


1. Introduction
Lao People’s Democratic Republic (Lao PDR) is a lower-middle-income country in South-East Asia with a population of 7.8 million (World Bank, 2025b), about 60% of which live in rural and remote areas (Lao Statistics Bureau and United Nations Children’s Fund 2024). Despite progress on development and health indicators in the previous decades, approximately 16% of the Lao population still lives below the poverty line (World Bank, 2025c), and maternal mortality remain the worst in the region (Lao Statistics Bureau and United Nations Children’s Fund 2024).
The Government of Lao PDR (GoL) is committed to achieving universal health coverage (UHC) by 2030 (Ministry of Health, 2022a) but access and uptake of essential services remain low (World Health Organization, 2025b). Central to achieving UHC is adequate, effective and equitable health financing but in Lao PDR this is challenged by low domestic expenditure on health and external financing which can be unpredictable, fragmented or misaligned with country needs (Kim et al., Reference Kim, Park, Lo, Keoprasith and Panyakeo2024). In response to these challenges faced by many low-and-middle-income countries, the Center for Global Development (CGD) has developed a ‘New Compact‘ approach comprising three elements: promoting locally-led, evidence-informed prioritisation; domestic-first resource allocation; and consolidated supplementary aid to strengthen country ownership and health outcomes (Drake et al., Reference Drake, Regan and Baker2023; Gheorghe et al., Reference Gheorghe, Baker, Guzman and Drake2024).
Here, we aim to understand enablers and barriers to reform and develop a roadmap towards more effective and sustainable health financing in Lao PDR, using the New Compact approach as a framework.
2. Health financing in Lao PDR
Most recent data (World Health Organization, 2025a) indicates total health expenditure (THE, inclusive of current and capital spending) in 2022 was 4,723,677 million Lao KIP (LAK) (377 million USD), comprising funding from donors (39.1%), government (27.2%), out-of-pocket expenditure (30.2%), social health insurance (3.3%) and corporations (0.1%).
In 2022, THE was 2.4% of GDP and general government health expenditure (GGHE – including external financing) was 9.6% of general government expenditure (GGE) (World Health Organization, 2025a). GoL is aiming for domestic GHE (DGHE – excluding external financing) to account for 9% of GGE, but in 2022 this was just 3.5% (World Health Organization, 2025a).
Current health expenditure (CHE or recurrent expenditure excluding capital costs) was LAK 4,386,686 million /USD 313 million (589,371 LAK / 42 USD per capita) in 2022, or 92.9% of THE. Primary health care (PHC) expenditure was LAK 313,290 (USD 22) per capita or 53.2% of CHE. Approximately 47.4% of total PHC expenditure came from donors, 31.9% from the domestic government, 19.8% was OOP and 0.9% from other sources (World Health Organization, 2025a).
Budget formulation within the Ministry of Health (MOH) occurs at the sub-national and national levels. At the sub-national level, the district governor office develops and submits the proposed budget and financial plan for the next fiscal year to the provincial governor’s office. Once agreement is reached, the budget is adopted and transmitted to the MOH. Micro-planning starting at the health centre level is incorporated into the district-level budget.
At the national level, each of the seven departments within the MoH are responsible for development of annual workplan and budget, under which fall detailed sub-workplans and programmes.
The GoL principally allocates health sector funding to three areas: technical support at national, provincial, and local levels; national health insurance (NHI), and; co-financing requirements, eg. for Gavi and the Global Fund for HIV, TB and Malaria. Funding requests by lower levels normally exceed the funds available, and the actual allocation may depend on the political priorities and negotiations at ‘the top‘ of the government (Government of the Lao P.D.R., 2024c)
In 2016 and 2017, the GoL moved to fund NHI premiums directly, and to automatically enrol the eligible population. Under the NHI, a fixed co-payment is payable to the provider by the patient at the time of care, and the remaining cost is reimbursed via a pre-payment based on expected demand and the estimated cost, as per the annual service contract between the NHI and the health facility (Ministry of Health, 2018). At present Vientiane Capital is not included in the NHI (Ministry of Health, 2022b), accounting for approximately 13.5% of the Lao population. Co-payments at the facility level have also increased recently (Ministry of Health, 2024).
