



Impact statement
This systematic review advances the field of youth mental health promotion by providing a rigorous synthesis of MHL interventions for individuals aged 15–24. Through critical appraisal of 24 studies spanning diverse global contexts, this work elucidates both the strengths and persistent gaps in current intervention strategies. While knowledge gains are a consistent outcome of MHL interventions, improvements in recognition, stigma reduction and help-seeking behaviours are less robust and often contingent upon the inclusion of diagnosis-specific content, contact-based approaches and cultural adaptation. The integration of positive mental health components, though still emerging, represents a promising direction for future work. Importantly, this review not only identifies methodological and contextual limitations such as the predominance of studies from high-income Western countries and the need for greater cultural adaptation and methodological rigour but also highlights the innovative practices and evolving trends within the field. The comprehensive mapping of intervention characteristics, delivery modalities and outcome domains clarifies what is currently effective and brings to light the growing adoption of flexible, multi-modal delivery formats and holistic, youth-centred approaches. By offering a clear framework for future research and practice, this review encourages the expansion of MHL models to include positive mental health, the systematic integration of cultural adaptation and the adoption of standardized, developmentally appropriate outcome measures. The insights generated here are directly relevant to researchers, practitioners and policymakers seeking to design and implement interventions that are not only effective but also equitable and contextually meaningful. Ultimately, this work supports the ongoing evolution of youth mental health promotion, paving the way for interventions that can make a lasting, positive impact on young people’s well-being worldwide.
Background
The World Health Organization (WHO, 2019) defines “youth” as persons between the ages of 15 and 24 years. This developmental stage spans both adolescence and young adulthood, representing a period of significant developmental change, marked by rapid psychosocial shifts, heightened emotional reactivity (Dahl and Gunnar, Reference Dahl and Gunnar2009), increased sensitivity to peer influences (Dahl, Reference Dahl2011) and active search for autonomy and identity (Schumacher and Camp, Reference Schumacher and Camp2010). While these changes are part of normal development, they can trigger or exacerbate mental health problems, particularly in those with pre-existing vulnerabilities (Lök et al., Reference Lök, Bademli and Canbaz2017; McGorry and Purcell, Reference McGorry and Purcell2009). If left unaddressed, these issues can lead to long-term negative impacts that extend beyond the individual to families and society (Lee and Yap, Reference Lee and Yap2024).
Mental health disorders are highly prevalent during this life stage and include conditions such as anxiety, depression, self-harm, suicidal ideation and attempts, substance use disorders and eating disorders (Cohen, Reference Cohen2022; Hoang et al., Reference Hoang, Goldacre and James2014; Madge et al., Reference Madge, Hewitt, Hawton, De Wilde, Corcoran, Fekete, Van Heeringen, De Leo and Ystgaard2008; Pearson et al., Reference Pearson, Janz and Ali2013; UNICEF, 2021). Despite this high burden, most young people experiencing mental health difficulties do not receive timely support, with estimates suggesting that 70–80% of affected youth do not access professional services (Thornicroft, Reference Thornicroft2007). Key barriers include stigma, embarrassment, poor symptom recognition and a preference for self-reliance (Gulliver et al., Reference Gulliver, Griffiths and Christensen2010). These gaps underscore the need for upstream, preventive approaches that enhance young people’s awareness, recognition and confidence in seeking help when needed.
One such approach is to improve their MHL, which Jorm et al. (Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997) originally conceptualized as “knowledge and beliefs about mental disorders which aid their recognition, management or prevention.” Jorm (Reference Jorm2000) further operationalized this concept through three core domains: (1) recognition of specific mental health disorders, (2) knowledge related to general information about mental health (including risk factors, causes and available services) and (3) attitudes towards mental health, including stigma reduction and the promotion of help-seeking behaviour. Over the course of time, MHL interventions have been widely used in schools, communities and public health campaigns to improve knowledge, reduce stigma and increase help-seeking behaviour (Kelly et al., Reference Kelly, Jorm and Wright2007; Lam et al., Reference Lam, Wong and Lam2019; Saxena et al., Reference Saxena, Funk and Chisholm2013).
Despite these contributions, there is now increasing recognition that youth MHL interventions should adopt a more holistic, developmentally appropriate approach. Mental health is defined not solely by the absence of illness but also by the presence of positive mental well-being, resilience and psychological functioning (Galderisi et al., Reference Galderisi, Heinz, Kastrup, Beezhold and Sartorius2015; Seligman, Reference Seligman2018). Strengths-based components such as emotion regulation, coping and self-care are therefore essential to support young people in maintaining mental well-being, not just preventing illness (Bjørnsen et al., Reference Bjørnsen, Espnes, Eilertsen, Ringdal and Moksnes2017; Kutcher et al., Reference Kutcher, Wei and Coniglio2016; Teixeira et al., Reference Teixeira, Coelho, Sequeira, Lluch i Canut and Ferre- Grau2019). While Jorm and colleagues (Jorm, Reference Jorm2012) later expanded the original framework to include prevention strategies, self-help techniques and first-aid skills, most youth MHL interventions continue to focus on Jorm’s (Reference Jorm2000) foundational three domains, though with growing interest in incorporating positive mental health components.
However, systematic evaluation of positive mental health integration within MHL frameworks remains limited. This trend towards broader conceptualizations has generated debate about MHL boundaries, as incorporating diverse constructs, including positive mental health and resilience, may compromise the conceptual coherence of MHL (Jorm, Reference Jorm, Yzer and Siegel2025; Spiker and Hammer, Reference Spiker and Hammer2019) as originally defined. This highlights the need to maintain conceptual clarity while responding to the developmental needs of youth populations who may benefit from more holistic approaches to mental health promotion. Additionally, existing reviews have not comprehensively examined how interventions integrate cultural adaptations or how different delivery modalities influence intervention effectiveness, particularly given the rapid expansion of technology-based approaches.
In the light of these gaps, the current systematic review aimed to provide a comprehensive synthesis of MHL interventions specifically designed for youth aged 15–24 years, as defined by WHO (2019). The review sought to examine intervention characteristics, delivery modalities, cultural adaptations and the integration of positive mental health components within Jorm’s (Reference Jorm2000) three-core-domain MHL framework: recognition, knowledge and attitudes. By systematically mapping global evidence and assessing methodological quality, this review sought to establish a foundation for developing more comprehensive, culturally responsive and developmentally appropriate youth MHL interventions.
Methods
Search strategy
This review intended to identify English-language publications that examined global evidence on MHL interventions for youth aged 15 to 24, with no restrictions placed on publication year or geographical region. A systematic literature search was conducted across multiple electronic scientific databases on 4 September 2024, including CINAHL, APA PsycArticles, APA PsycInfo, Scopus and PubMed.
The search employed a Boolean search strategy across the title, abstract and keywords of articles, using a combination of terms related to youth populations (e.g., adolescents, teenagers, young people, young adults), mental health concepts (e.g., mental health, mental illness, mental well-being, psychological well-being, mental wellness) and intervention-related keywords (e.g., program, prevention, promotion). The search terms were grouped into four main groupings and combined using Boolean operators. The key concepts were:
-
• Group 1: adolescent OR young people OR young person OR young adult OR youth
-
• Group 2: mental health OR mental illness OR mental disorder OR mental wellbeing OR mental well-being OR mental wellness OR psychological OR social OR stigma
-
• Group 3: health literacy OR mental health literacy OR care seeking OR help seeking OR help-seeking OR care-seeking OR behaviour OR knowledge OR recognize OR recognition OR attitude
-
• Group 4: intervention OR program OR prevention OR promotion
A conceptually identical search strategy was applied across all databases. Minor syntax variations reflected differences in database indexing and controlled vocabulary rather than conceptual differences in the search strategy. Full database-specific search strings and search dates are provided in the Supplementary Material.
Protocol and registration
This systematic review adhered to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021) to ensure methodological rigour and transparency. No review protocol was prospectively registered in PROSPERO or other systematic review databases prior to the commencement of this study.
Data extraction and analysis
This systematic review was guided by four primary research questions: (1) What are the characteristics and effectiveness of MHL interventions specifically targeting youth aged 15–24 years? (2) How do different delivery modalities (in-person, digital, blended) influence intervention outcomes and accessibility? (3) To what extent do current interventions incorporate cultural adaptations and positive mental health components? (4) What is the methodological quality of existing MHL intervention research for this population?
These research questions were operationalized using a PICOS framework. The population (P) comprised youth aged 15–24 years as defined by the WHO (2019), without restrictions on gender, ethnicity or geographical location. This age range encompasses late adolescence and emerging adulthood, representing a critical developmental period for mental health intervention. Studies involving participants with comorbid conditions likely to independently confound mental health outcomes were excluded to strengthen internal validity, including chronic medical illnesses, neurological disorders, severe physical disabilities, substance use disorders, intellectual disabilities and severe sensory impairments.
