



Impact statements
Our study addresses a neglected subject of investigation: the ethnoracial inequalities in suicide risk among young people exposed to interpersonal violence. Suicide risk factors do not operate in a vacuum; therefore, public policies must be directed toward those who need them most. We found that interpersonal violence was strongly associated with suicide risk among low-income youth in Brazil. Notably, the risk was 10.7 times higher among Indigenous youth and 3.14 times higher among Black youth, whereas the association was not significant among White youth. These findings reveal ethnoracial disparities in the association between interpersonal violence exposure and suicide risk in young populations and emphasize the urgent need for interventions that promote health equity and address structural racism.
Introduction
Suicide is one of the leading causes of death among adolescents and young adults worldwide and in Brazil (GBD, 2021 Suicide Collaborators 2025; Malta et al., Reference Malta, Minayo, Cardoso, Veloso, Teixeira, Pinto and Naghavi2021). Among the risk factors for suicide, interpersonal violence is a well-established one in adults (Goldman-Mellor and Qin, Reference Goldman-Mellor and Qin2024). However, its association among young people is less established (Smith et al., Reference Smith, McDermott, Jacob, Barnett, Butler, Shin and Koyanagi2020). Experiencing interpersonal violence, whether physical, sexual or psychological, has been linked to poor mental health outcomes in young people, including mental disorders (Fidalgo et al. Reference Fidalgo, Sanchez, Caetano, Andreoni, Sanudo, Chen and Martins2018; Quinlan-Davidson et al., Reference Quinlan-Davidson, Kiss, Devakumar, Cortina-Borja, Eisner and Peres2021; Grummitt et al., Reference Grummitt, Baldwin, Lafoa’i, Keyes and Barrett2024; Lee et al., Reference Lee, Wolke, Bärnighausen, Ouermi, Bountogo and Harling2024), psychiatric hospitalization (Stewart et al., Reference Stewart, Semovski and Lapshina2024; Toledo et al., Reference Toledo, Rodrigues, Alves, Guedes, de Araújo, Naslund, Barreto, Patel and Machado2024) and suicidal behaviors (Miranda-Mendizabal et al., Reference Miranda-Mendizabal, Castellví, Parés-Badell, Alayo, Almenara, Alonso, Blasco, Cebrià, Gabilondo, Gili, Lagares, Piqueras, Rodríguez-Jiménez, Rodríguez-Marín, Roca, Soto-Sanz, Vilagut and Alonso2019; Grummitt et al., Reference Grummitt, Baldwin, Lafoa’i, Keyes and Barrett2024), which may increase their risk of suicide. However, the impact of interpersonal violence and its associated traumas is not uniformly distributed across populations. Black populations, Indigenous communities, and also minoritized groups such as migrants have been disproportionately affected by Interpersonal violence (Wanzinack and Mélo, Reference Wanzinack and Mélo2025).
In Brazil, these inequities are particularly stark. In 2023, individuals identified as Black accounted for nearly 77% of homicides. Moreover, homicide rates were 2.7 times higher among Black populations than among non-Black populations. These disparities are even more pronounced among adolescents and young adults, who are disproportionately exposed to violence in contexts shaped by socioeconomic disadvantage and structural marginalization. Furthermore, Black Brazilians face elevated risks of lethal encounters with state actors, including police violence, which further compounds cumulative exposure to violence and amplifies vulnerability to adverse mental health and suicide-related outcomes (‘Ipea - Atlas da Violência v.2.8 - Atlas da Violência 2025’, 2025).
Shaped by a convergence of structural, social and psychological determinants of health, structural racism and interpersonal discrimination, combined with conditions such as neighborhood segregation, socioeconomic disadvantage and limited social support, expose these groups to unique stressors that may heighten their risk of suicide (Bernard et al., Reference Bernard, Smith and Lanier2022). Although, as previously mentioned, studies on the association between exposure to interpersonal violence and suicide among young people are scarce (Fedina et al., Reference Fedina, King, DeVylder and Herrenkohl2023), reports addressing ethnoracial inequities are even rarer.
Suicide among young people has increased markedly. In Brazil, between 2011 and 2022, suicide rates grew 6.14% (95% CI: 4.57–7.88) among those aged 10–24 years (Alves et al., Reference Alves, Fialho, de, Naslund, Barreto, Patel and Machado2024). Indigenous youth (10–24 years) have consistently shown the highest suicide rates between 2000 and 2020 (de Araújo et al., Reference de Araujo, Fialho, Alves, Cardoso, Orellana, Naslund, Barreto, Patel and Machado2023). Between 2011 and 2017, more than half of all suicides among young people aged 15–29 years occurred among Black individuals (Brasil, 2025). Despite these patterns, there is limited evidence on whether exposure to interpersonal violence contributes to ethnoracial inequalities in suicide risk among young people. Previous studies on young people’s violence exposure and mental health-related outcomes have largely examined suicidal ideation (Polanco-Roman et al., Reference Polanco-Roman, Alvarez, Corbeil, Scorza, Wall, Gould, Alegría, Bird, Canino and Duarte2021; Areba et al., Reference Areba, Mathiason, Jewett, Taliaferro and Borowsky2025; Chipalo and Jeong, Reference Chipalo and Jeong2025; Shahsavar and Choudhury, Reference Shahsavar and Choudhury2025), suicide planning (Sharpless et al., Reference Sharpless, Alvarez, Kershaw and Willie2025) and suicide attempts (Polanco-Roman et al., Reference Polanco-Roman, Alvarez, Corbeil, Scorza, Wall, Gould, Alegría, Bird, Canino and Duarte2021; Areba et al., Reference Areba, Mathiason, Jewett, Taliaferro and Borowsky2025; Chipalo and Jeong, Reference Chipalo and Jeong2025; Shahsavar and Choudhury, Reference Shahsavar and Choudhury2025), but rarely suicide itself. Even fewer studies, most of them in the United States, have assessed racial inequalities in suicide risk (Areba et al., Reference Areba, Mathiason, Jewett, Taliaferro and Borowsky2025; Sharpless et al., Reference Sharpless, Alvarez, Kershaw and Willie2025).
Understanding ethnoracial inequalities in suicide risk, especially in the context of exposure to interpersonal violence, is crucial for addressing socially driven health disparities rooted in structural and systemic inequities. Using population-based data from the 100 Million Brazilian Cohort, we aimed to examine racial disparities in the association between interpersonal violence exposure and suicide, framing our analysis through an equity lens and acknowledging that these disparities are shaped by structural determinants of health.
