


Anorexia nervosa is a debilitating eating disorder characterised by (a) severe restriction of energy intake resulting in significantly low body weight; (b) an extreme fear of weight gain; and (c) disturbances in the experience of the body and shape, overemphasis of these in self-evaluation or denial of the seriousness of the condition. 1 Talking therapies are currently implemented as first-line treatments. Despite the use of antidepressants and atypical antipsychotics to manage comorbid psychiatric symptoms, Reference Himmerich, Kan, Au and Treasure2 there are currently no pharmacological interventions approved for anorexia nervosa. Success rates of existing treatments remain low, with approximately 20–30% of those diagnosed developing chronic and enduring anorexia nervosa. Reference Eddy, Tabri, Thomas, Murray, Keshaviah and Hastings3 Anorexia nervosa has one of the highest mortality rates of all psychiatric conditions. Reference Arcelus, Mitchell, Wales and Nielsen4 Distinct from other psychiatric conditions, anorexia nervosa often becomes a part of a person’s identity (egosyntonic) and is regarded positively by the individual. Reference Gregertsen, Mandy and Serpell5 This results in resistance to conventional treatment, where greater anorexia nervosa severity is associated with lower readiness and motivation to change. Reference Geller, Brown, Zaitsoff, Menna, Bates and Dunn6 Indeed, pre-treatment motivation is a predictor of positive treatment outcomes. Reference Sansfaçon, Booij, Gauvin, Fletcher, Islam and Israël7
In the past decade, the safety and possible efficacy of psilocybin (the serotonin 2A receptor agonist found in ‘magic mushrooms’) alongside psychological support has been investigated as a novel treatment avenue for a range of psychiatric disorders. Reference Nutt and Carhart-Harris8 Naturalistic data indicated that psilocybin, alongside other serotonergic psychedelics, may be beneficial in the treatment of eating disorders, with reports of improvements in comorbid depressive symptoms and psychological well-being, as well as insight into the origin of the eating disorder. Reference Lafrance, Loizaga-Velder, Fletcher, Renelli, Files and Tupper9–Reference Spriggs, Kettner and Carhart-Harris11 An open-label feasibility study assessing high-dose psilocybin in ten participants with anorexia nervosa reported successful participant recruitment and retention, and improvements in shape and weight concerns at 1 month post-dosing. Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 Two clinically noteworthy cases of post-psilocybin hypoglycaemia were documented; however, the overall safety profile was positive. The current study further investigated the feasibility, safety and potential efficacy of psilocybin therapy in adult females with anorexia nervosa. Feasibility was assessed through recruitment, retention and adherence rates, whereas safety and tolerability were evaluated by monitoring adverse events and body mass index (BMI) over the study period. Anorexia nervosa psychopathology and motivation to change were also assessed at key time points to establish an initial impression of efficacy. We hypothesised that psilocybin treatment would be feasible and well tolerated, with potential to reduce clinical severity in this population.
Method
Study design and approvals
This was a single-arm, single-blind, within-individual, fixed-order pilot study investigating psilocybin therapy as a treatment for adult females with anorexia nervosa, adjunctive to treatment as usual. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human patients were approved by the Brent National Research Ethics Services (reference: 20/LO/0474) and the Medicines and Healthcare Products Regulatory Agency (reference: CTA 19174/0418/001-0001). It was sponsored by the Imperial Research Governance and Integrity Team. The National Institute for Health and Care Research Trust Imperial Clinical Research Facility (ICRF) provided site-specific approval and independent monitoring. Written informed consent was obtained from all individuals. The trial was registered with ISRCTN (ISRCTN10441504), ClinicalTrials.gov (NCT04505189) and EudraCT (2019-004054-28).
Participants
Eligible participants were females (assigned at birth) aged 21–65 years, with a primary DSM-5 diagnosis of anorexia nervosa that had likely been present for over 3 years. Participants were required to be registered with a UK-based specialist eating disorder care team and must not have achieved remission despite prior treatments. Exclusion criteria included a history of psychotic disorders, unstable medical or psychiatric conditions, contraindications to magnetic resonance imaging or electroencephalography and substance dependence within 6 months. Each participant was asked to identify a support person (e.g. family member, close friend) for external support.
Participants were recruited through two National Health Service (NHS) specialist eating disorder services and an online self-referral form, which was advertised on social media and through two charity websites: BEAT (the UK eating disorder charity) and MQ Mental Health Research. The recruitment target was 20 ‘study completers’, defined as completion of all requirements of the study up to and including the 6-week final in-person visit.
Screening process
Potentially eligible participants were sent the full participant information sheet. After obtaining initial written informed consent from all participants, remote screening consisted of two video calls with a study psychiatrist and therapist. Eligible participants then attended an in-person screening visit at the ICRF, where full written informed consent was obtained from all participants, and a comprehensive psychiatric and physical health assessment was conducted. Participants’ general practitioners (GPs) and specialist eating disorder teams subsequently confirmed suitability and verified prescriptions. Withdrawal from relevant medications (i.e. antidepressants) was overseen by study psychiatrists in consultation with the participants’ GPs and eating disorder teams. Participants discontinued selective serotonin reuptake inhibitors (SSRIs) to avoid blunting the psychedelic experience. Reference Bonson13,Reference Gukasyan, Griffiths, Yaden, Antoine and Nayak14
See the Supplementary Methods available at https://doi.org/10.1192/bjp.2026.10687 for the full eligibility criteria, details of support person involvement and screening procedures.
COMP360 psilocybin
The investigational drug COMP360 is a proprietary, pharmaceutical-grade, synthetic psilocybin formulation, optimised for stability and purity, developed by COMPASS Pathfinder Ltd, UK. It was formulated into the investigational medicinal product and delivered by ThermoFisher Scientific, USA. A licence covering the storage and dispensing of the Schedule One psilocybin was granted by the UK Home Office.
