findings were consistent with both hypotheses: Higher childhood unpredictability predicted greater adult PTSD symptoms across three different participant cohorts (male service members, adult females, and adolescents), and the effect of childhood unpredictability on adult PTSD was partially mediated by higher anhedonia symptoms in each cohort. Critically, the mediating effect of anhedonia symptoms remained significant in each cohort when covarying levels of childhood trauma and removing anhedonia-related symptoms from the PTSD outcome. Effects also remained significant in the male servicemember cohort when controlling for pre-deployment PTSD symptoms.
That childhood unpredictability predicted higher adult PTSD symptoms across three distinct longitudinal cohorts provides the strongest evidence to date that childhood unpredictability may act as a risk factor for adult PTSD. Although this association had been previously demonstrated in a cross-sectional investigation of Veterans (Spadoni et al., Reference Spadoni, Vinograd, Cuccurazzu, Torres, Glynn, Davis, Baram, Baker, Nievergelt and Risbrough2022), our study is the first to demonstrate a longitudinal association between childhood unpredictability and later PTSD, which provides more stringent evidence that a variable acts as a risk factor (Kraemer, Reference Kraemer1997). Additionally, the fact that childhood trauma and childhood unpredictability each predicted significant, unique variance in adult PTSD symptoms helps broaden our understanding of the relationship between ELA and adult PTSD risk by demonstrating that such risk may not only be amplified by the experience of severe negative events during childhood (Breslau et al., Reference Breslau, Koenen, Luo, Agnew-Blais, Swanson, Houts, Poulton and Moffitt2014) but also by the degree to which parental interactions and the household environment in childhood are unpredictable.
Although our study cannot speak definitively as to how childhood unpredictability confers risk for adult PTSD, our mediation findings suggest that it may partly stem from the disruption of reward processes earlier in life. A variety of studies have demonstrated that unpredictability early in life can disrupt maturation of reward and stress systems (Baram et al., Reference Baram, Davis, Obenaus, Sandman, Small, Solodkin and Stern2012; Davis et al., Reference Davis, McCormack, Arora, Sharpe, Short, Bachevalier, Glynn, Sandman, Stern, Sanchez and Baram2022; Davis et al., Reference Davis, Stout, Molet, Vegetabile, Glynn, Sandman, Heins, Stern and Baram2017; Granger et al., Reference Granger, Glynn, Sandman, Small, Obenaus, Keator and Davis2021). For instance, early life unpredictability in animals has been shown to reduce reward-seeking behavior in adulthood due, in part to the disruption of ventral striatum circuits that affect reward sensitivity, reward processing, and the motivational conflict between reward and threat (Levis et al., Reference Levis, Birnie, Bolton, Perrone, Montesinos, Baram and Mahler2022; Birnie et al., Reference Birnie, Kooiker, Short, Bolton, Chen and Baram2020; Bolton et al., Reference Bolton, Molet, Regev, Chen, Rismanchi, Haddad, Yang, Obenaus and Baram2018). Although they cannot directly interrogate the health of these circuits, self-reported anhedonia symptoms are consistent with the existence of disrupted reward processing, suggesting that the relationship between childhood unpredictability and anhedonia symptoms in our study may have derived from a similar mechanism. Importantly, disruptions in the ventral striatum and its associated reward circuitry have also been implicated in PTSD (for reviews, see Vinograd, Stout, & Risbrough, Reference Vinograd, Stout, Risbrough and Pizzagalli2022; Lokshina, Nickelsen, & Liberzon, Reference Lokshina, Nickelsen and Liberzon2021; Jia et al., Reference Jia, Ruderman, Pietrzak, Gordon, Ehrlich, Horvath and Levy2023), and anhedonia symptoms have been shown to increase risk for the development of subsequent PTSD (Acheson et al., Reference Acheson, Vinograd, Nievergelt, Yurgil, Moore, Risbrough and Baker2022). Taken together, these pieces of evidence are consistent with the hypothesis that early life unpredictability leads to increased anhedonia symptoms, which in turn confer risk for PTSD. Importantly, while there appears to be a particularly strong link between disrupted reward processing and anhedonia-related PTSD symptoms (Jia et al., Reference Jia, Ruderman, Pietrzak, Gordon, Ehrlich, Horvath and Levy2023; Lokshina et al., Reference Lokshina, Nickelsen and Liberzon2021; Vinograd et al., Reference Vinograd, Stout, Risbrough and Pizzagalli2022), the mediating effect of anhedonia symptoms in our study was unchanged when anhedonia-related content was removed from our PTSD assessments. Hence, the anhedonia-mediated effect of childhood unpredictability on PTSD cannot be explained as symptomatic overlap between PTSD and anhedonia, suggesting that it reflects a unique pathway that confers disruption in non-anhedonia-related PTSD symptoms.