The Lao Essential Services Health Package (EHSP) was first developed and endorsed by MOH in 2018, updated with minor changes in 2023 (Ministry of Health, 2023), with normative costing estimates produced based on the 2018 package (Prinja, Reference Prinja2020). The Lao EHSP lists 100 interventions which should be available at one or more levels of the health system. Interventions were agreed by all MoH departments, national centres, central hospitals and professional associations based on effectiveness, sustainability, feasibility, equity, acceptability and commitment criteria (Ministry of Health, 2023).
The EHSP and NHI are not linked, but within the EHSP, the NHI covers all consultations and admissions, while drugs, vaccines, tests and other commodities for immunisation, TB, HIV, malaria and family planning are provided by vertical programmes. Three factors impede the EHSP’s availability. First is the level of funding, with an estimated gap of 676,369 million LAK (53 million USD) between actual government and insurance expenditure (as % of THE) in 2022 and the estimated full cost of the EHSP (Prinja, Reference Prinja2020; World Health Organization, 2025a). Secondly, the EHSP was not developed with explicit reference to cost-effectiveness or other criteria which may be helpful in priority setting and resource allocation when the available resources are insufficient to meet the full cost of the package. Of EHSP interventions, the average cost-effectiveness ratio ranges from 1.7 USD per healthy year of life (HLY) gained for neonatal resuscitation to 10,552 USD per HLY gained for insulin injections for diabetes, with generally lower ACERs for maternal and child health and PHC interventions and higher ACERs at the secondary and tertiary level and for non-communicable disease interventions (Bertram et al., Reference Bertram, Chisholm, Watts, Waqanivalu, Prasad and Varghese2021; Ralaidovy et al., Reference Ralaidovy, Lauer, Pretorius, Briët and Patouillard2021; Stenberg et al., Reference Stenberg, Watts, Bertram, Engesveen, Maliqi, Say and Hutubessy2021). Third, the allocation of expenditure does not align with expected costs or highest priority services, with most spending allocated towards curative care or secondary and tertiary care rather than preventive care and primary health care (Prinja, Reference Prinja2020; World Health Organization, 2025a).
Several health donors are active in Laos but largely follow their own procedures for funding allocation and disbursement, with no forum for coordinated planning and budgeting with the GoL. Donors may also fund interventions (eg. HPV vaccination, intensive case finding for malaria elimination) which are outside the EHSP.
3. Implementing a new compact for health financing in Laos
Given the above, implementing the New Compact in Lao PDR could be beneficial. Firstly, evidence-based prioritisation could support (re)allocation of available resources towards the most essential health services based agreed criteria. Secondly, determining a path towards ‘domestic-first financing‘ for those essential services could ensure that government funding is clearly prioritised with greater emphasis on preventive care. Finally, there would be clarity on where donors could provide consolidated supplementary aid, aligned to global health priorities, for interventions which are important but not the most critical in the context.
Below we identify potential barriers and enablers and outline a roadmap towards realising the New Compact approach in Lao PDR.
4. Contextual and institutional factors impacting the new compact
With reference to the WHO guidance (World Health Organization, 2023b), we sought to describe the relevant contextual and institutional factors which should be considered in determining how to move budgeting and resource allocation in Lao PDR towards a New Compact approach.
4.1. Ownership, financing and political factors
Lao PDR is a single party state ruled by the Lao People’s Revolutionary Party (LPRP). The LPRP and GoL are committed to achieving UHC (Ministry of Health, 2023b). Public health facilities provide most health services in the country, and the GoL has significant control over where and how domestic resources are used to achieve health outcomes. Potential ‘reform windows‘ may present as a result of declining external assistance for health and reorientation of both domestic and external health financing towards PHC (Kim et al., Reference Kim, Park, Lo, Keoprasith and Panyakeo2024; Ministry of Health, 2021)
However accelerating progress towards UHC may require increasing domestic funding available and reallocation of existing funding (domestic and external), eg. further towards PHC. Actual domestic health expenditure has remained relatively stable in the last several years with fiscal space for health constrained by macroeconomic factors, including high public debt and declining purchasing power due to steep depreciation of the kip against the US dollar(World Bank, 2025b).
