

Introduction and Context
Gender in Society
With its currently 83.1 million citizens, Germany is the most populous country in the European Union. The traditional role model with women being the main providers of unpaid care work continues to exist in German society – with predictable negative consequences. Concerning their lifetime income, women earn only half as much as men. (Reference Boll, Jahn, Lagemann and Puckelwald1) In 2020, reactions to severe traumatic stresses and adjustment disorders were identified almost three times more often in women than in men – experts say mainly due to the double coping burden women carry. (2)
Concerning sexual harassment, several events in the last decade led to a wider public discussion about the topic. In 2013, the journalist Laura Himmelreich reported being sexually harassment by a politician. In the aftermath, thousands of women publicly shared their own experiences with sexual harassment under the hashtag #aufschrei, Geman for outcry. The debate that followed led to the first broad social debate about sexual harassment in Germany. (Reference Eddy and Cottrell3)
On New Year’s Eve 2015, hundreds of women were sexually harassed, some even raped, near the main train station in Cologne. More than 500 cases of sexual violence were officially reported, whereas only three of the perpetrators were convicted. (Reference Bosen4) The ensuing debate, again, brought focus to the topic and generated momentum for changes of the relevant laws. In fact, the events resulted in a reform of the law covering sexual offences, which now deems sexual harassment a criminal offence that can be pursued and punished under the law. (5)
Data on sexual harassment of women in Germany is scarce, but the existing data suggests that they are highly affected. Most of the available studies cover harassment in the workplace and report incidences as high as 70–80% depending on the type of harassment. One representative survey of the general population reported that 58.2% of German women had been affected by sexual harassment. (Reference Müller, Schröttle and Lebenssituation6)
Gender in Medicine
Approximately 63% of the nearly 98,700 medical students in Germany are women, with no significant drop until residency. (Reference Berufstätige Ärzte7) However, women are far less likely to hold higher ranked and leadership positions. In 2016, only 31% of senior physicians at thirty-four German university hospitals were women. (8) The situation becomes even worse for senior leadership positions such as university chairs, clinic directors or department heads: in 2019, women only held 13% of the leadership positions of the aforementioned hospitals. (9) Additionally, the German clinical workforce is less diverse than in other Western countries, with approximately 15% of the practising physicians holding a non-German passport, as recently reported by the German National Medical Board. (10)
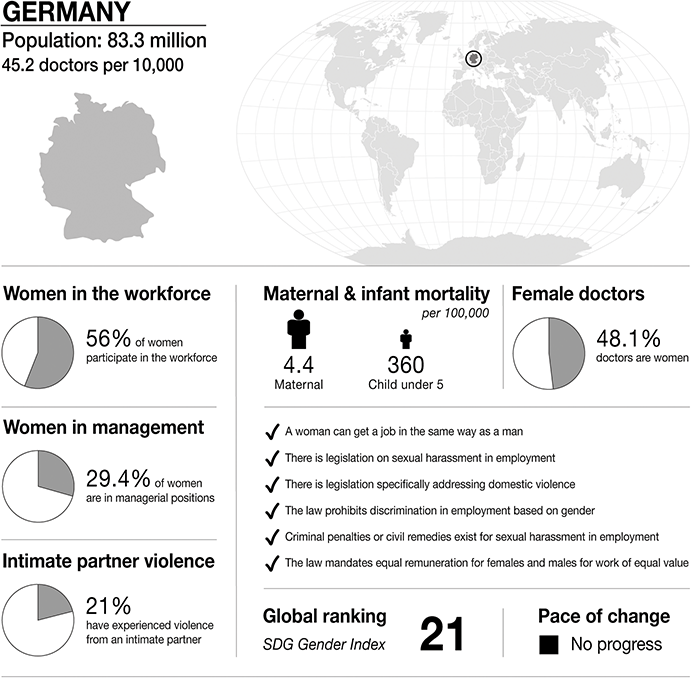
Infographic Germany. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.
