


Psychotic disorders are associated with high morbidity and mortality, Reference Simon, Stewart, Yarborough, Lynch, Coleman and Beck1 and have profound effects on individual subjective experience, Reference Fusar‐Poli, Estradé, Stanghellini, Venables, Onwumere and Messas2,Reference Fusar‐Poli, Estradé, Stanghellini, Esposito, Rosfort and Mancini3 including increased suicide rates, reduced quality of life, and substantial cognitive and functional impairments. Reference Bowden4–Reference McCutcheon, Reis Marques and Howes10 Evidence supports effectiveness of early intervention services (EIS) in mitigating these negative outcomes, Reference Birchwood, Todd and Jackson11–Reference Posselt, Albert, Nordentoft and Hjorthoj14 providing specialised, early-stage care to individuals experiencing first-episode psychosis (FEP). These services were initially developed with focus on reducing the duration of untreated psychosis (DUP), Reference Salazar de Pablo, Guinart, Armendariz, Aymerich, Catalan and Alameda15 and primarily centred on non-affective psychoses. Mood disorders, such as bipolar disorder and major depressive disorder (MDD) are associated with high prevalence of psychotic symptoms; Reference Aminoff, Onyeka, Ødegaard, Simonsen, Lagerberg and Andreassen16,Reference Ohayon and Schatzberg17 approximately 54% of individuals with bipolar disorder experience at least one psychotic episode. Reference Aminoff, Onyeka, Ødegaard, Simonsen, Lagerberg and Andreassen16 Similarly, although prevalence can vary, most studies suggest psychotic features are present in approximately 10–20% of individuals with MDD, with higher rates observed in clinical and in-patient settings (MDD with psychotic features (MDD-PF)). Reference Ohayon and Schatzberg17,Reference Wu, Zhao, Li, Yang, Peng and Zhou18 Diagnoses of these affective psychotic disorders can be made at first presentation, with a high degree of diagnostic stability (84%), Reference Fusar-Poli, Cappucciati, Rutigliano, Heslin, Stahl and Brittenden19 which is higher in cohorts of people with bipolar disorder. Reference Ruggero, Carlson, Kotov and Bromet20 Crucially, in bipolar disorder, diagnostic delay is substantial, with a systematic review suggesting delays of 6–10 years Reference Scott, Graham, Yung, Morgan, Bellivier and Etain21 and a recent meta-analysis suggesting a duration of untreated bipolar disorder of around 9 years, Reference Keramatian, Pinto, Tsang, Chakrabarty and Yatham22 contrasting with a median DUP of 14 weeks in non-affective psychosis. Reference Salazar de Pablo, Guinart, Armendariz, Aymerich, Catalan and Alameda15
Differences between affective and non-affective psychotic disorders exist across multiple domains, including aetiology, Reference Valli, Fabbri and Young23 neurobiology, Reference Jauhar, McCutcheon, Nour, Veronese, Rogdaki and Bonoldi24 clinical presentation, Reference Jauhar, Krishnadas, Nour, Cunningham-Owens, Johnstone and Lawrie25 course and outcome. Reference Coryell, Leon, Winokur, Endicott, Keller and Akiskal26,Reference Kotov, Fochtmann, Li, Tanenberg-Karant, Constantino and Rubinstein27 Although manic episodes in bipolar disorder are associated with higher risk of hospital admission, the overall course of bipolar disorder is generally more favourable than that of schizophrenia, Reference Heslin, Lappin, Donoghue, Lomas, Reininghaus and Onyejiaka28,Reference Tramazzo, Lian, Ajnakina, Carlson, Bromet and Kotov29 with schizophrenia following a more chronic, disabling trajectory, Reference Kahn, Sommer, Murray, Meyer-Lindenberg, Weinberger and Cannon30 often marked by progressive functional decline, Reference Harvey and Rosenthal31 persistent cognitive deficits Reference Colijn, Torres, Menon, Howard, Honer and Stowe32 and greater long-term impairment. Reference Jauhar, Johnstone and McKenna9 Treatment response also differs, with affective psychotic disorders responding better to pharmacotherapy Reference Yamada, Matsumoto, Iijima and Sumiyoshi33 (e.g. mood stabilisers such as lithium and lamotrigine Reference Maruki, Utsumi, Takeshima, Fujiwara, Matsui and Aoki34 ). Care is required with the use of antidepressants as monotherapy in bipolar disorder, because of the risk of treatment-emergent mania or rapid cycling. Reference Viktorin, Lichtenstein, Thase, Larsson, Lundholm and Magnusson35 However, in selected cases, particularly when mood stabilisers alone are insufficient, antidepressants may be considered in combination therapy. Reference Gitlin36 In MDD-PF, antidepressants in addition to antipsychotics are usually required. Reference Kruizinga, Liemburg, Burger, Cipriani, Geddes and Robertson37 Effectiveness of psychotherapies varies across disorders (e.g. psychoeducation being more effective in bipolar disorder and cognitive–behavioural therapy being more effective in depression Reference Jauhar, McKenna and Laws38–Reference Cuijpers, Karyotaki, Weitz, Andersson, Hollon and van Straten40 ), whereas schizophrenia often requires long-term antipsychotic treatment Reference Ostuzzi, Vita, Bertolini, Tedeschi, De Luca and Gastaldon41 and intensive psychosocial support. Reference Bighelli, Rodolico, García-Mieres, Pitschel-Walz, Hansen and Schneider-Thoma42 However, despite their transdiagnostic scope, EIS have historically focused more heavily on non-affective psychotic disorders, particularly schizophrenia spectrum disorders. Reference Shinn, Bolton, Karmacharya, Lewandowski, Yuksel and Baker43 Affective psychoses are often included within broader FEP studies, limiting development of targeted guidelines and intervention frameworks suited to their specific needs. Reference Chia, Cotton, Filia, Phelan, Conus and Jauhar44–Reference Jauhar, Ratheesh, Davey, Yatham, McGorry and McGuire46