The present study is not without limitations. First, only one cohort (male service members, N=317) included an earlier PTSD assessment that was concurrent with the anhedonia symptom assessment, which allowed us to test whether subsequent PTSD symptoms truly developed after anhedonia symptoms or were merely assessed after them. Second, the QUIC was administered close to a decade after childhood in the adult cohorts, rendering these participants susceptible to retrospective recall biases that could affect the validity of their scores. However, the fact that the QUIC was nonetheless associated with anhedonia symptoms that were assessed 10 years prior to the QUIC assessment suggests that its relations with anhedonia symptoms cannot be explained by state-dependent recall biases. Third, although we utilized self-reported anhedonia symptoms to make inferences about reward system functioning, the reward system is multifaceted, so its health can be interrogated in a variety of ways. For instance, behavioral paradigms that measure reinforcement learning and effort-based decision-making could index other aspects of the reward system that may be just as strong, if not stronger, mediators of the relationship between childhood unpredictability and PTSD. Finally, we did not test whether the pathway from childhood unpredictability through anhedonia symptoms might confer risk for other mental health issues besides PTSD. Indeed, cross-sectional data indicate that childhood unpredictability is also associated with greater anxiety disorder symptoms in adults and adolescents (Glynn et al., Reference Glynn, Stern, Howland, Risbrough, Baker, Nievergelt, Baram and Davis2019; Spadoni et al., Reference Spadoni, Vinograd, Cuccurazzu, Torres, Glynn, Davis, Baram, Baker, Nievergelt and Risbrough2022), suggesting that a similar risk pathway may be at play for anxiety-related issues.
This study also possesses several notable strengths. Chief among these is the reliability of our findings despite methodological, demographic, and developmental differences across cohorts. In particular, the effect of childhood unpredictability on PTSD and the mediating effect of anhedonia symptoms on this relationship were very similar across cohorts despite utilizing different instruments to assess PTSD (i.e. PCL-5 versus CAPS-IV) and anhedonia symptoms (i.e. MASQ-AD versus BDI-A) and adhering to different assessment schedules (e.g. QUIC administered a few years before anhedonia/PTSD in adolescent and adult female cohorts versus 10 years after in the male servicemember cohort). Relatedly, the consistency of our findings across different populations not only provides further assurance that the relations between childhood unpredictability, anhedonia symptoms, and PTSD are real, but also that they are generalizable to people of different backgrounds (e.g. adolescents versus adults, males versus females, civilians versus service members, etc.).
Clinically, our findings imply that risk for PTSD could be partially mitigated through two distinct strategies: (1) restoring reward system functioning during adolescence or (2) making childhood more structured and predictable. Although both strategies could be effective, the latter approach may be preferable for several reasons. First, fostering more consistent routines and stable caregiving environments could support the normative maturation of reward circuitry, thereby addressing the proximal vulnerability for PTSD implicated in our findings. Indeed, engagement in structured caregiving practices (e.g. structured meal or bedtime routines, regular play or family time) has been found to buffer against the development of depressive symptoms in preschool children (Glynn et al., Reference Glynn, Davis, Luby, Baram and Sandman2021; Davis & Glynn, Reference Davis and Glynn2024), consistent with animal models where predictable maternal care promoted healthy reward system development (Birnie et al., Reference Birnie, Short, De Carvalho, Taniguchi, Gunn, Pham, Itoga, Xu, Chen, Mahler, Chen and Baram2023; Bolton et al., Reference Bolton, Molet, Regev, Chen, Rismanchi, Haddad, Yang, Obenaus and Baram2018; Kangas et al., Reference Kangas, Short, Luc, Stern, Baram and Pizzagalli2022; Levis et al., Reference Levis, Birnie, Bolton, Perrone, Montesinos, Baram and Mahler2022). Second, making childhood more structured would also buffer against additional risk pathways that originate with childhood unpredictability, beyond that which occurs via reward system disruption. Such an assertion is consistent with our observation that anhedonia symptoms only partially mediated the relationship between childhood unpredictability and PTSD risk. Finally, promoting structure and predictability in daily routines represents a low-cost, non-invasive strategy that can be implemented within families or caregiving settings, especially when caregivers are provided with appropriate guidance and support. To this end, building awareness of the detrimental nature of childhood unpredictability among key stakeholders (e.g. parents, physicians) represents perhaps the most direct method for reducing its effects. Indeed, efforts are already underway to begin screening for unpredictable caregiving practices in pediatric settings so that caregivers are better equipped to guard against such practices in their daily lives (Glynn, Reference Glynn2025).
In conclusion, the present study found childhood unpredictability to be associated with greater adult PTSD symptoms and that this relationship is partially explained by higher anhedonia symptoms earlier in life. These findings implicate childhood unpredictability as a novel risk factor for adult PTSD and suggest that such risk may be conferred in part through the development of disrupted reward processes, which are consistent with the presence of higher anhedonia symptoms. Our results imply that risk for PTSD could be partially mitigated through making childhood more structured and predictable and possibly through interventions to enhance positive affect and reward processing in late adolescence/early adulthood (Davis & Glynn, Reference Davis and Glynn2024; Glynn et al., 2024). Future studies should more carefully track changes in childhood unpredictability, trauma, anhedonia symptoms, PTSD, and other variables over time and incorporate objective biological measures of stress reactivity and reward processing. Such work will help more firmly establish the mechanism through which childhood unpredictability confers risk for PTSD and allow us to develop more targeted interventions to reduce risk for PTSD.
Funding statement
Support for this work includes NIMH P50MH096889 (LMG, EPD, TZB, DGB, VBR), CSR&D VA Career Development Award IK2CX002640 (CH), VA Research Career Scientist Award (VBR), and the Center of Excellence for Stress and Mental Health (CH, CN, VBR).




 Open access
Open access