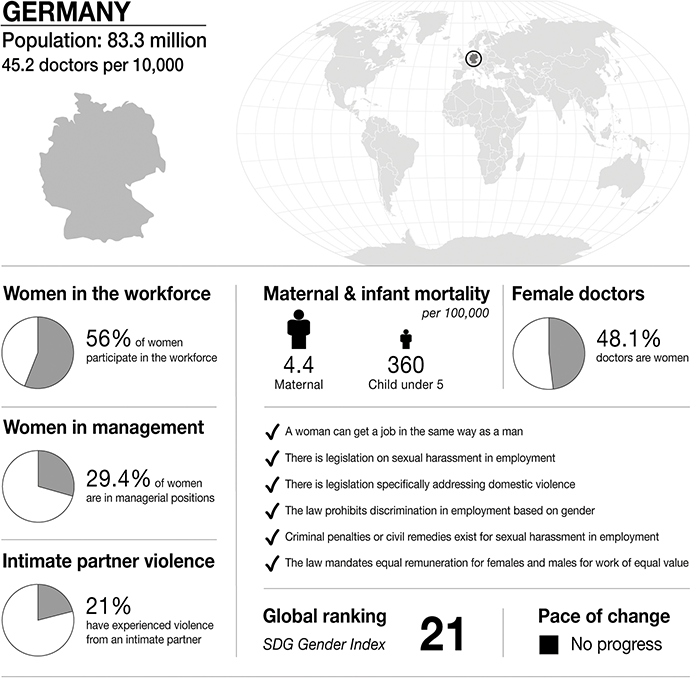
Figure 21.1 Long description
The infographic provides information about Germany, with a population of 83.3 million and 45.2 doctors per 10,000 people. It highlights several gender-related statistics. 56 per cent of women participate in the workforce. 29.4 per cent of women are in managerial positions. 21 per cent of women have experienced intimate partner violence. Maternal mortality is 4.4 per 100,000. Infant mortality under 5 is 360 per 100,000. 48.1 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Germany:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law mandates equal remuneration for females and males for work of equal value.
S D G Gender Index global ranking is 21, and is stable.
However, these facts are not always met with reflection about systemic barriers that women might face in medicine; rather, the high numbers of undergraduates are used by some critics to try to limit access for women into the medical profession. (Reference Freyschmidt11; Reference Dordowsky12). For years, there has been an ongoing debate in the community about the percentage of women entering medicine, some deeming it ‘too high’. The impending shortage of senior physicians and the need for more and better part-time models are paternalistically called ‘gender-based’ problems – according to the critics women would take up the majority of training positions only to afterwards drop out to have children and work part-time to be able to look after them. (Reference Freyschmidt11; Reference Dordowsky12)
Sexual harassment in the workplace is an important factor in the systematic discrimination that women doctors are facing in the medical profession. First, women are consistently more affected than men. (Reference Sojo, Wood and Genat13–Reference Mclaughlin, Blackstone and Uggen17) In Germany, only one representative study exists thus far, but it shows a very high prevalence among female physicians working in a large university hospital: 76.1% had experienced at least one form of sexual harassment at work. (Reference Djermester18) Second, sexual harassment has far-reaching negative consequences on health and work capacity of the affected person. (Reference Lindquist and McKay15; Reference Parker and Griffin19–Reference Victor, Wichman and Malakkla23). In the aforementioned study, 77.1% of the sexually harassed women doctors experienced negative consequences like emotional turmoil, negative health impacts or work deterioration due to the harassment. (Reference Djermester18) Third, sexual harassment as a display of power can help maintaining existing power structures (Reference Johnson, Widnall and Benya24–Reference Menon26) and strengthen the ‘glass ceiling’, which prevents women from access to leadership positions in a male-dominated environment. In fact, if a woman physician’s work performance decreases due to repeated sexual harassment at work, this could make her seem less qualified for a leadership position and therefore add to re-establishing antiquated gender stereotypes. (Reference Bursten27; Reference Fitzgerald, Shullman, Bailey, Richards, Swecker and Gold28). The German medical system is still very hierarchical and slow in its accommodation of flexible work structures and non-linear careers, which is also reflected in its struggles to integrate diverse career models due to personal choice or structural barriers. Gender-related harassment displays intersectional dimensions in Germany as well; however, these are poorly researched in the biomedical field. A recent survey of students and lecturers enquiring about discriminatory experiences beyond sexual harassment highlighted multiple sources of discrimination, with sex/gender still being the dominant one. (Reference Ludwig, Jenner, Berger, Tappert, Kurmeyer, Oertelt-Prigione and Petzold29)
Medical Education
Studying medicine in Germany involves at least five years of university education. Before taking the final exam, students have to work for one year in a hospital, taking one trimester in surgery, one in internal medicine and one in another specialty of their choice. After successfully passing the final exam, young doctors start their training as residents to become a specialist. It takes at least five years of training to become a specialist, in most cases up to eight years full-time. The medical specialist training in Germany is structured according to the general education guideline created by the German Medical Association. In accordance with this national guideline, the federal states define their own specialist training guidelines, which residents have to fulfill in order to become a specialist in the specific region/state. The guidelines include a detailed description of the skills, knowledge and number of operations/procedures a candidate has to participate in or lead, in order to become a specialist. Senior doctors are responsible for the supervision, creating a situation of dependence for the residents.
