


Introduction
Mental health has become a global health priority, as mental disorders constitute a significant burden of disease worldwide. Natural disasters exacerbate this existing burden by disrupting individuals, families, and communities both psychosocially and economically, thereby increasing vulnerability to mental health problems.Reference Usami, Lomboy and Satake1 Children are particularly more vulnerable because their emotional, cognitive, behavioral, and sensory development is incomplete, and they lack effective coping mechanisms to manage traumatic experiences. They may also fear the recurrence of disasters and the loss of loved ones.Reference Usami, Lomboy and Satake1–Reference Udomratn3 Studies estimate that 5–43% of disaster-affected children develop posttraumatic stress disorder (PTSD), while many others experience depression, anxiety, or other mental disorders.Reference Dyregrov, Yule and Olff4
On February 6, 2023, 2 consecutive earthquakes with magnitudes of 7.7 and 7.6 struck Kahramanmaraş province 9 hours apart in Türkiye. These twin earthquakes caused tens of thousands of deaths, massive destruction, and the displacement of approximately 2.7 million people. These earthquakes constitute a collective trauma with nationwide repercussions.5 In low- and middle-income countries such as Türkiye, women and young children are disproportionately affected by natural disasters, making mother–child dyads a particularly vulnerable group in terms of post-disaster mental health.Reference Farooqui, Quadri and Suriya6, Reference Kvestad, Ranjitkar and Ulak7
The acute mental health problems experienced by children affected by disasters depend on factors such as age, family support, personality, and the type and duration of the disaster.Reference Olness8 Disasters may negatively affect the autonomy and environmental exploration skills of children aged 1–3 years, increasing separation anxiety; in children aged 4–5 years, they may lead to psychosocial and behavioral problems such as re-enactment of the catastrophe, nightmares, aggression, and generalized anxiety.Reference Usami, Lomboy and Satake1 Experiencing one or more natural disasters before the age of 5 increases the risk of any mental health and substance use disorders in adulthood by 15.7%.Reference Maclean, Popovici and French9 Therefore, the early childhood period requires careful attention. Although recent studies have explored the psychological impact of the 2023 Türkiye–Syria earthquakes on school-aged children and adolescents,Reference Atabey, Karagöz Çetiner and Kaya Çimen10, Reference Polatgil and Yıldız11 no research has specifically focused on the mental health status of play-age children following the earthquakes.
Children’s outcomes after earthquakes are influenced not only by direct exposure but also by parental mental health and family dynamics. Maternal psychological well-being and the quality of the mother–child relationship play a central role in shaping children’s recovery and resilience.Reference Güler Aksu and İmrek12 Early diagnosis and intervention of mental symptoms in children are critical to supporting recovery and promoting long-term well-being. The existing literature emphasizes the need for holistic and family-centered mental health approaches in post-earthquake settings.Reference Demirci13
The disaster literature has rarely examined reciprocal effects of maternal and child mental symptoms. This literature reports that after controlling for predisaster symptoms, longitudinal actor-partner interdependence models indicate that mother’s and children’s mental symptoms are linked, and change in tandem and influence each other after a disaster.Reference Hausman and Black14, Reference Tunç, Çelik and Kaçmaz15 Previous findings demonstrate bidirectional cross-generational influences of mother and child on each other’s mental problems in contexts of mass trauma and pinpoint early childhood as a sensitive period for such mutual influences.Reference Yirmiya, Motsan and Kanat-Maymon16 Since the mental problems of parents and their related behaviors can be a secondary source of mental problems for children, integrated family-centered interventions and parent and family support services can improve the mental recovery of children after disasters. Especially mother-focused interventions may facilitate proper identification and adequate regulation of mother’s own as well as the child’s mental problems both in the short and long term after a disaster.Reference Tunç, Çelik and Kaçmaz15, Reference Yirmiya, Motsan and Kanat-Maymon16
Assessing children’s post-disaster mental health poses challenges for health care professionals, as many tools are available but vary in scope, complexity, and applicability.Reference Atazadeh, Mahmoodi and Shaghaghi17 The growing number and diversity of these tools may cause confusion in selecting a reliable and valid instrument for practical use. Single-item mental health scales, which have gained attention for their efficiency, may help health care providers rapidly screen mother–child dyads in disaster settings.Reference Ahmad, Jhajj and Stewart18 Since forcing children to talk about their traumas in the early months after an earthquake may not be appropriate,Reference Juth, Silver and Seyle19 we preferred using single-item questions about general mental health status. Scalable single-item screening tools SRMH (the Self-Reported Mother Mental Health) and MRCMH (the Mother-Reported Child Mental Health) are relatively easy to understand for mothers, place minimal response burden, and capture a mother’s global evaluation of their own and their children’s mental state, and hence both ill-health and positive aspects.Reference Yalçın, Tezol and Erat Nergiz20 These are important advantages especially in post-disaster settings. On the other hand, single-item tools provide limited contextual information on the nature and severity of symptoms or the type of mental health condition.21
Against this background, the present study aims to (i) evaluate the mental health of play-age children and their mothers affected by the 2023 Türkiye–Syria earthquakes using single-item scales, (ii) compare negative mental states before and after the disaster, and (iii) identify factors associated with these negative outcomes. Considering the profound developmental implications of early childhood trauma, this study seeks to address a critical gap in the literature on earthquakes and mental health in play-age populations.
