


Introduction
Municipal public health policy is the sum of actions undertaken by local authorities that result in resources being allocated to preventive interventions, such as non-compulsory vaccination programs, health-education programs in schools, anti-obesity schemes, etc. (cf Baggott Reference Baggott2010; Bernier and Clavier Reference Bernier and Clavier2011; Foldspang et al. Reference Foldspang, Birt and Otok2018). The COVID-19 pandemic proved the importance of such preventive policies, both at the central and local level. Across Europe, including Poland, municipal governments were often at the forefront of the fight to contain the spread of the virus. Acting as “first-movers,” they served not merely as agents of the central authorities but also as actors in their own right, especially in decentralized systems (Adeel et al. Reference Adeel, Catalano, Catalano, Gibson, Muftuoglu, Riggs and Sezgin2020). Yet even before the pandemic, with the steady rise in urban populations around the world, the role of cities had grown in particular, making urban health a prospering research stream in public health studies (Galea and Vlahov Reference Galea and Vlahov2005). This general trend reflects the transition from centralized to more decentralized and heterogeneous structures of welfare governance, observed by social policy scholars (e.g., Bertin and Carradore Reference Bertin and Carradore2016; Kazepov Reference Kazepov2010). It is also evident in important initiatives promoted by international organizations such as the WHO “healthy cities” project.
Despite its growing significance, local preventive policy has suffered particular neglect in the existing empirical literature – both in terms of the overall interest and the apparent lack of engagement with existing policy theories (cf Greer et al. Reference Greer, Bekker, Leeuw, Wismar, Helderman, Ribeiro and Stuckler2017; Kneale et al. Reference Kneale, Rojas-García, Raine and Thomas2017; Lilly et al. Reference Lilly, Kean, Hallett, Robinson and Selvey2023). This gap persists even though such policies are important for shaping health equity and social determinants of health (Schultz et al. Reference Schultz, Christina Zorbas, Yoong and Backholer2023). Moreover, decentralized institutional arrangements risk reinforcing Matthew Effects, whereby disadvantaged municipalities or population groups are underinvested, while better-off localities and groups benefit disproportionately (Babić and Šućur Reference Babić and Šućur2022; Bonoli and Liechti Reference Bonoli, Liechti, Busemeyer, de la Porte, Garritzmann and Pavolini2020). Few researchers, however, have addressed the differing patterns of local public health decision-making by referring to existing policy theories, since policy scholars would previously focus on studying the medical component of health systems and not on the proactive part that is public health (Lynch Reference Lynch2023). Recently, however, a growing number of scholars have advocated for a more effective combination of the perspectives offered by policy sciences and public health (Fafard and Cassola Reference Fafard and Cassola2020; Greer et al. Reference Greer, Bekker, Leeuw, Wismar, Helderman, Ribeiro and Stuckler2017; Lynch Reference Lynch2023). Against the backdrop of this rapprochement, existing explanations of differing patterns of public health policy need further improvement, notably in contexts like Poland, which so far has not been thoroughly investigated (cf Lilly et al. Reference Lilly, Kean, Hallett, Robinson and Selvey2023).
The main objective of this article is to examine the combinations of socio-political, demographic, and economic conditions related to the presence or absence of universal targeting in municipal public health policy. By focusing on configurations of selected structural factors, it seeks to go beyond the state of the art by capturing mixes of structural conditions that underpin different policy choices of local authorities, namely whether to invest in well-funded programs for large groups of beneficiaries or not. While it is clear that individual socio-political, demographic, and economic conditions are important for local decision-making in other policy contexts (Andreotti and Mingione Reference Andreotti and Mingione2016; Andreotti et al. Reference Andreotti, Mingione and Polizzi2012; Bertin and Pantalone Reference Bertin and Pantalone2018; Hajnal and Trounstine Reference Hajnal and Trounstine2010; Hanssen et al. Reference Hanssen, Pettersen and Tveit Sandvin2001; Jensen and Lolle Reference Jensen and Lolle2013), their interaction in the domain of local public health policy remains insufficiently studied.
Beyond its empirical contribution, the study advances discussions on the concept of universal targeting by applying it to the analysis of subnational public health policy. Universalism typically describes policy design that benefits all citizens as a social right (e.g., Esping-Andersen Reference Esping-Andersen1990). Preventive policies, however, are typically neither fully universal nor means-tested but rather benefit selected groups of citizens endangered by specific health hazards. Hence, “universalism” remains a more complex category in public health than in many other policy domains. Scholars have proposed that in specific policy domains universal design addresses just selected categories of citizens – becoming “universal targeting” or “targeting within universalism” instead (Cruz-Martínez Reference Cruz-Martínez2019, Reference Cruz-Martínez2020; Jacques and Noël Reference Jacques and Noël2021). Whereas pure universalism is not realistically feasible in such instances, policies can still benefit a selected, yet broad, group of recipients as a right. For example, when categories of citizens such as “parents with children” benefit from a certain policy, even though the entire population cannot be covered.
Public health researchers have independently reached similar conclusions and accordingly developed the concept of “proportionate universalism.” It recognizes that the implementation of public interventions needs to be proportionate compared to the risks or disadvantages faced by beneficiaries (Carey et al. Reference Carey, Crammond and De Leeuw2015; Marmot et al. Reference Marmot, Allen, Goldblatt, Boyce, McNeish, McNeish and Geddes2010). In other words, while programs are designed to be universal, they must also have an appropriate scale and equity-oriented goals to truly benefit those most in need (Marmot et al. Reference Marmot, Allen, Goldblatt, Boyce, McNeish, McNeish and Geddes2010; Marmot and Allen Reference Marmot and Allen2024). By connecting these differing conceptualizations of universalism, this article refers to two main forms of policy design in municipal public health: universal targeting (where well-funded public health programs reach a significant proportion of local residents) and non-universal targeting (where such programs are largely absent). Previous research suggests that universal targeting, just like universalism itself, can be implemented in heterogeneous ways (Carey et al. Reference Carey, Crammond and De Leeuw2015; Francis-Oliviero et al. Reference Francis-Oliviero, Cambon, Wittwer, Marmot and Alla2020; Jacques and Noël Reference Jacques and Noël2021). However, its implementation in varying contexts is still not well understood. Thus, beyond its empirical value, this article contributes to the expanding literature on “universal targeting” in social policy, both by investigating and verifying the concept in a previously unexplored policy context.