Law
In Germany, sexual harassment in the workplace is forbidden by law, according to the General Equal Treatment Act (AGG – Allgemeines Gleichbehandlungsgesetz). Regarding sexual harassment, the AGG states that employers are responsible for taking appropriate measures to protect their employees. If the employer does not fulfill their duty to do so, employees have the right to refuse to continue working. The law, moreover, states that employees who speak up against sexual harassment at work and file an official complaint must be protected from any disadvantages because of it. Additionally, sexual harassment can also be a criminal offence. According to §184i of the Criminal Code, perpetrators of sexual harassment can be imprisoned for up to five years, the same punishment which can be enacted for sexual assault or rape (§177 Strafgesetzbuch [StGB]). (5)
Medical Regulation – What Happens to Doctors Guilty of Misconduct?
In Germany, all doctors are obliged to register at the German Medical Association. In case of a severe form of professional misconduct, doctors can lose their license to practice as a doctor. According to public court rulings, there is one documented case in which a doctor lost his medical licence because of sexual harassment at the workplace, since he harassed several female trainees. (Reference Köln30)
The medical board of the region of Nordrhine-Westphalia (Ärztekammer Nordrhein) was the first and only of the German federal medical chambers so far to establish a central contact service, consisting of three women lawyers, to which all doctors of their federal state can turn to for help concerning sexual harassment in the workplace. Systematic promotion of bystander intervention is only about to begin in the German medical environment. So far, there is no real tradition of colleagues helping each other. To the contrary, an advisor working in the equal opportunities consultation office of Charité-Universitätsmedizin Berlin explains that a lot of her daily work revolves around the lack of solidarity between team members and everyone’s fear of harming their own careers by supporting survivors of sexual harassment. One project aims to address these unhealthy cultures by fostering effective bystander interventions addressing sexual harassment in academic medicine among students of the same institution.
Case Study
Prelude
Sabrina had already worked two years as a resident in the field of plastic surgery when she took a new job at a large academic hospital.
She describes the team atmosphere as friendly, although she recalls the relation between the colleagues as quite detached. The only exception was Dr T – he was her supervisor, only a few years older than her, and she quickly felt comfortable around him due to his friendly manners and informal interaction. Being the main supervisor for the residents, he oversaw their training and assigned who would do which operation.
After a while Sabrina noticed that he seemed to favour her over her colleagues when it came to interesting cases and rare interventions that every one of the residents was keen on getting their hands on to complete their training catalogue. He also missed no opportunity to stress that he could help her to complete her training in a shorter time and to promote her research ambitions. As he offered her a position on his research team, she was over the moon.
In retrospect, she identifies his grooming behaviour as one of the main reasons why it was so hard for her to recognize and fend off the harassment that followed.
He invested in gaining my trust, showing highly supportive behaviour. For quite a long time, I thought he was just being nice, and was grateful that he supported me, for the demands of the training and the research projects were challenging.
Another reason which made it hard for her to correctly identify his behaviour was that it shifted only gradually. Slowly, he started to search for more physical contact with her, sitting or standing very close to her and sometimes casually laying his hand on her shoulder or her thigh while they were going over some patients’ records.
I felt uncomfortable in those situations but didn’t know what to do. The first time he touched me like this, I was just taken by surprise and thought it might have been a mistake. When it happened again, I asked myself if maybe I was overreacting, that it might just be another amicable gesture of his. My uncertainty about the legitimacy of my feelings grew as I also observed him touch some of my fellow female residents and that they seemingly weren’t bothered. So, I thought, come on, don’t make a fuss about it, just suck it up and focus on your work.
However, his behaviour got more and more intrusive. He started making ambiguous comments, suggesting to ‘do some research together, just the two of us, without the others’. Although she felt more and more uncomfortable around him, she still couldn’t tell him to stop. Asked about the reasons for her reluctance, she stated that she still feared to offend him, damaging their – as she thought – amicable relationship. Moreover, he held a position of power over her, as he was the one assigning the tasks and operations and who got recognised on scientific papers.
The fact that I was still in training made me and my fellow residents structurally vulnerable to his harassment – I depended on his benevolence and his support to get along with my training and my scientific career.