Methods
Study design and data sources
This nationwide longitudinal study used data from the 100 Million Brazilian Cohort (Barreto et al., Reference Barreto, Ichihara, Pescarini, Ali, Borges, Fiaccone, R de C, Teles, Almeida, Sena, Carreiro, Cabral, Almeida, Barbosa, Pita, Barreto, Mendes, Ramos, Brickley, Bispo, Machado, Paixao, Rodrigues and Smeeth2022) linked with the Notifiable Diseases Information System (SINAN) (2011–2018), the National Hospital Information System (SIH) and the Mortality Information System (SIM). The 100 Million Brazilian Cohort (Barreto et al., Reference Barreto, Ichihara, Pescarini, Ali, Borges, Fiaccone, R de C, Teles, Almeida, Sena, Carreiro, Cabral, Almeida, Barbosa, Pita, Barreto, Mendes, Ramos, Brickley, Bispo, Machado, Paixao, Rodrigues and Smeeth2022), established by the Centre for Data and Knowledge Integration for Health (CIDACS) (Barreto et al., Reference Barreto, Ichihara, Almeida, Barreto, Cabral, Fiaccone, Carreiro, Teles, Pitta, Penna, Barral-Netto, Ali, Barbosa, Denaxas, Rodrigues and Smeeth2019), is a dynamic cohort created through data linkage between the Unified Registry for Social Programs (CadÚnico) and the Brazilian Health Information Systems. CadÚnico eligibility requires per capita monthly family income ≤half the minimum wage or familial income up to three minimum wages (Barreto et al., Reference Barreto, Ichihara, Almeida, Barreto, Cabral, Fiaccone, Carreiro, Teles, Pitta, Penna, Barral-Netto, Ali, Barbosa, Denaxas, Rodrigues and Smeeth2019, Reference Barreto, Ichihara, Pescarini, Ali, Borges, Fiaccone, R de C, Teles, Almeida, Sena, Carreiro, Cabral, Almeida, Barbosa, Pita, Barreto, Mendes, Ramos, Brickley, Bispo, Machado, Paixao, Rodrigues and Smeeth2022). At baseline (2011–2018), the cohort comprised over 131 million individuals from ~35 million families (Barreto et al. Reference Barreto, Ichihara, Pescarini, Ali, Borges, Fiaccone, R de C, Teles, Almeida, Sena, Carreiro, Cabral, Almeida, Barbosa, Pita, Barreto, Mendes, Ramos, Brickley, Bispo, Machado, Paixao, Rodrigues and Smeeth2022). Unlike the general Brazilian population, the cohort is overrepresented by children and young people. In terms of race/skin color and sex, however, the cohort mirrors the Brazilian general population, which is predominantly composed of Black individuals, which is the sum of individuals self-declared as Black and Pardas (Brown), and women (IBGE, Censo 2022, 2023).
Since 2011, it has been mandatory to record reports of violence from all healthcare services in Brazil, including both public and private services, in SINAN. The SINAN reports suspected or confirmed cases of violence and must be completed by healthcare-trained health professionals (TABNET – DATASUS, n.d.). Hospitalization data were obtained from the SIH, which includes hospital admissions funded by Brazil’s Unified Health System (SUS) (TABNET – DATASUS, n.d.). SIH records hospitalizations financed through SUS or by private hospital providers contracted by the SUS. Thus, it is possible that all individuals in the cohort are represented, given that the population is predominantly low-income and primarily relies on SUS for healthcare. SIH/SUS is estimated to cover ~75% of all hospitalizations in Brazil, with the remainder occurring exclusively in private settings not recorded in this database (‘Painel de Indicadores – PNS’, n.d.). Because a person hospitalized after a violent incident may also have a notification in SINAN, duplicates are possible; to avoid double-counting, records appearing in both systems were identified and removed before analysis. SIM is a nationwide information system for recording mortality data, encompassing all deaths in the country and their causes (TABNET – DATASUS, n.d.). Deaths were recorded according to the 10th revision of the International Classification of Diseases (ICD-10).
Data linkage
The linkage between the 100 Million Brazilian Cohort (100MCohort) baseline and health datasets occurred through a two-step process based on five individual-level identifiers (name, date of birth, sex, name of the mother and municipality of residence) using the CIDACS record linkage tool (Barbosa et al., Reference Barbosa, Ali, Araujo, Reis, Sena, Ichihara, Pescarini, Fiaccone, Amorim, Pita, Barreto, Smeeth and Barreto2020). Initially, entries were linked based on exact matching. Subsequently, entries that did not achieve deterministic linkage were connected based on pairwise similarity scores. The assessment of data linkage accuracy involved a manual validation process that examined a randomly chosen subset of records. This evaluation included an analysis of the receiver operating characteristic curve (ROC), measuring sensitivity and specificity indexes. The average sensitivity and specificity exceeded 92% during this validation procedure (Barbosa et al., Reference Barbosa, Ali, Araujo, Reis, Sena, Ichihara, Pescarini, Fiaccone, Amorim, Pita, Barreto, Smeeth and Barreto2020).
Study population, eligibility criteria and follow-up
We included individuals aged 10–29 years at baseline enrollment in the 100MCohort (January 1, 2011–December 31, 2018). Participants were followed from their baseline entry date until the earliest occurrence of three events: outcome (suicide), other death or the administrative censoring date of December 31, 2018. Baseline was defined as the date of first registration in the Cadastro Único, ensuring updated socioeconomic information and appropriate temporal alignment between covariates, exposures and outcomes. To preserve temporal ordering and minimize bias, individuals with records of self-harm or psychiatric hospitalization before cohort entry were excluded. Also, duplicate records were removed. Individuals with more than one psychiatric hospitalization were excluded to maintain comparability across first-event analyses. In addition, self-harm events recorded on the same date as suicide were excluded to reduce the risk of exposure misclassification.
Exposure and outcome
The exposure in this study was interpersonal violence victimization, measured using the SINAN-Violence database, part of Brazil’s Violence Surveillance System (‘TabNet Win32 3.3: VIOLÊNCIA INTERPESSOAL/AUTOPROVOCADA – Brasil’, n.d.) and the SIH. Within SINAN-Violence, interpersonal violence is defined as the intentional use of physical force or power against another person that results in physical pain, psychological distress or humiliation. We considered all types of interpersonal violence victimization recorded in SINAN-Violence. For hospitalizations due to interpersonal violence, we considered ICD-10 codes X85 to Y09. For the present analyses, only the first registered episode of interpersonal violence recorded in SINAN or SIH during the study period was included. The outcome was suicide, defined as death from intentional self-harm (ICD-10 codes X60–X84) (‘ICD-10 Version:2019’, n.d.).