To account for variations in public health policy design, this article addresses the question, “Which configurations of socio-political, demographic and economic conditions were consistently linked to the presence (and independently: the absence) of universal targeting in municipal public health policy?.” Building on it, the study employs fuzzy-set Qualitative Comparative Analysis (fsQCA), a configurative research method that identifies necessary and sufficient combinations of conditions linked to particular outcomes. The analysis presented here advances the theoretical perspective as formulated by Alberta Andreotti and Enzo Mingione in their studies of local welfare regimes (LWR, Andreotti and Mingione Reference Andreotti and Mingione2016; Andreotti et al. Reference Andreotti, Mingione and Polizzi2012). The LWR views each locality as a microcosm shaped by its unique institutional, demographic, infrastructural, and historical characteristics (ibid). Drawing on the comparative welfare state research of Esping-Andersen and others, the authors identify distinct groups of determinants of subnational variations in social policy, including economic, demographic, and socio-political conditions (Andreotti et al. Reference Andreotti, Mingione and Polizzi2012). This conceptual differentiation is used in this study to delineate potential conditions of universal targeting in municipal public health policy. By combining the LWR perspective with fsQCA, the analysis enables measurement of its configurative dimension – namely, the local combinations of conditions that shape policy design – while extending the theory beyond small-N applications without moving away from its case-oriented focus.
The comparison covers Poland’s 23 largest city counties – municipalities with county-level administrative status. On its own, Poland ranks among the most decentralized EU member states, placing third in decentralization at the local (gmina) level and eighth overall in terms of general decentralization (European Committee of the Regions 2020). Due to this high degree of autonomy, numerous public health responsibilities in Poland are delegated to local authorities. Unlike healthcare provision, which is centrally administered by the National Health Fund, municipalities can shape both the direction and content of the desired preventive public health programs (i.e., programy polityki zdrowotnej). These interventions can be initiated independently at all administrative levels and are frequently implemented in formal partnerships with local non-governmental organizations – unlike other mandated local schemes aimed at preventing the harmful use of alcohol. Local public health programs include non-compulsory vaccinations (e.g. against influenza), IVF treatments, anti-obesity campaigns, health education in schools, and screening tests (Sawicki et al. Reference Sawicki, Błoch and Świtalski2018). Since they arise from municipal decisions, they represent a direct expression of discretional municipal policymaking and form the primary focus of this article. Examining Poland’s example can, therefore, contribute to the existing research of local public health policymaking in decentralized systems by focusing on a previously overlooked, post-socialist country, where public health policy is largely locally organized (cf Lilly et al. Reference Lilly, Kean, Hallett, Robinson and Selvey2023).
The next section presents the conditions selected for the analysis. Their choice is justified based on literature review, case knowledge, and preliminary comparative analyses, in what forms an iterative research process. Next, the methods and operationalization (calibration) of the data are presented, followed by presentation and discussion of results, conclusions, and potential limitations of the analysis.
Literature review and conditions
The theoretical perspective applied here – the Local Welfare Regimes (LWR) theory – dictates the general types of conditions encompassed by the comparative analysis, namely economic, demographic and socio-political (Andreotti and Mingione Reference Andreotti and Mingione2016; Andreotti et al. Reference Andreotti, Mingione and Polizzi2012). These three categories incorporate factors affecting both the demand and supply of social services, but their specific configurations are argued to be context-dependent in LWR (ibid). To determine which conditions of universal targeting in municipal public health policy should be considered in the final analysis, preliminary inductive QCA tests were conducted, alongside a comprehensive literature review specified below (see also Table A2 in Appendix A). This combined strategy aimed to expand the analysis with additional relevant factors and their possible interactions to overcome the limitations of QCA regarding the number conditions it can effectively include. All conditions included in the final version of the comparison are outlined below.
Municipal affluence (AFFL)
At least since the groundbreaking research of the 1960s (Dawson and Robinson Reference Dawson and Robinson1963), indicators of municipal affluence and development have been treated as important factors driving the variation of sub-national public policy. Existing research on municipal public health policy agrees with this assessment to a significant extent. A range of empirical studies have argued that financial difficulties had a lasting impact on public health policies implemented in Italian regions (Adamo et al. Reference Adamo, Sturabotti, D’Andrea, Baccolini, Romano, Iannazzo, Marzuillo and Villari2017; De Vito et al. Reference De Vito, Massimi, Thiene, Rosso, D’Andrea, Vacchio, Villari and Marzuillo2016; Rosso et al. Reference Rosso, Marzuillo, Massimi, Vito, de Belvis, Torre, Federici, Ricciardi and Villari2015). Similarly, small-N comparisons of municipal preventive and health promotion policies in Sweden found that limited financial resources proved to be a significant policy constraint (Guldbrandsson et al. Reference Guldbrandsson, Bremberg and Bäck2005; Jansson and Tillgren Reference Jansson and Tillgren2010). On such a basis, it is reasonable to expect that comparatively richer cities will implement relatively well-funded and universal programs.