Given the aforementioned delay in diagnosis, individuals with affective psychoses (specifically bipolar disorder) may already be in contact with services, yet remain undiagnosed or misclassified. Reference Scott, Graham, Yung, Morgan, Bellivier and Etain21 Furthermore, in some individuals at clinical high risk for psychosis, affective symptoms consistent with a mood disorder may precede onset of positive psychotic symptoms, which often emerge later in illness course. Reference Correll, Penzner, Frederickson, Richter, Auther and Smith47–Reference Salazar de Pablo, Cabras, Pereira, Castro Santos, de Diego and Catalan49 Even when accessing FEP services, these people may not receive evidence-based treatments for affective disorders. Reference Jauhar, Ratheesh, Davey, Yatham, McGorry and McGuire46 Consequently, understanding how affective psychotic disorders are represented within EIS is essential to inform the development of diagnosis-sensitive clinical pathways within these services. With the planned international expansion of EIS, both in terms of geographical implementation and in broadening their remit beyond non-affective psychoses, delineating and understanding the proportion of affective psychotic disorders among individuals treated for FEP is crucial for informing service design, tailoring clinical management and guiding resource allocation. Although the incidence of affective psychotic disorders has been measured – a 2018 meta-analysis of 33 studies reported that affective psychoses occur at approximately a third of the rate of non-affective psychotic disorders (7.12 v. 22.53 per 100 000 person-years) Reference Castillejos, Martin-Perez and Moreno-Kustner50 – the true proportion of affective psychotic disorders within EIS settings remains unclear, with particular relevance for service provision.
We therefore sought to quantify the proportion of individuals diagnosed with affective psychotic disorders (bipolar disorder with psychotic symptoms and MDD-PF) and non-affective psychotic disorder (including schizoaffective disorder) among individuals treated for FEP in EIS. Additionally, we examined the influence of sociodemographic characteristics, geographical area, population income level, urbanicity and psychotic symptoms on these proportions.
Method
The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; identifier CRD42021257473; see Supplementary Material 1 available at https://doi.org/10.1192/bjp.2026.10602). Findings are reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow51 and the Meta-Analysis of Observational Studies in Epidemiology (MOOSE), Reference Stroup, Berlin, Morton, Olkin, Williamson and Rennie52 both of which are part of the EQUATOR Network guidelines (see Supplementary Tables 1 and 2). Reference Altman, Simera, Hoey, Moher and Schulz53
Search strategy and selection criteria
A multi-step, systematic search strategy was independently conducted by two researchers (S.S., A.C.) to identify relevant articles. The Web of Science database (Clarivate Analytics) was searched from inception until 17 July 2025. The Web of Science database incorporates the Web of Science Core Collection, BIOSIS Citation Index, KCI-Korean Journal Database, Medline, Russian Science Citation Index and SciELO Citation Index, as well as Cochrane Central Register of Reviews and Ovid/PsycINFO databases. The following search terms were used: (‘First episode psychosis’ OR ‘FEP’ OR ‘early psychosis’) AND (EIP OR ‘Early intervention’ OR EIS OR ‘Early Intervention Services’). Articles identified were first screened as abstracts, and after the exclusion of those that did not meet our inclusion criteria, the full texts of the remaining articles were assessed for eligibility and decisions were made regarding their inclusion in the review through consensus. Searches were completed by manually reviewing the references of previously published articles and extracting any additional relevant titles. Google Scholar was used to look for these articles and, particularly, previous reviews. Discrepancies were resolved by consensus between the research team, to reach a 100% agreement. Data extraction was initiated following PROSPERO registration (CRD42021257473) in 2021. The initial data extraction was first performed on 1 July 2024.