Eligible interventions addressed at least one primary outcome related to changes in MHL domains, which encompassed (1) recognition of specific mental health disorders; (2) knowledge related to general information about mental health (including risk factors, causes and available services); and (3) attitudes towards mental health, including stigma reduction and the promotion of help-seeking behaviour. These three domains aligned with Jorm’s (Reference Jorm2000) foundational framework and represented the predominant focus of youth MHL interventions. Interventions incorporating positive mental health components such as resilience, coping skills and well-being promotion were also eligible. For studies reporting multiple outcomes, only those emphasizing MHL outcomes as primary were included.
Comparison conditions (C) included waitlist controls, treatment as usual, no intervention controls or active comparison conditions. Single-group pre-post designs without control groups were also included given the exploratory nature of many MHL intervention research. Primary outcomes (O) measured changes in any of the three core MHL domains, while secondary outcomes included positive mental health indicators, help-seeking intentions or behaviours, and measures of cultural adaptation effectiveness where reported. Eligible study designs (S) comprised randomized controlled trials (RCTs), cluster-randomized trials, quasi-experimental studies, non-RCTs and feasibility trials. Studies with fewer than three participants were excluded to minimize selection bias and avoid over-pathologizing outcomes (Lee et al., Reference Lee, Yap and Ho2025), a step taken to enhance the overall reliability of findings.
The screening process involved four independent researchers working in two pairs to assess titles and abstracts for relevance. A fifth researcher was available to resolve any conflicts or disagreements. Full-text articles were retrieved for any studies that appeared to meet the inclusion criteria or where eligibility remained unclear following the initial screening. Full-text reviews followed the same conflict resolution process, with the fifth researcher providing arbitration if needed. Inter-rater agreement was monitored throughout the screening process to ensure consistency in study selection decisions. No automation or machine-learning tools were used at any stage of screening or exclusion; all records were reviewed manually by human reviewers.
During data extraction, each MHL domain was operationalized distinctly to ensure accurate coding. Recognition was coded separately only when studies explicitly assessed participants’ ability to identify specific symptoms, mental health conditions or mental health problems as a distinct outcome measure. Knowledge was coded when studies assessed participants’ understanding of general information about mental health, including risk factors, causes, prevalence and available services. Attitudes were coded when studies measured stigma, help-seeking intentions or beliefs about mental health treatment. Cultural adaptation was not assessed using predetermined criteria but emerged as a notable theme during data extraction. Interventions were identified as culturally adapted when they explicitly described modifications to content, delivery methods or personnel to align with specific cultural, linguistic or community contexts.
Relevant data, including study characteristics (e.g., publication year, country, study design), population details (e.g., age, gender, cultural background), intervention specifics (e.g., format, delivery method, duration) and outcome measures mapped to MHL domains, were extracted using a standardized Covidence data extraction template and collated into summary table (see Supplementary Table for details).