Procedure
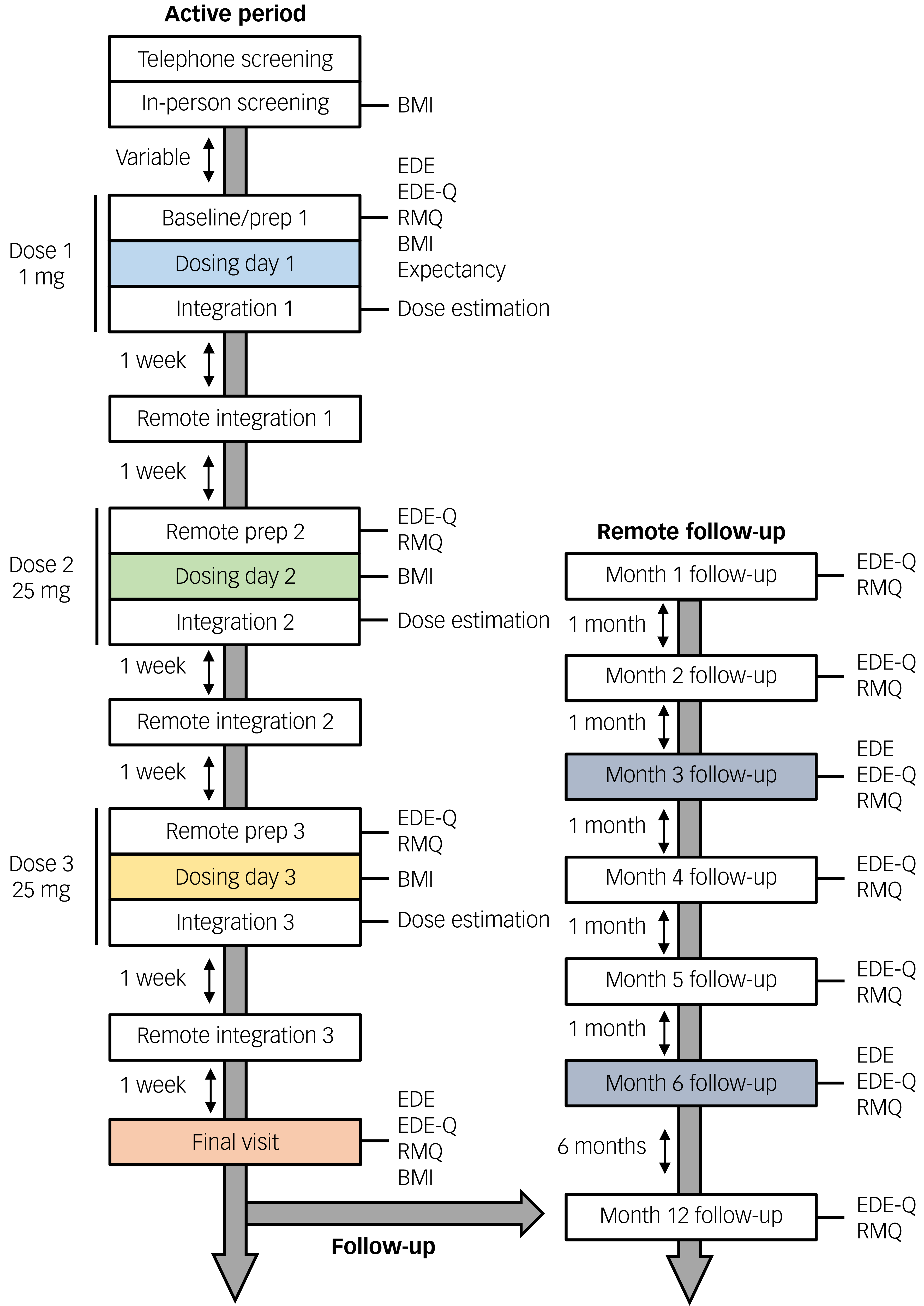
This single-blind study consisted of three fixed-order psilocybin dosing sessions (1 mg, 25 mg, 25 mg) over a 6-week period, each separated by 2 weeks. There were remote monthly follow-up visits for the first 6 months and a final remote 12-month follow-up (Fig. 1). Participants were informed that they would receive psilocybin at each dosing visit and that the maximum dose they would receive would be 25 mg; they were not aware of the order of doses or the strength of the two remaining doses. Each dosing day was preceded by a preparation session one day prior and followed by an integration session the next day. The baseline visit occurred one day before the first dosing session and entailed the dose 1 preparation session. The final visit took place 2 weeks after the final dosing session. Participants continued to receive treatment as usual from their NHS eating disorder service and/or private therapist throughout the study.
The timeline of the Panorexia study. Time points at which data were collected are indicated. BMI, body mass index; EDE, Eating Disorder Examination Interview; EDE-Q, EDE Questionnaire; RMQ, Readiness and Motivation Questionnaire.

Fig. 1 Long description
The flowchart illustrates the timeline of the Panorexia study, detailing the sequence of data collection points and activities. The process began with the Active Period, which included Telephone Screening and In-Person Screening, followed by the calculation of Body Mass Index (BMI). The Baseline/Prep 1 phase involved assessments using the Eating Disorder Examination (EDE), Eating Disorder Examination Questionnaire (EDE-Q), Readiness and Motivation Questionnaire (RMQ), and BMI. Dose 1 of 1 milligram of psilocybin was administered on Dosing Day 1, followed by Integration 1 and Dose Estimation. After a one-week interval, Remote Integration 1 was conducted. This process repeated with Remote Prep 2, Dosing Day 2 for Dose 2 of 25 milligrams of psilocybin, Integration 2, and another Dose Estimation. Following another one-week interval, Remote Integration 2 was performed. The cycle continued with Remote Prep 3, Dosing Day 3 for Dose 3 of 25 milligrams of psilocybin, Integration 3, and another Dose Estimation. After a final one-week interval, Remote Integration 3 was conducted. The Active Period concluded with the Final Visit, which included assessments using EDE, EDE-Q, RMQ, and BMI. The Remote Follow-Up period began with Month 1 Follow-Up, involving EDE-Q and RMQ assessments, followed by similar assessments at Month 2, Month 3, Month 4, Month 5, and Month 6 Follow-Up. The final follow-up occured at Month 12, involving EDE, EDE-Q, and RMQ assessments.