Inclusion and exclusion criteria
Consistent with previous studies, Reference Clemente, Diniz, Nicolato, Kapczinski, Soares and Firmo54,Reference Grande, Berk, Birmaher and Vieta55 we used the following inclusion criteria: (a) original, observational or randomised controlled studies of patients with FEP; (b) recruitment at first contact to EIS; (c) reported the total number of FEP cases; (d) reported the relative proportion of affective psychotic disorders (bipolar disorder with psychotic symptoms, MDD-PF) in the FEP samples, or data to calculate these values (schizoaffective disorder was extracted and analysed separately as a non-affective psychotic disorder); and (e) diagnosis was made using DSM 56 or ICD criteria 57 (any version) via structured interviews or clinical assessment, defined as a registered clinician giving a formal diagnosis without a structured interview. Exclusion criteria were (a) reviews, clinical cases, abstracts, conference proceedings and study protocols; (b) studies conducted in individuals with other designations and (c) studies that focused on the epidemiology of psychosis without examining those within EIS. Additional criteria for meta-analysis included independent or non-overlapping studies at a specific follow-up point, as well as availability of sample size data for analysis. Overlap was determined by examining the name of the programme/cohort, the city or cities where the study was conducted, and recruitment periods. No language restrictions were applied.
Schizoaffective disorder was classified a priori as a non-affective primary psychotic disorder, consistent with its placement within the schizophrenia spectrum grouping in the DSM-5-TR 56 and ICD-11, 58 and was analysed separately from bipolar disorder with psychotic features and MDD-PF.
Data extraction
Data extraction was carried out independently by three researchers (S.S., B.P., C.A.). Disagreements were resolved by senior authors (S.J., A.C.). Extracted characteristics of the included studies included the following: first author and year of publication; name of the sample/EIS; sample size; urbanicity; country; DUP reported by authors; designation of patients (affective psychotic disorder, bipolar disorder); diagnostic criteria (DSM, ICD); age (mean age, s.d., range); gender (% female); relative proportion data for disorders (bipolar disorder with psychotic symptoms and MDD-PF); follow-up duration (in months); positive, negative and general psychotic symptoms (measured by the Positive and Negative Syndrome Scale); functionality (measured by the Global Assessment of Functioning (GAF) scale) and quality assessment (see below).
Quality assessment
The quality assessment tool used was the Newcastle–Ottawa Scale Reference Wells, Shea, O’Connell, Peterson, Welch and Losos59 (NOS), independently scored by two reviewers (A.C., C.A.). Studies were scored on three domains: selection (maximum four points), comparability (maximum two points) and outcome (maximum three points). The total NOS score ranged from 0 to 9, with 0–2 indicating poor quality, 3–5 indicating fair quality and 6–9 indicating good/high quality. Disagreements were resolved by a senior author (S.J.). The NOS (Supplementary Table 3) was operationalised as previously reported. Reference Wells, Shea, O’Connell, Peterson, Welch and Losos59
Strategy for data synthesis
A meta-analysis was conducted to assess the pooled proportion of affective psychotic disorders in EIS, using the meta Reference Balduzzi, Rücker and Schwarzer60 and metafor Reference Viechtbauer61 packages in R version 4.4.2 on macOS (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/). The metaprop function from the meta package was used to calculate pooled proportion estimates under a random-effects model, applying logit transformation to stabilise variances. Between-study variance (τ 2) was estimated using the DerSimonian–Laird method. Between-study heterogeneity was assessed using the I 2-statistic, with values >75% indicating high heterogeneity. To aid interpretation under a random-effects framework, we additionally calculated 95% prediction intervals, reflecting the range of true effects expected in a new study. Reference Higgins, Thompson and Spiegelhalter62 Robustness was examined using leave-one-out influence analyses, repeating the meta-analysis after sequential exclusion of each cohort (for additional information see Supplementary Methods 1). Small-study effects were examined via visual inspection of funnel plot asymmetry, and formally tested using Egger’s regression intercept. Reference Egger, Davey Smith, Schneider and Minder63
Subgroup analyses were carried out by continent (Europe, Asia, North America, Australasia, South America, Africa and multiple continents), urbanicity (classified using the Eurostat degree-of-urbanisation framework: https://ec.europa.eu/eurostat/web/rural-development/methodology) and national income level (NIL) (low income/high-medium income/high income). The income classification (NIL) of different countries was extracted from the World Bank database, which categorises economies based on Gross National Income per capita, using the World Bank Atlas Method, 64 and has been used in other prevalence studies of psychiatric disorders. Reference Kessler, Angermeyer, Anthony, Graaf, Demyttenaere and Gasquet65
When at least ten Reference Higgins and Thompson66 independent samples were available for a given outcome, meta-regressions were conducted, to evaluate effect of the following variables on the proportion of affective psychotic disorders: (a) mean age at baseline; (b) percentage of females; (c) percentage of White ethnicity; (d) year of publication; (e) positive, negative and general psychotic symptom severity; (f) functioning and (g) NOS quality assessment. Meta-regression β-coefficients were calculated to test how the outcome variable changed with a unit increase in the meta-regression factors.