Large population (POP)
Population size is a standard control variable used in quantitative large-N comparisons of public policies and it has long been recognized as a significant predictor of sub-national variation in public spending, much like the state of the municipal economy (e.g., Fabricant and Lipsey Reference Fabricant and Lipsey1952). More broadly, the LWR perspective maintains that the structure of the population influences the distribution of needs within localities (Andreotti and Mingione Reference Andreotti and Mingione2016). Research in public health has also shown that the size of municipalities is an important condition affecting preventive spending, observing that the scale of programs determines the efficiency of service provision (Guldbrandsson et al. Reference Guldbrandsson, Wennerstad and Rasmussen2009; Santerre Reference Santerre2009; Simonsen-Rehn et al. Reference Simonsen-Rehn, Øvretveit, Laamanen, Suominen, Sundell and Brommels2006). In line with this prediction, universal targeting in public health policy should be detectable in the largest city counties.
Unhealthy population (POORHELTH)
In the context of public health programs, population health is a major characteristic of the population that shapes the demand for interventions and therefore cannot be overlooked. Public policies, at least declaratively, aim to address certain issues or social problems. In such pluralist perspective, as conceptualized by scholars like Zoltan Hajnal, Jessica Trounstine, and other authors, local government acts as a responsive mechanism that seeks to accommodate the needs by increasing public spending (Feiock and West Reference Feiock and West1993; Hajnal and Trounstine Reference Hajnal and Trounstine2010). In a similar vein, public health researchers have consistently argued that population health is an important condition influencing preventive policies that actually gain implementation (see Asthana and Halliday Reference Asthana and Halliday2006; Guldbrandsson et al. Reference Guldbrandsson, Bremberg and Bäck2005; Handler et al. Reference Handler, Issel and Turnock2001). The evidence base thus suggests that, in cities experiencing a relatively worse health situation, well-funded and universalistic policies are more likely to be present.
Strong civil society (CIVSOC)
As argued in the seminal works of Robert Putnam and his team, social capital and norms of reciprocity should be regarded as having an important positive influence on public policies at the local level, where social bonds are built organically (Johansson and Koch Reference Johansson, Koch, Johansson and Koch2016; Putnam et al. Reference Putnam, Leonardi and Nanetti2001). In public health research, stronger civil society has consistently been linked to better population health outcomes (Baum Reference Baum1999; Hawe and Shiell Reference Hawe and Shiell2000). Based on these findings, it is reasonable to assume that comparatively strong civil society should coincide with universal targeting in municipal public health policy among the investigated cases.
Substantial representation of women in city councils (WMR)
The existing literature on political determinants of public health policy appears contradictory. Some studies point to political preferences and stances playing a role in shaping public health interventions, with left-wing policymakers more likely to invest in them (Kim and Kim Reference Kim and Kim2022; Mead et al. Reference Mead, Thurston and Bloyce2022). In contrast, other scholars argue that public health is a depoliticized policy area. From this angle, political actors have little to gain from public health interventions, given their dispersed and long-term impact (Hoeijmakers et al. Reference Hoeijmakers, De Leeuw, Kenis and De Vries2007; Jacques and Noël Reference Jacques and Noël2022). The influence of the composition of local councillors, particularly the level of representation of women in official bodies, is also unclear. In other policy contexts, a higher share of women councillors has been linked to better-funded and more universal social policies (e.g., Bolzendahl and Brooks Reference Bolzendahl and Brooks2007; Funk and Philips Reference Funk and Philips2019). Accordingly, one can expect that cities with a substantial representation of women in city councils will be more inclined to implement universal targeting in municipal public health policy.
The preliminary QCA tests included two additional political conditions: “high share of progressive city councilors” and “above-average support for left-wing parties” (see Table A2 in Appendix A). However, these choices did not produce consistent and interpretable results, partially due to low variability of political preferences among the chosen cities (the vast majority leaned liberal in national elections). The lack of consistent results implies that political factors alone cannot explain differences in local authorities’ choices regarding public health policy design. In contrast, the literature supports the inclusion of the share of women in the city council as an alternative political condition relevant to local public health policymaking. Nevertheless, the chosen scope of the analysis should be kept in mind when interpreting the results presented in the following sections.
Methods and operationalization
In the analysis detailed here, fuzzy-set QCA has been employed to identify necessary and sufficient conditions for the presence (and separately the absence) of universal targeting in municipal public health policy among Poland’s largest municipalities. To this end, the statistical language R was used, together with appropriate SetMethods and QCA packages (see Oana and Schneider Reference Oana and Schneider2018; Thiem and Duşa Reference Thiem and Duşa2013). QCA is suited for medium-N comparisons embedded in case knowledge, as it combines the strengths of case-oriented and more formal large-N comparative approaches (Berg-Schlosser et al. Reference Berg-Schlosser, Meur, Rihoux, Ragin, Rihoux and Ragin2009; Ragin Reference Ragin1987). The method uses logical calculations to identify combinations of conditions linked consistently with a particular outcome. Or, in other words, it establishes empirical patterns of co-occurrence between conditions and the investigated outcome among the chosen cases (cf Greener Reference Greener2021). In practice, this involves determining if one set of cases is a subset of another (Oana et al. Reference Oana, Schneider and Thomann2021). In accordance with established practices (ibid), in this article an analysis of necessity is followed by an analysis of sufficiency, conducted separately for both the presence and absence of universal targeting. Consequently, this study offers new insights into the configurations of conditions under which local public health policies are developed.
Cities included in the analysis – presented on Map 1 – were selected based on their similarity to minimize possible confounding factors, following the Most Similar Systems Design (Przeworski and Teune Reference Przeworski and Teune1970). This strategy maximizes the variation of the explained phenomenon while minimizing the variance related to possible confounding conditions (Anckar Reference Anckar2008). Crucially, the included 23 cities were selected from 66 urban centers that also enjoy the county-level administrative status. Beyond this administrative similarity, the cases were chosen for their similarities in terms of political and cultural orientation – more liberal and secular than the rest of the city counties as illustrated in Table A1 in Appendix A – in order to largely exclude these factors from the analysis. Their political similarities are reflected in the local electoral performance of national centrist and liberal parties in the 2019 parliamentary elections; in 21 of 23 included cities the liberal opposition received more votes than the ruling right-wing coalition (Statistics Poland 2023). Likewise, none of the mayors was explicitly affiliated with right-wing political forces. As the name “city county” would also suggest, these administrative areas exercise both municipal rights and those existing in the county-level powiat units, of which there are over 300 in Poland. On this basis, they play an important role in the wider public health sector and implement relatively more public health programs than do the administrative units at local or regional (provincial) level.