Therapists provided support integrating emotion-focused family therapy, Reference Robinson, Dolhanty and Greenberg15 compassion-focused therapy Reference Gilbert16 and systemic therapy, informed by their specialised clinical experience.
For a comprehensive overview of the study visits and assessments, please refer to Spriggs et al Reference Spriggs, Douglass, Park, Read, Danby and de Magalhães17 and the Supplementary Methods.
Primary outcomes
Feasibility
Recruitment was assessed via retention at each stage of the screening process. Demographic information and reasons for exclusion were collected throughout the screening process. The retention rate was calculated as the percentage of enrolled participants who completed the active study period from baseline to the final visit.
Safety and tolerability
Adverse events were monitored up to the remote 12-month follow-up, assessed using the probing question ‘Have you experienced any change in your health since your last visit?’, in addition to unprompted self-report by participants. BMI was not a pre-registered outcome of the study, but was monitored as part of safety procedures at the baseline visit, dose 2, dose 3 and the final visit (Supplementary Section 2.5.5).
Clinical efficacy outcomes
The two primary outcomes were (a) the global output of the EDE Interview Reference Fairburn, Cooper and O’Connor18 and (b) the precontemplation output of the RMQ. Reference Geller, Brown, Srikameswaran, Piper and Dunn19 These were utilised to measure clinician-assessed severity of eating disorder symptoms and a self-reported index of motivation to change in relation to the eating disorder, respectively. The EDE Questionnaire (EDE-Q) Reference Fairburn, Cooper and O’Connor20 was a key secondary outcome and documented self-reported severity of eating disorder symptoms. To account for temporal variation in recovery from anorexia nervosa, the primary EDE end-points were the final visit, the 3-month follow-up and the 6-month follow-up; and for the RMQ, the primary end-point was the final visit. Comparison of RMQ precontemplation and global EDE-Q scores between dosing days were primary and key secondary outcomes, respectively.
Statistical analysis
Data were cleaned in Microsoft Excel and analysed in RStudio for MacOS (version 2024.12.1+563, Posit PBC, Boston, Massachusetts, US; https://rstudio.com/). One participant withdrew from the study following completion of dose 2 (first 25 mg); therefore, an intention-to-treat analysis was conducted with the last observation carried forward. This method was also implemented for missing data points.
Clinical efficacy data were entered into individual linear mixed-effect models (LMMs) to assess change over time from baseline while controlling for baseline scores, with main effect analysis of variance (ANOVA) and post hoc pairwise comparisons incorporated. Additional LMMs were conducted with concomitant antidepressant medication withdrawal included as a fixed effect, with data omitted from one participant who remained on 2.5 mg citalopram.
To assess the effect of individual doses on these outcome measures, the incremental change in global EDE-Q and RMQ precontemplation scores between doses was calculated, with the difference in raw and percentage change between doses assessed using a repeated-measures ANOVA. A p-value of <0.05 was considered statistically significant. Paired Cohen’s d effect sizes were calculated. No controls for multiple comparisons were implemented because of the exploratory nature of this pilot study. Descriptive statistics of outcome measures are available in the Supplementary Results.
Results
Recruitment and retention
Between April 2021 and April 2023, there were approximately 450 expressions of interest. Of these, 161 individuals were considered potentially eligible (the remainder were identified as immediately ineligible) and were sent the full participant information sheet; 100 attended telephone screening, 26 attended in-person screening and 21 individuals were enrolled in the study. A consort diagram (Supplementary Fig. S1) details this screening and recruitment process, and the reasons for exclusion.
The participant retention rate was 95.2%, with the recruitment target of 20 completers fulfilled. One participant withdrew following dose 2 (first 25 mg), because of the time and emotional obligations of the study.
Participant demographics
See Supplementary Tables S5 and S6 for summary and detailed demographic information of enrolled participants (n = 21). In summary, participants were aged between 23 and 52 years (mean 32; s.d. 7.1), had a BMI of between 14.3 and 20.5 kg/m2 (mean 16.4; s.d. 1.4), had an estimated illness duration of between 4 and 22 years (mean 10.8; s.d. 5.0) and had baseline EDE scores of between 1.3 and 5.7 (mean 3.2; s.d. 1.0). Sixteen of the enrolled participants were White British (76.2%), 14 had no religious orientation (66.7%), 17 were employed (81.0%) and 11 had a postgraduate degree or higher (55.4%). Eleven participants were reported to have psychiatric comorbidities (assessed by the Mini-International Neuropsychiatric Interview Reference Sheehan, Lecrubier, Sheehan, Amorim, Janavs and Weiller21 ), with generalised anxiety disorder (n = 7, 33.3%) and major depressive disorder (n = 5, 23.8%) being the most common. A total of 85.7% of participants reported never using psilocybin, with the other three reporting psilocybin use only once in their lives. Ten (47.6%) of the enrolled participants were withdrawn from contraindicated medication (e.g. SSRIs).
