


Introduction
Muscular dystrophies are a group of hereditary progressive skeletal muscle diseases. The most common type in this group is Duchenne muscular dystrophy (ORPHA:98896), which follows an X-linked recessive inheritance pattern. Its prevalence is 4.8 per 100,000 individuals. Reference Salari, Fatahi and Valipour1 Approximately 30–40% of cases are due to spontaneous mutations without a family history. Reference Salari, Fatahi and Valipour1,2 More than 90% of cases present with symptoms during early childhood, before the age of five. In this disease, which primarily affects the musculoskeletal system, the involvement of the respiratory and cardiac muscles, as well as the degree of this involvement, are the most important determinants of morbidity and mortality. 2–Reference Rall and Grimm11 During the disease, the contraction function of the heart decreases due to fibrosis of the heart muscle, leading to dilated cardiomyopathy and heart failure. Cardiac magnetic resonance imaging studies have demonstrated that cardiac muscle fibrosis typically begins in the posterobasal region of the left ventricle and subsequently spreads to the free wall of the left ventricle. Reference Sanyal, Johnson, Thapar and Pitner12,Reference Frankel and Rosser13
In the follow-up of patients diagnosed with Duchenne muscular dystrophy, routine assessments include history, cardiological examination, electrocardiography, and echocardiographic evaluation to detect cardiac involvement. Conventional echocardiographic methods can assess the global function of the heart. Recently introduced speckle-tracking echocardiography can evaluate regional contractility abnormalities and detect subclinical cardiac involvement. However, these methods are not available in every centre. Therefore, the search for easily applicable biomarkers for assessing cardiac involvement in Duchenne muscular dystrophy patients has emerged. N-terminal pro-brain natriuretic peptide is a neurohormone released from the ventricles in response to ventricular wall stress. It is a biomarker in guidelines for diagnosing chronic heart failure in adults. Reference McDonagh, Metra and Adamo14 A serum N-terminal pro-brain natriuretic peptide level above 125 pg/ml is used as a diagnostic criterion for chronic heart failure in adults. In 2025, the International Heart and Lung Transplantation Guidelines for the Management of Paediatric Heart Failure recommended serum brain natriuretic peptide/ N-terminal pro-brain natriuretic peptide level measurement in the integrated evaluation and monitoring of children with known heart failure to further define disease severity, disease progression, and response to therapy (Class I, Level of Evidence B). Reference Irwing, Azeka and Adorisio15 Additionally, brain natriuretic peptide/ N-terminal pro-brain natriuretic peptide is recommended as an adjunctive marker, not a stand-alone test, to aid in the diagnosis of new heart failure in symptomatic children (Class I, Level of Evidence B). There are studies in children and adolescents about N-terminal pro-brain natriuretic peptide normal values, but no threshold value for diagnosis of heart failure has been established in studies conducted in children. Reference Mu, Echouffo-Tchugui and Ndumele16,Reference Lam, Higgins and Zhang17 However, studies on N-terminal pro-brain natriuretic peptide value in children with Duchenne muscular dystrophy are limited. Reference Sheybani, Crum, Raucci, Burnette, Markham and Soslow18,Reference Schade van Westrum, Dekker and de Haan19
This study aims to evaluate the value of N-terminal pro-brain natriuretic peptide, a cardiac biomarker, in detecting cardiac involvement, as assessed by real-time three-dimensional echocardiography and three-dimensional speckle-tracking echocardiography, in children with Duchenne muscular dystrophy.
Material and methods
Study population
This cross-sectional study included individuals aged <21 years old who had been followed up for at least 1 year. The study included 38 boys who had been genetically diagnosed with Duchenne muscular dystrophy. Patients with congenital/acquired heart disease, chronic kidney disease, hepatic failure, autoimmune disease, infectious disease, and poor echocardiographic images were excluded from the study. Each participant underwent an interview about medical history, a detailed clinical examination, conventional, tissue Doppler, real-time three-dimensional echocardiography, and three-dimensional speckle-tracking echocardiography. Body mass index and body surface area were calculated using anthropometric measurements. The Haycock formula was used to calculate body surface area [body surface area = 0.024265 × height (cm) 0.3964 × weight (kg) 0.5378]. Height, weight, and body mass index were evaluated using other studies conducted in Turkey to calculate normal values. Reference Neyzi, Bundak and Gökçay20 The standard deviation scores of the blood pressure measurements of the patients included in the study were calculated. Reference Flynn, Kaelber and Baker-Smith21 All procedures contributing to this work comply with the ethical standards of the national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study has been approved by Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine Ethics Committee (E-83045809-604.01.01-790905 on September 26, 2023). Written informed consent was taken from all participants or their legal guardians.