Sabrina tried to avoid him at work, spending a lot of time and energy thinking about how best to keep away from him. This constant pondering took a lot of her mental capacity, and she recalls problems concentrating on her actual work. She thought about telling a colleague about her situation but didn’t dare because she feared the consequences of the harassment becoming public.
During my first weeks I overheard some of my colleagues talk about a female doctor who had filed a complaint about one of the doctors because of sexual harassment. Shortly afterwards, she had left the hospital. My colleagues mainly concentrated on what she in their opinion had done wrong and said things like ‘Why does she have to create such a drama’, ‘Our team atmosphere is so good, he would never do something like that’.
Sabrina was worried that her colleagues would despise her for reporting Dr T, so she didn’t. Moreover, it reinforced the idea in her that she might be the one being overly sensitive.
His harassment didn’t stop, however, and the more she tried to keep her distance, the more he became intrusive. He started to pressure her to meet him after work for drinks, implying he would withdraw his support should she refuse. She declined, desperately searching for excuses.
Eventually one day as the two of them were performing a surgical intervention, he stepped behind her and pressed himself against her.
I was so shocked by this blatantly transgressive assault that I could not do anything but to pretend nothing had happened and to continue with the operation. Not one of the bystanders said anything. After what felt like ages, I fled the operation room and asked a colleague to replace me, stating that I wasn’t feeling well.
Limbo
Sabrina called in sick for the following days, feeling deeply humiliated and overwhelmed by the necessity to navigate the situation. She reproached herself for not speaking up, telling him to stop and unmasking the harassment, and she was shaken by the thought that eventually she was incapable of standing up for herself.
I also felt betrayed by my colleagues who didn’t do anything to help me in that situation. Moreover, it hurt to acknowledge that the recent assault had not been an isolated case, but that I had felt sexually harassed by Dr T for the last couple of months. However, at least the assault served one purpose: I finally saw him and his actions as what they were – abusive, outrageous, and deeply unprofessional. And I give myself credit for not going back to work, as the idea alone to get near Dr T was utterly revolting.
Now being able to label her experiences as sexual harassment eventually helped her to go to the Women’s and Equal Opportunity Commissioner and file a complaint against Dr T.
When I wanted to report they told me that they needed a full protocol and that it needed to be with my full name. As long as I refused to reveal my name openly, no disciplinary actions could be taken against Dr T. That was a heavy blow for me. I would have preferred to remain anonymous because I feared the consequences of openly accusing him.
Sabrina also learned that it would be best if some of her colleagues would be able to confirm the harassment and be willing to testify publicly.
Exposure
So, she finally spoke to some of her colleagues about the incidents. Unfortunately, she had to find out that none of them was willing to appear as a witness against Dr T.
One of my colleagues, who had been in the operation room when the final assault happened, openly admitted that although she had been aware of what Dr T was doing to me, she refused to back me up in the reporting process for she was anxious it would have a negative career impact. Another one of the female residents told me he had also often made sexist remarks about her and had touched her butt several times. Nevertheless, she also didn’t want to ‘make a big fuss about it, as it doesn’t bother me as much as it apparently bothers you’.
To experience this lack of solidarity hurt Sabrina deeply, and it was only of small consolation that she didn’t have to go back to work. He continued working in the same department and in the same position he held before. On Sabrina’s side, even colleagues she had considered friends shunned her from then on. The legal process only led to a warning letter to Dr T, issued by the hospital. More extensive measures against him could have only been taken had another witness confirmed her allegations.
Aftermath
Two years after the incidents, Sabrina is still struggling with its impacts on her life and career. She recalls still getting overwhelmed sometimes by the thought that he just carried on as if nothing had happened, whereas it left her with a shattered career, searching for a new job and a feeling of self-loathing. She experiences thinking that if she had had the courage to confront him earlier this might have never escalated.
I am seeing a psychotherapist which helps, and I am back at work, though unfortunately not in my original specialty, as it is a small field where people know each other. My new colleagues seem to be nice, and it helps me a lot to be part of a team again. However, I have noticed that I am quite reserved towards them, like I can’t rely on people’s friendliness anymore. What I hope will prevail though is the anger over what happened to me, and I hope I will be able to use it should someone try to molest me again.
Reflection
Overall, the German situation demonstrates the compounded impact of (a) limited attention to the topic of sexual harassment in training and organizational management, (b) a lack of representation of women and gender-diverse individuals in medical leadership, and (c) an absence of structural and systemic systems of accountability. Ideally, a change process should address all of these dimensions – from the (a) micro to the (b) meso and (c) macro levels of society. Single change agents will not be able to address all dimensions at the same time. Indeed, a concerted effort is essential in raising attention, building structures to support survivors and preventative structures to reduce incidence of sexual harassment in the future.