23 city counties included in the comparison. Source: author’s own elaboration using GADM data (4.1, 2025) and R packages: sf (Pebesma Reference Pebesma2018) and ggplot2 (Wickham Reference Wickham2016).

While other partisan conditions, such as above-average support for left-wing parties, were initially included in empirical tests (see Table A2 in Appendix A), they yielded inconsistent results, skewing the analysis toward other structural explanations. Nonetheless, the investigated cases still exhibited significant variation in public health policy. This in practice ensured that the research aims were met: while political similarities between the cases and the MSSD design did limit the analysis in some sense, the chance was effectively taken to highlight the potential role of other structural conditions in municipal public health policymaking.
To measure universal targeting in municipal public health policy, it was necessary to formulate a measurement strategy that would allow for the inclusion of both the monetary and qualitative aspects of this concept. Accordingly, the fuzzy-set Universal Targeting Index (fsUTI) was developed, which draws on the existing databases provided by Statistics Poland (2023) and the Ministry of Health (2022). The fsUTI includes several key components. On the quantitative side, it contains information on municipal per capita spending on non-obligatory public health programs in 2019. Because these programs are implemented at the discretion of municipal policymakers, the associated spending can be regarded as indicative of the importance municipal authorities place on public health policy. Consistent with the chosen definition of “universal targeting,” the programs should also be of a certain scale and have sustainable funding to be considered as based on the principles of universalism (cf Cecchini et al. Reference Cecchini, Filgueira, Martínez and Rossel2015; Cruz-Martínez Reference Cruz-Martínez2020; Marmot et al. Reference Marmot, Allen, Goldblatt, Boyce, McNeish, McNeish and Geddes2010). As argued by Olivier Jacques and Alain Noel, the existing literature implies that “Universalism favours high levels of social expenditures (…).” The inclusion of spending in the index is therefore essential to ensure proper representation of the concept’s monetary aspect.
Beyond that, the fsUTI contains information on the content of policies implemented, indicating whether the preferred group of beneficiaries of the existing programs is broad (population-oriented) or narrow. Due to the shortcomings of the available data sources, simultaneous use was made of two universal targeting measures, with a view to the precision of the index being increased:
-
1. The share of participants in programs included within the “universal prevention” category (a legal designation used for statistical purposes under the National Health Programme);
-
2. The share of participants in programs targeting more than 1% of a given city’s population.
Combined with the measure dedicated to municipal spending on public health programs, the categories included in the fsUTI assess the extent to which municipalities prioritize the implementation of well-funded, universally targeted programs for broad categories of beneficiaries, as opposed to not pursuing such a policy. In broad terms, this approach aligns with Jon Kvist’s measurement of social rights in welfare states, which includes indicators of both generosity and accessibility (Kvist Reference Kvist2007).
Instead of typical arithmetic methods, the Universal Targeting Index (Figure 1) was constructed using the fuzzy-set approach (Büchel et al. Reference Büchel, Humprecht, Castro-Herrero, Engesser and Brüggemann2016; Trueb Reference Trueb2013) and follows the family resemblance strategy in set-theoretic concept formation (Barrenechea and Castillo Reference Barrenechea and Castillo2019). As a result, the presence of universal targeting in municipal public health policy is determined by the presence of high spending on the programs (a necessary attribute, a prerequisite, NA) combined with at least one criterion indicating the type of targeting and relative importance of universal design (a substitutable attribute, SA). In more precise terms, a high value of fsUTI (closer to 1) reflects the combination of the presence of higher-than-median spending on public health programs (>19 PLN per capita) and a high share of participants in universal public health programs officially designated as “universal” (SA1), or a high share of participants in programs substantial enough to be considered universal relative to the population size (SA2). The process of index construction and reasons for the inclusion of specific indicators are detailed in the Appendices.
Values for the fuzzy-set Universal Targeting Index in 2019.
Source: author’s own elaboration.

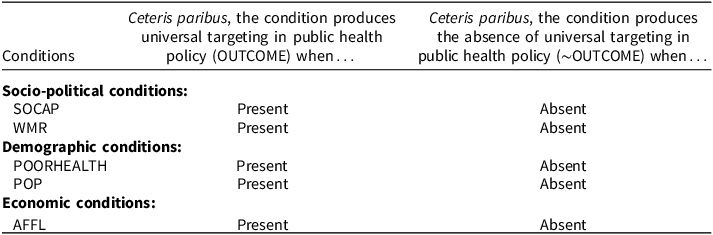
Following the recommendations of Oana and her research partners, the main parameters used to assess the empirical relevance of the results are consistency (inclusion score) and coverage (raw and unique, ibid). Likewise, given that QCA is fundamentally a qualitative method, directional expectations, instead of testable research hypotheses, are formulated in this article (outlined in the literature review section and presented in Table 1). It is important to note that while fsQCA emphasizes combinations of conditions present with a certain outcome, it does not estimate the effect of individual variables in isolation, unlike standard statistical analyses. Directional expectations, then, represent counterfactual arguments and may be applied only to some of the chosen conditions. While not testable, these hunches on the role of individual conditions in creating the outcome can leave the solution more parsimonious and easier to interpret when used in the relevant calculations (Oana et al. Reference Oana, Schneider and Thomann2021).