Methods
This analytical cross-sectional study was conducted in tertiary hospitals located in cities declared as earthquake-affected regions. Between the 8th and 12th weeks following the earthquake, mother–child dyads who were earthquake survivors and presented to well-child or general pediatric outpatient clinics were included in the study. The inclusion criteria for children were as follows: being 24–60 months old, and having no chronic disease or mental disorder. The inclusion criteria for mothers were as follows: proficiency in the Turkish language, and absence of mental disorders or substance dependence. Migrant mother–child dyads were excluded from the study. The mothers’ written consents were obtained to participate. This study was approved by Mersin University Clinical Research Ethics Committee (MEU 2023-04-12/241).
Data were collected between April 15 and May 15, 2023, through face-to-face interviews using a structured questionnaire form. Sociodemographic and earthquake-related characteristics of the participants were recorded, including the city in which they experienced the earthquake, housing damage, initial shelter after the earthquake, current shelter, current access to healthy food and clean water, and post-earthquake health problems of the child. Mothers were asked about their perceptions regarding the shelter, health, safety, hygiene, nutrition, education, and psychosocial support services provided to them after the earthquake, and were requested to rate these services on a scale from 0 to 10: 0–3 points as “poor,” 4–6 points as “moderate,” and 7–10 points as “good.”
The mental health of mothers and children was assessed using a single-item screening tool. The Self-Reported Mother Mental Health (SRMH) and the Mother-Reported Child Mental Health (MRCMH) instruments, validated by Yalçın et al.,Reference Yalçın, Tezol and Erat Nergiz20 are single-item mental health screening tools that can measure depression, anxiety, stress, and psychological distress in mothers, as well as psychosocial and behavioral strengths and difficulties in children aged 2–5 years.Reference Yalçın, Tezol and Erat Nergiz20 Mothers were asked 4 questions to assess their mental health status on the day before the earthquake and on the day of data collection (current status): (i) “How would you rate your overall sense of well-being and mental health? At the present time, would you say your mental health is.?”, (ii) “How would you rate your overall sense of well-being and mental health? The day before the earthquake, would you say your mental health is.?”, (iii) “How would you describe your child’s mental health? At the present time, would you say your child’s mental health is.?”, (iv) “How would you describe your child’s mental health? The day before the earthquake, would you say your child’s mental health is.?”. Mothers were asked to rate their own mental health status (SRMH) and that of their child (MRCMH) as follows: 1 = excellent, 2 = very good, 3 = good, 4 = fair, 5 = poor. Responses of “excellent, very good, good” on the 5-point Likert-type scale were defined as a positive mental state, while responses of “fair, poor” were defined as a negative mental state.Reference Yalçın, Tezol and Erat Nergiz20 Scores referring to the day before the earthquake were considered as pre-earthquake, and current scores were considered as post-earthquake.
Statistical Analyses
The statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 21.0. Normality was assessed with the Shapiro-Wilk test and histograms. For continuous variables median (IQR 25th–75th percentiles) values, for categorical variables numbers (n) and percentages (%) were given as descriptive statistics. Comparison of 2 dependent groups was examined with Wilcoxon Signed Ranks Test and McNemar test, while 2 independent groups were compared using the Mann–Whitney U test and Chi-square test. Univariate logistic regression analyses were first performed to explore potential predictors of negative post-earthquake SRMH and MRCMH. Variables with a P value < 0.25 in univariate analyses (Mann–Whitney U test for continuous variables and Chi-square test for categorical variables) were entered into the multivariable logistic regression model. Collinearity diagnostics were conducted, and no multicollinearity was detected (Variance Inflation Factor [VIF] and tolerance values were within acceptable ranges). The enter method was used for model construction. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were calculated for each predictor. A P value < 0.05 was considered statistically significant.
Results
Sociodemographic Characteristics
Sociodemographic characteristics are presented in Table 1. The median (IQR) age of the children was 40.5 (30.5–49.0) months; 48% were male, and 35.3% were firstborn. Before the earthquake, 85.7% of the children were cared for by their mothers, and this rate increased to 90.8% after the earthquake. The median (IQR) ages of mothers and fathers were 31 (27.5–35) years and 34 (30–38) years, respectively. A total of 57.3% of mothers and 66% of fathers had a high school or university education level. Regarding maternal employment status, 77.5% were not working either before or after the earthquake, 16.7% were employed both before and after the earthquake, and 5.8% had left or lost their jobs due to the earthquake. Among the families, 21.8% had only one child, and 89.5% were nuclear families.
Sociodemographic and earthquake-related characteristics, n = 400

Table 1. Long description
The table is divided into four main thematic areas.
1. Child-related factors:
* Median age is 40.5 months.
* Gender: 192 males (48.0 percent) and 208 females (52.0 percent).
* Gestational age: 363 (90.7 percent) were born at 37 weeks or more.
* Nutrition: 242 (60.5 percent) had exclusive breastfeeding in the first 6 months.
* Primary caretaker: Shifted from 85.7 percent mothers before the earthquake to 90.8 percent after.
2. Living province and health status:
* Most affected cities: Adiyaman (39.8 percent), Sanliurfa (25.5 percent), and Adana (18.8 percent).
* House damage: 24.5 percent undamaged, 33.5 percent light damage, 18.5 percent moderate, 17.0 percent heavy, and 6.5 percent collapsed.
* Post-earthquake health: 72.5 percent reported illness (fever, diarrhea, or rash), and 33.8 percent reported sleep problems.
3. Mother and Family-related factors:
* Mother’s median age: 31 years.
* Mother’s education: 42.7 percent primary school, 34.5 percent high school, and 22.8 percent college.