Some progress has been made in recent years in terms of data collection, public attention and establishment of exemplary implementation processes. The Federal Antidiscrimination Agency (Antidiskriminierungsstelle des Bundes – ADS) has commissioned a report about the incidence of sexual harassment and abuse in the professional field, hosted conferences on the topic and made it one of their primary focuses. In addition to data collection and outreach, they also provide independent consultation services for parties that cannot obtain support within their work environment or do not want to address potential experiences and events through internal channels. The report, published in 2022, has demonstrated that the health field is one of the most significantly affected domains, especially for hierarchically disadvantaged workers, such as junior nurses or health workers experiencing intersectional discrimination. (Reference Schröttle, Meshkova and Lehmann31)
The media has started to cover the topic more extensively in recent years. Instances of prominent cases of sexual harassment up to entire structures of deceit and cover-up have been exposed in different industries. The music and film industry had to reckon with a number of very public cases, as well as the publishing and media industry. Academia and extra-academic research organizations have been the centre of prominent and oftentimes structurally embedded cases as well. Of course, media coverage is partially driven by the topics that will gain most attention, but nevertheless, the sheer number of reports and affected industries clearly shows the systemic pattern. The growing attention to the topic and its systemic dimensions is, however, often also faced with growing backlash and recurrent patterns of singling out ‘bad actors’ until their eventual redemption in other positions or branches of the industry. The very structures that should prevent harassment and should protect survivors are oftentimes led by powerful actors with ties to the perpetrators – which might explain the limited consequences seen to date.
Structural change is somewhat easier to implement in organizations at the meso level, rather than broadly at the macro level. Starting in 2018 the Max Delbrück Center in Berlin, a large research organization, has implemented a broad and participatory process to design a campaign to reach all employees and raise awareness for the topic and develop internal guidelines for the prevention of harassment and structural interventions in case of incidents. (32) After an internal case of harassment, the organisation decided to tackle their insufficient intervention polices and wanted to implement a participatory process to increase representation and ownership of the process by the employees. In an initial open call, all employees interested in participating in the future task force were asked to contact human resources, which led to more than fifty individuals signing up (in an organisation with about 1,200 personnel). Among those who signed up were the official representatives of the teaching assistants, PhD students and postdoctoral groups that were already organised in a representative structure (representing about 500 employees). Furthermore, administrative staff, as well as principal investigators and professors, joined the initiative. A moderated co-creative process over eight months led to the concerted development of the envisioned deliverables through participation of all employee groups within the organisation, either through direct participation or through representation of their professional group. The process was extremely successful in delivering a new concerted guideline for the prevention of sexual harassment, clear internal procedures for the management of harassment cases, and a broad information campaign to sensitise all employees. An additional achievement of the participatory process was the feeling of ownership that the participants experienced during and after the process, especially groups that are usually less involved in decision-making processes.
At the macro level, to achieve structural and systemic levels of accountability, larger societal practices would have to be addressed. This would mean interventions to support accountability among all members of society leading to the kind of collective responsibility that would reduce primary occurrence and engender bystander interventions. While the legal framework has been expanded with §184i of the Criminal Code in 2016, allowing for the imprisonment of perpetrators of sexual harassment for up to five years, this paragraph has rarely been invoked to date and there have not been any exemplary cases. In addition to a legal framework, everyday interventions in school, universities and workplaces would have to be systematically devised. The reality is that it is very much up to teachers, lecturers and employers to incorporate the subject into their teaching or training activities.
Furthermore, the broad societal attention is also fostering some backlash in a context of shifting political priorities and preferences. Germany, as many other European countries, is experiencing a paternalist and right-wing backlash as a consequence of the progress made over the last decades. ‘Traditional’ values, which translate primarily into curtailing women’s rights, are erected as a beacon of right wing and nationalist parties, and criticism of feminist topics is one major unifying issue. The promotion of equal rights and, hence, the prevention of harassment – sexual or otherwise – is seen as a ‘woke’ attitude and openly ostracized by these political actors. Overall, the enactment of structural interventions to encourage equity and prevent harassment will most likely be left up to individuals and single organizations, and vocal advocates, rather than becoming a concerted political strategy for change.
In conclusion, harassment prevention in Germany is a moving field, with some progress made, but with a substantial need for upscaling of interventions to broadly address the topic at a societal level.

 Open access
Open access