Results
Sample characteristics
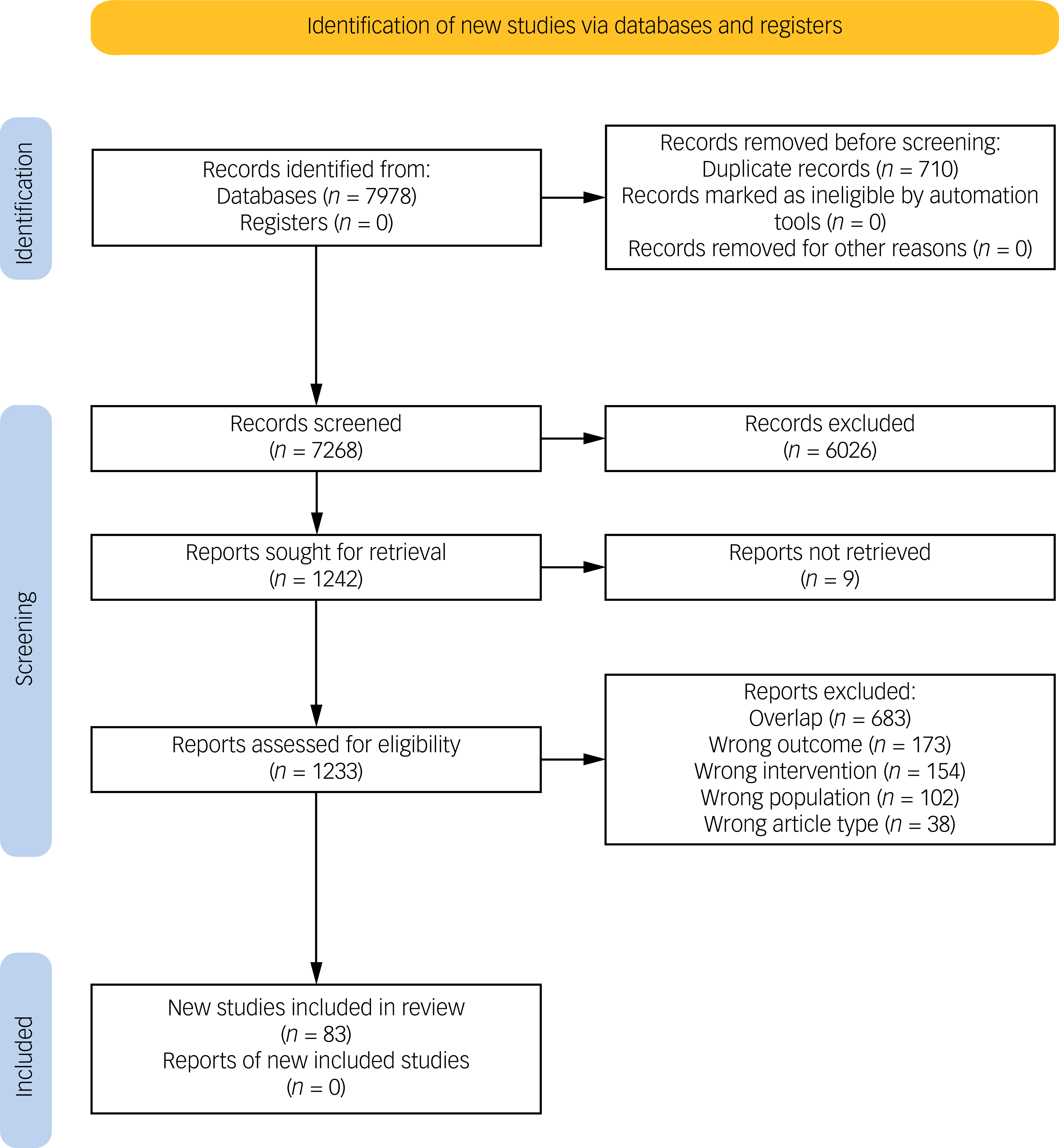
A total of 7978 records were identified through the literature search. After screening, 1242 full-text articles were assessed for eligibility. After excluding those not meeting inclusion criteria, 83 studies were included, reporting on 83 independent EIS cohorts (see Fig. 1 for PRISMA flowchart). The key characteristics of the included studies are outlined in Supplementary Table 4, and Supplementary Table 5 provides details on the primary reasons for article exclusion.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart. Reference Haddaway, Page, Pritchard and McGuinness67

The overall database comprised 30 946 individuals with a FEP. The mean age of the participants at baseline was 24.95 years (s.d. = 3.89; range 18.05–38.3 years) and 34.78% were female. Most studies were conducted in Europe (53.01%), followed by North America (27.71%) and Oceania (7.23%).
Although most included diagnoses were reported at baseline (n = 78, 93.98%), there was considerable variation in follow-up duration of the included cohorts, with mean follow-up of 41.17 months (s.d. = 53.98 months; range 1–252 months; median = 18 months).
There were no significant differences in sociodemographic characteristics between EIS that included affective psychotic disorders in their initial admission criteria (n = 71) and those that did not (n = 12). The percentage of females was similar in both groups (no: 36.06%, yes: 33.11%), as was mean age (no: 24.09 years, s.d. = 4.05; yes: 25.50 years, s.d. = 2.82). Likewise, GAF scores showed no significant differences (no: 42.82, s.d. = 9.83; yes: 38.73, s.d. = 7.35). Among the 12 EIS that explicitly excluded affective psychotic disorders in their admission criteria, none contributed cases of bipolar disorder or MDD-PF to the pooled analyses. However, these cohorts did include individuals diagnosed with schizoaffective disorder at first presentation, consistent with its a priori classification as a non-affective psychotic disorder in this review. Detailed cohort-level diagnostic contributions are reported in Supplementary Table 4.