Outcome data across included studies were characterized by substantial heterogeneity in study design, outcome measures and statistical reporting. While all studies reported sufficient outcome information to allow classification of intervention effects at the domain level, reporting of statistical indices (e.g., effect sizes, confidence intervals) was inconsistent. To ensure standardization and comparability across studies, quantitative effect sizes were therefore not extracted or synthesized. Instead, outcomes were synthesized using a structured narrative approach, categorizing intervention effects within each MHL domain as demonstrating positive improvement, mixed or partial findings, or no significant change, based on the direction and statistical significance of results as reported by the original authors. This approach was consistent with PRISMA guidance for narrative synthesis, where meta-analysis is not appropriate due to heterogeneity in intervention content, outcome measures and reporting practices.
Methodological quality
Risk of bias for the included studies was assessed using Covidence’s quality assessment tool, which evaluates biases from: 1) sequence generation, 2) allocation concealment, 3) blinding of participants and personnel, 4) blinding of outcome assessment, 5) incomplete outcome data, 6) selective outcome reporting and 7) any other source if any. Each domain was rated as high, low or unclear by four independent researchers working in two pairs, with disagreements resolved through discussion or, when necessary, consultation with the fifth researcher, consistent with the screening and full-text review processes. The level of evidence for each study was determined using the National Health and Medical Research Council (NHMRC, 2009) evidence hierarchy. This hierarchy ranged from Level I (systematic reviews of Level II studies) to Level IV (case series with post-test or pre-test/post-test outcomes). Since this review focused on original intervention studies, reviews and case series were excluded. The included evidence comprised Level II studies (RCTs), Level III-1 studies (pseudo-RCTs), Level III-2 studies (comparative studies with a concurrent control group) and Level III-3 studies (comparative studies lacking a concurrent control group). This review was based solely on publicly available literature, so ethical approval was not required.
Results
Study selection and characteristics
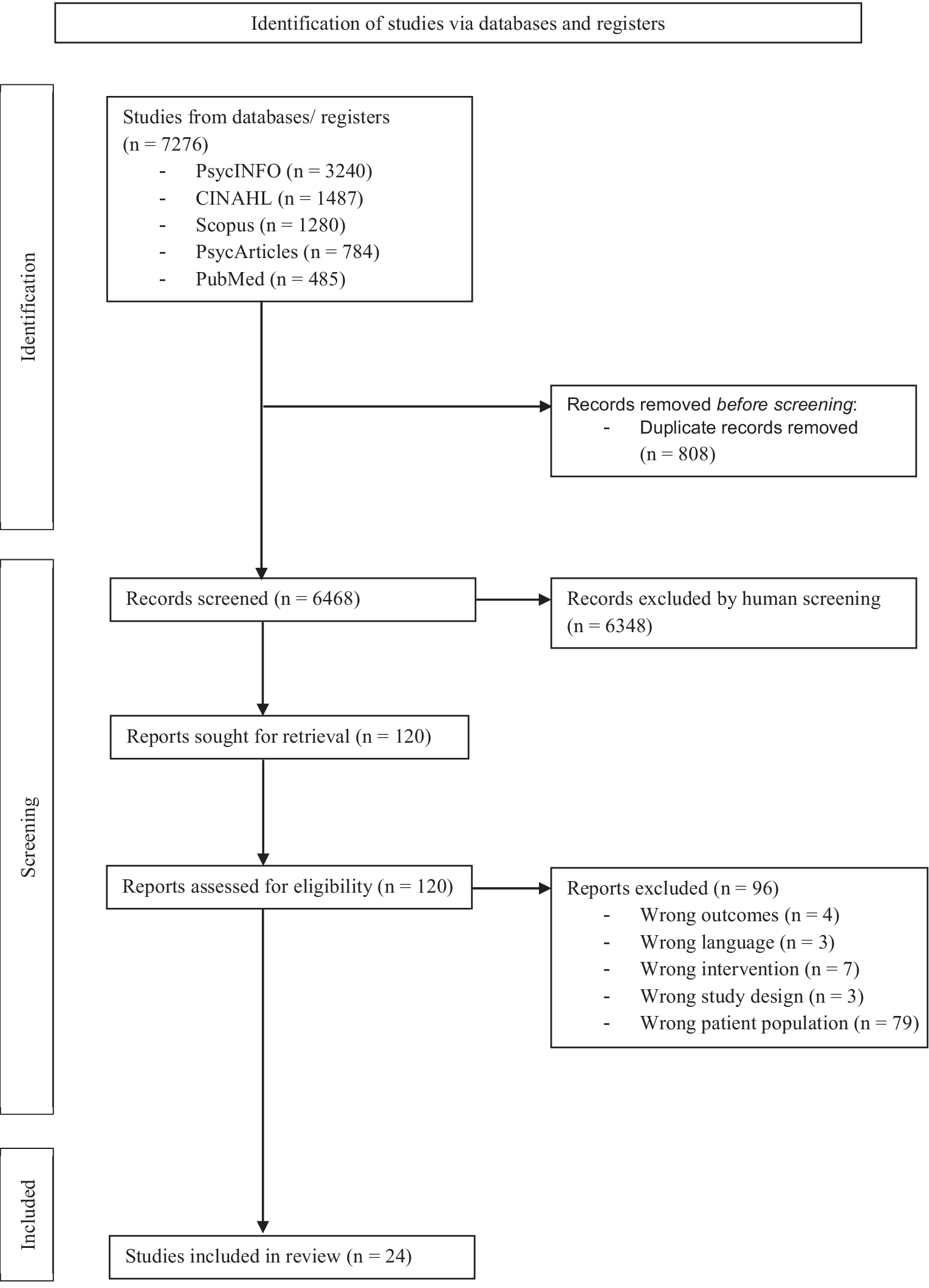
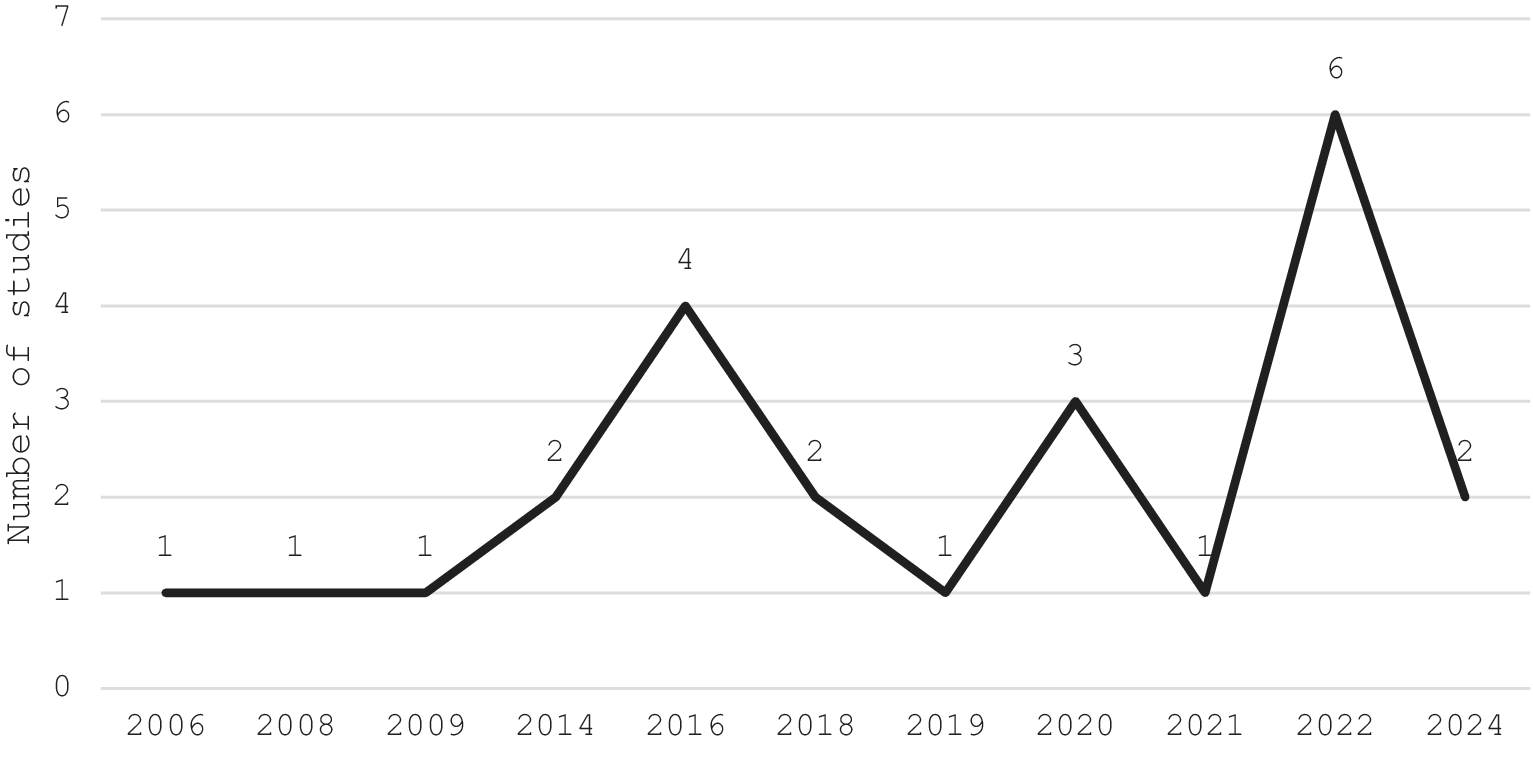
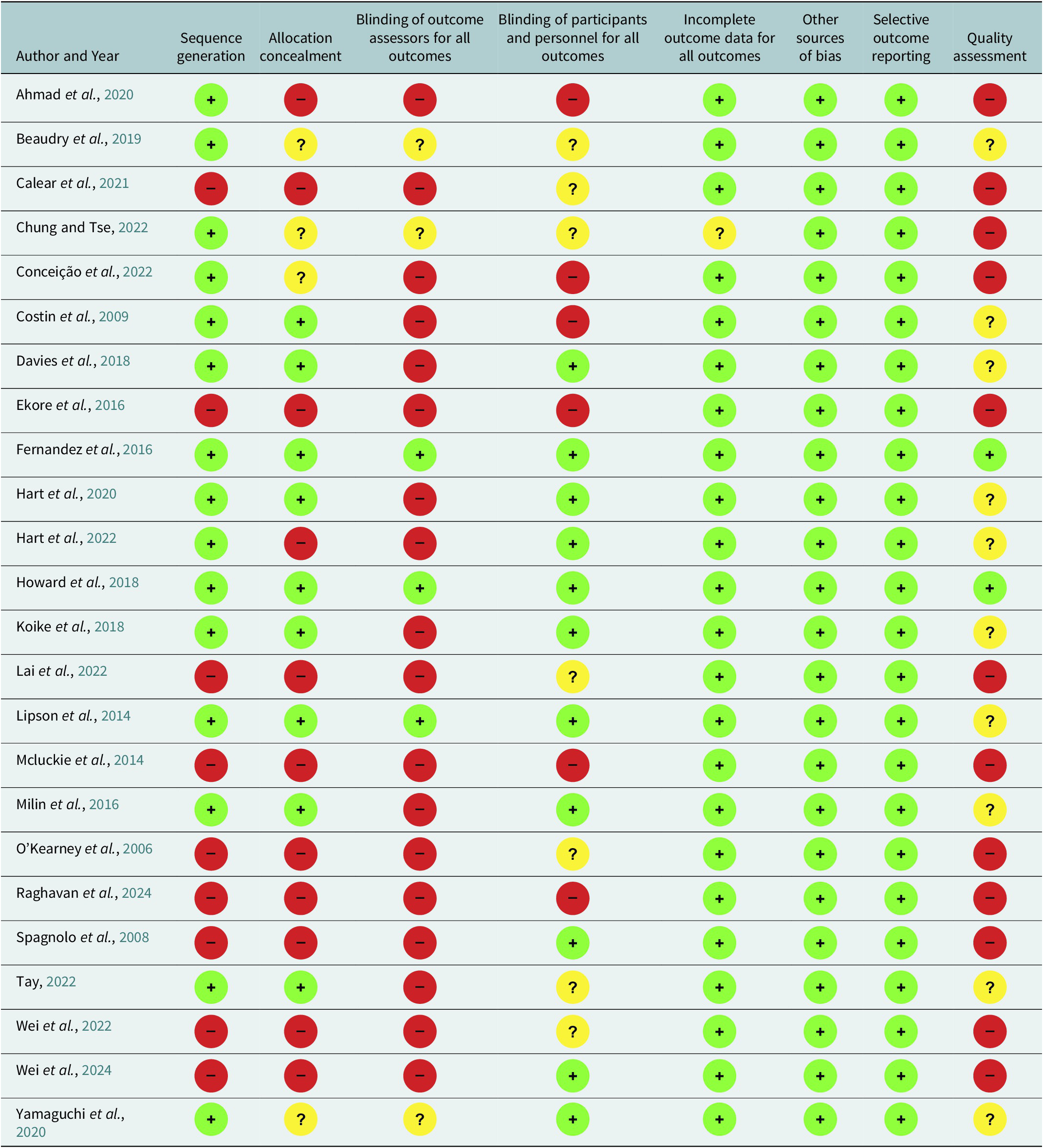
A total of 7,276 records were retrieved, of which 24 studies met the inclusion criteria and were retained for analysis (see Figure 1 for the PRISMA flowchart). All studies applied intention-to-treat analyses and together enrolled 13,624 participants (M range = 20 to 2,543 per study). Publication years spanned from 2006 to 2024, with a marked rise in 2022 (see Figure 2). Of the 24 studies, 23 (95.8%; e.g., Davies et al., Reference Davies, Beever and Glazebrook2018; O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006) sampled youth in educational settings; only Costin et al. (Reference Costin, Mackinnon, Griffiths, Batterham, Bennett, Bennett and Christensen2009) recruited from the general public via the electoral roll. An overview of the risk of bias and methodological quality for the 24 included studies is presented in Table 1. Among these, two studies were evaluated as having a low risk of bias and were deemed to be of high methodological quality. Ten studies were categorized as having an unclear, indeterminable, inapplicable or unreported risk of bias. The remaining twelve studies were assessed as having a high risk of bias and were of low quality. The level of evidence for each study, as classified according to the NHMRC hierarchy, is summarized in the Supplementary Table. Fourteen studies were identified as Level II evidence (e.g., Beaudry et al., Reference Beaudry, Swartz, Miller, Schweizer, Glazer and Wilcox2019; Howard et al., Reference Howard, Griffiths, McKetin and Ma2018), one study as Level III-1 (Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020), three studies as Level III-2 (Calear et al., Reference Calear, Morse, Batterham, Forbes and Banfield2021; O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006; Wei et al., Reference Wei, Kutcher, Austen, Comfort, Gilham, MacDougall, McKenna, McKinnon, Thompson, Yeo, Zhang, Baxter and Matheson2022), and six studies as Level III-3 (e.g., Mcluckie et al., Reference Mcluckie, Kutcher, Wei and Weaver2014; Wei et al., Reference Wei, Gilham and Kutcher2024).
PRISMA flowchart.

Distribution of studies across publication years.