* Employment: 77.5 percent are not employed.
* Family structure: 89.5 percent nuclear and 10.5 percent extended.
4. Living conditions after the earthquake:
* First sheltering: Motor vehicle (32.3 percent), Tent (32.0 percent), and Temporary house (29.0 percent).
* Current sheltering: 65.0 percent in temporary houses and 14.5 percent in containers.
* Food and water: 50.5 percent have unlimited access to balanced food, and 73.3 percent have unlimited access to safe water.
Data are median (interquartile range, IQR), and number (percentage).
Earthquake-related Characteristics
Earthquake-related characteristics are presented in Table 1. While 24.5% of participants’ homes were undamaged, 23.5% had homes that were severely damaged or destroyed. A total of 27.3% had family members who were injured or died during the earthquake. The 3 most common initial shelter types after the earthquake were motor vehicles (32.3%), tents (32%), and temporarily rented or shared houses (29%). At the time of data collection (8–12 weeks after the earthquake), the three most common current shelters were temporarily rented or shared houses (65%), containers (14.5%), and dormitories (10.8%). Regarding food access, 50.5% of participants had unlimited access to healthy food, 34.5% had access to healthy food only during 3 main meals, and 15% had limited access to food with no regular meals. A total of 26.7% had limited access to clean/safe water. Following the earthquake, 72.5% of children experienced febrile, diarrheal, or rash-related illnesses, 33.8% had sleep problems, and 13.5% experienced accidents or injuries.
Mothers’ Perceptions of the Services Offered to Them
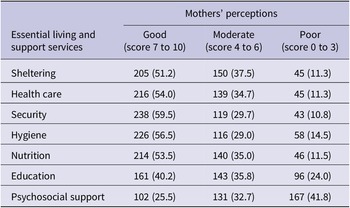
While 51.2% of mothers rated shelter services, 54% rated health services, 59.5% rated security services, 56.5% rated hygiene services, and 53.5% rated nutrition services as “good” (score 7–10), 59.8% rated education services and 74.5% rated psychosocial support services as “moderate–poor” (score 0–6) (Table 2).
Mothers’ perceptions of the services offered to them, n = 400

Table 2. Long description
The table consists of four columns. The first column lists the Essential living and support services. The subsequent three columns represent Mothers’ perceptions: Good (score 7 to 10), Moderate (score 4 to 6), and Poor (score 0 to 3). Data is presented as frequency followed by percentage in parentheses.
* Sheltering: Good 205 (51.2), Moderate 150 (37.5), Poor 45 (11.3).
* Health care: Good 216 (54.0), Moderate 139 (34.7), Poor 45 (11.3).
* Security: Good 238 (59.5), Moderate 119 (29.7), Poor 43 (10.8).
* Hygiene: Good 226 (56.5), Moderate 116 (29.0), Poor 58 (14.5).
* Nutrition: Good 214 (53.5), Moderate 140 (35.0), Poor 46 (11.5).
* Education: Good 161 (40.2), Moderate 143 (35.8), Poor 96 (24.0).
* Psychosocial support: Good 102 (25.5), Moderate 131 (32.7), Poor 167 (41.8).
Single-item Characteristics
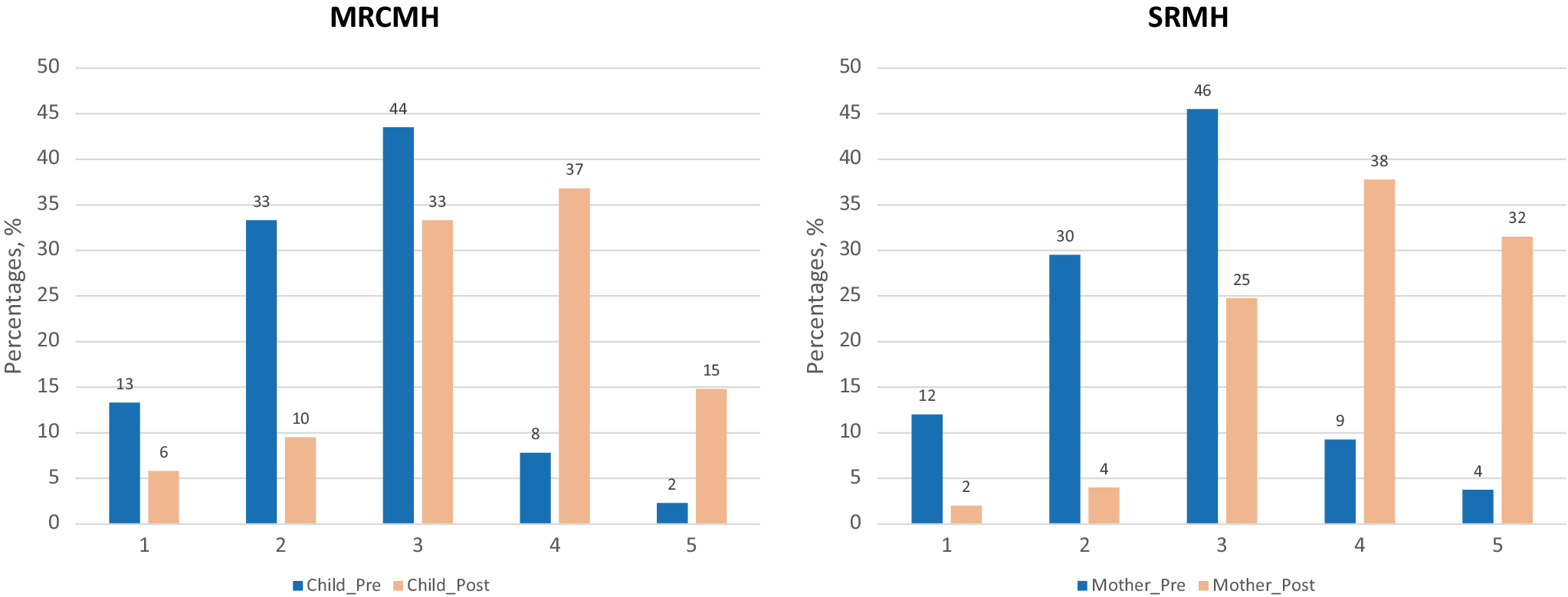
Single-item mental health characteristics are presented in Table 3. Before the earthquake, 90% of children and 87% of mothers had positive mental health, whereas after the earthquake, these rates decreased to 48.5% for children and 30.8% for mothers. With the earthquake, the prevalence of fair mental health increased from 8% to 37% in children and from 9% to 38% in mothers; the prevalence of poor mental health increased from 2% to 15% in children and from 4% to 32% in mothers (Figure 1).