Safety and tolerability
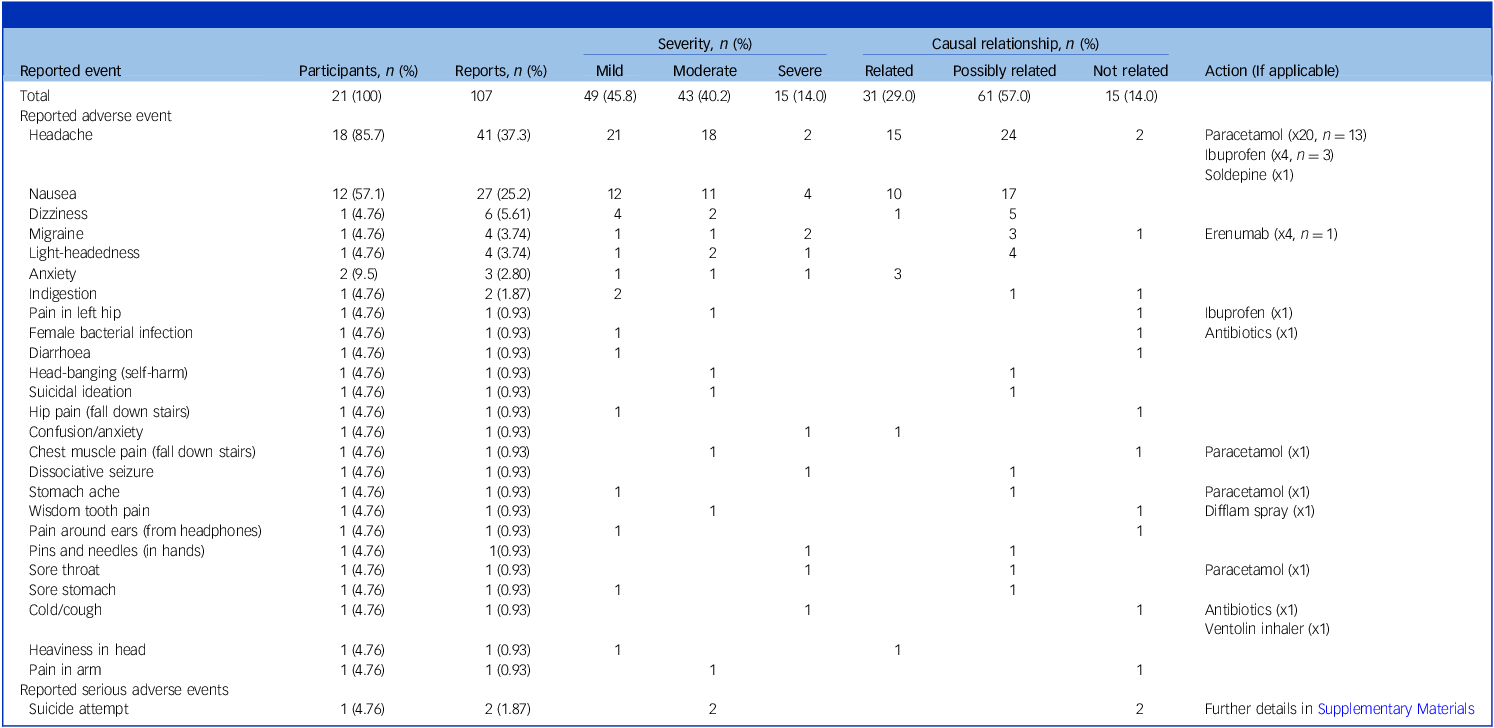
Psilocybin was well tolerated (Table 1). All participants reported at least one adverse event, with 107 reported in total. The majority of the reported adverse events were classified as mild (45.8%) or moderate (40.2%), and ‘possibly related’ to the pharmacological intervention (57.0%). The most common adverse events were transient headaches (37.3%) and nausea (25.2%). The administration of tranquillising medication (lorazepam) was not required for any participant.
Summary of adverse events and serious adverse events reported over the study period, including 12-month follow-up

Table 1 Long description
The table presents a summary of adverse events and serious adverse events reported during a study period, including a 12-month follow-up. It includes data on the number of participants and reports, severity levels, causal relationships, and actions taken. The table has 21 rows and 8 columns, with headers such as Reported adverse event, Participants, Reports, Severity, Causal relationship, and Action. Notable adverse events include headache, nausea, dizziness, and migraine, with varying severity and causal relationships. Actions taken include the administration of medications like paracetamol, ibuprofen, and soldipine.
One participant attempted to end their life on two occasions, approximately 7 and 9 months after the final study visit. These events were reported as serious adverse events (SAEs), and were deemed to be of moderate severity and unlikely to be related to the investigational medicinal product (psilocybin). See Supplementary Section 2.4.1 for further details of these events.
EDE interview
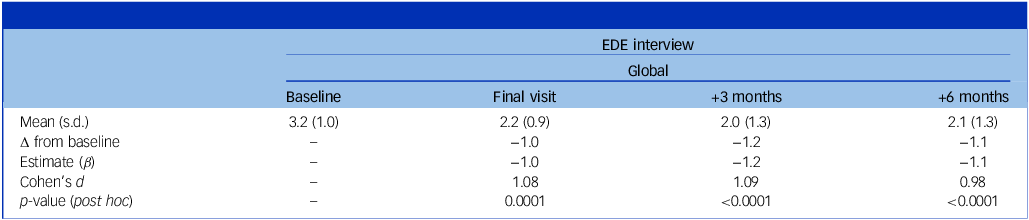
There was a significant reduction in global EDE scores over time (F(3, 60) = 15.5, p < 0.0001), with marked improvements observed at the final visit (β = –0.96, p = 0.0001, d = 1.08), 3-month follow-up (β = −1.20, p < 0.0001, d = 1.09) and 6-month follow-up (β = −1.09, p < 0.0001, d = 0.98) (Fig. 2 and Table 2). Baseline severity was a significant predictor of symptom change (β = 0.74, p < 0.0001), where participants with higher initial symptom severity experienced greater reductions over the study period. Antidepressant medication withdrawal was not found to be a significant fixed effect (p = 0.07, n = 20).
