

1. Introduction
Digital health services can improve access, quality, and efficiency within healthcare systems (FDA, 2020). In this article, we view them as cocreated value exchanges (Reference KimbellKimbell, 2011; Reference Sampson and FroehleSampson & Froehle, 2006) in the healthcare domain enabled by digital technologies. An example includes remote patient monitoring, where patients measure and share health data (such as blood pressure or glucose levels) from their homes. Another example is video consultations, which enable patients and healthcare professionals to meet without being in the same physical location. Although there is promise in adopting such services, their implementation faces many barriers. For example, they can be incompatible with existing technological infrastructures, clinical workflows, and regulatory constraints (Reference Greenhalgh, Wherton, Papoutsi, Lynch, Hughes, A’Court, Hinder, Fahy, Procter and ShawGreenhalgh et al., 2017; Reference Ross, Stevenson, Lau and MurrayRoss et al., 2016). Additionally, they often need to become part of a complex healthcare system which are unpredictable, where small adaptations can have unforeseeable consequences (Reference Plsek and GreenhalghPlsek & Greenhalgh, 2001). A well-managed process is therefore essential for successful implementation.
To strengthen the understanding of how the design field can contribute to the implementation of digital health services, we seek to clarify the concept of implementation from a design perspective. Informed by Reference Greenhalgh, Robert, Macfarlane, Bate and KyriakidouGreenhalgh et al. (2004) and Reference May, Finch, Mair, Ballini, Dowrick, Eccles, Gask, MacFarlane, Murray, Rapley, Rogers, Treweek, Wallace, Anderson, Burns and HeavenMay et al. (2007), we start our investigation by viewing implementation as a phase within an effort to change a system, where a service (already conceptually developed) is introduced or modified within a given context. In the case of this paper, the context is the healthcare system to which the services must become part of.
Some design researchers have previously explored how design can be used to support implementation across different contexts. In service design, Reference Overkamp and HolmlidOverkamp and Holmlid (2017) have argued that implementation needs to be considered throughout the development process, and Reference Almqvist, Pfannstiel and RascheAlmqvist, (2018) highlights the role of structured handovers from those who created the service to those who will implement it. Additionally, Reference YuYu (2021) investigated barriers to realising services in a business context, and identified design-relevant approaches to address them, such as envisioning potential customer experiences and understanding their needs. In the context of complex sociotechnical systems, Reference Norman and StappersNorman and Stappers (2015) argue for the importance of continued designer involvement during implementation, as they note that this is where core difficulties typically arise. In healthcare, specifically, design contributions have been explored by Reference Bodell, Pannunzio, Houwen, Lamé, Snelders and KleinsmannBodell et al. (2025), who identified design knowledge domains that can support digital health implementation, including codesign, prototyping, and human-centeredness. Additionally, Reference Li, Grisot, Suoheimo, Jones, Lee and SevaldsonLi and Grisot (2025) explored how service ecosystem design can support the implementation of remote care, and Reference Lin, Hughes, Katica, Dining-Zuber and PlsekLin et al. (2011) have shown that combining design and change management can aid implementation in hospital settings.
Despite this prior research, a lack of consensus persists regarding the meaning of digital health service implementation from a design perspective, as well as the conceptual relation between digital health service design and implementation. Such a lack of consensus affects the work of designers, who may have different ideas about the specific goals they are addressing when contributing to digital health implementation, and hinders a shared understanding of the role of design in digital health implementation from a research perspective. To address this, we aim to make a step towards clarifying these concepts and their relation. This will be explored from the perspectives of design professionals, as they are directly involved in the processes through which new services become part of existing systems. In this paper, we will therefore answer the following two research questions: what are design professionals’ perspectives on (1) when a digital health service can be considered implemented, and (2) how design relates to implementation in complex systems? By answering these questions, we aim to establish clearer goals and roles for design during this phase.