Decision-making power related to health financing is also distributed across and between levels of government. The MOH oversees the entire healthcare system, across three levels of governance: central, provincial, and district. However, most facilities and financing for health services are managed at the provincial and district levels, and provincial governors have total authority to allocate funding received from the central government or which they raise themselves, within and between sectors and services falling under the provincial government’s responsibility. This flexibility does not exist for targeted support that is provided by donors (World Bank, 2024a).
Historically, all decisions concerning human and financial resources in the health care sector must be routed through the central level, represented by the MoH and other ministries, notably the Ministry of Finance (MoF), which is responsible for overall fiscal policy and sectoral allocations of the annual recurrent budget. The Ministry of Planning and Investment (MPI) oversees capital budget allocation, whereas the Ministry of Home Affairs manages the total number of civil servants and sectoral allocations, including the annual recruitment of health personnel at all levels (World Bank, Reference Bank2023). Constitutional power-sharing arrangements are also under political influence (Figure 1).
Government-level power sharing in Lao PDR. (Viphonephom et al., Reference Viphonephom, Kounnavong and Reinharz2024).

The autonomous hospitals programme started in 2024 and covers 8 to 10 hospitals at present. It allows hospitals greater decision-making power eg. hospitals can exceed the human resource quotas if they have the resources to do so (Government of the Lao P.D.R., 2024b; World Health Organization, 2023a)
Any proposed changes to the budget process may be resisted by programmes and/or geographic entities which have historically received funding amounts disproportionate to need or value for money, as indicated by burden of disease, intervention cost-effectiveness and other measures. Government flexibility particularly at the central level is also influenced by factors such as co-financing requirements of global health initiatives, which require ‘ring-fencing‘ of funds for specific commodities that may not always align with the highest priority interventions.
4.2. Accountability and oversight
Despite ongoing efforts, public financial management and particularly accountability for expenditure below the provincial level remains sub-optimal due to poor reporting systems and capacity (World Bank, Reference Bank2019). Budget execution cycles at sub-national level are often compressed due to delays in disbursement from the national level. These gaps in budget execution result in delayed procurements and low human resources expenditure, and subsequently poor service readiness at facility level (World Bank, Reference Bank2018, Reference Bank2019).
The implication for New Compact implementation is that even if budget formulation processes can be reformed, funding will not always flow effectively to where it is needed for delivery of essential services.
4.3. Evidence
Evidence is not systematically used in decision-making in Lao PDR. A study (Phommachanh et al., Reference Phommachanh, Sittimart, Ananthakrishnan, Vongsack, Soysouvanh, Ashley, Teerawattananon, Dabak and Mayxay2025) based on interviews and surveys with numerous government and non-government stakeholders found decisions are often based on opinions rather than evidence. A partial exception is immunisation, where the National Immunisation Technical Advisory Group has made recommendations on new inclusions to the schedule based on appraisal of existing evidence on burden of disease and vaccine effectiveness. However, long-term government budget impact (minus donor co-financing) or cost-effectiveness relative to other health interventions is generally not considered.
Appetite exists among the MoH and other stakeholders for greater appraisal and use of evidence – including economic evidence – in resource allocation. The Unit for Health Evidence and Policy (UHEP) has recently been established and presents a mechanism by which both demand and supply of evidence-based decision-making can be strengthened, eg. by using health technology assessment (HTA) as a tool. Capacity building and institutionalisation of the use of evidence in decision-making will be critical in moving towards greater evidence-based prioritisation and domestic first financing of essential health services, as envisioned by the New Compact.
4.4. Equity
Coverage of essential health services such as maternal and child health care varies substantially by province, rurality, ethnicity and socio-economic status (Lao Statistics Bureau and United Nations Children’s Fund, 2024). Yet government budget allocations are based on adding a percentage to the previous budget, rather than health needs or population size, with no correlation as a result in THE per capita and population size (World Health Organization, 2025a).