Risk of bias assessment. The risk of bias of the included studies was assessed using Covidence’s quality assessment tool

Note: Green circle: low risk; yellow circle: unclear, cannot be determined, not applicable or not reported; red circle: high risk.
Fifteen studies (62.5%; e.g., Chung and Tse, Reference Chung and Tse2022; Tay, Reference Tay2022) used RCT designs, of which five were cluster-randomized (e.g., Hart et al., Reference Hart, Cropper, Morgan, Kelly and Jorm2020; Lipson et al., Reference Lipson, Speer, Brunwasser, Hahn and Eisenberg2014). Nine studies (37.5%; e.g., Raghavan et al., Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024; Wei et al., Reference Wei, Gilham and Kutcher2024) were quasi-experimental, of which six were without control groups (e.g., Mcluckie et al., Reference Mcluckie, Kutcher, Wei and Weaver2014; Spagnolo et al., Reference Spagnolo, Murphy and Librera2008). According to the adapted NHMRC hierarchy, two studies (8.3%; Fernandez et al., Reference Fernandez, Tan, Knaak, Chew and Ghazali2016; Howard et al., Reference Howard, Griffiths, McKetin and Ma2018) were rated as having a low risk of bias, 12 (50%; e.g., Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006) high risk and ten (41.7%; e.g., Davies et al., Reference Davies, Beever and Glazebrook2018; Wei et al., Reference Wei, Gilham and Kutcher2024) unclear. Fourteen studies (58.3%) provided Level II evidence, one (4.2%) Level III-1, three (12.5%) Level III-2 and six (25.0%) Level III-3, reflecting a predominance of moderate-quality experimental designs supplemented by several rigorous randomized trials.
Intervention modes
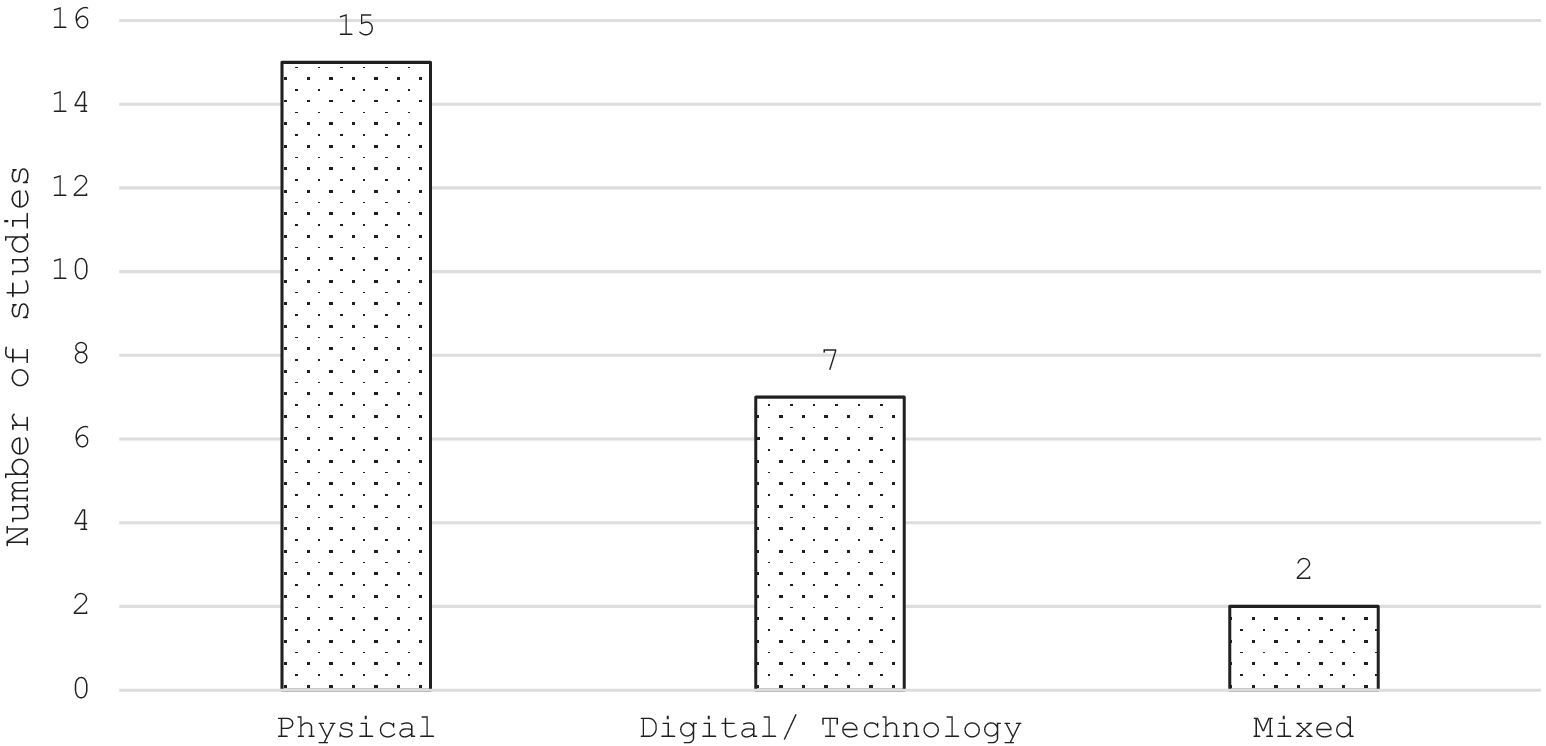
Twenty-three interventions employed a psychoeducational framework; only one study (O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006) explicitly grounded its content in a cognitive–behavioural therapy “MoodGYM” model. Delivery formats fell into three clear categories: 15 interventions (62.5%) were delivered exclusively in person, including through lectures, role-plays or small-group discussions (e.g., Ekore et al., Reference Ekore, Abdulmalik, Ajuwon and Bella-Awusah2016; Lai et al., Reference Lai, Lien, Chen and Lin2022); seven (29.2%) were digital-only, utilizing self-paced e-learning modules, mobile applications or filmed social contact (O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006; Tay, Reference Tay2022); and two (8.3%) adopted blended designs that combined online activities with face-to-face components (Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Know Before You Go: Wei et al., Reference Wei, Gilham and Kutcher2024).
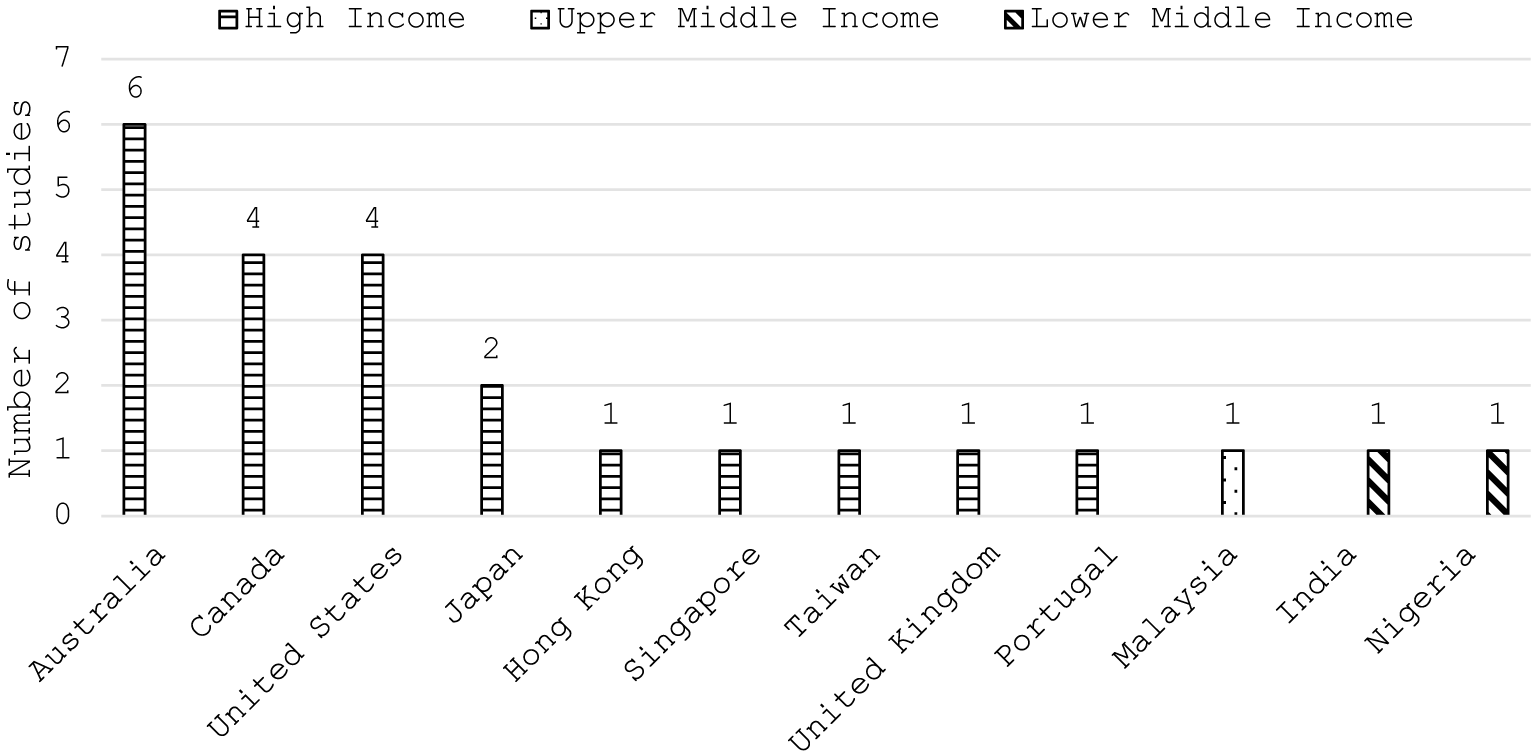
The current review also applied the World Bank’s economy classification and categorized the countries of study implementation based on gross national income (GNI) per capita into three income categories: high income, upper middle income, and low and lower middle income (a similar approach was adopted in Lee et al., Reference Lee, Yap and Ho2025). Most interventions (n = 14; 58.3%) occurred in high-income Western countries: Australia (n = 6), the United States (n = 4) and Canada (n = 4). One study (4.2%) was conducted in an upper-middle-income country (Malaysia) and two (8.3%) in low- or lower–middle-income countries (LMICs, including India and Nigeria). The geographical concentration revealed the prevalence of digital-only MHL interventions, especially in high-income Western contexts, whereas physical and blended formats appeared across both high- and lower-resource contexts, illustrating an economic imbalance in the MHL evidence base (see Figure 3). Despite these disparities, the results suggested a growing international commitment to enhancing youth MHL, with studies spanning diverse cultural and geographical contexts including Asia, Africa, Europe, North America and Oceania. This signals a shared recognition of youth MHL as a public health priority.