Global EDE interview results from baseline to the 6-month follow-up

Table 2 Long description
The table presents global EDE interview results from baseline to 6-month follow-up. It includes four columns: Baseline, Final visit, +3 Months, and +6 Months. The rows display mean scores with standard deviations, changes from baseline, estimates, Cohen’s d, and p-values. Notable trends include a reduction in mean scores from 3.2 at baseline to 2.2 at the final visit, 2.0 at 3 months, and 2.1 at 6 months. The changes from baseline are -1.0, -1.2, and -1.1 respectively. Estimates remain consistent at -1.0, -1.2, and -1.1. Cohen’s d values are 1.08 at the final visit, 1.09 at 3 months, and 0.98 at 6 months. All p-values are less than 0.0001, indicating significant reductions over time.
EDE, Eating Disorder Examination; Δ, change.
Last observation at baseline carried forward for the withdrawn participant. N = 21.
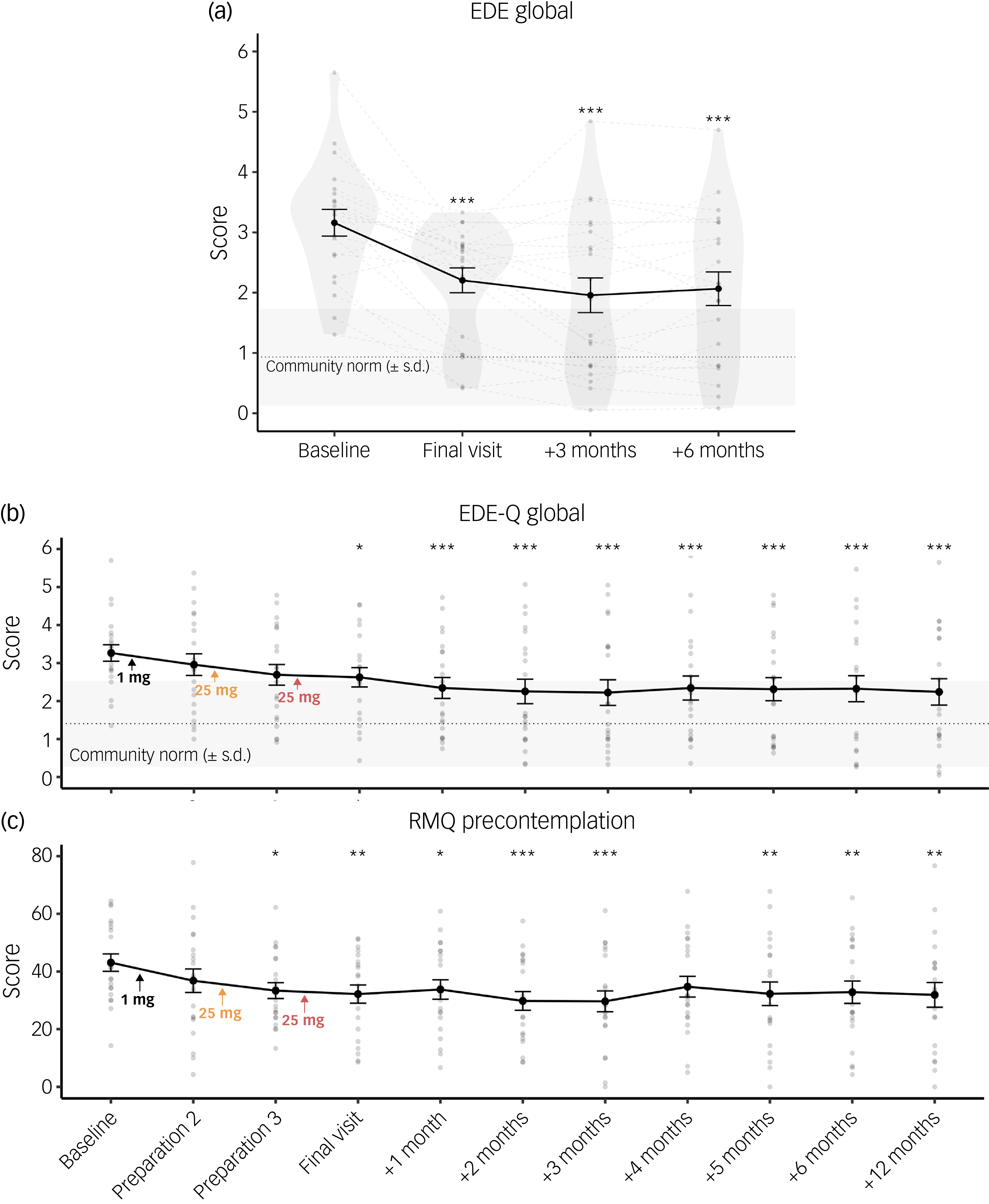
(a) Violin plot of global Eating Disorder Examination (EDE) interview scores from baseline to 6-month follow-up. Last observation carried forward from baseline for one withdrawn participant. (b) Global EDE-Q and (c) RMQ precontemplation scores from baseline to 12-month follow-up. Last observation carried forward for one withdrawn participant, in addition to missing data for participants at 4 months (n = 1), 5 months (n = 3), 6 months (n = 1) and 12 months (n = 1). Individual data points are shown as light grey dots (a–c), with matched participant data illustrated with dashed grey lines (a). The horizontal black line and grey box demonstrate mean community norm (‘remission zone’) +/– SEM, respectively (a, b). *p < 0.05, **p < 0.01, ***p < 0.001, N = 21. EDE-Q, Eating Disorder Examination Questionnaire; RMQ, Readiness and Motivation Questionnaire.