Single-item characteristics of mother-child pairs, n = 400

Table 3. Long description
The table presents data for 400 mother-child pairs across two timeframes: Pre-earthquake and Post-earthquake.
For M R C M H (mother-reported mental health of child) scores:
- Excellent: dropped from 53 (13.3 percent) to 23 (5.8 percent).
- Very good: dropped from 133 (33.3 percent) to 38 (9.5 percent).
- Good: dropped from 174 (43.5 percent) to 133 (33.3 percent).
- Fair: increased from 31 (7.8 percent) to 147 (36.8 percent).
- Poor: increased from 9 (2.3 percent) to 59 (14.8 percent).
Overall M R C M H shifted from 90.0 percent Positive (Excellent-Very good-Good) pre-earthquake to 48.5 percent Positive post-earthquake.
For S R M H (self-reported mental health of mother) scores:
- Excellent: dropped from 48 (12.0 percent) to 8 (2.0 percent).
- Very good: dropped from 118 (29.5 percent) to 16 (4.0 percent).
- Good: dropped from 182 (45.5 percent) to 99 (24.8 percent).
- Fair: increased from 37 (9.3 percent) to 151 (37.8 percent).
- Poor: increased from 15 (3.8 percent) to 126 (31.5 percent).
Overall S R M H shifted from 87.0 percent Positive pre-earthquake to 30.8 percent Positive post-earthquake.
MRCMH: mother-reported mental health of child, SRMH: self-reported mental health of mother.
*Excellent-Very good-Good = positive; **Fair-Poor = negative.
Frequencies of pre- and post-earthquake single-item scale points.
MRCMH; mother-reported mental health of child, SRMH; self-reported mental health of mother. Five-point scales: 1; excellent, 2; very good, 3; good, 4; fair, 5; poor.

Figure 1 Long description
The figure consists of two panels. Both panels use a y-axis labeled Percentages, % ranging from 0 to 50 and an x-axis with scale points 1 through 5. Blue bars represent pre-earthquake data and peach bars represent post-earthquake data.
Left Panel: M R C M H (mother-reported mental health of child).
* Scale 1: Blue 13, Peach 6.
* Scale 2: Blue 33, Peach 10.
* Scale 3: Blue 44, Peach 33.
* Scale 4: Blue 8, Peach 37.
* Scale 5: Blue 2, Peach 15.
The data shows a significant shift from lower scale points (better health) to higher scale points (poorer health) after the earthquake.
Right Panel: S R M H (self-reported mental health of mother).
* Scale 1: Blue 12, Peach 2.
* Scale 2: Blue 30, Peach 4.
* Scale 3: Blue 46, Peach 25.
* Scale 4: Blue 9, Peach 38.
* Scale 5: Blue 4, Peach 32.
Similar to the first panel, there is a pronounced rightward shift toward poorer mental health ratings post-earthquake, particularly in categories 4 and 5.
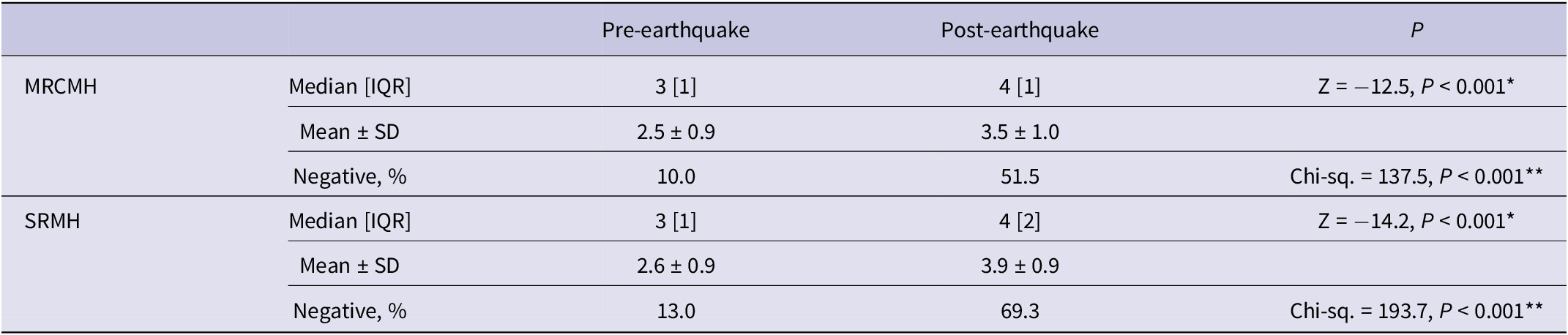
The median MRCMH score was 3 before the earthquake and 4 after the earthquake, and the difference between these scores was significant (P < 0.001). The increase in the prevalence of negative mental health status in children from 10% to 51.5% after the earthquake was statistically significant (P < 0.001). The median SRMH score was 3 before the earthquake and 4 after the earthquake, and the difference between these scores was significant (P < 0.001). The increase in the prevalence of negative mental health status in mothers from 13% to 69.3% after the earthquake was statistically significant (P < 0.001) (Table 4).