Distribution of studies across countries.

Targeted MHL domains
Content analyses were organized around the three core MHL domains, specifically (1) recognition of specific mental health disorders; (2) knowledge related to general information about mental health (including risk factors, causes and available services); and (3) attitudes towards mental health, including stigma reduction and the promotion of help-seeking behaviour. Most interventions (18/24; 75.0%) covered all three domains, reflecting a dominant triadic approach in the field. Every study (24/24; 100%) targeted knowledge, covering definitions, causes, prevalence and service pathways. Seventeen interventions (70.8%; e.g., Chung and Tse, Reference Chung and Tse2022; Fernandez et al., Reference Fernandez, Tan, Knaak, Chew and Ghazali2016) incorporated attitudinal or stigma-reduction components, such as social-distance measures and assessments of personal and perceived stigma. Of the 18 studies (75.0%) that incorporated a recognition component, ten (54.2%; e.g., Beaudry et al., Reference Beaudry, Swartz, Miller, Schweizer, Glazer and Wilcox2019; Davies et al., Reference Davies, Beever and Glazebrook2018) focused exclusively on identifying symptoms of mental health issues. In contrast, eight studies (20.8%; e.g., O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006; Wei et al., Reference Wei, Gilham and Kutcher2024) combined disorder recognition with positive mental health competencies such as stress management, emotion regulation and interpersonal effectiveness.
Intervention effectiveness
Recognition
Eighteen studies incorporated recognition of mental health issues as part of their target MHL approach. Of these, ten studies (55.6% of the total sample; 83.3% of recognition-focused studies) demonstrated clear improvements in recognition outcomes, typically reflected in increased accuracy in identifying symptoms or mental health conditions from vignettes or structured items. Examples include Davies et al. (Reference Davies, Beever and Glazebrook2018) and Beaudry et al. (Reference Beaudry, Swartz, Miller, Schweizer, Glazer and Wilcox2019), which reported significant post-intervention gains in correct identification of mental health problems, as well as Chung and Tse (Reference Chung and Tse2022), where participants showed improved recognition following a contact-based human library intervention. In contrast, three studies (16.7%) reported mixed or limited recognition effects. These studies typically embedded recognition within broader well-being or skills-based interventions, making recognition effects difficult to isolate. For instance, O’Kearney et al. (Reference O’Kearney, Gibson, Christensen and Griffiths2006) emphasized mood management within a CBT-based digital programme, while Wei et al. (Reference Wei, Gilham and Kutcher2024) combined disorder recognition with positive mental health competencies, reporting improvements that were not specific to recognition alone. The remaining six studies did not assess recognition outcomes and were therefore excluded from recognition analyses.
Knowledge
All studies (24/24; 100%) assessed mental health knowledge as a core outcome, making this the most consistently evaluated MHL domain. Twenty-one studies (87.5%) reported clear positive improvements in knowledge related to mental health definitions, causes, risk factors or service awareness. For example, Lai et al. (Reference Lai, Lien, Chen and Lin2022) and Fernandez et al. (Reference Fernandez, Tan, Knaak, Chew and Ghazali2016) demonstrated significant gains in participants’ understanding of mental health conditions and available support pathways following psychoeducational interventions. The remaining three studies (12.5%) reported mixed or modest knowledge gains, often where baseline knowledge levels were already high or where knowledge outcomes were secondary to attitudinal or skills-based objectives. Overall, knowledge gains were observed across physical, digital and blended delivery formats.
Attitudes
Seventeen studies evaluated attitudinal outcomes, including stigma-related beliefs or help-seeking attitudes. Of these, twelve studies (70.6%) demonstrated positive attitudinal change, most commonly reductions in personal or perceived stigma. Interventions incorporating contact-based elements were particularly prominent among those showing positive effects. For example, Chung and Tse (Reference Chung and Tse2022) and Calear et al. (Reference Calear, Morse, Batterham, Forbes and Banfield2021) reported improvements in stigma-related measures following exposure to lived-experience narratives. However, five studies (29.4%) reported mixed or non-significant attitudinal effects, particularly for help-seeking outcomes. In several cases, improvements were observed for stigma-related attitudes but not for intentions to seek professional help, highlighting variability across attitudinal subdomains.
Sustainability of effects at follow-up
Eighteen studies included follow-up assessments. Among these, ten studies (55.6%) demonstrated sustained intervention effects, most frequently for knowledge-related outcomes (e.g., Calear et al., Reference Calear, Morse, Batterham, Forbes and Banfield2021; Davies et al., Reference Davies, Beever and Glazebrook2018). The remaining eight studies (44.4%) reported mixed or attenuated effects at follow-up, with attitudinal and help-seeking outcomes more likely to diminish over time. This pattern suggests that while short-term gains are common, longer-term maintenance is less consistently achieved across MHL domains.
Effectiveness by delivery mode
Among the 15 face-to-face interventions, 13 studies (86.7%) reported positive effects on at least one MHL domain, with several demonstrating improvements in stigma-related attitudes (e.g., Ekore et al., Reference Ekore, Abdulmalik, Ajuwon and Bella-Awusah2016; Lai et al., Reference Lai, Lien, Chen and Lin2022). Of the seven digital-only interventions, five studies (71.4%) demonstrated positive outcomes, primarily for knowledge and recognition (e.g., Davies et al., Reference Davies, Beever and Glazebrook2018; Tay, Reference Tay2022), while two reported mixed effects, particularly for attitudinal measures. Both blended interventions (2/2; 100%) demonstrated positive outcomes across multiple domains (e.g., Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Wei et al., Reference Wei, Gilham and Kutcher2024), though conclusions are limited by small numbers.
Diagnostic focus and cultural adaptation
Among the 12 diagnosis-specific interventions, ten studies (83.3%) demonstrated positive recognition outcomes (e.g., Beaudry et al., Reference Beaudry, Swartz, Miller, Schweizer, Glazer and Wilcox2019; Hart et al., Reference Hart, Cropper, Morgan, Kelly and Jorm2020), compared to five of the 12 transdiagnostic interventions (41.7%), suggesting stronger recognition effects when diagnostic content was explicitly included. Cultural adaptations were explicitly reported in five studies (20.8%), all of which demonstrated positive outcomes in at least one MHL domain. These adaptations commonly involved incorporating individuals with lived experience into programme development or delivery, enhancing cultural congruence and aligning intervention content with participants’ social and cultural contexts. Notably, four of these five studies (80.0%) reported improvements in attitudinal or stigma-related outcomes (e.g., Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Raghavan et al., Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024), whereas one culturally adapted intervention demonstrated improvements limited to knowledge and recognition outcomes (Spagnolo et al., Reference Spagnolo, Murphy and Librera2008). By comparison, 10 of 19 non-adapted interventions (52.6%) reported attitudinal improvements, indicating a potential advantage of culturally tailored approaches for affective MHL outcomes.