Fig. 2 Long description
The image contains three graphs that illustrate the outcomes of anorexia nervosa treatment over time. The first graph is a violin plot showing global Eating Disorder Examination interview scores from baseline to six-month follow-up. The second graph displays global EDE-Q scores from baseline to twelve-month follow-up. The third graph presents RMQ precontemplation scores over the same period. Each graph includes individual data points represented as light grey dots, with matched participant data illustrated with dashed grey lines in the first graph. The horizontal black line and grey box in the first and second graphs demonstrate the mean ‘community norm’, sometimes used as an indicator of ‘remission,’ plus or minus the standard error of the mean. Significant differences are indicated with asterisks, where * denotes p < 0.05, ** denotes p < 0.01, and *** denotes p < 0.001. The graphs collectively show the progression and changes in scores over time, highlighting the effectiveness and challenges of current treatments for anorexia nervosa.
Excluding the withdrawn participant, all participants except for two showed reductions in global EDE scores between baseline and the final visit. Scores for six (final visit), ten (3-month follow-up) and eight (6-month follow-up) participants fell within one standard deviation of the ‘community norm’, including two participants who were within this bracket at baseline.
There was a significant main effect of time on EDE subscale scores of dietary restraint (F(3, 60) = 15.0, p < 0.0001), eating concerns (F(3, 60) = 15.7, p < 0.0001), shape concerns (F(3, 60) = 7.9, p = 0.0001) and weight concerns (F(3, 60) = 3.4, p = 0.02). Subscales demonstrated a consistent pattern of sustained improvement up to the 6-month follow-up, except for weight concerns, which failed to maintain significance at 6 months. The greatest numerical decrease across scales was seen at the 3-month follow-up (Supplementary Table S8).
EDE-Q
A significant main effect of time was seen on global EDE-Q scores (F(10, 200) = 6.6, p < 0.0001), with reductions seen from the final visit to the 12-month follow-up compared with baseline. There was a trend-level reduction at the preparation 3 visit (pre-dose 3) (β = –0.57, p = 0.09, d = 0.61). Maximal numerical change was noted at the 3- and 12-month follow-up, showing a 1.1-point reduction (Fig. 2(b), Supplementary Table S10). Antidepressant medication withdrawal was not found to be a significant fixed effect (p = 0.28, n = 20).
A repeated-measures ANOVA revealed no significant main effect of dose on raw (F(2, 40) = 0.88, p = 0.42) or percentage incremental change (F(2, 40) = 1.34, p = 0.27) in global EDE-Q scores across all dosing sessions (Supplementary Table S11).
RMQ
A significant main effect of time on RMQ precontemplation scores was identified (F(10,200) = 3.99, p < 0.0001). Significant reductions were demonstrated after dose 2 (first 25 mg) (β = –9.71, p = 0.01, d = 0.89). Decreases were sustained across the 12-month follow-up period (p = 0.0017, d = 0.65), with a maximum reduction seen at the 2-month (β = –13.3, p = 0.0001, d = 0.86) and 3-month follow-ups (β = –13.4, p < 0.0001, d = 0.88). Reductions at 4 months trended toward significance (β = –8.36, p = 0.065, d = 0.58) (Fig. 2(c), Supplementary Table S13). Antidepressant medication withdrawal was not found to be a significant fixed effect (p = 0.42, n = 20).
The repeated-measures ANOVA results revealed no significant main effect of dose on raw incremental change (F(2, 40) = 0.85, p = 0.44) or percentage incremental change – with the removal of an extreme outlier – in RMQ precontemplation scores (F(2, 38) = 0.69, p = 0.51) (Supplementary Table S14).
Discussion
This study provides evidence of the feasibility of psilocybin therapy as an adjunct treatment for anorexia nervosa. This was indexed through (a) successful recruitment of the target sample size, despite the resistance to treatment and harm avoidance associated with anorexia nervosa; Reference Abbate-Daga, Amianto, Delsedime, De-Bacco and Fassino22,Reference Frank, DeGuzman, Shott, Laudenslager, Rossi and Pryor23 (b) a high retention rate of 95.2%; and (c) positive tolerability and safety data (e.g. adverse events). This is particularly pertinent given the drop-out rates of between 20 and 70% observed in both community treatment and clinical research. Reference Abbate-Daga, Amianto, Delsedime, De-Bacco and Fassino22,Reference Dejong, Broadbent and Schmidt24 The adverse events reported here are consistent with those observed in a prior psilocybin trial in anorexia nervosa from Peck et al, Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 other clinical populations Reference Yerubandi, Thomas, Bhuiya, Harrington, Villa Zapata and Caballero25 and those anticipated by Downey et al. Reference Downey, Chaphekar, Woolley and Raymond-Flesch26 Peck et al Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 reported two cases of post-dosing hypoglycaemia; however, this was not formally evaluated in our study, but no relevant symptoms were observed, although this does not equate to absence of occurrence. The lower baseline BMI in the current study (16.7 kg/m2 v. 19.7 kg/m2 in Peck et al Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 ) provides reassurance of favourable safety in more physically vulnerable cohorts. Reference Mehler and Brown27 However, caution is warranted when extrapolating findings to others living with anorexia nervosa because of the strict eligibility criteria producing a relatively homogenous sample.
The baseline global EDE mean score (3.2) was in line with those of individuals with anorexia nervosa receiving out-patient care (means: 3.32 and 3.33). Reference Byrne, Wade, Hay, Touyz, Fairburn and Treasure28,Reference Fairburn, Cooper, Doll, O’Connor, Palmer and Dalle Grave29 At the 6-week final visit, only three participants had not experienced improvements, including the excluded participant. When using the ‘community norm’ as an indicator of ‘remission’, six participants (28.6%) at the final visit, ten participants (47.6%) at the 3-month follow-up and eight participants (38.1%) at the 6-month follow-up were within this zone. It is noted, however, that two of these individuals were already within the ‘community norm’ range at baseline. However, both participants had a primary diagnosis of anorexia nervosa, and their symptoms were confirmed at screening. Although this limits measurable improvement, it primarily highlights the disorder’s complexity and indicates the EDE’s potential failure to fully capture the psychopathology in certain phenotypic profiles.