Comparison of pre- and post-earthquake mental status of mother-child pairs, n = 400

Table 4. Long description
The table is divided into two primary sections: M R C M H (mother-reported mental health of child) and S R M H (self-reported mental health of mother). Each section includes three rows of data comparing Pre-earthquake and Post-earthquake values.
For M R C M H:
- Median [I Q R]: Pre-earthquake is 3 [1], Post-earthquake is 4 [1]. Z equals minus 12.5, P is less than 0.001.
- Mean plus or minus S D: Pre-earthquake is 2.5 plus or minus 0.9, Post-earthquake is 3.5 plus or minus 1.0.
- Negative percentage: Pre-earthquake is 10.0 percent, Post-earthquake is 51.5 percent. Chi-squared equals 137.5, P is less than 0.001.
For S R M H:
- Median [I Q R]: Pre-earthquake is 3 [1], Post-earthquake is 4 [2]. Z equals minus 14.2, P is less than 0.001.
- Mean plus or minus S D: Pre-earthquake is 2.6 plus or minus 0.9, Post-earthquake is 3.9 plus or minus 0.9.
- Negative percentage: Pre-earthquake is 13.0 percent, Post-earthquake is 69.3 percent. Chi-squared equals 193.7, P is less than 0.001.
Footnotes indicate that Z-scores were calculated via Wilcoxon Signed Ranks Test and Chi-squared values via McNemar test.
MRCMH: mother-reported mental health of child; SRMH: self-reported mental health of mother.
*Wilcoxon Signed Ranks Test;**McNemar test.
Associated Factors for Post-earthquake Negative Mental Health
Compared to the positive SRMH group, the negative SRMH group, and compared to the positive MRCMH group, the negative MRCMH group, had significantly higher frequencies of the following variables (P < 0.05): being cared for by the mother, unemployed mother, severely damaged or destroyed home, presence of febrile, diarrheal, or rash-related illness in the child after the earthquake, initial and current shelter being outside of a house, limited access to healthy food and clean/safe water, and perceiving the services provided as less than “good” (Table 5). The frequency of having a family member injured or deceased in the earthquake was higher in the negative SRMH group than in the positive SRMH group (31% vs. 18.7%, P = 0.010). The median number of people sharing the same shelter was 5 (4–10) in the negative MRCMH group compared to 5 (4–6) in the positive MRCMH group (P = 0.003).
Differences in child–mother–family-living conditions between positive and negative post-earthquake SRMH and MRCMH

Table 5. Long description
The table is divided into two main sections: Post-earthquake S R M H (Self-Reported Mental Health of mother) and Post-earthquake M R C M H (Mother-Reported Mental Health of child). Each section is further divided into Positive and Negative outcomes with associated p-values.
* Child-related factors: Primary caretaker before and after the earthquake shows significant differences. For S R M H, mother as primary caretaker after the earthquake was 83.7 percent in positive vs 93.9 percent in negative (p = 0.001). For M R C M H, it was 86.1 percent vs 95.1 percent (p = 0.002).
* Mother-related factors: Employment status is significant for both. In S R M H, 22 percent of positive cases were employed vs 14.4 percent in negative (p = 0.022). In M R C M H, 21.1 percent positive vs 12.6 percent negative (p = 0.043).
* Earthquake-related factors: Housing damage is highly significant (p = 0.001 for S R M H; p = 0.003 for M R C M H). Undamaged or lightly damaged housing was more prevalent in positive outcomes (71.5 percent for S R M H positive vs 52 percent negative).
* Sheltering and living conditions: Current sheltering in temporary housing and access to safe water are highly significant (p < 0.001). Unlimited access to safe water was reported by 89.4 percent of S R M H positive mothers vs 66.1 percent of negative mothers.
* Perceived service quality: All service categories (sheltering, healthcare, security, hygiene, nutrition, education, and psychosocial support) show highly significant p-values (p < 0.001 or p < 0.05), with positive mental health outcomes correlating strongly with ‘good’ service ratings.
MRCMH: mother-reported mental health of child; SRMH: self-reported mental health of mother.
* Others included motor vehicle, tent, closed fairground, container, hotel, dormitory.
Data are median (interquartile range, IQR), and number (percentage).