Outreach services are highly dependent on donor funding and access in rural and remote areas may be threatened if this funding ceases (Kim et al., Reference Kim, Park, Lo, Keoprasith and Panyakeo2024). Implementation of NHI and previously the free maternal and child ehealth scheme do not necessarily reduce out-of-pocket costs or inequities faced by disadvantaged households (Nagpal et al., Reference Nagpal, Masaki, Pambudi and Jacobs2019; Quach et al., Reference Quach, Mayxay, Bounvilay, Thammavong, Bounkhoun, Phaiphichit, Kingkeooudom, Phangmanixay, Souvannasing, Ashley, Nguyen, Carvalho and Russell2025). These inequities can be exacerbated by differences in the quality of care between geographic areas (Nagpal et al., Reference Nagpal, Masaki, Pambudi and Jacobs2019).
A New Compact approach to health financing will only improve service coverage and ultimately health outcomes if barriers to access and uptake among underserved populations and geographies in Lao PDR are addressed.
4.5. Ideological and cultural factors
Lao PDR is socialist in orientation, which pre-supposes a high level of commitment to essential health services which are affordable to all. Yet communities have historically not had a voice in what health services are prioritised or an ability to hold the health system accountable for performance and quality of care. Models of community engagement involving both the health and home affairs sectors, show promise in increasing local trust and ownership of health services and thus contribute to their ongoing improvement and sustainability (Kubota et al., Reference Kubota, Elliott, Ounaphom, Phrasisombath, Xaymongkhonh, Phimmachak, Souksavanh, Volaot, Kounnavong, Haenssgen, Horiuchi, Bode, Odugleh-Kolev, Seal and Lo2024). Implementing the New Compact could identify the opportunity for GoL to focus on the core package it provides to its citizens and strengthen the link with communities.
5. Stakeholder positions and influence
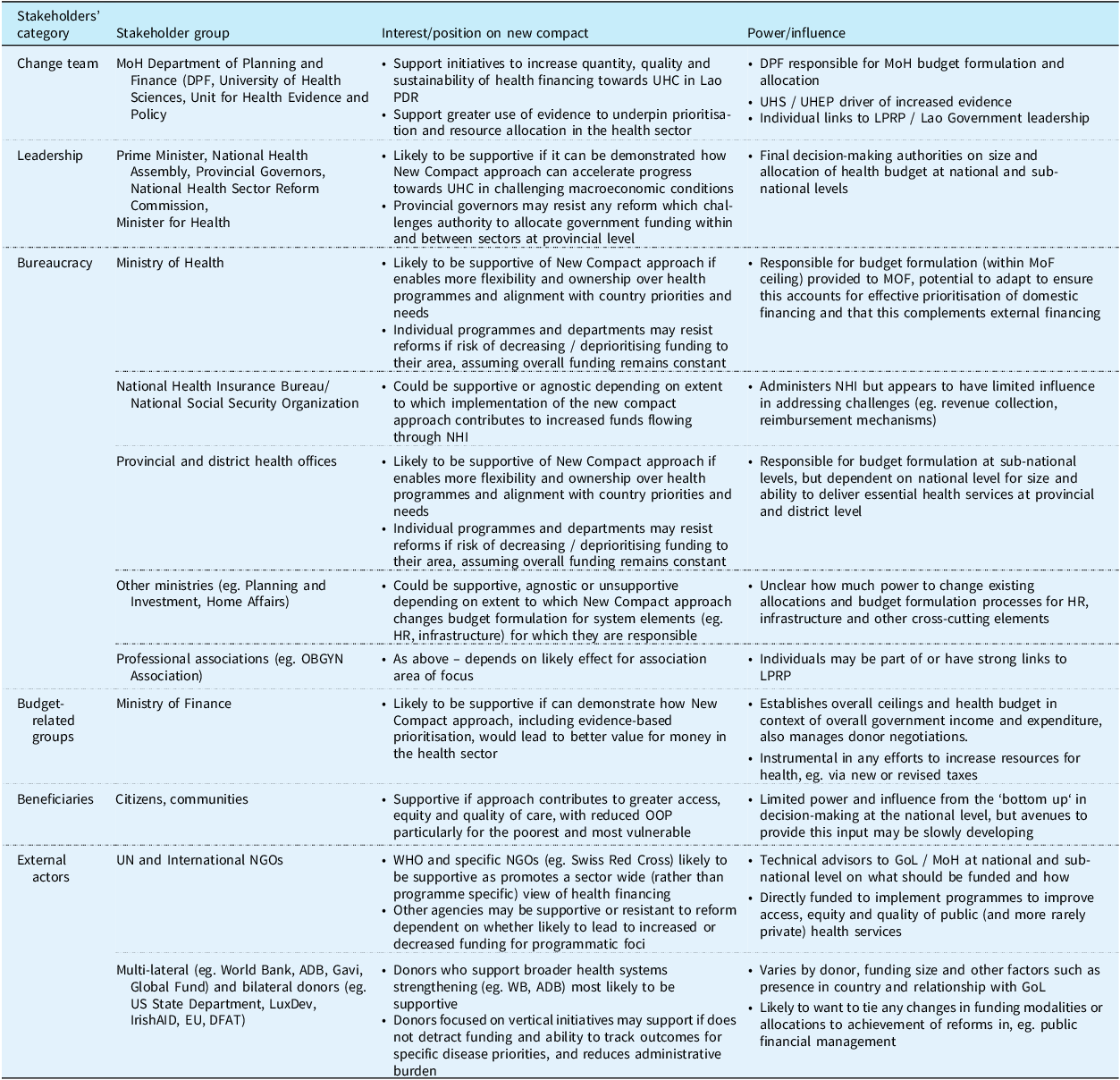