2. Method
To explore the relation between design efforts and implementation, we conducted 24 semi-structured interviews with design professionals. Before conducting the study, we obtained ethical approval from the Human Research Ethics Committee at the university of the first author.
All authors are based in a design faculty. The first and fourth authors have prior industry experience in implementing digital health services. These backgrounds provided shared experiences with interviewees and familiarity with the context, which supported data collection and analysis (e.g., in how follow-up questions were asked and how codes were generated). This way, our design orientation and past industry experience have contributed to how we connected with and interpreted our data. The second and third authors have academic backgrounds with an understanding of professional design practice based on education and research on service design, collaborative design, and the role of design in organisations.
2.1. Sampling
The design professionals were selected using a purposeful sampling strategy, which involved selecting individuals who met specific criteria that helped answer the research question (Reference Cash, Isaksson, Maier and SummersCash et al., 2022; Reference PattonPatton, 1990). The criteria for the participants were:
-
• Has a Master’s degree in design, and as such can be considered a design professional.
-
• Has been a part of implementing at least one digital health service into a complex system involving patients and/or healthcare professionals.
-
• Is employed in a non-academic role, to ensure a focus on practice rather than research.
-
• Is working within the Dutch healthcare system, allowing for a more focused discussion since the interviewer is familiar with this context.
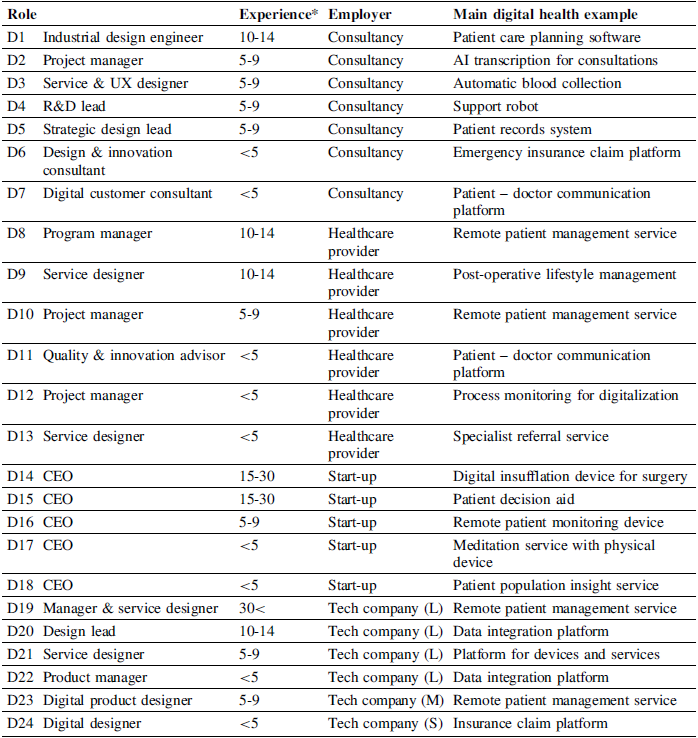
Within these criteria, we sought diversity in terms of employer, attended university, and years of experience. Participants were recruited through the authors’ networks (n=11), snowball sampling (n=9), and LinkedIn searches (n=5). One of these participants was excluded after the interview, as it was found that the participant did not work directly on implementation as defined within the context of this study. Table 1 gives an overview of the details of the interviewed participants. Invitations to the participants were sent via email, including a description of the interview topics. This description served two purposes: to verify that participants met the selection criteria and to help them prepare for the interview.
Participant details

Note: Large (L), Medium (M), Small (S) tech companies and Start-ups (viewed as micro company) are defined from the EU SME Definition based on number of employees (European Commission, n.d.).
* Experience is counted as years from graduation.