Variation in improvement between participants was large, a similar finding to Peck et al. Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 This variation became more pronounced later into the follow-up period, indicating that some participants were able to maintain these improvements and others were not. Exploratory study measures, Reference Spriggs, Douglass, Park, Read, Danby and de Magalhães17 such as personality, psychological insight and therapeutic alliance, may elucidate factors that contributed to this variation. However, this variation may reflect post-study life changes and the simple effect of time, confounding the intervention’s causal impact.
With the caveat that efficacy comparisons between trials can be questioned, we note that conventional treatments (e.g. specialist supportive clinical management, Maudsley model of anorexia nervosa treatment for adults, enhanced cognitive–behavioural therapy) have shown larger immediate reductions in global EDE scores than the present intervention, Reference Byrne, Wade, Hay, Touyz, Fairburn and Treasure28,Reference Fairburn, Cooper, Doll, O’Connor, Palmer and Dalle Grave29 but that the maintenance of these improvements up to 6 months is comparable. However, the participants in our study were ‘treatment-resistant’ and had found similar conventional treatments unsuccessful at maintaining their remission. Given the generally favourable efficacy data from this trial, a direct (i.e. between-participants) comparison of psychedelic-therapy with existing treatments for anorexia nervosa is warranted, with participants stratified by illness severity and disorder subtype (restricting/binge-purge). Because of the limited efficacy of pharmacological interventions, an alternative comparison may be with evidence-based talking therapies in wait-list, delayed treatment designs with matched psychological support and follow-ups extending 12–24 months. Reference Austin, De Silva, Ilesanmi, Likitabhorn, Miller and Sousa Fialho30 Other recommendations for psychedelic randomised controlled trials include ethically approved mild deception of dose or an active placebo to improve blinding. Reference Muthukumaraswamy, Forsyth and Lumley31
Conventional treatments differ from psychedelic therapy in that they are implemented weekly for approximately 40 weeks and include nutritional interventions. Participants in this study received a roughly equivalent amount of therapy hours (approximately 50 h of therapeutic contact), albeit condensed over a shorter period (6 weeks). The inclusion of talking therapy or ‘psychological support’ is an inherent feature of the conventional model of psychedelic therapy currently being trialled for various disorders. There was no nutritional intervention or focus on weight restoration in the current trial. Instead, emphasis was placed on self-compassion and the inclusion of family members (as support persons) in the therapeutic process, including the provision of education and skills (Supplementary Section 1.1), although support people were not present during dosing sessions.
In the efficacy data, we found the greatest improvements in the subscales of dietary restraint and eating concerns, indicating reductions in thoughts about rules specific to food and caloric restriction, and reduced preoccupation and guilt related to eating. This contrasts with Peck et al, Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 who reported significant improvements exclusively in the shape and weight concerns subdomains, with no significant improvement in dietary restraint or eating concerns. The highest scores at baseline in our study were in the dietary restraint and eating concerns subscales, in direct contrast to the participants in the Peck et al study. Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 Furthermore, all but one participant in our study had a BMI within the underweight range (<18 kg/m2), whereas 50% of the cohort in the Peck et al study Reference Peck, Shao, Gruen, Yang, Babakanian and Trim12 were categorised as partially weight-restored. These participant differences may explain the contrasting subscale findings between studies and could indicate that the potential benefit of psilocybin therapy may be mediated through different mechanisms of action, depending on each patient’s stage of illness severity and motivation for recovery.
EDE-Q and EDE results were largely consistent with each other; the former are patient-reported, whereas the latter are clinician-administered. It was hypothesised that improvements in eating disorder psychopathology would be greater following the 25 mg psilocybin doses, compared with the 1 mg placebo. However, this hypothesis was not confirmed; rather, all doses were of statistically equivalent, short-term therapeutic value to participants. Interpretation of this effect is complicated by the peak EDE-Q clinical response being observed 3 and 12 months post-intervention. Moreover, the study design did not allow for a legitimate or equally weighted comparison between doses because of the single-arm, fixed order and brief (i.e. 2 week) period between doses. The early improvements observed in this trial appear to align with similar observations with non-drug-assisted psychotherapies for eating disorders. Reference Chang, Delgadillo and Waller32
Clinical improvements at the final visit and beyond, therefore, cannot be confidently attributed to any specific intervention within the study, but rather to the entire treatment protocol. A between-participants design is required to compare the relative efficacy of psilocybin versus placebo or the putative dose-dependency of response to psilocybin therapy for anorexia nervosa. Although this limitation of the study design is noted, the primary objective of the study was not to test high-dose psilocybin’s superiority over a placebo dose of psilocybin, but rather to assess the feasibility and safety of this particular treatment protocol in this cohort of individuals with anorexia nervosa, for which the results are favourable.
The significant improvement in RMQ precontemplation over the follow-up period indicates that participants were transitioning to ‘contemplation’, in which they were better able to acknowledge the seriousness of their disorder, had more desire to change and had greater motivation to engage in the actions required for recovery. Like the EDE-Q, no single dosing session had a greater immediate effect on change.
Wider extrapolation of the current results is limited by several factors. First, despite efforts made to recruit a diverse cohort, there was a high percentage of highly educated White females. This is representative of those who undergo residential treatment for eating disorders, Reference Fisher, Henretty, Cox, Feinstein, Fornari and Moskowitz33 those partaking in psychotherapeutic clinical research Reference Burnette, Luzier, Weisenmuller and Boutté34 and, by education, race and ethnicity, those who participate in research investigating psychedelics. Reference Wen, Singhal, Jones, Zeifman, Mehta and Shenasa35 However, this demographic profile may afford them higher cognitive reserve to facilitate therapeutic engagement, and a more stable home and work environment in which integration takes place, with greater access to additional clinical care. The reproducibility of these findings in more diverse cohorts needs to be determined in future studies. The decision to recruit exclusively female (assigned at birth) individuals means a sample was recruited that well-represents those most affected by anorexia nervosa; however, the resulting inability to extrapolate to other populations is an obvious limitation. Additionally, the individual who conducted the EDE interviews was not blinded to the dosing regimen (Supplementary Table S9 presents comparative independent rater scores). Furthermore, as this was a feasibility study, the sample size was small, and analyses were treated as exploratory and thus were not controlled for multiple comparisons. Accordingly, no conclusive findings are reported.