Proportion of affective psychotic disorder
Most diagnoses in included studies were reported at baseline (93.98%). The estimated pooled proportion of affective psychotic disorder, including bipolar disorder and MDD-PF, was 18% (k = 70; 95% CI 15.44–20.60%; I 2 = 95.6%; median 19.5%; interquartile range (IQR) 11.2–25.3%), with a wide 95% prediction interval (3.6–39.4%), reflecting substantial between-service heterogeneity. Individual study estimates varied considerably, ranging from 1 to 57%, reflecting high heterogeneity (Fig. 2; Supplementary Fig. 1). For each pooled estimate, the between-study variance (τ 2) and study-level weights are reported in the Supplementary Material, alongside forest and funnel plots (Supplementary Figs 1–12), which illustrate that heterogeneity arises from a wide dispersion of cohort-level proportions rather than from a small number of highly influential studies. Leave-one-out analyses showed that the pooled proportion was highly stable, with exclusion of individual cohorts resulting in only minimal changes in the pooled estimate (range 17.4–18.3%), indicating that no single study disproportionately influenced the overall result.
Proportion of psychotic disorder. Affective psychotic disorders include bipolar disorder with psychotic symptoms and major depressive disorder with psychotic features. Non-affective psychotic disorders include schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder, brief psychotic disorder and other primary psychotic disorders. Pooled proportions are category-specific and derived from partially overlapping sets of studies; they are not mutually exclusive and should not be summed or interpreted as components of a single total.

A sensitivity analysis restricted to the 71 studies that did not explicitly exclude affective psychotic disorders yielded nearly identical estimates (e.g. bipolar disorder with psychotic features: 12.4%; MDD-PF: 7.7%), indicating that the inclusion of the remaining 12 studies did not materially affect the pooled proportions.
The proportion of bipolar disorder type 1 within FEP populations was 12.00% (k = 44; 95% CI 9.39–14.80%; I 2 = 93.8%; median 12.2%; IQR 7.5–17.7%), with a wide 95% prediction interval (1.6–28.9%) and substantial between-study variability (Fig. 2; Supplementary Fig. 2). Only two studies estimated proportion of bipolar disorder type 2, at 14.58% (k = 2; 95% CI 11.97–17.39%) (Fig. 2; Supplementary Fig. 3). The proportion of MDD-PF, based on 28 studies, was estimated at 7.19% (95% CI 5.39–9.21%), with considerable between-study variability (I 2 = 91.1%) (Fig. 2; Supplementary Fig. 4).
Proportion of non-affective psychotic disorder
The proportion of individuals with schizoaffective disorder was estimated at 7.40% (k = 49; 95% CI 5.78–9.19%; I 2 = 92.5%) (Fig. 2; Supplementary Fig. 5). A meta-analysis of 79 studies estimated the proportion of schizophrenia at 45.48% (95% CI 40.33–50.68%; I 2 = 98.7%) (Fig. 2; Supplementary Fig. 6). The proportion of individuals with schizophreniform disorder was 14.28% (k = 34; 95% CI 10.12–19.00%; I 2 = 96.8%), with substantial between-study variability (Fig. 2; Supplementary Fig. 7). The proportion of delusional disorder was estimated at 4.22% (k = 27; 95% CI 2.79–5.90%; I 2 = 92.2%), with high between-study heterogeneity (Fig. 2; Supplementary Fig. 8).
Psychosis not otherwise specified had an estimated proportion of 17.86% (k = 45; 95% CI 13.49–22.69%; I 2 = 98.3%) (Fig. 2; Supplementary Fig. 9). The proportion of substance-induced psychosis was 5.42% (k = 25; 95% CI 3.85–7.23%; I 2 = 93.4%) (Fig. 2; Supplementary Fig. 10).
Finally, the proportion of other psychotic disorders, defined in the studies as brief psychotic disorders or other unspecified psychotic conditions, was estimated at 11.43% (k = 49; 95% CI 8.35–14.83%; I 2 = 98.2%) (Fig. 2; Supplementary Fig. 11).
For further details on the proportion estimates, see Supplementary Results 1.
Subgroup analyses and meta-regression
Regarding sociodemographic variables, a higher percentage of females was associated with a slight but significant decrease in the proportion of affective psychotic disorder (β = −0.0050; p = 0.0041). However, age, percentage of White participants and year of publication were not significant moderators (Supplementary Table 6).