Statistical analysis
Descriptive analyses included absolute and relative frequencies for categorical covariates and means with standard deviations for continuous covariates. We estimated the suicide rates as the number of suicide deaths per 100,000 person-years at risk, along with 95% CIs (overall and by ethnoracial group).
To examine the association between interpersonal violence and suicide, we conducted multivariable Cox proportional hazards regression analyses. The models were adjusted for the following baseline covariates: age (10–14, 15–19, 20–24 and 25–29 years); sex (male or female); household size (1–2, 3–4 and ≥5 members); education level of the oldest household member (never attended school, preschool, primary or less, junior high, high school and college/university); employment status of the oldest household member (yes or no); area of residence (urban or rural); and region of residence (Central-West, North, Northeast, South and Southeast). Household conditions were summarized in a composite variable based on access to public services (treated piped water, sanitation, electricity and garbage collection) and housing material (brick construction). This variable ranged from 0 to 5, with 0 indicating the absence of all factors and 5 indicating the presence of all factors.
We also included prior self-harm and psychiatric hospitalizations as covariates in the models, as these are well-recognized confounders of suicide in the literature (Tidemalm et al., Reference Tidemalm, Långström, Lichtenstein and Runeson2008; Whiting et al., Reference Whiting, Lichtenstein and Fazel2021) and were associated with both the exposure and the outcome in our study population (Supplementary Table S1). Self-harm events were identified from two sources: SINAN-Violence notifications and SIH hospitalization records. According to the Brazilian Ministry of Health definitions, a self-harm notification was recorded when the field “Was the injury self-inflicted?” was marked “Yes” and the perpetrator–victim relationship indicated “the person themselves.” Hospitalizations for self-harm were defined using ICD-10 codes X60–X84, and the earliest episode captured in either source was included in the analyses. In addition, we considered prior hospitalization for mental disorders (yes/no) and identified from the first record during follow-up in which the primary diagnosis was classified under ICD-10 codes F00–F99.
Stratified Multivariate Cox regression models with extended specification were used to estimate HRs with 95% CIs (Therneau, Reference Therneau, Lin and Fleming1997; Therneau and Grambsch, Reference Therneau and Grambsch2000). Further information can be found in the Supplementary Material (Supplementary Table S2). We used Kaplan–Meier survival curves to estimate time-to-event outcomes by ethnoracial group and compared survival functions across groups.
To assess the robustness of the findings, we performed a sensitivity analysis excluding the co-variables for psychiatric hospitalization and prior self-harm from the statistical models, given their well-established role as strong risk factors for suicide, to determine whether associations persisted in their absence. Furthermore, due to the limited number of events in some categories, we fitted models adjusted only for age and sex to test potential collinearity in the fully adjusted models and to verify the consistency of the results (Supplementary Tables S3–S7). We also re-fitted the same models, stratified by race/skin color, using self-harm as the outcome to examine whether the associations between exposure to interpersonal violence and suicidal behaviors persisted across racial and ethnic categories when self-harm was considered as an alternative outcome (Supplementary Table S8). Finally, to evaluate potential effect heterogeneity by race/skin color, we fitted the overall models with and without race/skin color as a covariate and, in addition, included multiplicative interaction terms between exposure to interpersonal violence and race/skin color. Interaction was formally tested using Wald tests (testparm) (Supplementary Tables S9–S11).
Analysis of ethnoracial inequalities
Considering that understanding the relationship between exposure to interpersonal violence and suicide across racial groups is essential for identifying socially driven health inequalities, we performed comparative analyses by race. Self-reported race was used as a proxy for exposure to structural racism and its systemic effects (Williams et al., Reference Williams, Lawrence and Davis2019; Braveman and Parker Dominguez, Reference Braveman and Parker Dominguez2021; Lett et al., Reference Lett, Asabor, Beltrán, Cannon and Arah2022), as previous studies conducted with the 100MCohort (Rebouças et al., Reference Rebouças, Goes, Pescarini, Ramos, Ichihara, Sena, Veiga, Rodrigues, Barreto and Paixão2022, Reference Rebouças, Paixão, Ramos, Pescarini, Pinto-Junior, Falcão, Ichihara, Sena, Veiga, Ribeiro, Rodrigues, Barreto and Goes2024; Paixao et al., Reference Paixao, Ferreira, Pescarini, Wong, Goes, Fiaccone, de, Reboucas, Cardoso, Smeeth, Barreto, Rodrigues and Ichihara2023). Differences in outcomes across these categories are understood to result from social determinants rather than biological or cultural factors, as race is a socially constructed concept created to hierarchize people based on their phenotypic characteristics rooted in racism (Williams and Mohammed, Reference Williams and Mohammed2013; Williams et al., Reference Williams, Lawrence and Davis2019; Braveman and Parker Dominguez, Reference Braveman and Parker Dominguez2021; Hamed et al., Reference Hamed, Bradby, Ahlberg and Thapar-Björkert2022). This approach aligns with the theoretical framework that systemic racism influences the distribution of resources, access to healthcare and health outcomes, often reflected in Brazil through phenotypic characteristics such as skin color (Jones, Reference Jones2000; Werneck, Reference Werneck2016; Hamed et al., Reference Hamed, Bradby, Ahlberg and Thapar-Björkert2022; Lett et al., Reference Lett, Asabor, Beltrán, Cannon and Arah2022; Rebouças et al., Reference Rebouças, Goes, Pescarini, Ramos, Ichihara, Sena, Veiga, Rodrigues, Barreto and Paixão2022; Paixao et al., Reference Paixao, Ferreira, Pescarini, Wong, Goes, Fiaccone, de, Reboucas, Cardoso, Smeeth, Barreto, Rodrigues and Ichihara2023).
In Brazil, race is self-declared and classified into five categories: Pretas /Black, Parda/Brown, Indigenous, Asian descent and White (Anjos, Reference Anjos2013; ‘Painel Cor ou Raça’, n.d.). Pretas/Black and Pardas/Brown categories were combined to reflect the socio-political category of the “Black population,” which can be used as an analytic group, in line with Brazil’s National Policy for the Health of the Black Population (‘Política Nacional de Saúde da População Negra 3a edição, 2017). Suicide is a rare event, and due to limited sample sizes, which resulted in model nonconvergence, it was not possible to analyze Asian descendant groups. Further details are provided in the Supplementary File (Supplementary Table S12).