2.2. Data collection
In the interviews, we employed a semi-structured interview approach guided by a topic guide to facilitate a natural and dynamic dialogue (Reference Fielding, Thomas and GilbertFielding & Thomas, 2008), which also. allowed for spontaneous questioning based on the relevance of emerging topics (Reference PattonPatton, 1990). We conducted the interviews between June 30, 2023, and January 19, 2024, with 10 conducted in person and 14 online. They were scheduled for 60 minutes, and the audio-recordings lasted between 45 and 75 minutes, averaging 55 minutes. Before the interviews, the participants provided informed written consent.
The interview guide comprised five parts, of which two (accounting for about five to ten minutes each in the 24 interviews) most directly addressed the research questions of this study. However, we also coded segments in the three other parts of the interviews whenever they were relevant to these same questions. In the two parts reported in this study, we asked the participants to openly reflect on (1) when they view a digital health service to be implemented, and (2) how they view the relation between design and implementation. As a follow-up to the second part, they were asked whether design and implementation are distinct or overlap, which later became the opening question for discussing the second part. The three other parts concerned the participants’ background and a key project, actions during implementation, and a self-assessment of their contribution to nine implementation strategy categories.
2.3. Data analysis
To analyse the transcripts, we employed reflexive thematic analysis, which treats themes as the outcomes of an inductive, iterative, and reflexive process (Reference Braun and ClarkeBraun & Clarke, 2021). We chose it because it aligns with the exploratory nature of our study and leverages the researchers’ subjective skills, treating their past experiences as a resource rather than a bias to be avoided. We adopted it with a constructionist epistemological view, seeing meaning as being socially produced (Reference Braun and ClarkeBraun & Clarke, 2006).
Following this method, we transcribed the data verbatim and read the transcripts to note initial ideas for potential codes and themes, guided by the two research questions. The first and fourth authors then independently coded one interview at a time (in ATLAS.ti, v23.2.1), comparing and discussing their approaches to reach a shared level of abstraction. This process continued for five rounds until agreement was reached. The first author then revised the initial five and coded the remaining 19 transcripts. Following the coding, the first author grouped the codes into potential themes based on patterns of shared meaning for each of the two topics. Finally, the first author presented the themes with illustrative extracts. All authors then iteratively reviewed and refined the themes for clarity and consistency.
3. Results
In this section, we first present the design professionals’ perspectives on when digital health services can be considered implemented (3.1) and then their perspectives on the relation between design and implementation in complex systems (3.2).
3.1. Perspectives on when digital health services are implemented
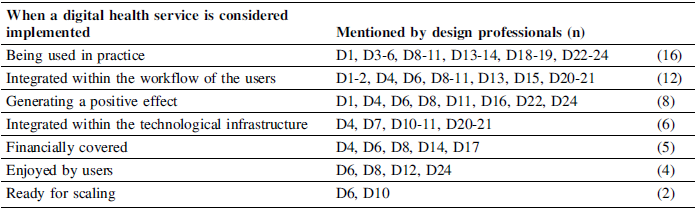
From the analysis of participants’ open answers, we identified seven themes, presented in Table 2. Following is a description of each theme, with quotes from the participants.
Perspectives on when a digital health service is considered implemented

3.1.1. Being used in practice
A common criterion expressed by participants was that it is being used in practice. One participant answered: “For me, it’s there, and it’s working in whatever form. It might be a very, very simplified form, but like something that works in the real world” (D5). The importance of long-term sustainability was also highlighted, as one participant noted: “I mean that takes time to kind of see if it gets routinized. If people continue to use it the way they’re supposed to use it. If it’s not going wrong. If they’re not going to push it aside and do it still the traditional way” (D11).
3.1.2. Integrated within the workflow of the users
Several participants emphasized that implementation requires the service to become integrated into users’ daily workflows, where its use is socially normalized to the point that it feels routine. One participant described: “When the staff use it to the point that they kind of forget that they’re using it, that it doesn’t feel like it’s this new weird thing. It’s just kind of a part of their daily reality to the point where they just forget that they used to do things differently” (D20). Another participant echoed this sentiment, saying: “I think it should be integrated in how people provide care” (D4).