Directional expectations
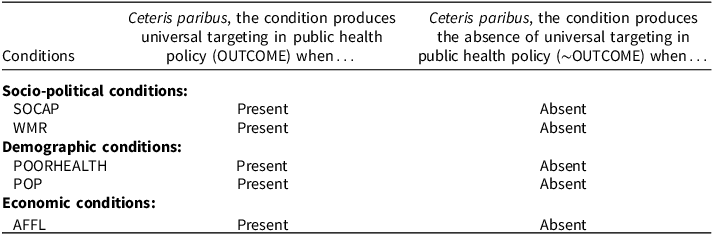
Source: author’s own elaboration, the format adopted from Hinterleitner, Sager, and Thomann Reference Hinterleitner, Sager and Thomann2016.
Note: “∼” signifies the absence of directional expectation.
In set-theoretic methods, such as fsQCA, operationalization is accompanied by a process of calibration that determines the membership of cases in sets representing relevant conditions and the outcome. In the fuzzy-sets version of the method, cases are assigned membership scores ranging from 0 (complete absence) to 100 (complete presence), based on the values of indicators. The conversion point, or “crossover point,” designates the value at which a condition changes from being considered more absent than present. In this study, the direct method of calibration is applied (Oana et al. Reference Oana, Schneider and Thomann2021), alongside the relevant robustness tests based on the protocol proposed by Oana and Schneider (Reference Oana and Schneider2021).
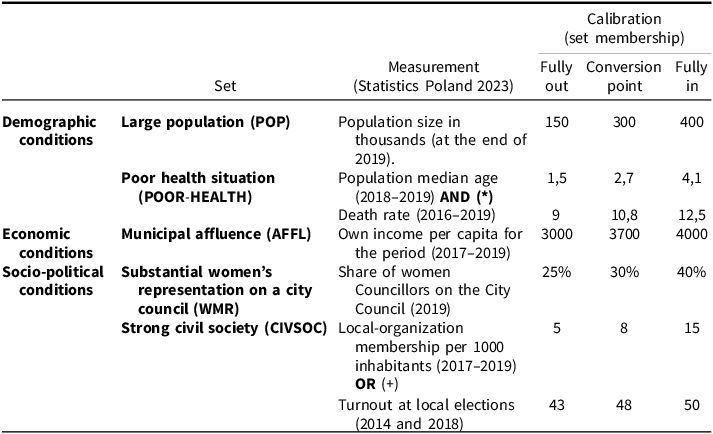
For example, to measure municipal affluence, income per capita data were utilized. To account for possible fluctuations due to the electoral cycle, an average income was calculated over three consecutive years (2017–2019). The conversion point was set slightly above the mean value for the chosen cases. Similarly, the dichotomous set containing cases with a high share of women among local councillors (above 30%) was based on the average seats held by women in this period. The conversion point corresponds to the concept of substantial representation, as used by international organizations to promote gender-based quotas in government (Dahlerup Reference Dahlerup, Ballington and Karam2005). On the other hand, the population size was measured as of the end of 2019, since it does not tend to vary sharply on a year-to-year basis. To ensure adequate coverage, the set of the largest cities includes municipalities that had at least 300,000 inhabitants – above the median and below the mean among the chosen city counties. All included cases would also be classified as “large” in official statistics (Statistics Poland 2018), so cities included in the set are the largest municipalities in the country. Calibration choices are summarized in Table 2.
Operationalization and calibration choices

Source: author’s own elaboration.
As QCA allows the combination of individual conditions into higher-order concepts (see Oana et al. Reference Oana, Schneider and Thomann2021), a conjunction and disjunction of sets were created to measure social capital and assess the existing health situation in municipalities. For population health, the conjunction of high median age in 2019 (above the mean of 42.9) and above-average death rate between 2016 and 2019 (greater than 10.9 per 1000 inhabitants) defines a city as having a relatively “unhealthy” population. The death rate is a standard indicator of population health, while median age is a summary measure of the population’s age structure – an aspect that goes far in predetermining the profile of health needsFootnote 1 (see Ritchie and Roser Reference Ritchie and Roser2019). A disjunction of above-average participation rate in local organizations between 2017 and 2019 (greater than 8.4 per 1000 inhabitants) and high turnout at 2014 and 2018 local elections identifies cases with a “strong civil society,” that is, the other higher-order set. Participation in local elections in Poland has recently been linked to social embeddedness (Markowski et al. Reference Markowski, Żerkowska-Balas and Stanley2023), while indicators of local civil society are commonly used in the measurement of social capital (most famously by Putnam et al. Reference Putnam, Leonardi and Nanetti2001). In the created conjunction, both indicators must be present to label the health situation as “poor,” whereas in the disjunction only one of the described conditions is required to be present for the concept to apply (Oana et al. Reference Oana, Schneider and Thomann2021). In sum, the conjunction makes the measurement of the health situation more selective, while the disjunction for “strong civil society” renders it more inclusive compared to the use of a single indicator.
Operationalization and calibration of some conditions, such as the strength of local civil society, were impeded by data availability and quality (e.g., missing data). For higher-order concepts described above, additional indicators were used to enhance measurement precision. Potential measurement validity issues were also further addressed in the robustness tests. Using the Oana and Schneider protocol (Oana and Schneider Reference Oana and Schneider2021), alternative indicators and conversion points for selected conditions were retested and compared with the initial analysis to detect potential inconsistencies. The robustness metrics, presented in Appendix B, indicate that alternative specifications resulted in similar QCA outcomes, supporting the primary operationalization choices.
Results
The analysis of necessity reveals that no individual condition is necessary for the occurrence or absence of universal targeting in municipal public health policy among the selected cities (see Table A3 in Appendix A). No economic, demographic, or socio-political condition shows the needed consistency to be considered necessary (>0.9; Oana et al. Reference Oana, Schneider and Thomann2021). However, two combinations of conditions met the criteria of empirical relevance, suggesting that they could be regarded as potential prerequisites for the absence of universal targeting. That said, as these combinations are not equivalents of any higher-order theoretical concepts and only address the non-presence of the phenomenon, they remain largely uninterpretable on their own according to the existing methodological guidelines (cf Schneider Reference Schneider2019).