Echocardiographic assessment
The transthoracic echocardiographic examinations of the patients were performed by the same experienced echocardiography specialist using a Philips Epiq echocardiography device (Philips Healthcare, Inc., Andover, MA) and appropriate transducers. Each patient was evaluated according to the American Society of Echocardiography guidelines using two-dimensional, M-mode, colour, pulse, continuous-wave Doppler, and tissue Doppler echocardiography. Reference Lang, Badano and Mor-Avi22 With M-mode echocardiography, the left ventricular end-diastolic and systolic diameters were measured and indexed to body surface area. The fractional shortening was recorded. Using pulse Doppler echocardiography, early diastolic flow (E) and late diastolic flow (A) were measured at the mitral valve. The E/A ratio was calculated. Using tissue Doppler echocardiography, systolic (S’), early diastolic (E’), and late diastolic (A’) velocities were measured at the mitral lateral annulus, and the E’/A’ and E/E’ ratios were calculated. A shortening fraction < 28% and an ejection fraction < 55% are accepted as abnormal.
The real-time three-dimensional echocardiographic images were recorded during 4–6 cardiac cycles by the X5-1 matrix transducer. The frame rate of the images was 15–30 per second. The data were digitally recorded and analysed using Tomtec Arena software, Version 40 (Philips Healthcare, Unterschleissheim, Germany). The left ventricular end-diastolic and systolic volumes were measured by real-time three-dimensional echocardiography and indexed to body surface area. The ejection fraction was recorded. Myocardial deformation was evaluated with three-dimensional speckle-tracking echocardiography. Global longitudinal, circumferential, and radial strains were recorded with three-dimensional speckle-tracking echocardiography. The amount of myocardial deformation is expressed as positive or negative values and is stated as a percentage. During myocardial contraction, the ventricular wall shortens and thickens. The shortening of the ventricular wall compared to before contraction is expressed with negative values (longitudinal and circumferential strain), and the thickening is expressed with positive values (radial strain). Further information about the method was mentioned in our previous articles. Reference Eroğlu, Yüksel, Karagözlü, Acar, Gökalp and Evliyaoğlu23–Reference Eroğlu, Gökalp, Atik, Önal, Acar and Saltık25 Additionally, the longitudinal, circumferential, and radial strains of the 16 regions of the left ventricle were recorded.
Serum N-terminal pro-brain natriuretic peptide levels
Serum N-terminal pro-brain natriuretic peptide values of the patients, which were part of the laboratory tests included in the study, were measured in the biochemistry laboratory using the “Roche Diagnostics™ Cobas E 801, Mannheim, Germany” kit.
In this study, the relationship between the serum N-terminal pro-brain natriuretic peptide values of patients and demographic data, conventional, tissue Doppler, real-time three-dimensional echocardiography, and three-dimensional speckle-tracking echocardiography data was investigated. A serum N-terminal pro-brain natriuretic peptide level above 125 pg/ml is used as a diagnostic criterion for chronic heart failure in adult guidelines. Reference McDonagh, Metra and Adamo14 No threshold value has been established in studies conducted in children. We compared the demographic data, conventional, tissue Doppler, real-time three-dimensional, and three-dimensional speckle-tracking echocardiography data of patients with N-terminal pro-brain natriuretic peptide levels of 125 pg/ml or below and those with N-terminal pro-brain natriuretic peptide levels above 125 pg/ml.
Statistical analysis
The statistical analyses of the study were performed using IBM SPSS v.25 (IBM Corp., Armonk, NY, USA) software. Descriptive statistics for categorical variables were expressed as frequency (n) and percentage (%). The normality of the data distribution was assessed using the Shapiro-Wilk test. Continuous variables were presented as mean, standard deviation, median, and interquartile range. The Mann-Whitney U test was applied to compare continuous variables between two independent groups. Spearman correlation analysis was used to determine the relationship between two continuous variables. A p-value of < 0.05 was considered statistically significant.