3.1.3. Generating a positive effect
Participants also emphasized the importance of the service having a meaningful impact, for example, through more efficient workflows or improved health outcomes. As one participant put it: “And you made a difference. So you have achieved your impact. […] Sometimes you find out the impact is a bit different, but at least positive” (D8). Similarly, another participant said: “I think the most important crucial part in implementation is the long-term effect” (D4).
3.1.4. Integrated within the technological infrastructure
Making the service compatible with the existing technological infrastructure (software and hardware) was also considered important. One participant explained: “There needs to be a process where you kind of adapt things within the current system that is already there in place so we can implement the new service. For example, with the ICT, we had to make a new coupling connection so it could connect the current electronic patient dossier to the new service” (D11). Another participant also brought up the integration into the technological infrastructure, saying: “Where needed at all levels to make sure that this is kind of responsibly embedded within the IT infrastructure of that organisation” (D20).
3.1.5. Financially covered
Financial sustainability, such as reimbursement or cost-effectiveness, was seen as critical for considering a service implemented for some participants. One participant stated: “I would really define that as reimbursed, because if you want to make a business around it, it has to be reimbursed” (D17). D8 added to this notion of financial sustainability, stating: “How does that relate to the actual results in cost reduction or in amount of readmissions or admissions to the hospital. […] If you don’t do that [measure results], you can never say like I’ve successfully implemented it.”
3.1.6. Enjoyed by users
Some participants considered the digital health service implemented when users found value and enjoyment from using it. D11 stated: “So if people are content with it and are happy to use it, I think then it’s effectively implemented.” Another participant, similarly, noted the importance user satisfaction, saying: “You can also have like a set of factors like people are happy to use it.” (D24).
3.1.7. Ready for scaling
Two participants considered a service implemented when scaling started, one saying: “Then you test it in a smaller environment with the pilot, and then once it’s proven to be valuable and you start scaling it, I would say from the moment you start scaling it to other patients” (D6).
3.2. Perspectives on the relation between design and implementation
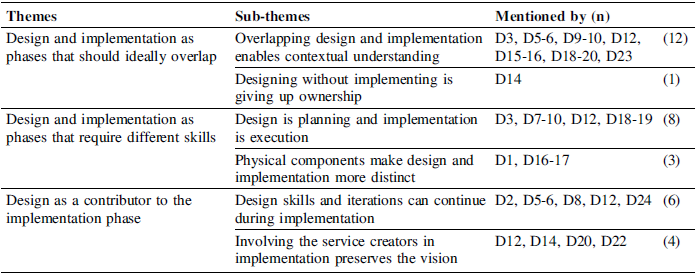
From the analysis, we elicited three themes and six sub-themes, as shown in Table 3. Below, we provide a brief description of each theme, accompanied by supporting quotes.
Perspectives on the relation between design and implementation

3.2.1. Design and implementation as phases that should ideally overlap
The first view shows that some participants see design and implementation as phases that should overlap. Below, the two sub-themes relating to this theme are presented.
Overlapping design and implementation enables contextual understanding. One participant noted that overlapping design and implementation uncovers valuable insights for good design, explaining: “With implementing, new insights for design arise, so you’ll always go back to finding new improvements […] it stays an iterative process” (D9). This iterative approach ensures that what is being designed is continuously refined based on real-world interactions. Another participant highlighted the importance of implementing early to understand how the service works in its context, explaining: “As quick as possible, you want implementation to see how it works and to improve.” (D3).
Designing without implementing is giving up ownership. D14 argued that to take ownership of a designed service, designers must stay engaged through both design and implementation, reaping the rewards only when the product is successfully realised, stating: “Being a designer as a consultant is a bit of an awkward situation because you’re painting a picture, but you’re not part of the area where it’s implemented. […] So that we are there when you’ve implemented and people are actually happily using the product and paying for it, that’s when you have implemented and, that’s where you get rewarded.”