Multivariable logistic regression analyses were conducted to identify predictors of post-earthquake negative SRMH and MRCMH. For post-earthquake negative SRMH, significant predictors included limited access to safe water (AOR = 2.52, 95% CI: 1.10–5.75, P = 0.029) and good perception of security services (AOR = 0.30, 95% CI: 0.12–0.73, P = 0.008). Post-earthquake negative MRCMH was strongly associated with post-earthquake negative SRMH (AOR = 8.65, 95% CI: 4.70–15.91, P < 0.001). For post-earthquake negative MRCMH, significant predictors were out-of-house sheltering (AOR = 3.13, 95% CI: 1.72–5.69, P < 0.001), good perception of nutritional services (AOR = 0.46, 95% CI: 0.22–0.96, P = 0.039), and pre-earthquake negative MRCMH (AOR = 4.68, 95% CI: 1.87–11.73, P = 0.001). Additionally, post-earthquake negative SRMH was a strong predictor for post-earthquake negative MRCMH (AOR = 11.35, 95% CI: 5.92–21.76, P < 0.001) (Table 6).
Predictors for post-earthquake negative SRMH and MRCMH

Table 6. Long description
A table presenting Adjusted Odds Ratios A O R, 95 percent Confidence Intervals C I, and p-values for predictors of negative mental health outcomes. The table is divided into two main sections: Post-earthquake S R M H (self-reported mental health of mother) and Post-earthquake M R C M H (mother-reported mental health of child).
Key significant predictors (p < 0.05) include:
* Access to safe water (limited vs. unlimited): A O R 2.52 for negative S R M H.
* Security services (good vs. moderate or poor): A O R 0.30 for negative S R M H.
* Current sheltering (others vs. temporary housing): A O R 3.13 for negative M R C M H.
* Nutrition services (good vs. moderate or poor): A O R 0.46 for negative M R C M H.
* Post-earthquake M R C M H (negative vs. positive): A O R 8.65 for negative S R M H.
* Pre-earthquake M R C M H (negative vs. positive): A O R 4.68 for negative M R C M H.
* Post-earthquake S R M H (negative vs. positive): A O R 11.35 for negative M R C M H.
Other predictors listed include primary caretaker, mother’s employment status, number of children, child health issues (fever, diarrhea, sleep problems, injuries), and access to food. Non-significant values are provided for these categories across both mental health outcomes.
MRCMH: mother-reported mental health of child; SRMH: self-reported mental health of mother; AOR: adjusted odds ratio; CI: confidence interval.
* Others included motor vehicle, tent, closed fairground, container, hotel, dormitory.
Discussion
In order to meet the mental health needs of play-age children in earthquake-affected regions, it is essential first to identify the incidence and predictors of mental health problems. In this study, during the second–third months following the earthquake, the prevalence of negative mental health was 52% among play-age children and 70% among their mothers. Overall, post-earthquake mental health outcomes were most consistently predicted by limited basic resources (water and nutrition services), not good service quality, and pre-existing or co-occurring negative mental health status.
It is known that the frequency of psychosocial difficulties increases in children after earthquakes.Reference Olness8 According to our findings, the prevalence of negative mental health among play-age children increased from 10% before the 2023 earthquakes to 52% after the earthquakes. Within the first 5 months following the 2023 earthquakes, psychiatric problems were identified in 100% of earthquake-affected children and adolescents presenting to child and adolescent psychiatry outpatient clinics, whereas prior to the earthquake only 21% of these cases had a psychiatric diagnosis.Reference Atabey, Karagöz Çetiner and Kaya Çimen10 After the Great East Japan, 2016 Kumamoto, 2018 Lombok, and Sichuan earthquakes, the proportion of children with mental health problems reached epidemic proportions (23% to 54.5% prevalence) in affected regions.Reference Mashiko, Yabe and Maeda22–Reference Liu, Wang and Shi25 The variability in the prevalence of post-earthquake mental health problems can be attributed to factors such as the country in which the earthquake occurred, the severity and duration of exposure, the timing of the assessment, and the methods used for evaluation.
Several risk and protective factors for psychological disorders in children and adolescents after disasters have been identified. (i) Demographic risk factors include older age, female gender, being an only child, low parental education level, and rural residence.Reference Güler Aksu and İmrek12, Reference Liang, Zhou and Liu26 In our study, among play-age children with negative mental health after the earthquake, we found higher frequencies of being cared for by the mother and having a working mother; however, no sociodemographic factor was identified as an associated factor of negative MRCMH. (ii) Pre-earthquake risk factors include physical illness, low self-esteem, adverse life events, prior traumas, and parents with mental problems.Reference Güler Aksu and İmrek12, Reference Liang, Zhou and Liu26, Reference Andrades, García and Kilmer27 In our study, we did not investigate adverse life experiences or previous traumas, and we found that the pre-earthquake SRMH scores of mothers were similar between the negative and positive MRCMH groups. However, we demonstrated that pre-earthquake negative MRCMH and post-earthquake negative SRMH increased the risk of post-earthquake negative MRCMH. (iii) Earthquake-related objective risk factors include the loss of a family member and bereavement, injury of family members or acquaintances (friends, relatives, etc.), witnessing an injury/death, separation from family, personal injury, hospitalization/surgery/amputation, being trapped under debris, damage to the home, and loss of property, whereas protective earthquake-related objective factors are being with family, living under good standards, and being sheltered at home.Reference Güler Aksu and İmrek12, Reference Dutta, Peña and Holcomb28 In our study, among play-age children with negative mental health after the earthquake, we found higher frequencies of having a severely damaged or destroyed home, being sheltered outside the home environment, and experiencing febrile, diarrheal, or rash-related illnesses after the earthquake; however, no earthquake-related objective factor was identified as a predictor of negative MRCMH. (iv) Post-earthquake environmental risk factors include displacement, inadequate social support, delays in seeking care and support, domestic violence, and unmet basic needs, whereas protective post-earthquake environmental factors are early return to routine life, provision of mental health services, adequate social support, a positive family and school environment, and fulfillment of basic needs.Reference Güler Aksu and İmrek12, Reference Fujimaki, Tanno and Kuno29 In our study, among play-age children with negative mental health after the earthquake, we found higher frequencies of limited access to healthy food, limited access to clean water, living with a greater number of people in the same environment indicating overcrowding, and inadequate shelter, health, safety, hygiene, nutrition, education, and psychosocial support; inadequate nutrition services were identified as a predictor of negative MRCMH. We interpreted this finding to mean that in the aftermath of a disaster, adequate nutrition is a top priority for mothers in terms of their children’s mental well-being.