Conditions of universal targeting (OUT)
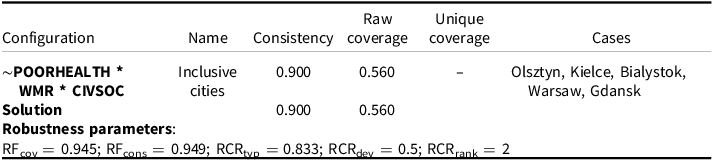
The analysis of sufficiency constituted the second step of the procedure. The conducted analysis reveals only one distinct configuration consistently linked to the presence of universal targeting in the selected municipalities (OUT), as presented in Table 3. This group includes cities both medium-sized cities (Olsztyn, Kielce, and Bialystok) and larger metropolitan areas (Warsaw and Gdansk). In these cases, the absence of relatively poor population health coincided with the presence of high levels of social capital and substantial representation of women in local politics. One deviant case is also part of the solution, namely Gdynia. There, the combination of conditions implying the presence of universal targeting coincides with its absence, contrary to the solution formula.
Sufficient combinations of conditions for universal targeting (intermediate solution)

Source: author’s own elaboration. The crossed-out cities are deviant cases (consistency in kind).
Note: “*” denotes “AND”, while “∼” stands for the absence of a condition. PRI score for the solution: 0.815. For elaboration on robustness parameters see Appendix B.
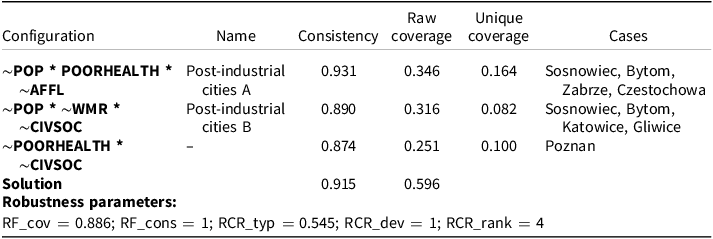
Conditions of the absence of universal targeting (∼OUT)
A separate analysis of sufficiency for the absence of universal targeting in municipal public health policy produced three consistent combinations of conditions (see Table 4). Given that causal claims in set-theoretic methods are made only for the presence of a given phenomenon (the: positive pole of concepts,” in line with Beach and Pedersen Reference Beach and Pedersen2019, p. 62), the lack of well-funded universal targeting should be treated as a broad presence of non-universal targeting in all its shapes and forms. The first two configurations contain cities mostly located in the same region, the Silesian voivodship. They are characterized by a comparatively smaller population and, in some cases, by poor health indicators. Poznan, a large and affluent city, is the sole (non-deviant) representative of the last combination, where a non-universal municipal public health policy is also observed. Its most striking characteristic, indicated by fuzzy scores, is the relative lack of high levels of social capital.
Sufficient combinations of conditions for the absence of universal targeting (intermediate solution)

Source: author’s own elaboration. The crossed-out cities are deviant cases (consistency in kind).
Note: “*” denotes “AND”, while “∼” stands for the absence of a condition. PRI score for the solution: 0.865. For elaboration on robustness parameters see Appendix B.
Discussion and conclusions
The main aim of this article was to examine how structural conditions, previously found to influence local policymaking, interact to create combinations that coincide with the presence or absence of universal targeting in public health policies across Poland’s 23 largest cities. Universal targeting was defined here as the predominance of well-funded public health programs offered to large groups of beneficiaries, whereas non-universal targeting referred to cases where such programs were largely absent. Drawing on the Local Welfare Regimes perspective of Andreotti and Mingione, as well as on the literature review, expectations were formulated that universal targeting would be present in places characterized by a combination of several factors: a large population, general affluence, unhealthy population, substantial representation of women in city councils, and strong civil society. Consequently, these conditions were included in the comparative analysis that utilized fuzzy-set Qualitative Comparative Analysis (fsQCA). Overall, the findings indicate that the presence of universal targeting in local public health policy reflects not only a younger and healthier population but also broader local governance factors.
In particular, the results of this study show the consistent role of the combination of substantial representation of women in local politics and strong civil society in driving the presence of well-funded and universally targeted public health policies in Poland’s largest cities. This finding is consistent with broader scholarship that emphasizes the impact of these factors in shaping social and public health policies and the Local Welfare Regimes perspective (e.g., Baum Reference Baum1999; Bolzendahl and Brooks Reference Bolzendahl and Brooks2007; Funk and Philips Reference Funk and Philips2019; Hawe and Shiell Reference Hawe and Shiell2000; Johansson and Koch Reference Johansson, Koch, Johansson and Koch2016). To be specific, it mirrors Vivien Lowndes’ conclusions that women’s representation and social capital reinforce each other, as women are more likely to draw upon social capital as a political resource, which has a direct positive impact on participatory local policymaking (Lowndes Reference Lowndes2004). These dynamics, when combined with favorable conditions like the absence of poor population health, seem to support the emergence of universal targeting in local public health. In Table 3, this configuration is referred to as including “inclusive cities,” because it showcases the institutional environment fostering participatory development of local public health policies. While the evidence for the tendency of women councillors to be more supportive of care-related policies (Andersen et al. Reference Andersen, Bulte, Gneezy and List2008; but see Martínez-Córdoba et al. Reference Martínez-Córdoba, Benito and García-Sánchez2023) or their more agreeable behavior once elected (Swift and VanderMolen Reference Swift and VanderMolen2021, but see Lawless et al. Reference Lawless, Theriault and Guthrie2018) remains mixed, the consistent presence of the combination of substantial representation of women in city councils and strong civil society observed in this article stresses its relevance in the domain of public health.