3.2.2. Design and implementation as phases that require different competencies
A second, seemingly contradicting, view of how design relates to implementation shows how design and implementation differ in focus. Below, the two sub-themes relating to this theme are presented.
Design is planning and implementation is execution. Some argue that design comes before implementation, describing design as the initial phase focused on generating, testing, and refining ideas, while implementation involves putting those ideas into real-world practice. One participant explained: “It’s usually design and then implementation. Maybe there’s a small overlap, but I wouldn’t say they go parallel.” (D7). Another participant highlighted how design serves as the groundwork for implementation, stating: “Designing is really like the first phase of making your products. Then you would test it with users, but not yet really implement it […] When you really implement it, it’s used by a lot of care professionals and maybe also by patients” (D12). These views reflect a sequential nature where design explores solutions and implementation focuses on making them work, as also noted by D8: “Implementation is less creative and it’s more geared to make the design function properly”.
Physical components make design and implementation more distinct. As one participant explained regarding physical products in the healthcare field: “You need to certify your product before you can really move, and to certify, you need to have a fixed product” (D16), which limits the ability to make adaptations. Moreover, another participant noted that: “For some projects, there needs to be sort of a line because you need to start production and have a number of devices ready before you can really implement it” (D1). This shows that when services include physical components, the transition from design to implementation is perceived as more distinct, partly due to the certification process.
3.2.3. Design as a contributor to the implementation phase
The third identified perspective of how design relates to implementation shows that some regard design as a practice involving skills and ways of working that can contribute to the implementation phase. Below, the two sub-themes are elaborated upon.
Design skills and iterations can continue in implementation. The iterative nature of design enables continuous improvement and adaptation based on feedback and evolving needs, which can also continue during implementation. One participant explained: “For me, implementation is a phase in a project, and design happens throughout it in many shapes and forms […] At the beginning of a project, design tends to be more explorative, answering hypothetical questions and at the end it’s more evaluative” (D5). Another participant explained: “Implementation means you can iterate, and that’s a design skill. Adapt, of course, but that’s different from creating new solutions” (D8).
Involving the service creators in implementation preserves the vision. One design professional noted: “If you created the design, I would definitely like to be part of the implementation phase to make sure it’s implemented the way I envisioned it and to see how it actually works in real life” (D12). By staying engaged, designers can address discrepancies between the intended use and its practical application. Another participant warned against disconnecting designers from implementation, saying: “The people who were bringing it on weren’t the people who designed it, […] that was a really dangerous point for the project” (D20).
4. Discussion
Next, we discuss our results in relation to the two research questions, examining what design professionals consider the endpoint of implementation (4.1) and its relation to design (4.2). Following, we reflect on implications for design practice and research (4.3) and consider study limitations (4.4).
4.1. When a digital health service is implemented
We found that when design professionals consider a digital health service as implemented vary considerably. When comparing the identified criteria, we notice that Being used in practice is a pre-requirement for both indications of service sustainment and system impact. This criterion may also involve a temporal dimension, where continued use over time further indicates service sustainability. In these terms, this can be seen as an initial stepping stone towards implementation from a design perspective. All other proposed criteria but the last could then be placed within two categories of implementation goals:
-
• Integration between the service and system.
-
• Impact of the service on the system.
Within this categorisation, Financially covered, Enjoyed by users, Integrated within the workflow of the users, and within the technological infrastructure, fit within the first category, while Generating a positive effect fits within the second category. We note that the two categories should not be seen as independent of one another. For example, improved integration may lead to greater impact, and significant impact may motivate stakeholders to accept the service or work harder to integrate it. However, the goals in these categories are conceptually distinct, as the first focuses on making the service stick to the system, and the other on the effects (positive and negative) it has on the system. Defining satisfactory levels within these categories may help designers align implementation efforts in practice and provide researchers with a structure to study design contributions in this domain. Finally, the last criterion, Ready for scaling, appears to sit somewhat apart from the others. This is because scaling efforts can occur in parallel with implementation; as such, a service may be considered ready for scaling before it is even implemented in a system, making readiness for scaling a problematic criterion for implementation. However, when services are scaled after an initial implementation, readiness for scaling can be seen as a positive indicator of progress.