During the acute period after the February 2023 earthquakes, the unmet needs for drinking water, toilets, shelter, heating, clothing, and health care, as well as during the subacute period, the inadequately met needs for clothing, education, and social activities, were found to be factors increasing the risk of mental disorders in children and adolescents.Reference Yakşi and Eroğlu30 We found that during the subacute period, lack of shelter in the home environment increased the risk of negative MRCMH by 3.1 times, whereas perceiving nutrition services as “good” reduced the risk of negative MRCMH by 0.46 times in play-age children. In provinces affected by the February 2023 earthquakes, among breastfeeding mothers with children aged 0–2 years, those who were unemployed, living in tents, living in containers, or living in temporary houses and those without access to complementary food exhibited higher post-traumatic stress.Reference Öz, Küçükkelepçe and Kurt31 Similarly, in our study, the frequencies of unemployed mothers, non-home shelter, and limited access to healthy food were higher among mother–child dyads with negative mental health.
The assessment of children’s mental health cannot be considered separately from family members and family dynamics. Changes and disruptions in family–peer–child systems, along with environmental conditions, are determinants of the impact on child mental health after disasters.Reference Demirci13, Reference Mizuki, Kobayashi and Maeda32 Following an earthquake, paternal stress and maternal depression increase the risk of psychopathology in children, while child psychopathology increases the risk of internalizing problems in parents.Reference Güler Aksu and İmrek12, Reference Forresi, Caputi and Scaini33 Therefore, it is important to assess the mental health of earthquake-affected parents and to review the associated risk factors. These risk factors include the severity of earthquake exposure, loss of family members, exposure to multiple stressors, previous exposure to stressful events, and adverse living conditions. Low educational level and low socioeconomic status are also among the risk factors.Reference Kvestad, Ranjitkar and Ulak7, Reference Demirchyan, Khachadourian and Armenian34 In mothers with negative mental health after the earthquake, we found higher frequencies of being the primary caregiver of the child, being unemployed or leaving work due to the earthquake, having a severely damaged or destroyed home, having a family member injured or deceased in the earthquake, being sheltered outside the home environment, limited access to healthy food, limited access to clean water, and perceiving the services provided for basic needs as inadequate. Limited access to clean water and inadequate security services were identified as predictors of negative SRMH. In addition, we demonstrated that post-earthquake negative MRCMH increased the risk of negative SRMH.
In our study, the prevalence of negative mental health among mothers was 70%, and a considerable proportion of mothers did not rate the basic needs services provided as “good.” During the post-earthquake recovery process, parental dissatisfaction and perceptions of inequality have been shown to predict lower parental happiness and higher levels of child depression.Reference Koyama, Fujiwara, Yagi and Mashiko35 The 2023 earthquakes have been reported to cause significant distress, anxiety, and PTSD among Turkish parents, with 90% expressing concerns about their children’s safety.Reference Dörttepe, Başkaya and Solmaz36 In our study, 59.5% of mothers rated post-earthquake security services as “good,” and perceiving security services as “good” reduced the risk of negative maternal mental health by 0.3 times. We interpreted this finding to mean that in the aftermath of a disaster, security is a top priority for mothers in terms of their own mental well-being. Since we demonstrated that negative maternal mental health increased the risk of negative mental health in children, improving security services will support both maternal and child mental health.
The February 2023 earthquakes struck not only southeastern Türkiye but also Syria, significantly affecting the well-being and psychological health of millions of people in both countries. As mental health resources are limited in both settings, the psychosocial needs of affected children have not been adequately met.Reference Ahmed, Saied and Nashwan37 In our study, only one-quarter of mothers rated post-earthquake psychosocial support services as “good.” This finding highlights the high prevalence of inadequately met psychosocial needs, supporting previous findings.Reference Aydın, Çelik and Açoğlu38
Post-earthquake mental assessment should aim to identify individuals at high risk of developing mental health problems, be conducted with locally adapted tools, encompass the parent–child dyad, and focus on improving family well-being.Reference Kurt, Uygun and Aker39 Although children and parents may respond differently to earthquakes, the most appropriate approach is to evaluate them as a dyad. Previous studies provide new evidence showing a unidirectional pathway from parental earthquake-related symptomatology to the overall mental health of children. In situations where both parents and children are exposed to disasters, their post-traumatic mental responses are reciprocal. Parental psychopathology is among the predictors of emotional and behavioral difficulties in children.Reference Demirci13 Parental positive mental health is the most effective facilitator of children’s recovery and resilience. Dyadic approaches are encouraged in understanding post-traumatic mental health among earthquake-affected families because the psychosocial difficulties of school-age children and adolescents after an earthquake are significantly correlated with their mothers’ psychopathologies such as chronic stress and distress.Reference Usami, Lomboy and Satake1, Reference Akdağ, Arıcı Gürbüz and Bozduman Çelebi40–Reference Nawa, Nakamura and Fujiwara43 According to our findings, there is a positive association between maternal post-earthquake negative mental health and child post-earthquake negative mental health in the 2–5 year age group. In this context, our study has contributed data to the existing literature specifically concerning play-age children.