The likely positions and influence of key stakeholders vis-a-vis the New Compact approach in Lao PDR are outlined in Table 1, with the change team encompassing academia and MoH representatives responsible for initial analysis and New Compact roadmap development.
Stakeholder analysis

6. Other factors influencing readiness to adopt the New Compact
Additional considerations in determining the likelihood of success if Lao PDR was to adopt the New Compact include health systems capacity and the status of donor harmonisation and transition efforts (Drake et al., Reference Drake, Demeshko, Kiros, Memirie, Norheim, Kaddar, Chalkidou, Baker and Yakhelef2025).
Organisational capacity to plan, cost, budget, implement and monitor priority health services may be weak particularly at lower levels, and service access and quality unpredictable at the facility (rather than outreach) where there is dependence on government funding. There is an estimated 1.23 health personnel per 1,000 population and recent reductions in civil service quotas may further decrease the availability of health personnel in public facilities (World Health Organization, 2023a). An integrated public health commodities supply chain between the central, provincial, district and facility levels is in place, yet frequent shortages of essential medicines still occur (Bunde et al., Reference Bunde, Herrera, Chanthala, Posner and Sohkivong2025). Finally, the establishment of the DHIS 2 has been critical to improving data availability but work to increase quality and use in decision making is ongoing. A NHI management system to track payment claims does not exist but is a priority for establishment under the National Digital Health Strategy 2023–2027 (Ministry of Health, 2023).
There are ongoing programmes and strategies to address readiness gaps among MoH, donors and partners, some of which are referred to in Table 1.
The autonomous hospitals programme, which is fee for service, may incentivise over servicing, increase OOP costs and reduce access for the most vulnerable (Geng et al., Reference Geng, Yu and Chen2016).