In conclusion, this study provides evidence of the feasibility, safety and potential efficacy of this protocol of psilocybin therapy as an adjunct treatment in this cohort of females with anorexia nervosa. The feasibility of recruitment and retention of participants was established, and the reported adverse events are in line with existing psychedelic research. Significant improvements in eating disorder psychopathology and motivation to change were observed after the completion of all dosing sessions in this psilocybin therapy protocol. These improvements appeared to be cumulative, did not statistically differ based on psilocybin dose and were generally sustained across the follow-up period.
Because of the homogenous nature of the current sample, the extensiveness of screening and psychotherapeutic procedures, and limitations in the study’s design, we caution against extrapolation. However, given the sparsity of effective treatments for anorexia nervosa, this study’s findings support the case for more research into psychedelic therapy as a novel therapeutic strategy for anorexia nervosa and related disorders. Indeed, there are now numerous other clinical trials investigating psychedelic therapy in eating disorders and related conditions currently underway (e.g. NCT05481736, NCT06399263, Schneier et al Reference Schneier, Feusner, Wheaton, Gomez, Cornejo and Naraindas36 ).
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10687
Data availability
The data that support the findings of this study are available from the corresponding author, H.M.D., upon reasonable request. The analytic code and materials supporting the findings of this study are available from the corresponding author, H.M.D., upon reasonable request.
Acknowledgements
The research was conducted at The National Institute for Health and Care Research (NIHR) ICRF. We would like to thank the Clinical Data Systems team at the Imperial Clinical Trials Unit for their support. All authors affiliated with the Imperial College London Division of Psychiatry are supported by the NIHR Imperial Biomedical Research Centre. We would like to acknowledge other members of the Centre for Psychedelic Research who provided assistance with data collection and guidance, particularly Roberta Murphy, Joann Mallett, Joseph Peill and Fernando Rosas. We thank Bronwyn Lee at the University of Sydney for taking the time to provide independent scores of the EDE interviews conducted in this study (Supplementary Table S9). The research presented in this manuscript formed a section of a PhD thesis submitted by H.M.D., Reference Douglass37 which is currently embargoed for 12 months. The authors have permission to reuse this material in the current manuscript.
Author contributions
H.M.D. analysed the data, created the figures and wrote the original and revised versions of the manuscript. M.J.S., K.G., D.E., D.J.N. and R.L.C.-H. provided supervision and guidance. Data were interpreted by H.M.D., M.J.S., K.G., D.E., D.J.N. and R.L.C.-H. The study was conceived by M.J.S., R.L.C.-H. and D.J.N. The protocol was written by M.S., R.L.C.-H., D.E. and D.J.N. A.L., D.N. and R.J.P. contributed to protocol design. Study documentation was written by M.J.S. Regulatory approvals were obtained by H.M.D., M.J.S., D.E., D.J.N. and R.L.C.-H. Funding was acquired by R.L.C.-H. The trial was coordinated by H.M.D., M.J.S. and K.G., with administrative support provided by J.T.F. and G.S. Data were collected by H.M.D., M.J.S., K.G., J.D., F.M., K.L.A., L.M., J.M., S.A., J.T.F., G.S. and R.J.P. The statistical analysis plan was written by M.J.S. and A.B. The trial clinical team were J.D., F.M., K.A., L.M., K.L.A., J.M., S.A., T.R. and R.J.P. Clinical supervision and guidance were provided by T.R., A.L., D.E., R.J.P. and D.J.N. All authors reviewed and contributed to this article and approved the submitted version.
Funding
This work was supported by the Nikean Foundation, Valor Equity Partners and other funders of the Centre for Psychedelic Research. H.M.D. was funded by the Imperial College London President’s PhD Scholarship and Valor Equity Partners. R.L.C.-H. is supported by the Nostromo Foundation, Ralph Metzner Distinguished Professorship, the Larsen Family and Cohen Foundation.
Declaration of interest
The authors report that COMPASS Pathways provided them with the investigational drug COMP360 (a proprietary, pharmaceutical-grade, synthetic psilocybin formulation, optimised for stability and purity, developed by COMPASS Pathfinder Ltd). The authors also report that the Centre for Psychedelic Research at Imperial College London has received grants or drug materials from the following companies with interests in the psychedelic field: Compass Pathways, Small Pharma, The Usona Institute, Beckley Psytech (now AtaiBeckley) and Filament Health. H.M.D. reports receiving financial support to present this work at conferences from the Source Research Foundation and The Multidisciplinary Association for Psychedelic Studies. K.G. reports receiving Fellowship funding from the Rosetrees Trust. R.L.C.-H. reports receiving consulting fees as a scientific advisor from Entropy Neurodynamics, Red Light Holland, Otsuka and Mindstate Design Labs. D.J.N. reports receiving consulting fees from Algernon Pharmaceuticals Inc, owning stock options in Neurotherapeutics, and being the unpaid chair of the Psychedelic Access and Research European Alliance (PAREA) and Drug Science – two charities that work to improve understanding of and access to psychedelic medicines. D.E. reports receiving consulting fees as an advisor from Aya Biosciences, Lophora Aps, Clerkenwell Health and Mindstate Design Labs. A.L. reports receiving royalties for a clinical manual on emotion-focused family therapy that they authored and receiving consulting fees from Imperial College London for staff training and supervision. The other authors declare no competing interests.



 Open access
Open access
eLetters
No eLetters have been published for this article.