Results
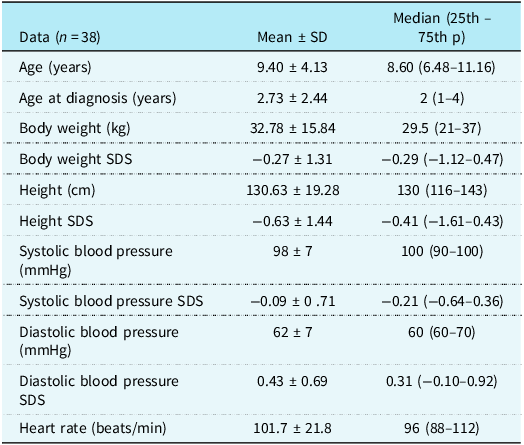
The demographic data of the patients are presented in Table 1. In the study group, 12 out of the 38 patients were unable to walk due to the severity of their disease and were mobilised using a wheelchair. The medications used by the patients: the most commonly used medication group was corticosteroid-type drugs, with 21 patients using them regularly, while 17 patients used them irregularly or not at all. The number of patients receiving angiotensin-converting enzyme inhibitor therapy was 6. Four patients were excluded from the study because of poor echocardiographic images.
Demographic data

Table 1 Long description
The table presents demographic data for 38 patients, detailing various health metrics. It includes columns for mean and median values with standard deviations and percentiles. Key metrics are age, age at diagnosis, body weight, body weight SDS, height, height SDS, systolic blood pressure, systolic blood pressure SDS, diastolic blood pressure, diastolic blood pressure SDS, and heart rate. Each row provides specific data points for these metrics, such as age in years, body weight in kilograms, height in centimeters, and blood pressure in millimeters of mercury. The table highlights the variability and central tendencies of these health indicators among the patients.
P= percentile; SD= standart deviation; SDS= standart deviation score.
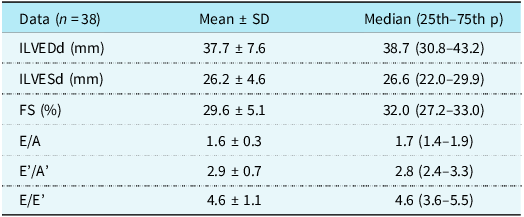
The conventional and tissue Doppler echocardiographic data of the patients are presented in Table 2. The real-time three-dimensional echocardiographic and three-dimensional speckle-tracking echocardiography data of the patients are presented in Table 3.
Conventional and tissue Doppler echocardiography
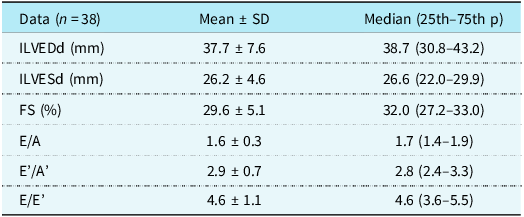
Table 2 Long description
The table presents data on conventional and tissue Doppler echocardiography, focusing on measurements such as ILVEDd, ILVESd, FS, E/A, E'/A', and E/E'. It includes mean values, standard deviations, and median values with percentiles for 38 patients. The table has four rows and three columns, detailing cardiac function parameters in millimeters and percentages.
ILVEDd= indexed left ventricular end-diastolic diameter; ILVSd= indexed left ventricular systolic diameter; FS= fractional shortening; P= percentile; SD= standart deviation.
Real-time three-dimensional echocardiography and three-dimensional speckle-tracking echocardiography
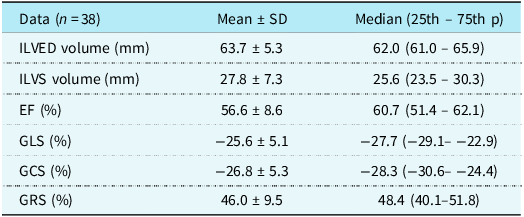
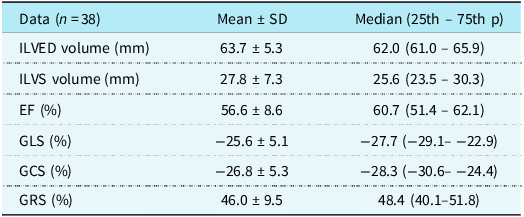
Table 3 Long description
The table presents echocardiographic data for 38 patients, comparing mean values with standard deviation, median values, and 25th to 75th percentiles. The measurements include ILVED volume in millimeters, ILVS volume in millimeters, EF in percentage, GLS in percentage, GCS in percentage, and GRS in percentage. Each row lists these values for the respective measurements, providing a comprehensive overview of the cardiac function parameters.