In the subgroup analysis by continent, substantial heterogeneity was observed (Q = 1575.2; d.f. = 69; p < 0.0001; I 2 > 89% across subgroups). Under the random-effects model, the pooled prevalence of affective psychosis was 16.8% (95% CI 14.7–19.0%) in Europe (k = 38), 6.9% (95% CI 3.1–11.9%) in Asia (k = 7), 19.4% (95% CI 12.0–28.1%) in Oceania (k = 9) and 26.2% (95% CI 18.3–34.9%) in North America (k = 14). Only one study each was available for South America (29.4%; 95% CI 15.1–46.0%) and for multi-continental samples (27.7%; 95% CI 25.1–30.4%). The test for subgroup differences was significant (Q = 64.1; d.f. = 5; p < 0.0001), indicating that prevalence estimates varied significantly across continents (Supplementary Table 6). In the meta-regression analysis with continent as a moderator, Europe was used as the reference group. Compared with Europe, studies conducted in Asia showed a significantly lower prevalence of affective psychosis (β = –0.16; p = 0.002), whereas studies from North America showed a significantly higher prevalence (β = 0.11; p = 0.005). No significant differences were observed for Oceania or South America, although the latter was represented by only one study.
In the subgroup analysis by NIL, pooled prevalence of affective psychotic disorder was highest in the low NIL group (k = 1; 21.9%; 95% CI 16.1–28.3%) and in the low–medium NIL group (k = 1; 19.3%; 95% CI 14.4–24.7%). The high NIL group (k = 59) showed a pooled prevalence of 18.9% (95% CI 16.3–21.8%), whereas the lowest prevalence was observed in the high–medium NIL group (k = 7; 9.7%; 95% CI 4.0–17.5%).
When stratified by urbanicity, pooled proportion of affective psychotic disorders was higher in urban settings (k = 49; 19.9%; 95% CI 16.7–23.2%) compared with rural settings (k = 21; 13.9%; 95% CI 10.5–17.7%). The difference between subgroups was statistically significant (p = 0.0268).
Among clinical characteristics, neither positive, negative, general nor total symptom scores were significantly associated with proportion of affective psychotic disorders. Similarly, GAF scores and NOS scores did not influence proportion estimates (Supplementary Table 6). For complete meta-regression estimates please see the Supplementary Material.
Heterogeneity and quality of included studies
Heterogeneity varied across analyses (I 2 ranged from 0 to 98.3%) but was very high (>90%) for almost all pooled estimates. The scale ranged from 5 to 9, with a mean of 7.37 (s.d. = 1.19) (Supplementary Table 7). Visual inspection of funnel plots and Egger’s regression did not suggest marked small-study effects (Supplementary Fig. 12). However, given the very high between-study heterogeneity observed across analyses, these assessments should be interpreted cautiously and considered exploratory rather than definitive indicators of absence of bias.
Discussion
Summary of findings
In this systematic review and meta-analysis, we examined the diagnostic composition of FEP cases treated within EIS, focusing on the proportion of affective and non-affective psychotic disorders across services and contexts. To the best of our knowledge, this is the first systematic review and meta-analysis to examine the relative proportion of affective and non-affective psychotic disorders in treatment-seeking FEP samples, i.e. people attending EIS. We found a pooled proportion of 18% for affective psychotic disorder across included studies, with substantial variability between studies. Given the substantial between-service heterogeneity, the pooled estimate should be interpreted as an average across heterogeneous EIS rather than as a single stable parameter; accordingly, the wide prediction interval indicates that the proportion of affective psychoses may vary markedly across services depending on local eligibility criteria and diagnostic practices. Bipolar disorder was the most prevalent form of affective psychotic disorder at 12%, followed by MDD-PF at 7.19%. Schizophrenia accounted for nearly 45.48% of cases, plus an additional 14.28% classified as schizophreniform disorder.
EIS have been developed and implemented within heterogeneous service models, with some programmes – such as those reported in the USA Reference Mueser, Penn, Addington, Brunette, Gingerich and Glynn68 and Spain Reference Mayoral-van Son, Juncal-Ruiz, Ortiz-García de la Foz, Vázquez-Bourgon, Setién-Suero and Tordesillas-Gutiérrez69 – explicitly restricting inclusion to non-affective psychoses, whereas others, particularly within the UK National Health Service framework, Reference NHS70 adopt a fully transdiagnostic approach that includes both affective and non-affective psychotic disorders. Consistent with this heterogeneity, our findings show substantial between-study variability in the proportion of affective psychotic disorders across EIS cohorts, while nonetheless indicating that affective psychoses constitute a meaningful minority of presentations within services that accept them.
Female gender was associated with a slight but significant decrease in the proportion of affective psychotic disorder. This is somewhat counterintuitive, given that MDD is approximately twice as prevalent in females Reference Kuehner71 and bipolar disorder has an equal prevalence across gender. Reference Merikangas, Akiskal, Angst, Greenberg, Hirschfeld and Petukhova72 However, these general prevalence patterns may not directly translate to the subset of affective disorders with psychotic features. A possible explanation is differential patterns of help-seeking and access to services, where females with affective psychotic symptoms may be more likely to receive care in primary or general psychiatric settings rather than within specialised EIS. A qualitative study of pathways to care in early psychosis found that women’s help-seeking was often dismissed or downplayed by both family members and clinicians, partly because of stereotypes portraying them as ‘overdramatic’ or ‘too functional’ to warrant specialised care. Reference Ferrari, Flora, Anderson, Haughton, Tuck and Archie73 These gendered dynamics may contribute to their underrepresentation in early intervention programmes.