There is no formal mechanism for donor harmonisation though funds pooling occurs in limited instances, for example with the World Bank Health and Nutrition Service Access (HANSA) II Program which is jointly funded by the World Bank, DFAT, The Global Fund and Gavi (World Bank, 2024a). Efforts to transition specific government services away from donors are pending. Lessons learned from Gavi transition discussions include the need for greater attention to operational costs (eg. outreach), for consistent timeframes and transition criteria, and for measuring progress towards financial and programmatic sustainability to start at the beginning of donor investments rather than a few years prior to the anticipated transition (Bahuguna et al., Reference Bahuguna, Masaki, Jeet and Prinja2023)
7. Roadmap towards a new compact in Lao PDR
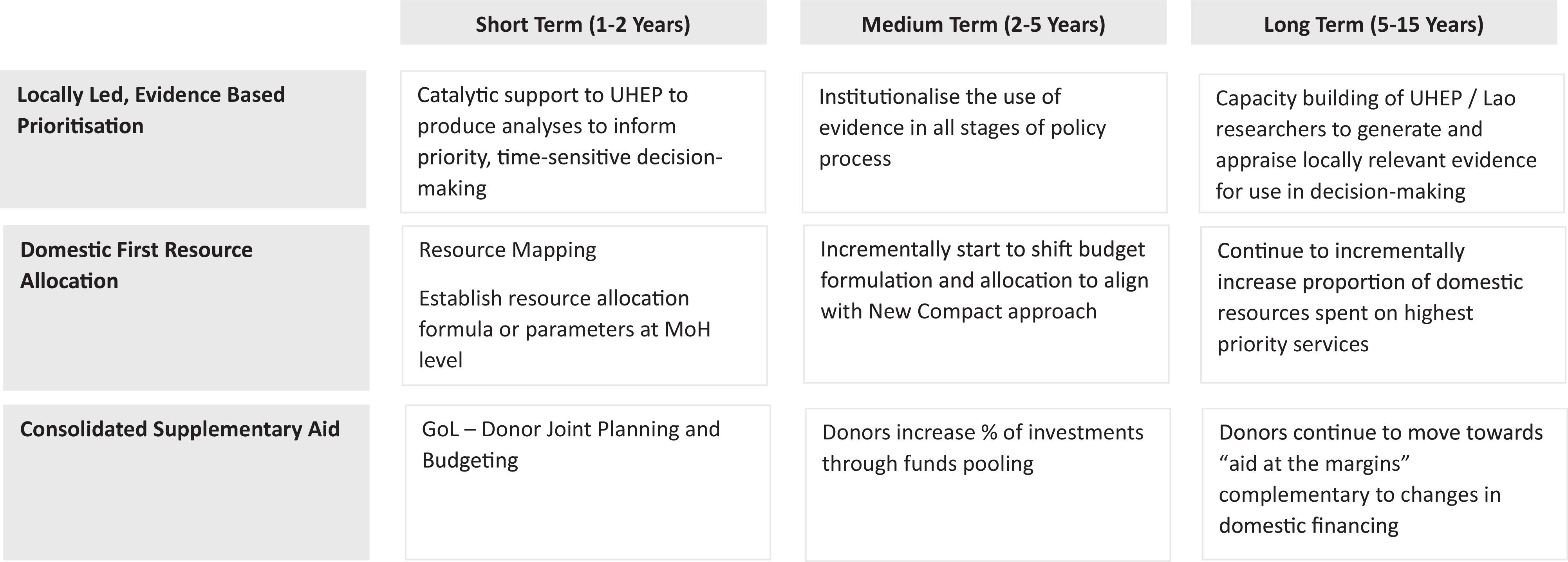
Despite the significant challenges, there are opportunities and strategies which GoL, donors and partners can deploy to optimise health financing. These are described below and at Figure 2, in relation to the three pillars of the New Compact approach.
Proposed roadmap towards New Compact implementation in Lao PDR.

7.1. Locally led evidence-informed prioritisation
On the supply side, UHEP provides a platform to generate policy relevant evidence on the effectiveness and cost-effectiveness of programmes, interventions and service delivery models using methods such HTA. Recognising limited local capacity, external organisations could fund catalytic short term technical assistance and support UHEP to produce analyses in one or two policy-relevant, time-sensitive areas to help define, test and refine processes by which HTA can be incorporated into decision-making, and build further demand for evidence-informed decision making. These analyses should also include equity and the distributional impacts of a new or existing intervention (Pearson-Stuttard and Owolabi, Reference Pearson-Stuttard and Owolabi2025).
In the Lao context, there are least two high priority questions. The first is, given Gavi transition in the coming years, which vaccines in the current portfolio should be prioritised for public sector funding as opposed to donor or private sector funding, or a blended approach. A hypothetical approach to applying the New Compact to vaccination programmes has been developed (Morton et al., Reference Morton, Briones, Demeshko, Baker and Drake2024) and could be adapted and applied in the Lao context.