The analysis was conducted using R version 4.1.2 and Stata version 15.1. Ethical approval for this study was obtained from Centro de Pesquisas Gonçalo Moniz, Fundação Oswaldo Cruz, Bahia (CAAE: 84842624.4.0000.0040).
Results
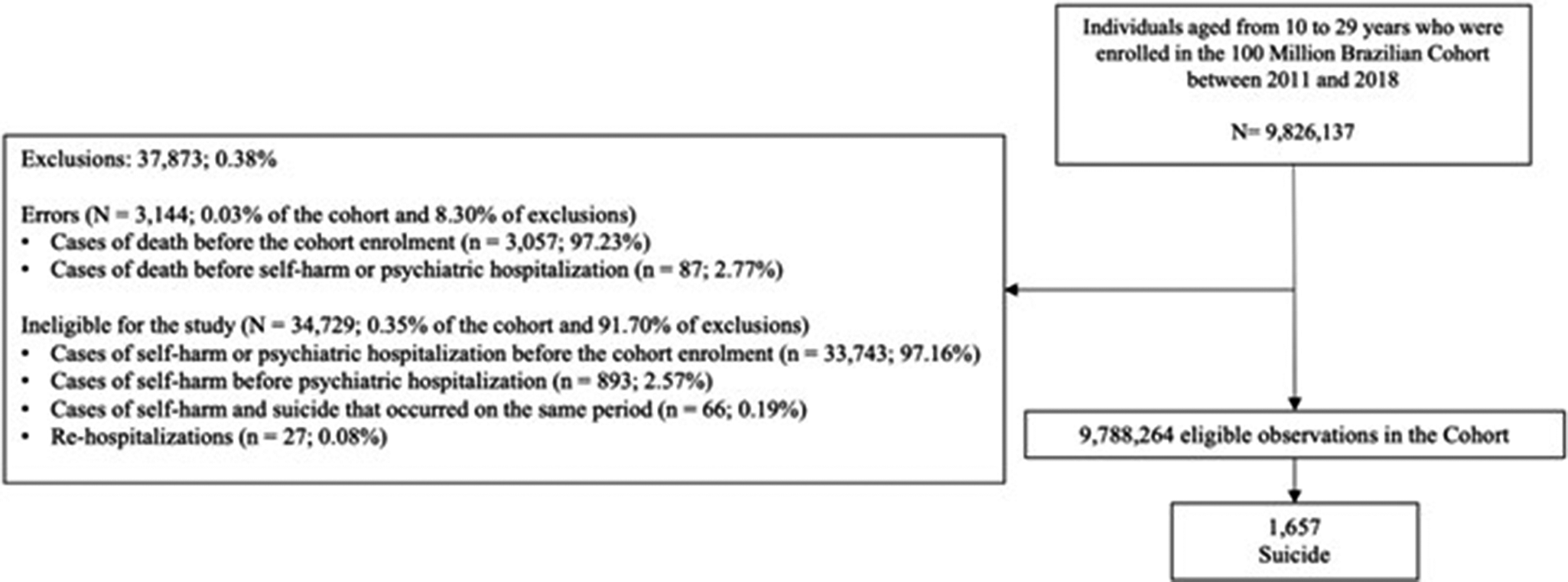
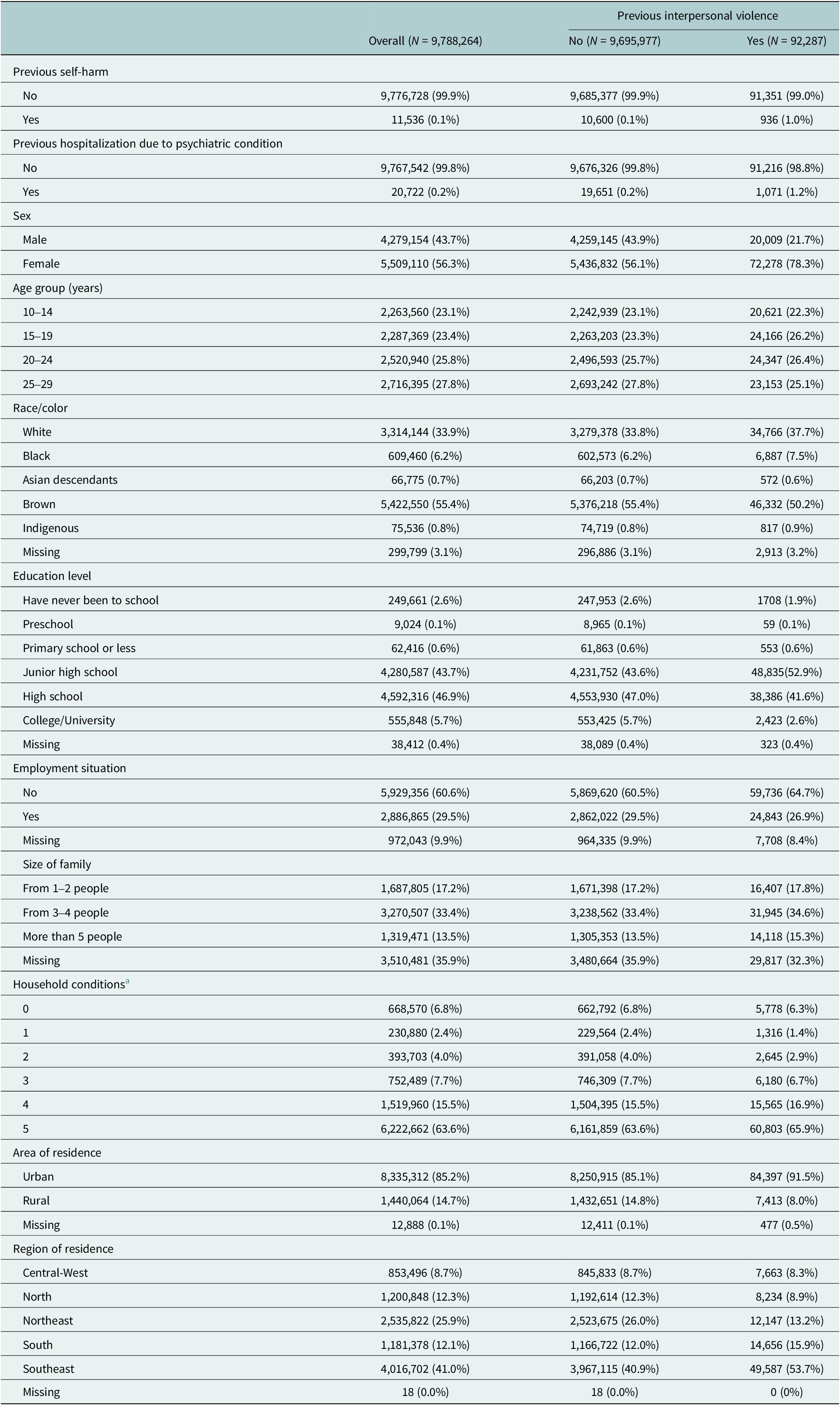
Among 9,788,264 young people aged 10–29 years enrolled in the 100 Million Brazilian Cohort between 2011 and 2018, 92,287 (0.94%) had at least one record of interpersonal violence (Figure 1). During follow-up, 1,657 suicides were identified. Individuals exposed to interpersonal violence were more likely to be female, younger, living in urban areas, residing in the Southeast region and to have the oldest household member unemployed compared with those without a history of interpersonal violence (Table 1).