Other factors such as age, percentage of White participants and year of publication did not significantly influence proportion estimates. However, the proportion of affective psychotic disorders in FEP varied significantly geographically. Compared with Europe, the proportion of affective psychosis was significantly lower in Asia, whereas in North America, proportion was higher. These variations may reflect regional differences in diagnostic practice, cultural perceptions of affective symptoms (and therefore access to care) or structural factors influencing access to EIS. Reference Richardson, Hameed, Perez, Jones and Kirkbride74–Reference Omer, Finnegan, Pringle, Kinsella, Fearon and Russell76 Differences in study settings, including sample population, geographic region and healthcare access, may explain variations in findings. Reference Jongsma, Turner, Kirkbride and Jones77–Reference Lasalvia, Tosato, Brambilla, Bertani, Bonetto and Cristofalo79
In our analysis, affective psychotic disorders appear less common in rural areas than urban settings, consistent with prior research. Reference Szöke, Charpeaud, Galliot, Vilain, Richard and Leboyer80 Urban environments often present higher levels of social fragmentation, socioeconomic deprivation and environmental stressors, all of which have been associated with increased risk of psychotic disorders. Reference Fett, Lemmers-Jansen and Krabbendam81 Although affective psychotic disorders appeared less common in rural areas in our sample, it is important to note most existing evidence on urbanicity and psychosis risk relates to non-affective psychoses. Reference Fett, Lemmers-Jansen and Krabbendam81 Although the link between urbanicity and schizophrenia is well established, evidence for an association with affective psychotic disorders is far more limited and inconsistent. Reference Fett, Lemmers-Jansen and Krabbendam81,Reference Schofield, Thisted Horsdal, Das-Munshi, Thygesen, Pedersen and Morgan82 Individuals in urban areas had more frequent contact with medical services (77%) compared with those in rural areas (52%), Reference Dahlberg, Forsell, Damstrom-Thakker and Runeson83 despite similar rates of anxiety and depression symptoms. These findings suggest availability and accessibility of mental health services in urban settings may contribute to the higher proportion of affective psychotic disorders observed in our review.
On the other hand, the proportion of affective psychotic disorder was significantly lower in those with high-medium NIL compared with those in the high NIL group. In contrast, only single studies contributed data for the low and low–medium NIL groups, limiting the generalisability of findings in these categories. Differences in healthcare infrastructure and access across NIL levels may substantially influence the detection and reporting of affective psychotic disorders. This occurs despite the well-established association between low NIL and higher prevalence of affective psychotic disorders. Reference Hakulinen, Komulainen, Suokas, Pirkola, Pulkki-Råback and Lumme84
In contrast, clinical characteristics such as psychotic symptom severity and global functioning were not significantly associated with the proportion of affective psychotic disorder in our sample. This differs from previous studies showing that patients later diagnosed with bipolar disorder tend to have better baseline functioning and fewer negative symptoms. Reference Salagre, Grande, Vieta, Mezquida, Cuesta and Moreno85 A likely explanation is that inclusion in EIS requires marked, pervasive psychotic symptoms and impairment, potentially excluding milder affective cases with better prognosis. Notably, such differences have been observed outside of EIS settings, following longer-term diagnostic follow-up. Reference Peralta, Janda, de Jalon, Moreno-Izco, Sánchez-Torres and Cuesta86 These results indicate that severity of psychotic symptoms, as measured by clinical scales, may not be the primary determinant in distinguishing affective psychotic disorder from other psychotic disorders in FEP populations at baseline.
Importantly, the moderators examined in this review – such as gender, age, geographical region, ethnicity, NIL and urbanicity – should be interpreted as indexing contextual and study- or service-level characteristics, rather than individual-level clinical or biological risk factors.
Strengths and limitations
This study provides the most comprehensive synthesis to date on the proportion of affective psychotic disorders in FEP cohorts. Its clinical relevance is strengthened by the focus on individuals treated within EIS, which provides more standardised and comparable data than studies conducted in heterogeneous, non-EIS settings. This enhances the clinical meaningfulness of the results, as they reflect real-world service use and diagnostic practices.
Limitations include lack of data from some geographical regions, such as South America and Africa. We acknowledge that diagnoses in FEP cohorts may change over time, although meta-analysis suggests reasonable diagnostic stability for schizophrenia (90%) and affective psychotic disorders (84%), Reference Fusar-Poli, Cappucciati, Rutigliano, Heslin, Stahl and Brittenden19 with better diagnostic stability for bipolar disorder. Reference Morgan, Lappin, Heslin, Donoghue, Lomas and Reininghaus87 Because most diagnoses in the included studies were assigned at first presentation, early diagnostic reclassification could not be examined and may contribute to discrepancies between service eligibility criteria and observed diagnostic distributions.
Although schizoaffective disorder occupies a diagnostically hybrid position, with criteria that span both primary psychotic symptoms and major mood episodes, we classified schizoaffective disorder a priori as a non-affective psychotic disorder, in line with its placement within the primary psychotic disorders grouping in the DSM-5-TR 56 and ICD-11 58 and its general management within schizophrenia spectrum pathways in many EIS. This decision inevitably simplifies an underlying clinical continuum, but provides a nosologically consistent and service-relevant practice, allowing us to focus the affective group specifically on bipolar disorder with psychotic features and MDD-PF.