At the same time, the combination of universal targeting with high collective-health scores runs contrary to the formulated directional expectation and challenges the view that local governments tend to accommodate needs of the population with increased social commitments (Feiock and West Reference Feiock and West1993; Guldbrandsson et al. Reference Guldbrandsson, Bremberg and Bäck2005; Hajnal and Trounstine Reference Hajnal and Trounstine2010). This provides an argument for the role of population health to be reconsidered in the examined context and signals the potential presence of the Matthew Effect across the investigated cities (cf Babić and Šućur Reference Babić and Šućur2022; Bonoli and Liechti Reference Bonoli, Liechti, Busemeyer, de la Porte, Garritzmann and Pavolini2020). Hence, for the absence of poor population health, it may be speculated that a comparatively healthy population is in itself a product of path dependency and feedback effects – i.e. well-funded programs, local development, and general trends that existed before 2019. Alternatively, the existing universal programs could have been implemented in a proportionate manner, addressing the needs of the most vulnerable groups through selective actions and reflecting a more balanced approach to public health. This speculation is further supported by the fact that universal targeting appears to be combined with the presence of at least some forms of residual policies. For instance, 19 selectively-targeted programs were implemented in Kielce, and as many as 128 in the case of Gdansk. Indeed, both factors could contribute to the absence of an unhealthy population.
Since QCA is an iterative research method, further examination of cases is crucial to contextualize the comparative findings. In light of case-specific knowledge, the nature of universal targeting in municipal public health programs appears even more complex. Whereas such programs cover large numbers of citizens, they remain primarily focused on health promotion efforts. These actions typically include workshops held in schools, designed to influence children’s long-term health behaviors. The city of Gdansk serves here as an emblematic case, as it is a robust typical case in light of the post-QCA assessment of the results (it remains typical even against major changes in calibration choices; see Appendix B). In 2019, local authorities in Gdansk funded 90 universal programs, of which a majority (68) were dedicated to health education in schools, including among disadvantaged children. Similar patterns were observed in Kielce and Bialystok. Although limited to only a few municipalities, these findings suggest that universal targeting in Poland’s largest cities aligns with a more general preference for funding health promotion efforts.
Interpreting the absence of well-funded universal targeting remains more challenging. The heterogeneity of non-universal policy across the selected cities and the low level of unique coverage of the individual configurations limit the interpretation of the findings for the “negative pole” (absence) of the investigated concept. Nevertheless, such absence is linked to several combinations of conditions. Interestingly, the majority of observations characterized by the absence of universal targeting are located in the Upper-Silesian conurbation, a sub-region of several medium-sized municipalities located in close proximity (configurations referred to as “Post-industrial” A and “Post-industrial B” in Table 4). The potential to scale up public health programs remains constrained in these cases by the existing administrative divisions. This possible negative impact of institutional fragmentation on public health policymaking mirrors the conclusions of social policy scholars in other policy contexts (see e.g., Bifulco Reference Bifulco2016). According to the same QCA results, the structure of health needs (“unhealthy population”) is also associated in a consistent manner with the absence of universal targeting in public health policy. As Silesia was traditionally an industrial region dominated by coal mining and heavy industry, the poor population health context must be regarded as a direct product of its historical circumstances and path dependency – as evidenced in mortality statistics. The Silesian cities discussed had an average death rate of some 11.89, while for all the cases representing “universal targeting” group the corresponding figure was of around 10.01 per 1000 inhabitants (calculated for the period between 2016 and 2019, excluding deviant cases). Therefore, in cities with higher health risks, more universal and better-financed policy was not pursued.
Given its outlier status, Gdynia warrants further investigation, particularly due to its geographical proximity to Gdansk. Both cities belong to the same metropolitan area (the “Tri-City”) and share many important structural characteristics, even as they differ in the predominant design of municipal public health policy. Prior studies suggest that mayors of both cities have consistently pursued different leadership styles and competing policy objectives in other areas (Sagan Reference Sagan2014). Future in-depth comparisons could therefore explain differences existing in the Tri-City, as well as in Upper Silesia, e.g., by employing case study methods like process tracing.
The main theoretical contributions that arise from this study relate both to the concept of universal targeting and the broader development of the Local Welfare Regimes perspective. Regarding the former, the findings confirm the view, expressed recently by various authors in other contexts (Carey et al. Reference Carey, Crammond and De Leeuw2015; Francis-Oliviero et al. Reference Francis-Oliviero, Cambon, Wittwer, Marmot and Alla2020; Jacques and Noël Reference Jacques and Noël2021), that universal targeting can find implementation in a variety of ways, ranging from rudimentary to more generous and proportionate. In expanding our understanding of universal targeting through the LWR perspective, the analysis also indicates that local public health policymakers in Poland do not adhere to a single policy design. Instead, they prioritize a combination of universal and non-universal targeting in pursuing policy objectives. The findings on the hybridity of local policies in this domain confirm the observation by Giovanni Bertin and Marco Carradore that the diversification process within welfare states occurs both on the local scale and at the level of specific welfare policies (Bertin and Carradore Reference Bertin and Carradore2016).
The fuzzy scores also point to this, as does further case analysis and the conservative solution of QCA (minimized without logical reminders; that is, configurations that are null but possible, presented in Tables A4 and A5 in Appendix A). These results reveal at least two subtypes for universal targeting configurations. Affluent and populous metropolises, Warsaw and Gdansk, exemplify a more generous subtype of universal targeting, where well-funded universal programs were complemented with a diverse number of selective (residual) public health interventions. Smaller, less affluent city counties like Olsztyn, Kielce, and Bialystok face greater obstacles to upscaling municipal public health actions. As outlined in the theoretical section of this article, the former, more generous arrangement is referred to as “proportionate universalism” by public health scholars (Carey et al. Reference Carey, Crammond and De Leeuw2015). By contrast, in the latter subtype, the authorities could only implement a few dozen programs overall, even though they had access to financial resources (Bialystok – 34, Olsztyn – 5 and Kielce – 31; cf Warsaw – 293 and Gdansk – 220). The findings thus suggest that universal targeting – like universalism per se – can be generous (proportionate) or not (non-proportionate), as should be expected from the public health literature (see Carey et al. Reference Carey, Crammond and De Leeuw2015; Marmot et al. Reference Marmot, Allen, Goldblatt, Boyce, McNeish, McNeish and Geddes2010).