EF= ejection fraction; GCS= global circumferential strain; GLS= global longitudinal strain; GRS= global radial strain; ILVED= indexed left ventricular end-diastolic; ILVS= indexed left ventricular systolic; P= percentile; SD= standart deviation.
There was no statistically significant correlation between serum N-terminal pro-brain natriuretic peptide levels and demographic or clinical variables (age, age at diagnosis, body weight SDS, height SDS, blood pressure SDS, and heart rate) nor with conventional and tissue Doppler echocardiographic indices (indexed LV diameters, fractional shortening, E/A, E′/A′, and E/E′) or real-time three-dimensional echocardiographic data (LV end-diastolic volume, LV end-systolic volume, and ejection fraction). Likewise, N-terminal pro-brain natriuretic peptide was not significantly correlated with global myocardial strain indices measured by three-dimensional speckle-tracking echocardiography, including global longitudinal strain, global circumferential strain, and global radial strain (all p > 0.05; Supplementary Table S1). The corresponding scatter plots for age, left ventricular volumes, ejection fraction, global longitudinal strain, global circumferential strain, and global radial strain are presented in Supplementary Figure S1 and confirm the absence of significant associations.
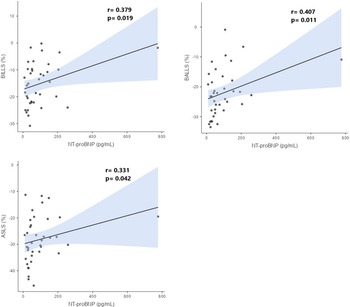
In contrast, N-terminal pro-brain natriuretic peptide levels showed moderate, statistically significant correlations with several regional strain parameters. Among longitudinal strain values, basal inferolateral longitudinal strain, basal anterolateral longitudinal strain, and apical septal longitudinal strain were moderately and significantly associated with NT-proBNP (r = 0.379, p = 0.019; r = 0.407, p = 0.011; and r = 0.331, p = 0.042, respectively). For radial strain, basal inferolateral radial strain and basal anterolateral radial strain were moderately and significantly correlated with N-terminal pro-brain natriuretic peptide (r = –0.351, p = 0.031 and r = –0.328, p = 0.045, respectively) (Supplementary Table S1). These relationships are illustrated in Figure 1 (longitudinal strain) and Figure 2 (radial strain). Correlations between N-terminal pro-brain natriuretic peptide and all other regional segmental strain parameters are provided in full in Supplementary Table S1.
Correlation curves between N-terminal pro-brain natriuretic peptide and basal inferolateral longitudinal strain (BILLS), basal anterolateral longitudinal strain (BALLS), and apical septal longitudinal strain (ASLS). Note: The shaded area indicates the 95% confidence interval.

Figure 1 Long description
Three scatter plots illustrate the correlation between N-terminal pro-brain natriuretic peptide (NT-proBNP) levels and three types of longitudinal strain measurements: basal inferolateral longitudinal strain (BILLS), basal anterolateral longitudinal strain (BALLS), and apical septal longitudinal strain (ASLS). Each plot features a linear regression line with a shaded area indicating the 95% confidence interval. The x-axis represents NT-proBNP levels in picograms per milliliter, while the y-axis represents the percentage change in longitudinal strain. The top left plot shows a correlation coefficient (r) of 0.379 with a p-value of 0.019 for BILLS. The top right plot shows a correlation coefficient (r) of 0.407 with a p-value of 0.011 for BALLS. The bottom plot shows a correlation coefficient (r) of 0.331 with a p-value of 0.042 for ASLS. Each plot includes scattered data points representing individual measurements.
Correlation curves between N-terminal pro-brain natriuretic peptide (NT-proBNP) and basal inferolateral radial strain (BILRS) and basal anterolateral radial strain (BALRS). Note: The shaded area indicates the 95% confidence interval.

Figure 2 Long description
Two scatter plots side by side show the correlation between NT-proBNP levels and BILRS and BALRS percentages. The left scatter plot depicts the correlation between NT-proBNP levels in picograms per milliliter and BILRS percentage. The right scatter plot depicts the correlation between NT-proBNP levels in picograms per milliliter and BALRS percentage. Each plot features a trend line with a shaded area indicating the 95 percent confidence interval. The left plot shows a correlation coefficient of negative 0.351 with a p-value of 0.031, indicating a statistically significant negative correlation. The right plot shows a correlation coefficient of negative 0.328 with a p-value of 0.045, also indicating a statistically significant negative correlation. The x-axis for both plots represents NT-proBNP levels ranging from 0 to 800 picograms per milliliter. The y-axis for the left plot represents BILRS percentage ranging from 0 to 75 percent, while the y-axis for the right plot represents BALRS percentage ranging from 0 to 50 percent. The trend lines in both plots show a downward slope, indicating that as NT-proBNP levels increase, both BILRS and BALRS percentages decrease. All values are approximated.