Flowchart of the selected population.

Baseline characteristics by interpersonal violence

a Household conditions were measured using a composite score (0–5) based on access to public services (treated piped water, sanitation, electricity and garbage collection) and brick housing; higher scores indicate better conditions, with 0 indicating the absence of all factors and 5 indicating full presence.
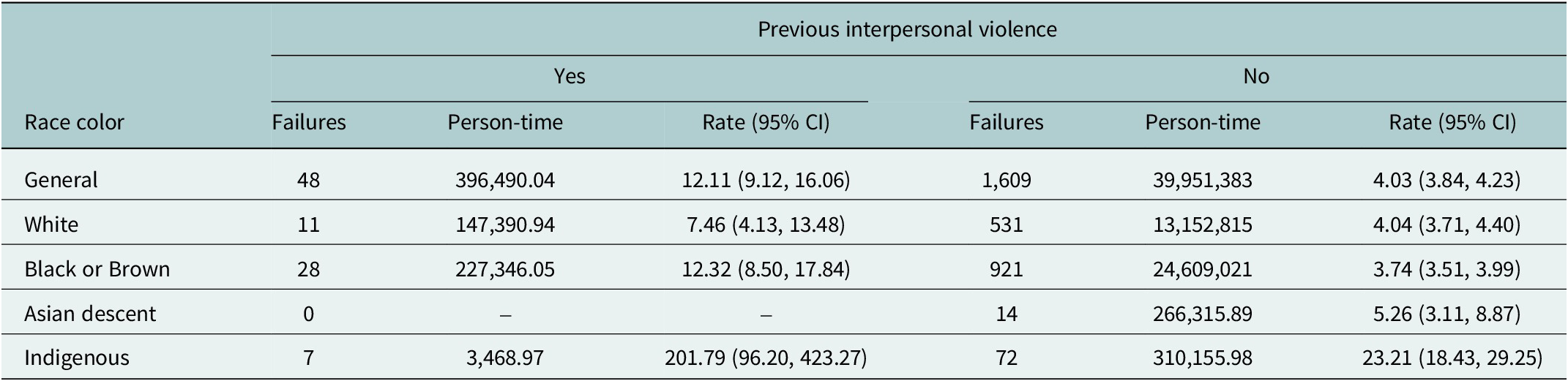
The suicide rate among those exposed to interpersonal violence was 12.11 per 100,000 person-years (95% CI: 9.12–16.06), compared with 4.03 per 100,000 person-years (95% CI: 3.84–4.23) among those without exposure. When compared by race, suicide rates among exposed individuals were highest among Indigenous individuals (201.79 per 100,000 person-years; 95% CI: 96.20–423.27), followed by Black individuals (12.32; 95% CI: 8.50–17.84). White individuals had the lowest rates (7.46 per 100,000 person-years; 95% CI: 4.13–13.48) (Table 2).
Suicide person-years rate (per 100,000) by previous interpersonal violence