Most interviewed designers mention criteria situated relatively early in this process chain, with most participants considering a service to be implemented from the moment it is put to use, while others consider it implemented only once some degree of integration or impact is achieved. This might reflect a tendency for designers to be more familiar with (and attentive to) early implementation phases, possibly since these early implementation phases more often overlap with new service development, which designers are typically involved in. This focus on contributing in the early phases has also been observed in design research in healthcare more generally (Reference Huynh-Dagher, Lamé, Duong and JankovicHuynh-Dagher et al., 2022). We also note that the diversity of views likely reflects differences in professional profiles. For example, participants working in healthcare provider organisations tended to stress the long-term use and integration within clinical workflows. Start-up participants, on the other hand, emphasized the importance of the service being used and reimbursed. This may highlight the need to align the understanding of the concept across different contexts.
In these terms, we propose that designers in healthcare might use the above characterisation to articulate project-specific implementation goals, thereby creating a shared language among designers and other relevant stakeholders involved in the implementation. To increase the granularity of integration and impact as implementation goals, we suggest adopting existing frameworks. To discuss and evaluate implementation goals regarding integration, designers could consider using implementation outcomes, such as acceptability, feasibility, and adoption, which can be used to describe how well a service has been adopted and embedded within a system (Reference Proctor, Silmere, Raghavan, Hovmand, Aarons, Bunger, Griffey and HensleyProctor et al., 2011). For discussing implementation goals regarding impact, designers could use the Quadruple Aim framework, which considers improvements in population health, patient experience, cost-effectiveness, and the work-life of healthcare professionals (Reference Bodenheimer and SinskyBodenheimer & Sinsky, 2014). These frameworks offer one approach to adding granularity, and their widespread use in healthcare supports alignment with existing implementation literature and practice.
4.2. The relation between design and implementation
We identified three perspectives on how design professionals understand the relation between design and implementation in complex systems. The first two are: Design and implementation as phases that should ideally overlap, and Design and implementation as phases that require different skills. These two perspectives view design and implementation as two separate phases in changing a system. In contrast, we have a third perspective: Design as a contributor to the implementation phase. This perspective views design as a practice and implementation as a phase, positioning them on different dimensions.
We note that the differences in responses appear to be influenced by the materiality of the service. For example, design professionals with a physical component as part of their service (e.g., D3, D16, D17) emphasized the divide between developing the service and implementing it, due to regulatory constraints such as CE-marking. This suggests that the perceived boundary between the phases may be shaped by the service’s practical constraints. Additionally, we observe that some participants described their contributions to implementation as design contributions, while others did not, seeing what they do during implementation as something other than designing. Yet, we note that the interview responses also exemplify that health service implementation requires continued design work, as introducing services into complex systems, such as healthcare, entails iterative adaptations to both the service and its context. Not seeing such contributions as design may limit how we position design in the improvement of healthcare systems, making design only about what comes before realising change.
As such, we propose positioning design work as a contributor to implementation, rather than as a preceding or parallel phase. We refer to this positioning as design for implementation, to emphasise the role of design as a contributor within the implementation phase. Especially in complex systems, where the introduction of new services can have unforeseeable consequences (Reference Plsek and GreenhalghPlsek & Greenhalgh, 2001), we foresee that design approaches can be useful for identifying emerging issues and addressing them. This would also position design in accordance with existing views on implementation within healthcare, for example, by Reference Greenhalgh, Robert, Macfarlane, Bate and KyriakidouGreenhalgh et al. (2004) and Reference May, Finch, Mair, Ballini, Dowrick, Eccles, Gask, MacFarlane, Murray, Rapley, Rogers, Treweek, Wallace, Anderson, Burns and HeavenMay et al. (2007), developing as a discipline that can support implementation through contributions that complement existing approaches. For example, when implementing a video consultation service, design contributions can focus on realising the service within its system, such as defining the workflows for how and when to use it within routine care, and ensuring that the video-calling software functions with the hardware available in the local context.