Discussion
Taken together, the intervention effectiveness findings indicated that youth MHL interventions most consistently improved mental health knowledge, showed more variable effects on recognition outcomes and demonstrated the greatest heterogeneity in attitudinal and help-seeking outcomes. Knowledge gains were observed across nearly all studies and delivery formats, whereas recognition improvements were more pronounced in diagnosis-specific interventions and less consistently demonstrated in transdiagnostic approaches. Attitudinal outcomes, particularly stigma reduction and help-seeking intentions, showed mixed effects and appeared more sensitive to intervention features such as contact-based components and cultural adaptation. Given the predominance of moderate-to-high risk of bias across studies, these patterns were interpreted as indicative of relative strengths and limitations across intervention approaches rather than as definitive evidence of efficacy. Risk-of-bias assessments were therefore used to contextualize the reliability of observed effects and to support cautious identification of intervention features that appear promising, while acknowledging constraints imposed by study quality.
Heterogeneity in intervention delivery mode
Examining delivery modalities across diverse economic contexts revealed significant global patterns in how MHL interventions were implemented and accessed. Among the reviewed studies, a notable pattern emerged in terms of delivery modes: 15 out of 24 interventions primarily utilized physical formats, often delivered through face-to-face sessions in school or community settings. This included programmes such as the Mental Health Gap Action Programme (mhGAP), the Human Library intervention and Silence is Deadly, which employed varied physical approaches including facilitator-led training, live presentations, in-person sharing of experience and open discussions (Calear et al., Reference Calear, Morse, Batterham, Forbes and Banfield2021; Chung and Tse, Reference Chung and Tse2022; Ekore et al., Reference Ekore, Abdulmalik, Ajuwon and Bella-Awusah2016). This physical mode of delivery appeared to offer several advantages for youth populations. In-person formats allow for real-time interaction with facilitators, enabling the immediate clarification of misconceptions, adaptive delivery in response to participants’ needs and reinforcement of learning through guided discussion (Jorm, Reference Jorm2012; Wei et al., Reference Wei, Hayden, Kutcher, Zygmunt and McGrath2013). These settings also facilitate peer engagement, which can foster group cohesion and reduce stigma through shared experiences (Gulliver et al., Reference Gulliver, Griffiths and Christensen2010). Many physical interventions incorporated experiential learning strategies such as role-playing, group discussions and scenario-based exercises, which have been shown to improve knowledge retention and develop practical skills in help-seeking and emotion regulation (Koller and Bertel, Reference Koller and Bertel2006; Pinfold et al., Reference Pinfold, Toulmin, Thornicroft, Huxley, Farmer and Graham2003).
There was also a marked geographical concentration from this review where digital interventions were more frequently implemented in high-income Western countries such as Australia, the United States and the United Kingdom. This pattern aligns with global trends in MHL research. For instance, a recent meta-analysis by Yeo et al. (Reference Yeo, Reich, Liaw and Chia2023) reported that digital MHL programmes are disproportionately concentrated in high-income Western countries, where broader infrastructural advantages make implementation more feasible. In the United States, for example, 85% of individuals own a smartphone and 77% have broadband access, enabling greater accessibility to digital interventions in these contexts. Reported advantages of digital delivery in these contexts likely reflect scalability, flexibility and infrastructure availability rather than the inherent superiority of digital formats. Self-paced programmes, such as MoodGYM, HOPE and the e-learning version of Mental Health First Aid (MHFA), allow participants to engage with content at their own pace and according to individual comprehension levels (Davies et al., Reference Davies, Beever and Glazebrook2018; O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006; Tay, Reference Tay2022). Moreover, video-based formats and online modules are cost-effective and capable of reaching wide audiences. When digital programmes include interactive components or social contact (e.g., contact with a facilitator or credible presenter), they have shown outcomes comparable to in-person interventions in terms of improving knowledge, reducing stigma and promoting help-seeking (Conceição et al., Reference Conceição, Rothes and Gusmão2022; Koike et al., Reference Koike, Yamaguchi, Ojio, Ohta, Shimada, Watanabe, Thornicroft and Ando2018; Yeo et al., Reference Yeo, Reich, Liaw and Chia2023).
However, the increased reliance on digital formats creates significant equity concerns. Youths in low-resource settings may face limited internet access, lower levels of digital literacy and weaker infrastructure to support online platforms (WHO, 2022). Even within high-income settings, digital access is not equally distributed. Robin and colleagues (Robinson et al., Reference Robinson, Cotten, Ono, Quan-Haase, Mesch, Chen, Schulz, Hale and Stern2015) caution that broadband connectivity varies significantly by income level, educational attainment and rural versus urban residence. Additionally, digital content that lacks cultural or linguistic adaptation may be less relatable and less effective, particularly for minority or underserved groups (Ellis et al., Reference Ellis, Draheim and Anderson2022). This geographical concentration reflects the dominance of Western models in MHL research, potentially limiting global applicability and highlighting critical gaps in evidence from LMICs. The economic disparity between high-income settings favouring digital formats and LMICs with limited digital infrastructure presents substantial challenges for programme scalability and accessibility. In such contexts, physical formats or blended models combining digital and face-to-face elements may prove more appropriate and effective where technology access remains constrained.
In light of these considerations, the current findings support the use of a mixed delivery model as a viable and equitable approach. Hybrid programmes that combine the strengths of both digital and physical modes, for example, blending online modules with in-person classroom activities, can enhance accessibility while preserving the interpersonal benefits of face-to-face delivery (Wei et al., Reference Wei, Gilham and Kutcher2024). Crucially, the choice of delivery mode should be matched to local contexts and resource availability, with interactive digital interventions suited to high-income settings and physical formats remaining more practical in low-resource environments. A flexible, context-sensitive approach is essential for optimizing the global reach and impact of MHL programmes.
Distribution of MHL domains
The analysis of 24 included studies integrating Jorm’s (Reference Jorm2000) three core domains provided an insight into current content priorities and effectiveness approaches. The current review found that most programmes aligned with the core components of MHL. However, there was a marked emphasis on the dissemination of factual knowledge about mental health conditions. A majority of interventions focused on increasing awareness of symptoms, causes and evidence-based treatments for a wide range of mental health issues, including depression, anxiety, suicide, psychosis, schizophrenia, substance use and eating disorders (e.g., Hart et al., Reference Hart, Cropper, Morgan, Kelly and Jorm2020; Hart et al., Reference Hart, Morgan, Rossetto, Kelly, Gregg, Gross, Johnson and Jorm2022; Lipson et al., Reference Lipson, Speer, Brunwasser, Hahn and Eisenberg2014; Yamaguchi et al., Reference Yamaguchi, Ojio, Foo, Michigami, Usami, Fuyama, Onuma, Oshima, Ando, Togo and Sasaki2020). These programmes typically aimed to enhance the recognition of specific disorders by educating participants on symptom profiles, diagnostic criteria and available treatment options. For instance, Costin et al. (Reference Costin, Mackinnon, Griffiths, Batterham, Bennett, Bennett and Christensen2009) incorporated outcome measures related to depression recognition and help-seeking knowledge. However, their findings indicated no significant improvement in symptom recognition following a brief e-card intervention, highlighting the challenge of achieving substantive outcomes through short-form educational tools.
Attitudes towards mental illness, particularly stigma and willingness to seek help, emerged as the second most addressed domain. Roughly half of the reviewed programmes incorporated content or measured outcomes related to stigma reduction or the normalization of mental health help-seeking (e.g., peer norms, trust in professionals). Some of these interventions employed contact-based strategies, such as personal narratives or video testimonials from individuals with lived experience of mental illness, which are widely recommended for effectively reducing stigma (Seedaket et al., Reference Seedaket, Turnbull, Phajan and Wanchai2020). However, these components were not always integrated in a sustained or theoretically grounded manner, and stigma-related outcomes were frequently secondary rather than primary endpoints.
The domain of recognition, defined as the ability to identify when oneself or another person may be experiencing a mental health problem, was often implicitly covered within the broader knowledge category but rarely examined as a standalone target (e.g., Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Beaudry et al., Reference Beaudry, Swartz, Miller, Schweizer, Glazer and Wilcox2019; Ekore et al., Reference Ekore, Abdulmalik, Ajuwon and Bella-Awusah2016; Mcluckie et al., Reference Mcluckie, Kutcher, Wei and Weaver2014; Milin et al., Reference Milin, Kutcher, Lewis, Walker, Wei, Ferrill and Armstrong2016; Yamaguchi et al., Reference Yamaguchi, Ojio, Foo, Michigami, Usami, Fuyama, Onuma, Oshima, Ando, Togo and Sasaki2020; Wei et al., Reference Wei, Kutcher, Austen, Comfort, Gilham, MacDougall, McKenna, McKinnon, Thompson, Yeo, Zhang, Baxter and Matheson2022). A minority of studies explicitly assessed whether participants could accurately recognize symptoms of mental health issues or knew how and where to access appropriate services (e.g., Costin et al., Reference Costin, Mackinnon, Griffiths, Batterham, Bennett, Bennett and Christensen2009; Hart et al., Reference Hart, Cropper, Morgan, Kelly and Jorm2020; Lai et al., Reference Lai, Lien, Chen and Lin2022). This limited attention to recognition is important, given that accurate identification of mental health issues is a necessary precondition for effective help-seeking and early intervention.