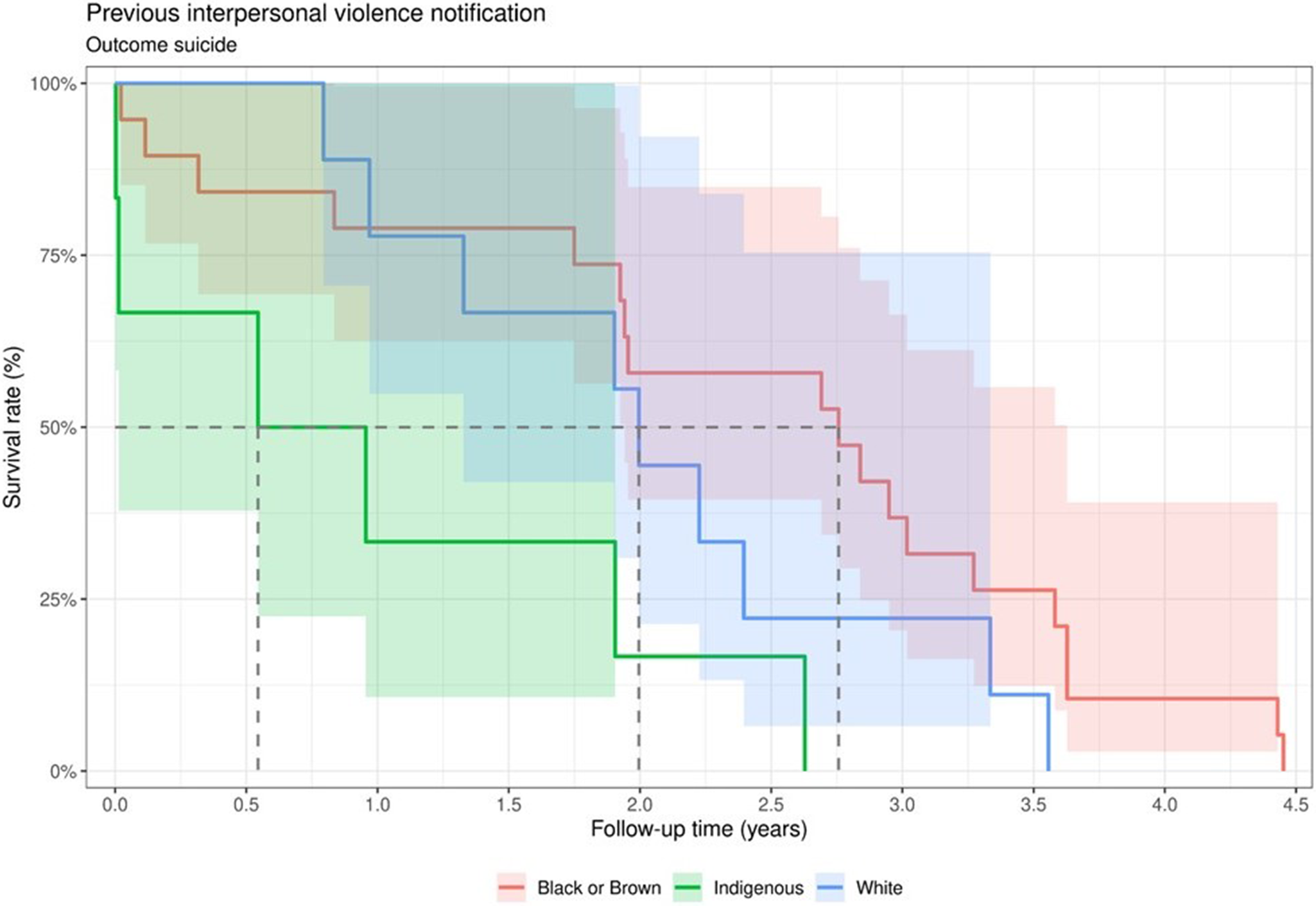
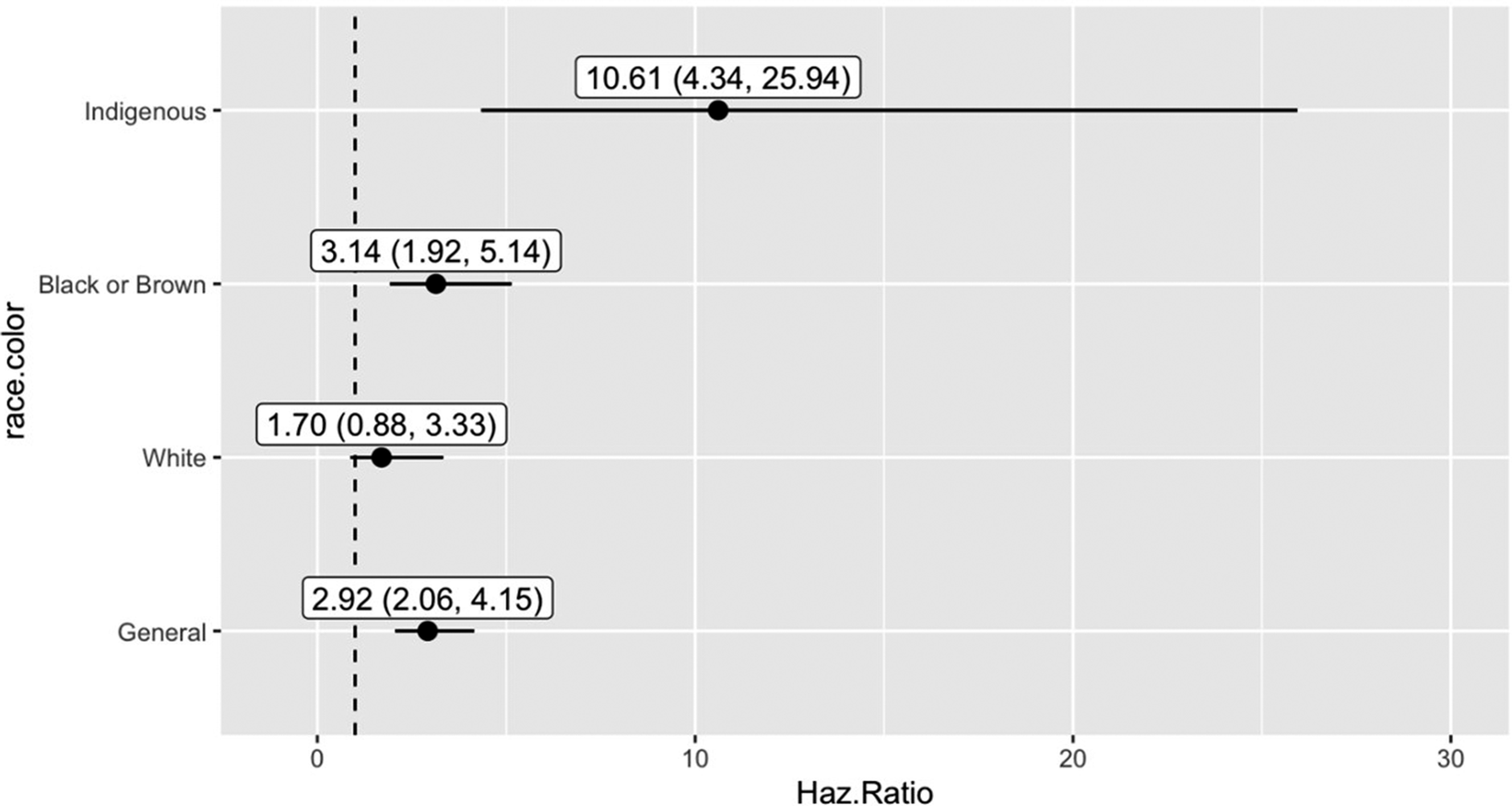
Survival probabilities after interpersonal violence exposure decreased more rapidly among Indigenous individuals (median survival time ~ 1 year), indicating the highest cumulative incidence of suicide over follow-up. However, CIs overlapped across race/skin color groups (Figure 2). Annual proportional mortality from suicide following exposure to interpersonal violence by race/skin color is presented in Supplementary Figure S12. Being exposed to interpersonal violence was associated with a higher risk of suicide (HR: 2.92; 95% CI: 2.06–4.15). The analysis by race showed a higher association among Indigenous individuals (HR: 10.61; 95% CI: 4.34–25.94), followed by the Black population (HR: 3.14; 95% CI: 1.92–5.14). Among White individuals, the association was not statistically significant (HR: 1.70; 95% CI: 0.88–3.33) (Figure 3).
Kaplan–Meier estimates (with 95% confidence intervals) of time-to-event for suicide following violence notification by race, Brazil, 2011–2018.