4.3. Implications and future research
Echoing Reference Norman and StappersNorman and Stappers’ (2015) call for designer involvement during implementation in complex sociotechnical systems, D14 highlighted the importance of designers taking ownership of the application of their work and tackling the challenges inherent in realising the services they develop. To facilitate this goal, our exploration has focused on clarifying the concept of implementation from the perspective of design practitioners. Through our categorisation of implementation endpoints from a design perspective, we hope to help practitioners and researchers align their views to describe the scope and how design work can contribute to implementation processes. In doing so, we highlight the possibility and opportunity for design professionals to take additional ownership in realising change, rather than leaving implementation to others. This way, design professionals and researchers can be more intentional with their contributions to implementations, for example, in grant proposals, consultancy offerings, and internal project communication.
In the future, we call for further research on the role of design for implementation within complex systems such as healthcare. With this, we can push traditional (service) design research, such as that of Reference Overkamp and HolmlidOverkamp and Holmlid (2017) and Reference Almqvist, Pfannstiel and RascheAlmqvist (2018), to consider design as a direct contributor during the implementation phase, and not only as something being done before it. Some notable design contributions within healthcare systems have been made by Reference Lin, Hughes, Katica, Dining-Zuber and PlsekLin et al. (2011); Reference Li, Grisot, Suoheimo, Jones, Lee and SevaldsonLi and Grisot (2025), and Reference Bodell, Pannunzio, Houwen, Lamé, Snelders and KleinsmannBodell et al. (2025), each illustrating how design can contribute to realising change within complex systems in the healthcare domain. As of now, these studies remain relative exceptions within the field, which could greatly benefit from a stronger research agenda that treats implementation as a legitimate and necessary domain of design inquiry. Building such a discourse can help improve current practice and guide education as well, for instance, by showing design students how their skills can be applied to implementation. By integrating design more deliberately into implementation efforts, we can strengthen these processes and, in doing so, contribute to the continued improvement of healthcare systems.
4.4. Limitations
This study presents some limitations, particularly in its coverage of only one country, which may limit the international generalizability of our results. Additionally, in conducting the study, past experiences with and readings on design that position implementation as something happening after design may have affected our initial understanding of the relation between design and implementation. Without these past experiences, we may have been more open to viewing the relation differently.
5. Conclusions
This study reports on interviews with a diverse sample of 24 design professionals encompassing various roles, organisations, and amounts of experience who have implemented digital health services in complex systems. We explored their perspectives on when such services can be considered implemented and how design relates to implementation. In doing so, we found little consensus on either point, but rather a rich collection of perspectives.
Based on the results of the interviews, we proposed a categorisation of implementation goals from a design perspective, including two categories (integration and impact) and a prerequisite (being used in practice). These categories can be made operational through the application of existing frameworks. Using them in practice can help articulate satisfactory goals for implementations and in research to position academic contributions effectively. Additionally, we argue for positioning design contributions to implementation as design for implementation, emphasizing the potential of using practice and knowledge from design as a direct contributor to the implementation of services, rather than as something that happens in parallel or only before implementation. This positioning enables a consideration of the implementation phase, where digital health services are introduced or modified within a context, as a relevant area for further design inquiry. In turn, such inquiry can support improving design contributions toward implementation processes, leading to enhanced health outcomes, better experiences, and increased efficiency within healthcare systems.

 Open access
Open access