A smaller subset of interventions incorporated components aimed at fostering positive mental health or the cultivation of skills related to emotional resilience, coping and stress management. Notably, only a limited number of studies (e.g., Lai et al., Reference Lai, Lien, Chen and Lin2022) explicitly incorporated components aimed at strengthening protective factors or teaching strategies for mental health maintenance, which are increasingly recognized as essential elements of a more holistic, strengths-based approach to MHL. This signals a persistent gap in the field, where many interventions remain deficit-oriented and fail to systematically promote mental wellness or resilience (Bjørnsen et al., Reference Bjørnsen, Espnes, Eilertsen, Ringdal and Moksnes2017; Kutcher et al., Reference Kutcher, Wei and Coniglio2016; Teixeira et al., Reference Teixeira, Coelho, Sequeira, Lluch i Canut and Ferre- Grau2019).
Cultural adaptation: A persistent blind spot
Assessment of cultural responsiveness across the reviewed interventions highlighted an important limitation in the current evidence base, but one that required careful interpretation given the geographical distribution of studies. As shown in Figure 3, most included interventions were implemented in high-income Western countries, where cultural adaptation may not be necessary in all cases. However, across the literature, explicit reporting of cultural or contextual tailoring was uncommon, including limited description of linguistic adaptation, culturally grounded framings of mental health and distress, or structured adaptation processes (e.g., stakeholder co-design, formative qualitative work or culturally specific case vignettes). Only five studies explicitly documented cultural adaptation (Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Calear et al., Reference Calear, Morse, Batterham, Forbes and Banfield2021; Conceição et al., Reference Conceição, Rothes and Gusmão2022; Raghavan et al., Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024; Spagnolo et al., Reference Spagnolo, Murphy and Librera2008). This scarcity constrained interpretation of transferability and scalability, particularly for implementation in culturally and linguistically diverse youth populations and in low- and middle-income settings where explanatory models of distress, help-seeking pathways and service availability may differ substantially (see Figure 4).
Distribution of intervention delivery modes.

This limitation is particularly salient given the growing body of research underscoring the central role of culture in shaping how mental health is perceived, discussed and responded to (Kågström et al., Reference Kågström, Juríková and Guerrero2023). Many interventions adopted Western diagnostic categories, help-seeking norms and individualistic coping models, which may have variable cultural transferability across different sociocultural contexts. Mental health constructs such as depression, anxiety and psychosis are not necessarily understood, experienced or described in the same way across cultures (U.S. Department of Health and Human Services, 2001). For example, somatization often functions as an “idiom of distress” in cultures where overt emotional expression is inhibited and psychiatric stigma remains pervasive (Kleinman, Reference Kleinman1977). Additionally, the Western emphasis on self-disclosure and individual agency in help-seeking may not resonate in contexts where family-based decision-making or spiritual healing practices are predominant (Atilola, Reference Atilola2015; Furnham and Hamid, Reference Furnham and Hamid2014). When applied beyond their original contexts, MHL interventions that privilege Western models of mental health may risk marginalizing indigenous belief systems, alternative healing traditions and culturally specific idioms of distress (Bhatia and Ram, Reference Bhatia and Ram2009). Therefore, it is essential to understand culture not as a fixed or singular entity but as a complex, evolving tapestry of internalized values, social norms, behaviours and meaning-making systems (Kaiser and Kohrt, Reference Kaiser and Kohrt2019).
Only a minority of interventions in the current review (Ahmad et al., Reference Ahmad, Leventhal, Nielsen and Hinshaw2020; Calear et al., Reference Calear, Morse, Batterham, Forbes and Banfield2021; Conceição et al., Reference Conceição, Rothes and Gusmão2022; Raghavan et al., Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024; Spagnolo et al., Reference Spagnolo, Murphy and Librera2008) explicitly integrated sociocultural tailoring by involving individuals with lived mental health experience in both programme design and delivery. This participatory approach enhanced cultural congruence and ensured that content resonated with participants’ local norms and values. These contact-based strategies sought to reduce stigma and foster relatability by embedding first-person narratives of navigating mental health challenges within the context of local services and community practices (Chung and Tse, Reference Chung and Tse2022; Fernandez et al., Reference Fernandez, Tan, Knaak, Chew and Ghazali2016; Spagnolo et al., Reference Spagnolo, Murphy and Librera2008). For example, Calear et al. (Reference Calear, Morse, Batterham, Forbes and Banfield2021) developed materials specifically to challenge prevailing masculine norms that impede help-seeking among adolescent males, thereby illustrating how gender-sensitive adaptations can improve both relevance and impact.
Additionally, differences in national healthcare systems and service availability further underscore the importance of contextual adaptation. As noted by WHO (2021), many LMICs experience limited governmental investment in mental health services, which restricts public access to adequate care. This structural barrier highlights the need for MHL interventions to include locally relevant information about accessible services and to address culturally embedded barriers to help-seeking. In sum, to maximize both acceptability and effectiveness, MHL interventions must be culturally responsive, incorporating the language, values and realities of the populations they aim to serve.
Beyond knowledge: Towards holistic and culturally responsive MHL
One of the most striking findings of this review is the disconnect between the inclusion of positive mental health content and the evaluation of corresponding outcomes: although eight interventions incorporated positive mental health or life-skills components, only one study explicitly measured positive mental health outcomes. This mismatch between intervention content and outcome measurement represented one of the clearest empirical gaps identified in the current evidence base and substantially limited conclusions about whether broader, strengths-based MHL approaches confer added benefit beyond traditional knowledge-focused models.
Taken together with the domain distribution and cultural adaptation findings, the current evidence emphasized the importance of interventions evolving beyond traditional frameworks. As identified in the present review, all 24 MHL interventions incorporated the delivery of mental health knowledge such as causes and risk factors of mental disorders, as well as pathways to care, as core psychoeducational content. This underscores the centrality of the knowledge domain in the design of MHL interventions. As highlighted in the preceding section, cultural responsiveness is equally essential. There is a growing need to conceptually broaden MHL beyond the narrow transmission of information about mental illness. Indeed, MHL is increasingly recognized as a multifactorial construct (Kutcher et al., Reference Kutcher, Bagnell and Wei2014). Although the relationship between mental health knowledge and stigma has been well documented (Evans-Lacko et al., Reference Evans-Lacko, Little, Meltzer, Rose, Rhydderch, Henderson and Thornicroft2010; Griffiths et al., Reference Griffiths, Christensen and Jorm2008; Hadlaczky et al., Reference Hadlaczky, Hökby, Mkrtchian, Carli and Wasserman2014), with lack of knowledge considered a contributor to negative attitudes and discrimination (Thornicroft, Reference Thornicroft2006), simply equipping individuals with information about mental illnesses does not necessarily result in stigma reduction or increased help-seeking intentions (Howard et al., Reference Howard, Griffiths, McKetin and Ma2018). Therefore, effective MHL interventions must move beyond knowledge transmission and adopt a more holistic approach.
One key limitation of the current MHL framework is its primary focus on identifying and understanding psychiatric conditions, with limited attention to mental well-being as a whole (Kutcher et al., Reference Kutcher, Wei and Coniglio2016). However, the absence of mental illness does not equate to the presence of mental well-being. Kutcher et al. (Reference Kutcher, Wei and Coniglio2016) redefined MHL to include “understanding of how to obtain and maintain good mental health,” highlighting that positive mental health is a crucial dimension alongside the recognition of mental disorders. Cultivating positive mental health can yield lasting benefits, fostering resilience and holistic well-being (Bjørnsen et al., Reference Bjørnsen, Espnes, Eilertsen, Ringdal and Moksnes2017; Bjørnsen et al., Reference Bjørnsen, Ringdal, Espnes, Eilertsen and Moksnes2018; Teixeira et al., Reference Teixeira, Coelho, Sequeira, Lluch i Canut and Ferre- Grau2019).
Among these interventions, positive mental health elements were incorporated through knowledge-based and/or skill-based approaches. For example, The Curriculum Guide included a module emphasizing positive mental health to build adolescents’ self-help competencies through classroom learning (Mcluckie et al., Reference Mcluckie, Kutcher, Wei and Weaver2014; Milin et al., Reference Milin, Kutcher, Lewis, Walker, Wei, Ferrill and Armstrong2016). Other interventions aimed to equip participants with coping and stress management strategies, skills for building healthy relationships (O’Kearney et al., Reference O’Kearney, Gibson, Christensen and Griffiths2006; Raghavan et al., Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024; Wei et al., Reference Wei, Kutcher, Austen, Comfort, Gilham, MacDougall, McKenna, McKinnon, Thompson, Yeo, Zhang, Baxter and Matheson2022; Wei et al., Reference Wei, Gilham and Kutcher2024) and techniques for managing thoughts and emotions (Lai et al., Reference Lai, Lien, Chen and Lin2022; Tay, Reference Tay2022). Despite the inclusion of such content, only one study specifically evaluated positive mental health outcomes (Lai et al., Reference Lai, Lien, Chen and Lin2022). This points to a critical gap in the field and underscores the need for future research to systematically measure this dimension to understand the impact of interventions better.