A second priority question pertains to the benefits package which is currently based on a ‘negative’ list, e. stipulates services which are excluded as mentioned above, with all other services implicitly included (Ministry of Health, 2022b). HTA including incremental cost-effectiveness analysis could determine which items in the EHSP should be prioritised for available funding, including via NHI, and which items could be added or removed as resource levels change (Norheim and Watkins, Reference Norheim and Watkins2023). Criteria which could be considered for relevance in Lao PDR include burden of disease, effectiveness, cost-effectiveness, equity, financial risk protection, equity, feasibility and budget impact (World Bank, 2025a).
Potential revisions to the EHSP could also be proposed, based on cost-effectiveness analysis and comparison of estimated costs and health benefits with the current EHSP.
On the demand side, a National Assembly decree (Government of the Lao P.D.R., 2024a) establishes the role and purpose of UHEP, but further efforts are needed to institutionalise the use of evidence. This should include establishing standard processes for conduct of HTA so relevant to policy and local context, developing a reference case with technical specifications for HTA in Lao PDR, estimating country-specific cost-effectiveness thresholds and determining mechanisms for stakeholder engagement (World Health Organization, 2021).
In the longer term, capacity building of Lao staff should continue through supporting postgraduate degrees in HTA, health policy and health economics, with focus on priority investment areas and supplemented by on-the-job training, peer exchange and participation in relevant global networks.
Prioritisation of cost components within programme budgets can also help ensure existing resources yield the greatest value for money. The MoH at all levels can prioritise plans and budgets towards meeting the direct costs of service delivery, recognising this is the cost component with the strongest relationship to coverage. Integrating planning and budgeting between programme areas can achieve savings although models of care may still need to be tested for feasibility and effectiveness in producing health outcomes compared to vertical programme
7.2. Domestic first resource allocation
Moving towards a scenario where domestic resources fund the highest priority services requires understanding existing funding patterns and variations in funding levels and outcomes between programme and geographic areas. MoH can initiate resource mapping across programmes and funding sources from central to the provincial, district and health centre levels. Greater visibility on donor funding will clarify which services and geographies the government should allocate resources to and reduce likelihood of some provinces and districts receiving funding disproportionate to need, i.e., being over or underfunded. It could also strengthen evidence-based planning at all levels, including with embedded technical assistance.
Estimating which cost-effective interventions can be funded via the current government budget could assist with determining where to start in shifting towards domestic first financing.
Fairness in budget formulation could also be enhanced by establishing resource allocation formula inclusive of financial and human resources, and incorporating updated cost estimates, burden of disease, size of catchment population, rurality and other relevant dimensions (Hanson et al., Reference Hanson, Brikci and Erlangga2022). This formula could be applied in conjunction with resource mapping to establish budget ceilings or allocate available resources proportionally according to need, rather than relying on historically derived budgets which may not be needs-based or accurately reflect current costs.
An outcome from these steps could be an increased proportion of government funding for PHC, which alongside increasing funding for routine operational costs would be key to transition planning for donors who currently fund a substantial proportion of essential services.
The budget process can also be linked more explicitly to results, including service readiness and coverage. While coverage data is increasingly available, quality remains variable and does not in itself provide insight into which factors contribute to low or high performance. Recent analysis confirms that many health facilities lack the basic requirements (eg. commodities) to deliver essential services (Bunde et al., Reference Bunde, Herrera, Chanthala, Posner and Sohkivong2025), and understanding the role of financing in these gaps is critical to addressing them. Strengthening monitoring at the provincial and district level is a priority of the new Health Sector Development Plan (HSDP) 2026–2030 (Ministry of Health, 2025).
We also recognise changing resource allocation practice will need to occur incrementally, perhaps first applied to new rather than existing funding or programmes. In the longer term, this should incorporate transition from donor funding for interventions prioritised by the country.
Structural changes currently underway, including merging MPI into MoF; within MoH combining the nutrition and maternal and child health centres; and transferring administration of NHI to the National Social Security Bureau, should help improve efficiency and coordination within government.
Ultimately ensuring government financing of all essential health services will require increasing the fiscal space for health including through tax reform (World Bank, 2024b), and improving public financing management and budget execution so funds are actually used for their intended purpose. These requirements are discussed in depth elsewhere (World Bank, Reference Bank2018, Reference Bank2019) and are outside the scope of this paper.