Cox models estimates*: general and by race color, Brazil, 2011–2018. Note: *Adjusted by age, sex, education level, employment situation, size of family, household conditions, region of residence, area of residence, previous self-harm notification and previous hospitalization for mental disorders.

Sensitivity analyses
Sensitivity analyses excluding prior self-harm and psychiatric hospitalization yielded results consistent with the primary analyses. While the association between interpersonal violence and suicide remained significant among White individuals, effect estimates for Black and Indigenous individuals were substantially higher, suggesting heterogeneity across racial groups (Supplementary Tables S3–S7). Additional analyses using self-harm as the outcome showed a similar pattern (Supplementary Table S8). Formal test of heterogeneity, including Wald’s test, supported these differences, with the interaction significant for the Indigenous group and a >20% change in effect estimates between models, further indicating potential effect modification by race/skin color of the association between interpersonal violence victimization and suicide (Supplementary Tables S9–S11).
Discussion
In this large, nationwide cohort of 9,788,264 young people aged 10–29 years, exposure to interpersonal violence was strongly associated with an increased risk of suicide. Overall, suicide rates were nearly three times higher among those exposed compared with those unexposed. Moreover, interpersonal violence exposure increased the risk of suicide even more among Indigenous and Black youth, highlighting pronounced racial inequalities in suicide risk: Indigenous individuals had the highest rates (10.69 times higher), followed by Black individuals (3.14 times higher), compared with White peers (HR: 1.70; 95% CI: 0.88–3.33). Survival analyses showed that post-violence suicide risk was highest among Indigenous youth (median survival ~ 1 year), reflecting stark ethnoracial disparities in cumulative incidence. These findings underscore how structural racism shapes unequal exposure to interpersonal violence and suicide risk in Brazil, reflecting deep-rooted ethnoracial inequities.
Our findings are consistent with international evidence showing that interpersonal violence, including physical assault, sexual violence and domestic abuse, is a potent risk factor for suicide in adolescence and young adulthood (Hershberger et al., Reference Hershberger, PiLkington and D’Augelli1997; Fidalgo et al. Reference Fidalgo, Sanchez, Caetano, Andreoni, Sanudo, Chen and Martins2018; Angelakis et al., Reference Angelakis, Austin and Gooding2020). A meta-analysis of longitudinal studies has demonstrated that young people exposed to interpersonal violence have a 2- to 10-fold increased risk of suicidal behavior compared with their nonexposed peers (Castellví et al., Reference Castellví, Miranda-Mendizábal, Parés-Badell, Almenara, Alonso, Blasco, Cebrià, Gabilondo, Gili, Lagares, Piqueras, Roca, Rodríguez-Marín, Rodríguez-Jimenez, Soto-Sanz and Alonso2017). In Brazil, previous studies have shown the high prevalence of violence exposure among adolescents, particularly in urban areas with high social vulnerability, and its associations with psychiatric disorders (Fidalgo et al., Reference Fidalgo, Sanchez, Caetano, Andreoni, Sanudo, Chen and Martins2018; Woolley and Macinko, Reference Woolley and Macinko2018Miliauskas et al., Reference Miliauskas, Junger, Hellwig, Bloch and de Souza Lopes2023; Wille Augustin et al., Reference Wille Augustin, Rinozi Teixeira and Kolves2025). Although few studies have specifically investigated ethnoracial inequalities in the association between violence and suicide, and even fewer have included Indigenous populations, the strong association observed among Indigenous and Black youth in our study is consistent with evidence from other settings. In the United States, for example, Native American and Black youth exhibit higher rates of both violence exposure and suicide compared with White youth (Hua et al., Reference Hua, Lee, Rahmandar and Sigel2023; Wolf et al., Reference Wolf, Rivara, Orr, Sen, Chapman and Woolf2024; Bell et al., Reference Bell, Nicoletti and Ammerman2025). Similarly, studies in Canada and Australia have documented elevated suicide rates among Indigenous populations in the face of violence (Pollock et al., Reference Pollock, Naicker, Loro, Mulay and Colman2018; Dickson et al., Reference Dickson, Cruise, McCall and Taylor2019).
Historical processes of oppression, enslavement and systemic marginalization rooted in racism have placed Black and Indigenous populations in socially and economically constrained environments, increasing their exposure to violence and limiting access to protective resources (Jones, Reference Jones2000; Werneck, Reference Werneck2016; Scott-Jones and Kamara, Reference Scott-Jones and Kamara2020; Bell et al., Reference Bell, Nicoletti and Ammerman2025). In Brazil, in urban areas, the escalation of police violence in territories predominantly occupied by Black populations creates chronic tension and a constant state of alert, increasing suicide risk among youth both directly through violent encounters and indirectly by placing them in continuous zones of conflict (Bordin et al., Reference Bordin, Duarte, Ribeiro, Paula, Coutinho, Sourander and Rønning2018; Cruz et al., Reference Cruz, Silva, Jakaite, Krenzinger, Valiati, Gonçalves, Ribeiro, Heritage and Priebe2021). This environment, combined with the lack of schools, safe recreational spaces and other protective resources, constrains life opportunities and further amplifies vulnerability to mental health problems and suicidal behavior (Cruz et al., Reference Cruz, Silva, Jakaite, Krenzinger, Valiati, Gonçalves, Ribeiro, Heritage and Priebe2021).
Suicide rates among Indigenous populations in Brazil have historically been higher than those observed in the general population (de Araújo et al., Reference de Araujo, Fialho, Alves, Cardoso, Orellana, Naslund, Barreto, Patel and Machado2023; Alves et al., Reference Alves, Fialho, de, Naslund, Barreto, Patel and Machado2024), reflecting longstanding social, economic and historical inequities. Despite this, relatively few studies have systematically explored the social markers contributing to this elevated risk, leaving critical gaps in our understanding of the social and structural determinants involved. In recent decades, Brazil has experienced an intensification of the exploitation and seizure of Indigenous lands, processes of dispossession that have increased violence in Indigenous territories (Miotto, Reference Miotto2022). These dynamics may contribute to elevated suicide rates among communities that lose their villages and family members, in addition to exposure to other forms of systemic violence that further exacerbate the risk of suicide among victims and their families (Alves et al., Reference Alves, Fialho, de, Naslund, Barreto, Patel and Machado2024). The more rapid decline in survival probabilities among Indigenous youth (median ~ 1 year) after exposure to violence indicates that not only are these groups at higher overall risk, but suicide events also occur sooner following violent experiences. These represent enduring inequalities that continue to drive persistent disparities over time.