On the basis of this synthesis, four interrelated domains emerge as essential for guiding the next generation of youth MHL interventions. First, culturally individualized frameworks must replace one-size-fits-all models: interventions should draw on local perspectives and indigenous knowledge systems so that definitions of wellness, distress and recovery resonate with community values and lived experience (Kutcher et al., Reference Kutcher, Wei and Coniglio2016). Second, programmes should expand their scope from illness identification to the active promotion of positive mental well-being; embedding strategies that build resilience, optimism and life-skills aligns with the Positive Mental Health Literacy (PMeHL) framework and supports holistic flourishing (Bjørnsen et al., Reference Bjørnsen, Espnes, Eilertsen, Ringdal and Moksnes2017; Carvalho et al., Reference Carvalho, Sequeira, Querido, Tomás, Morgado, Valentim, Moutinho, Gomes and Laranjeira2022). Third, content must move beyond basic symptom recognition to foster a deeper understanding of underlying risk factors, causal mechanisms and culturally specific expressions of distress, thereby acknowledging the complex interplay of social, environmental and cultural determinants. Finally, sustained efforts to reduce stigma and to cultivate help-seeking behaviours remain indispensable; interventions that explicitly address culturally embedded barriers and leverage trusted community networks will be most effective at creating inclusive, supportive environments for young people.
One of the studies included in this review by Raghavan et al. (Reference Raghavan, Chandrasekaran, Paul, Pattabiraman, Mohan, Durairaj, Currie, Lilford, Furtato, Madan, Birchwood, Meyer, Sood, Chadda, Mohon, Shah, John, Padmavati and Iyer2024) exemplified this comprehensive and integrative approach. Their intervention addressed general mental health knowledge, recognition of mental disorders and promotion of positive mental health. Importantly, it also facilitated open discussions on personal experiences and culturally embedded attitudes towards mental health. This enhanced both the flexibility and contextual relevance of the intervention. Their multifaceted design ensured that mental health promotion strategies were not only evidence-based but also culturally congruent. Therefore, adapting and extending beyond the current MHL framework offers a promising and conceptually coherent pathway forward that warrants systematic empirical evaluation.
Drawing on the findings of this review, it is timely to critically re-examine whether existing definitions of MHL sufficiently capture the lived realities of young people across diverse cultural contexts. Such an expansion may address identified limitations in current youth MHL interventions and warrants systematic empirical evaluation, particularly with respect to positive mental health, attitudinal change and long-term outcomes.
Methodological quality and risk of bias implications
Building on the effectiveness patterns described above, interpretation of these findings must be situated within the methodological quality of the evidence base. A critical finding of this review concerns the overall methodological quality of the included studies. Only two studies (8.3%) demonstrated low risk of bias, while half of the studies (50%) were rated as high risk, with the remainder (41.7%) having unclear risk assessments. This distribution highlights opportunities for strengthening the evidence base for youth MHL interventions. Notably, these methodological challenges are not unique to MHL research but reflect broader systemic issues in intervention research, where achieving high methodological standards remains challenging due to practical, ethical and resource constraints (Jilcha, Reference Jilcha2025; Reid et al., Reference Reid, Walker, Usher, Jackson, Shepherd and Marriott2024; Sanjari et al., Reference Sanjari, Bahramnezhad, Fomani, Shoghi and Cheraghi2014).
The methodological limitations primarily stemmed from inadequate randomization procedures, lack of allocation concealment, absence of blinding protocols and incomplete outcome data reporting. Many quasi-experimental studies lacked appropriate control groups, while several randomized trials failed to adequately describe their randomization methods or implement proper blinding procedures. These methodological considerations introduce potential for selection bias, performance bias and detection bias (Higgins et al., Reference Higgins, Green and Van Den2020), which may influence effect sizes and should be considered when interpreting reported outcomes.
The variation in methodological quality has important implications for interpreting this review’s findings. The effectiveness of interventions should be interpreted cautiously, recognizing that methodological factors may influence reported outcomes (Higgins et al., Reference Higgins, Green and Van Den2020). The heterogeneity in methodological approaches makes it challenging to draw definitive conclusions about which intervention components are most effective. These quality considerations are particularly relevant given the growing implementation of MHL interventions in educational and community settings (e.g., Amado-Rodríguez et al., Reference Amado-Rodríguez, Casañas, Mas-Expósito, Castellví, Roldan-Merino, Casas, Lalucat-Jo and Martín2022; Wei et al., Reference Wei, Hayden, Kutcher, Zygmunt and McGrath2013). While the current evidence base shows promise and provides valuable insights into intervention approaches, continued methodological strengthening holds potential to enhance the robustness of future recommendations. These methodological considerations, alongside subsequent study-specific limitations, should be kept in mind when interpreting this review’s findings.
Limitations and future directions
Five key limitations must be acknowledged in interpreting this review’s findings. First, focusing on Jorm’s (Reference Jorm2000) three-domain framework excluded interventions targeting prevention strategies or first-aid skills from the expanded framework, potentially underestimating the breadth of existing MHL approaches and their comprehensive benefits for youth. Second, restrictions on age range (15–24 years), exclusion of comorbid conditions, English-language publications and lack of grey literature search may have omitted culturally diverse research, particularly from non-Western contexts where mental health concepts differ significantly, thereby constraining global applicability. Third, substantial heterogeneity across study designs, intervention durations and outcome measures precluded meta-analytical synthesis and definitive effectiveness conclusions, making it difficult to identify optimal intervention components. Fourth, post hoc assessment of cultural adaptation using non-predetermined criteria may have led to inconsistent identification and underestimated true cultural responsiveness. Finally, inconsistent operationalization of MHL domains, with recognition frequently subsumed under knowledge, limited understanding of domain-specific contributions and effects.
Future research should prioritize the following recommended areas to advance the field. Conceptual development should focus on creating developmentally appropriate adaptations of the five-domain framework (Jorm, Reference Jorm2012) through staged approaches. Methodological standardization requires adopting validated outcome measures across all MHL domains, particularly for recognition and positive mental health components, to enable robust comparisons and meta-analysis. Cultural responsiveness should be enhanced through systematic development of culturally adapted interventions using participatory approaches with local stakeholders, while establishing explicit criteria for assessing cultural adaptation in future reviews. Global representation can be improved by including non-English databases, grey literature sources and diverse populations, including the consideration of broader age ranges beyond 15–24 years to capture the full spectrum of youth MHL interventions, with examination of age-specific patterns and developmental context influences. Longitudinal evaluation should incorporate long-term follow-ups to examine sustainability. Through these targeted improvements, future research can build a more inclusive, methodologically rigorous and culturally responsive evidence base serving diverse youth populations globally. Specifically, educators require evidence-based guidance on integrating culturally adapted MHL curricula within diverse educational contexts, while policymakers need robust effectiveness data to inform funding decisions and implementation strategies that address digital equity concerns across different economic settings. These stakeholder-specific recommendations are essential for translating research findings into sustainable, equitable practice.
Conclusion
This systematic review of 24 studies encompassing 13,624 youth participants indicates that current MHL interventions for young people aged 15–24 are predominantly concentrated in high-income Western settings, are methodologically variable and are primarily focused on illness identification rather than holistic mental wellness. While interventions demonstrated global reach across Asia, Africa, Europe, North America and Oceania, significant gaps persist in the reporting and implementation of cultural adaptation, the integration of positive mental health components and overall methodological rigour. The dominance of knowledge-focused approaches, with all 24 interventions targeting this domain, coupled with limited attention to cultural adaptation (only 5 interventions, 20.8%) and positive mental health promotion (8 interventions, 33.3%), suggests that current MHL frameworks may not fully address the diverse needs and contexts of global youth populations. The concentration of digital interventions in high-income countries further highlights equity concerns with implications for access and scalability. Interpretation of intervention effectiveness is constrained by methodological limitations, with only 8.3% of studies demonstrating low risk of bias and half rated as high risk, underscoring the need for more rigorous evaluation. Moving forward, the field would benefit from culturally responsive, holistic approaches that extend beyond symptom recognition to actively promote mental wellness and resilience. Future interventions should adopt flexible, multi-modal delivery formats that address digital inequities while incorporating local perspectives, indigenous knowledge systems and community-driven adaptations. This review provides a foundation for strengthening the conceptual scope, methodological quality and contextual relevance of youth MHL interventions to support more equitable and effective mental health promotion globally.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10174.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10174.
Data availability statement
The data supporting the findings of this study are available within the paper and its Supplementary Material files.
Author contribution
The authors confirm contribution to the paper as follows: study conception and design: Ming Hao Lee and Moon-Ho Ringo Ho; data collection: Ming Hao Lee; data screening and analysis: Ming Hao Lee, Xin Yi Lee, Kah Hui Yap, Kellie Lum and Yan Hin Swen Goh; interpretation of results: Ming Hao Lee; draft manuscript preparation: Ming Hao Lee; all authors reviewed the results and approved the final version of the manuscript.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.



 Open access
Open access