7.3. Consolidated supplementary aid
An ‘aid at the margins‘ approach in Lao PDR is likely a long-term goal given the current level and type of health expenditure supported by donors. In the short term, donors can consider eg. gradual tapering of co-payments, informed by evidence of the relative priority of commodities which are currently donor funded, and provide leverage to governments to shift towards domestic first financing more quickly, as additional resources are also mobilised (Drake et al., Reference Drake, Demeshko, Kiros, Memirie, Norheim, Kaddar, Chalkidou, Baker and Yakhelef2025). The aforementioned cost-effectiveness analysis of the EHSP could also inform donor funding.
Donors should also consider how to reduce fragmentation and increase government ownership for overall results of the health sector through joint planning and budgeting (Witter and Baker, Reference Witter and Baker2024) at national and sub-national levels, aligned to the HSDP. A sector wide approach to date not been tested in Lao PDR and could be a medium to longer term consideration. Donors can consider further real or virtual fund pooling similar to the HANSA II project, tied to specific disease or programme outcomes while providing funds recipients (government or other) with greater flexibility in which inputs are funded and how. The next HSDP is also committed to modernising budget estimation, procurement, and investment processes to make them quicker, more transparent, and auditable (Ministry of Health, 2025). If implemented, this should increase donor confidence in PFM systems and feasibility of increased funds pooling including on-budget support. Donors should also clearly stipulate preconditions for pooling or on-budget support to be considered.
The MoH has issued guidelines for managing overseas development assistance (ODA) to improve transparency, and alignment with government strategies (Government of the Lao P.D.R., 2024c) and the ODA Management Information System has been established as the central reporting platform. Participation and compliance across partners and levels of the health system will be critical to New Compact implementation in Lao PDR. Also critical is incorporation of New Compact principles and broader stakeholder engagement in finalising and implementing the HSDP and upcoming revision of the Health Financing Strategy 2026–2030, under leadership of the Department of Planning and Financing within the MoH.
Figure 2 summarises the proposed roadmap towards New Compact implementation in Lao PDR. Additionally specific approaches will be required to gather support for the New Compact principles from key stakeholders as per Table 1. These could include, one, consensus and coalition building by the change team around the new compact approach. Two, conducting modelling and supporting implementation of test cases from national to sub-national levels to demonstrate potential and real health benefits and health financing sustainability through reallocation of current spending. Three, demonstrating how vertical programme outcomes could still be maintained even if a proportion of direct funding is diverted.
8. Conclusion
There is significant opportunity for both GoL and donors to improve health financing for UHC in Lao PDR. In the short term, providing technical assistance for specific use cases on evidence informed priority setting and strengthening GoL-donor coordination behind these priorities will be crucial to creating longer term change.
Acknowledgements
Thank you to Lao Ministry of Health officials who participated in consultations on the New Compact – Dr. Bounxou Keohavong (Director General, Food and Drug Department, Dr. Khamxay Dejluxay (Director General, Department of Health Care and Rehabilitation), Dr. Daodouangchanh Bulommavong (Acting Director General, Cabinet), Dr. Sommana Rattana (Director General, Department of Health Care and Rehabilitation), and Dr. Ketkesone Phrasisombath, Deputy Director, Department of Hygiene & Health Promotion. Thank you to Dr Viengmany Bounkham (Ministry of Health, Lao PDR), Eunkyoung Kim (World Health Organisation, Lao PDR), Chanhsy Samavong and Manav Bhattarai (World Bank, Lao PDR) for useful discussions on the New Compact. Thank you also to Chris Painter (Health Intervention and Technology Assessment Program Foundation, Thailand) and Anastassia Demeshko and Peter Baker (Center for Global Development) for commenting on the manuscript.
Financial support
This study was supported by the Center for Global Development and the Foreign Commonwealth and Development Office. The Lao-Oxford-Mahosot Hospital-Wellcome Trust Research Unit receives core funding from Wellcome.
Competing interests
Tom Drake was employed at the Center for Global Development until September 2025. CGD proposed the New Compact. Bounseuth Keopasith was the Director General, Department of Planning and Finance at the Lao Ministry of Health until the end of 2025. At the time of writing, the authors had no formal financial or institutional relationships that could unduly influence this study.


 Open access
Open access