The analysis thus extends the Local Welfare Regimes perspective by bringing to light divergent sources of territorial inequities arising from decentralized policy arrangements. While such inequalities were previously connected mainly to characteristics of supply-side conditions, such as overall fiscal capacity or income (see the seminal work by Andreotti and Mingione Reference Andreotti and Mingione2016), the present findings indicate the importance of demand-side factors – particularly population health status alongside other place-based determinants. The QCA results therefore show that municipalities with relatively better population health scores, when combined with other social factors, tend to implement universally targeted and well-financed preventive policies. As stated earlier, these patterns could reinforce existing health disparities, consistent with Matthew Effects in other policy areas (Babić and Šućur Reference Babić and Šućur2022; Bonoli and Liechti Reference Bonoli, Liechti, Busemeyer, de la Porte, Garritzmann and Pavolini2020). Integrating these insights into the LWR perspective advances the theory by showcasing the role of specific interactions between supply – and demand – conditions in shaping particular policy domains.
Furthermore, the analysis demonstrates the potential of combining the LWR perspective with QCA. It emphasizes that different types of municipal targeting in public health policy are produced by heterogenous sets of conditions; i.e. causal asymmetry. This approach enabled the identification of numerous unique mixes of determinants and public health policies across a medium number of cases, expanding the traditional application of the LWR perspective beyond small-N investigations (Johansson and Koch Reference Johansson, Koch, Johansson and Koch2016; Łukasiewicz et al. Reference Łukasiewicz, Oren and Tripathi2023). In consequence, the analytical strategy proved effective in highlighting the complex pathways that municipalities follow in their implementation of universal (or non-universal) targeting in public health policy and in measuring the investigated outcome using a fuzzy-set family resemblance concept formation strategy. This indicates that analyses of Local Welfare Regimes can be conducted in various policy contexts and need not be limited to a small number of cases.
The presented study also offers several practical implications for policymakers, above all regarding the fragmentation of public health governance in metropolitan areas (in Poland’s case, e.g., Upper Silesia and Tri-City). Fragmentation can divide resources between competing municipalities, hindering potential coordination. The results suggest fostering cross-municipal partnerships and renewed engagement with local civil society in implementing bottom-up public health interventions, as cities with the most developed policies invested heavily in third-sector engagement.
Study limitations
This study faced several limitations. The employed method – fsQCA – has several shortcomings, as pointed out by its critics (e.g., Tanner Reference Tanner2014). It detects regularities but is limited in establishing causal links on its own. Compared to standard quantitative methods, its findings are also less generalizable, and it remains sensitive to researchers’ choices in set calibration. Recent methodological developments, like the robustness tests protocol (Oana and Schneider Reference Oana and Schneider2021), address some of these concerns. Nonetheless, fuzzy-set QCA offers several key advantages in the present context. It assumes that causal processes are often asymmetric and idiosyncratic, so it aligns uniquely well with the central claim of the LWR theory – to the effect that local policy is highly heterogeneous, context-dependent, and cannot be fully explained by referring to singular and isolated factors affecting policy decisions (cf Andreotti and Mingione Reference Andreotti and Mingione2016). Therefore, the theoretical assumptions of the analysis remain consistent with the epistemology of QCA. Likewise, employing fuzzy sets allows for a hybrid measurement of the universal targeting concept, combining both qualitative and quantitative features. This is crucial for capturing its complexity and non-monetary dimensions. Finally, the employed methodological approach proved effective in overcoming data limitations that would constrain quantitative methods. Follow-up qualitative studies, especially of outlier cities, would further strengthen the validity of the findings and could employ methods such as process tracing or traditional case studies.
The case selection strategy (MSSD) and the limited number of selected cases within a single national context (Poland) also constrain the external validity of the findings. Data availability limited measurement of universal targeting in municipal policies to a single pre-pandemic year (2019). However, although the chosen case selection strategy restricts generalization to some extent, it was crucial for delimiting conditions in the QCA context and ensured better case comparability. Some measurement issues were further mitigated using the Oana and Schneider (Reference Oana and Schneider2021) robustness tests protocol.
Despite these limitations, the comparison provides novel insights into an understudied policy area and the concept of universal targeting while integrating for the first time the Local Welfare Regimes perspective with a configurative set-theoretic method (QCA) in the domain of public health policy. Future research should aim to extend and verify these findings in cross-national settings. Contexts warranting additional comparative attention include other decentralized countries in the region and beyond, particularly post-socialist states, where local administrative units play a significant role in shaping preventive policies. The influence of partisan conditions on municipal public health policymaking should also be addressed, given that this important dimension fell beyond the scope of this study due to case selection and inconsistent preliminary QCA results.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0143814X26101007
Data availability statement
Replication materials are available in the Journal of Public Policy Dataverse at https://doi.org/10.7910/DVN/YMUVN2.
Acknowledgements
I would like to extend my sincere gratitude to my supervisor, Maria Theiss, for her mentorship throughout this project. I am also thankful to Rossella Ciccia, who helped develop this work during my research stay at the University of Oxford (generously supported by the University of Warsaw’s IDUB scheme). Finally, my thanks go to the experts – including faculty colleagues – who provided crucial feedback during my presentations at several meetings, conferences, and workshops, notably during the QCA PDW 2023 in Antwerp and the 21st ESPAnet Annual Conference 2023 in Warsaw.
Funding statement
This research was funded by the National Science Centre, Poland (grant number: 2022/45/N/HS5/00531).
Competing interests
I have no conflicts of interest to disclose.





 Open access
Open access