Additionally, findings relating to NIL should be interpreted with caution. The small number of studies in two subgroups and the unbalanced NIL distribution required broad categorisation and limited the use of more nuanced measures (e.g. relative deprivation). Consequently, these analyses are exploratory and highlight the need for further research in diverse socioeconomic contexts. In the same way, alternative urbanicity classifications (e.g. Organisation for Economic Co-operation and Development frameworks) could not be systematically applied because granular location-level data were not consistently reported across studies.
Our findings should be interpreted in light of the fact that EIS vary widely in their organisational structure and recruitment pathways. A further limitation is the substantial heterogeneity observed across studies, which likely reflects genuine differences in diagnostic practices, sampling methodology and EIS eligibility criteria. Some recruit on a catchment basis, whereas others rely on referrals from traditional care pathways or even convenience samples; others report on research subsamples rather than consecutive clinical cohorts. Each of these dimensions profoundly shapes the diagnostic composition of EIS populations. Because such information was not consistently reported across primary studies, we were unable to include it in moderator analyses. Our estimates therefore reflect pooled proportions across heterogeneous contexts, which are likely to mirror the reach and implementation of services, rather than any universal distribution of affective versus non-affective psychoses. Accordingly, our pooled proportions should be interpreted as describing diagnostic composition within existing EIS, rather than population-level prevalence at first episode. Future studies should systematically document and report service-level features (e.g. inclusion criteria, catchment design, referral sources) to enable a more nuanced understanding of heterogeneity.
Implications
Notwithstanding the above limitations, our findings raise important questions about the extent to which affective psychoses – particularly bipolar disorder with psychotic features and MDD-PF – are recognised. In our meta-analysis, affective psychoses accounted for approximately 18% of all cases, highlighting a clear subgroup of people within EIS for whom care pathways may be less explicitly differentiated, particularly in services where protocols are primarily structured around non-affective psychoses. Our results suggest that EIS models may benefit from more systematic detection and management of affective disorder presentations, through routine use of structured mood-oriented screening at initial presentation (e.g. the Mood Disorders Questionnaire, Montgomery-Åsberg Depression Rating Scale and Calgary Depression Rating Scale), Reference Wang, Woo, Ahn, Ahn, Kim and Bahk88 and dedicated clinical pathways that integrate disorder-specific pharmacological and psychosocial interventions. This emphasis on diagnosis-sensitive pathways within early intervention frameworks is consistent with prior calls for improved recognition and targeted management of first-episode mania and bipolar disorder within EIS settings. Reference Chia, Cotton, Filia, Phelan, Conus and Jauhar44,Reference Jauhar, Ratheesh, Davey, Yatham, McGorry and McGuire89 Strengthening these elements within EIS could facilitate earlier, more accurate diagnosis, and support more appropriate treatment allocation for this important subgroup.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10602
Data availability
The data supporting the findings of this study are available from the corresponding author, S.J., upon reasonable request.
Acknowledgements
We would like to thank Moxun Zheng (BSc) and Yung Teng Lee (MSc) for their support in data extraction. The authors used a generative AI language model (ChatGPT, GPT-4, OpenAI, 2025) under human supervision to support clarity and readability in the drafting of this manuscript. AI assistance was limited to phrasing and editorial refinement in sections of the Introduction, Discussion and the Author contributions statement. The model was not used to generate scientific content, perform data analysis or draw conclusions. All outputs were critically reviewed, edited and approved by the authors to ensure accuracy and scientific integrity.
Author contributions
A.C. and S.S. conceptualised and designed the study. S.S., S.K., C.A. and A.C. conducted the systematic search and screening of studies. S.S., S.K., B.P. and A.C. performed data extraction and quality assessment. A.C., S.S. and B.C. conducted the statistical analyses and interpreted the results. S.S. contributed to the interpretation and framing of findings, drawing on both academic expertise and lived experience of bipolar disorder. R.A.M., P.S., A.T., R.S., A.R., D.Q., P.F., P.F.-P., A.H.Y. and R.M.M. contributed to the methodological refinement, contextualisation of results and critical revision of the manuscript. C.A. and B.P. contributed to the design of extraction tools and consistency checks. S.J. provided senior supervision and strategic guidance. A.C. and S.S. drafted the manuscript. All authors reviewed and approved the final version.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of interest
A.C. reports grants and personal fees from the Instituto de Salud Carlos III. She has also received research support from the Basque Government and honoraria from Janssen-Cilag, ROVI, Otsuka and Lundbeck, all outside of the submitted work. P.F.-P. is supported by #NEXTGENERATIONEU, funded by the Ministry of University and Research National Recovery and Resilience Plan, project MNESYS (PE0000006) – A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022). A.H.Y. is a member of the British Journal of Psychiatry Editorial Board. He was not involved in the peer-review or decision-making process for this manuscript. All other authors declare no conflicts of interest.




 Open access
Open access
eLetters
No eLetters have been published for this article.