These findings are shaped by structural racism, which systematically disadvantages Indigenous and Black populations in Brazil. Historical racial stratification has placed these groups in socially and economically marginalized positions, increasing their exposure to violence through residential segregation, over-policing and limiting protection from justice systems (Sousa Filho et al., Reference Sousa Filho, Sousa Filho, Pedeira, Santos, Guimarães, Ferreira, Alves, Nascimento, Paiva, Andrade, Góes, Barreto and Aquino2023; Gómez-Restrepo et al., Reference Gómez-Restrepo, Diez-Canseco, Brusco, Jassir Acosta, Olivar, Carbonetti, Hidalgo-Padilla, Toyama, Uribe-Restrepo, Rodríguez Malagon, Niño-Torres, Godoy Casasbuenas, Stanislaus Sureshkumar, Fung, Bird, Morgan, Araya, Kirkbride and Priebe2025). Interpersonal violence intersects with broader social determinants of health. Indigenous and Black youth are disproportionately exposed to poverty, segregation and restricted educational and employment opportunities (Miliauskas et al., Reference Miliauskas, Junger, Hellwig, Bloch and de Souza Lopes2023; Wanzinack and Mélo, Reference Wanzinack and Mélo2025), increasing both the likelihood of victimization and mental distress. Violence itself has direct psychological effects, including trauma, depression, post-traumatic stress disorder and substance misuse, all of which elevate suicide risk (Na et al., Reference Na, Shin, Kwak, Lee, Jester, Bandara, Kim, Moutier, Pietrzak, Oquendo and Jeste2025). Chronic exposure fosters hypervigilance, hopelessness and maladaptive coping, further amplifying pathways to self-harm (Na et al., Reference Na, Shin, Kwak, Lee, Jester, Bandara, Kim, Moutier, Pietrzak, Oquendo and Jeste2025).
This study highlights ethnoracial disparities in the association between violence and suicide. Recognizing that racism systematically shapes exposure to violence, with profound consequences for mental health and suicidal behavior among Indigenous and Black populations in Brazil, underscores the urgent need for interventions that advance health equity (Alvarez et al., Reference Alvarez, Polanco-Roman, Breslow and Molock2022). Such interventions should adopt an intersectional perspective, addressing the interconnections among social markers of oppression, including race, education, socioeconomic status and land ownership. From a public health perspective, suicide prevention strategies must move beyond individual-level approaches to tackle systemic drivers of inequity (Machado, Reference Machado2025). Addressing these structural determinants is critical to achieving the Sustainable Development Goal of reducing suicide rates by one-third by 2030. Confronting institutional racism must be central to these efforts, accompanied by adequate resource allocation and sustained political commitment.
Strengths and limitations
The strengths of this study include the use of a large, nationwide cohort drawn from multiple linked administrative data sources, enabling longitudinal follow-up, the investigation of a rare outcome and minimizing selection bias. The robust adjustment for sociodemographic and household characteristics, along with stratified analyses, provides novel insights into racial/skin color disparities in the relationship between interpersonal violence and suicide.
Nonetheless, limitations should be acknowledged. First, the study population is composed of individuals and their families living in socioeconomic vulnerability. Thus, the results cannot be extrapolated to the entire Brazilian population. At the same time, it is important to note that this population is also the primary user of Brazil’s public health system, and exposure to interpersonal violence in this study was ascertained through health system records. Consequently, the associations observed in this study may provide a particularly reliable assessment of violence-related risks within socioeconomically vulnerable populations. Misclassification of exposure is possible, and suicide deaths may also be underreported or misclassified, particularly in remote regions, which could disproportionately affect Indigenous populations. However, health system data in Brazil have improved in both quality and coverage over recent years, which helps to mitigate these concerns (Rebouças et al., Reference Rebouças, Alves, Ferreira, Marques, Guimarães, GR de, PFPS, Teixeira, Ortelan, Silva, Rocha, Falcão, Pinto Junior, Pescarini, Paixão, MF de, de CR, MYT and Barreto2025). Residual confounding cannot be ruled out, including unmeasured factors such as family history of mental illness, community-level social cohesion or differential access to lethal means. Finally, while self-declared information about what happened may be biased, for example, a person may try to hide interpersonal violence by reporting self-harm, and vice versa, hospitalization data in Brazil are completed by medical doctors using ICD codes for diagnosis, reflecting the physician’s clinical assessment and judgment. Notification data are also completed by health professionals based on their technical evaluation, rather than relying solely on self-reports.
Despite these limitations, the findings provide compelling evidence of the intertwined role of interpersonal violence and structural inequities in shaping suicide risk among Brazilian youth.
Conclusion
In this nationwide cohort of nearly 10 million young people in Brazil, exposure to interpersonal violence was strongly associated with an increased risk of suicide, with markedly higher risks among Indigenous and Black youth. These findings provide rare longitudinal evidence that interpersonal violence contributes to ethnoracial inequalities in suicide mortality, highlighting how structural racism and social disadvantage shape vulnerability to both violence and its lethal mental health consequences. Suicide prevention strategies for young people must, therefore, extend beyond individual-level interventions to include violence prevention and structural policies that address racial inequities.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10179.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10179.
Data availability statement
All data supporting this study were obtained from the Center for Data and Knowledge Integration for Health (CIDACS). Restrictions apply to accessing these data, which contain sensitive information, are licensed for exclusive use in the current study and, due to privacy regulations from the Brazilian Ethics Committee, are not openly available. Controlled access to the data is possible upon reasonable request and with express permission from CIDACS (mail to cidacs.curadoria@fiocruz.br) and approval from an ethics committee.
Author contributions
FA and DBM conceptualized the study. EF conducted the analyses. EF and FA verified the underlying data. FA drafted the manuscript. LA edited it. AF reviewed and added critical content to the manuscript, including the interpretation of the analyses and data. DBM supervised the analyses, data interpretation and manuscript writing. All authors had access to the data, contributed to the interpretation and discussion and approved the final version of the manuscript. FA and LT had the final responsibility for submission.
Financial support
Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number R01MH128911. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interest
The authors declare no competing interests.
Ethics statement
Ethical approval for this study was obtained from Centro de Pesquisas Gonçalo Moniz, Fundação Oswaldo Cruz, Bahia (CAAE: 84842624.4.0000.0040).



 Open access
Open access