Mental health problems, inadequate sanitation, lack of access to clean water and safe food, and malnutrition constitute major health issues for children affected by earthquakes.Reference Dube, Moffatt and Davison44 Environmental health risks of the 2023 Türkiye–Syria earthquake in affected areas include structural damage, ground shaking, water and air contamination, displacement and crowding, disease outbreaks, and mental health issues. The risk of malnutrition also became evident.Reference Ahmed, Chandran and Hussein45–Reference Froeschl, Zagli and Erucar47 Consequently, inadequate access to unlimited healthy food, injuries and accidents, limited access to safe water, diarrheal diseases and febrile respiratory illnesses, rash diseases mostly cutaneous infectious illnesses and scabies, and unfavorable health care, educational, economic, and psychosocial facilities were the noticeable health issues for our participants. Also, negative mental health status increased from 10% to 52% in play-age children and from 13% to 70% in their mothers. Poor perceptions of the services, sheltering, health care, security, hygiene, nutrition, education, and psychosocial support were more common in mothers with negative mental health. Ensuring and maintaining family-friendly shelter, healthy nutrition, unlimited access to clean water, safety, and positive maternal mental health will be protective against mental health problems in play-age children.
The needs of individuals and communities change over time following disaster events.Reference Gao and Wang48 During the acute (1–7 days after the earthquake) and subacute (8–30 days after the earthquake) phases, most people’s priority is basic safety and survival. Once that need is secured, and the recovery phase begins, other psychosocial needs emerge that had been previously frustrated and unfulfilled. In early recovery phase, although the affected population is in a more stable period of transition, ongoing adversities are common and complicate recovery. Psychosocial needs, distress, concern, and dissatisfaction may also be intense in the recovery phase.Reference Gao and Wang48 The timing of data collection in our study fell on the early recovery phase after the earthquakes. We propose that this timing enabled mothers to state their own and their children’s mental status reliably.
Globally, the impact of disasters on children’s mental health and the search for practical tools to measure these effects are becoming increasingly important issues. In earthquake situations, medical care services primarily focus on physical health. However, the mental health problems of earthquake-affected children and families should be addressed with equal priority.Reference Atazadeh, Mahmoodi and Shaghaghi17 As there is often a shortage of mental health specialists in earthquake-affected regions, the recognition of mental problems in children and families frequently falls to other health care or social service workers.Reference Peyravi, Ahmadi Marzaleh and Khorram-Manesh49 Single-item scales, SRMH and MRCMH, may provide practicality in screening, assessing, and monitoring negative mental health in mother–child dyads affected by earthquakes, thereby facilitating early and rapid interventions in emergency shelters, mobile clinics, community outreach, and early childhood programs.
This study has several strengths. First, it specifically focused on play-age children and evaluated mother–child dyads together. Second, a valid, reliable, rapid, and easily applicable screening tool was used to identify mother–child dyads who developed negative mental health after the earthquakes. Third, the selected screening tools have the capacity to identify multiple mental health problems; for example, negative SRMH may indicate depression, anxiety, stress, and psychological distress in mothers, while negative MRCMH may point to abnormal difficulties (covering internalizing and externalizing problems) and abnormal prosocial behaviors in children. Fourth, the large sample size provided sufficient statistical power to examine numerous confounding variables.
Study Limitations
In contrast to its strengths, our study has several limitations. These include the cross-sectional study design without making causal inferences and longitudinal follow-up, the fact that the mental health status of family members other than the mother–child dyad was not assessed, and the evaluation of services for basic needs based solely on the mother’s subjective perception. A mother in a negative mental state may be more likely to perceive services negatively. Hence subjectivity of service ratings rather than objective measures of aid delivery has potentially created a circular correlation. A potential recall bias when rating pre-earthquake mental health states has been possible. Child and maternal mental health were assessed via mother-report only, and as such the data are subject to willingness to report completely and truthfully. Lastly, the exclusion of the migrant/refugee dyads may have limited generalizability. Further longitudinal follow-up studies considering also paternal mental health and broader family dynamics are needed to distinguish between acute stress reactions and the development of chronic conditions like PTSD.
Conclusions
Our findings may raise awareness about mental health issues and coping strategies in play-age children and mother dyads. To mitigate the impact of earthquakes on mental health, play-age children should be sheltered in a home environment, have access to healthy food and clean water, and be provided with safety. The mental health of young children and their parents in earthquake-affected regions should be addressed and supported together.
Author contribution
Study conception and design: ÖT, SSY, BG, HA, AB, MEN, EÖ. Acquisition of data: ÖT, BG, HA, AB, MEN, EÖ. Analysis and interpretation of data: ÖT, SSY. Drafting of manuscript: ÖT. Critical revision: SSY. All authors approved the final version of the manuscript and agree to be accountable for authenticity and integrity of the work.
Funding statement
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
The authors have no relevant financial or nonfinancial interests to disclose.
Competing interests
The authors declare no competing interests.
Ethical standards
This study was performed in line with the principles of the Declaration of Helsinki and the study protocol was approved by Mersin University Clinical Research Ethics Committee (MEU 2023/241).
Informed consent was obtained for all participants.





 Open access
Open access