When patients were stratified according to N-terminal pro-brain natriuretic peptide level (≤125 pg/mL vs. >125 pg/mL), there was no statistically significant difference between the two groups in terms of demographic characteristics, conventional and tissue Doppler echocardiographic measurements, or real-time three-dimensional echocardiographic data (Supplementary Tables S2 and S3). Similarly, most global and regional strain measurements did not differ significantly between the groups, with the exception of basal anterolateral longitudinal strain, which was significantly more impaired in patients with N-terminal pro-brain natriuretic peptide > 125 pg/mL compared with those with N-terminal pro-brain natriuretic peptide ≤ 125 pg/mL (median –19.70 [–22.25 to –11.10] vs. –24.45 [–28.80 to –19.20], p = 0.032; Supplementary Table S4).
Discussion
In our study, no relationship was found between serum N-terminal pro-brain natriuretic peptide levels and conventional and tissue Doppler echocardiographic data, volume, and contraction data measured by real-time three-dimensional echocardiography, as well as global contraction data measured by three-dimensional speckle-tracking echocardiography in children with Duchenne muscular dystrophy. A relationship was found only between serum N-terminal pro-brain natriuretic peptide levels and some regional contraction data in the basal and apical regions. There was a moderate correlation between serum N-terminal pro-brain natriuretic peptide levels and longitudinal and radial strain in left ventricular basal anterolateral and inferolateral regions and longitudinal strain in the apical septal region. It was concluded that N-terminal pro-brain natriuretic peptide is a very important marker in detecting regional contraction abnormalities in children with Duchenne muscular dystrophy.
Currently, the expected life span of patients with Duchenne muscular dystrophy is around 30 years Reference Landfeldt, Thompson, Sejersen, McMillan, Kirschner and Lochmüller4,Reference Eroğlu, Yüksel, Karagözlü, Acar, Gökalp and Evliyaoğlu23,Reference Kieny, Chollet and Delalande26 . The involvement of respiratory and cardiac muscles is one of the leading causes of morbidity and mortality. Opportunities for supportive treatment for respiratory failure have increased. Non-invasive respiratory support therapies can be applied to these patients. Heart failure has been identified as the most common cause of death with the reduction of deaths related to respiratory failure. Reference Goyder, Roalfe and Jones27 Many studies conducted in patients with Duchenne muscular dystrophy have shown that early detection of heart failure improves quality of life and survival. Reference McDonagh, Metra and Adamo14,Reference Taylor, Ordóñez-Mena and Roalfe28,Reference Taylor, Hobbs, Marshall, Leyva-Leon and Gale29 Therefore, the search for a cardiac biomarker has emerged to evaluate cardiac involvement using an easily accessible and repeatable method. N-terminal pro-brain natriuretic peptide is an important cardiac biomarker frequently used to diagnose and monitor heart failure. A serum N-terminal pro-brain natriuretic peptide level above 125 pg/ml is used as a diagnostic criterion for chronic heart failure in adult guidelines. Reference McDonagh, Metra and Adamo14 In 2025, the International Heart and Lung Transplantation Guidelines for the Management of Paediatric Heart Failure recommended serum brain natriuretic peptide/ N-termimal pro-brain natriuretic peptide level measurements in the integrated evaluation and monitoring of children with known heart failure to further define disease severity, disease progression, and response to therapy (Class I, Level of Evidence B). Reference Irwing, Azeka and Adorisio15 Additionally, these biomarkers are recommended as adjunctive markers, not a stand-alone test, to aid in the diagnosis of new heart failure in symptomatic children (Class I, Level of Evidence B). There are studies in children and adolescents about N-terminal pro-brain natriuretic peptide normal values, but no threshold value for diagnosis of heart failure has been established in studies conducted in children. Reference Mu, Echouffo-Tchugui and Ndumele16,Reference Lam, Higgins and Zhang17 In the future, further multicenter studies should aim to establish normative ranges and validate N-terminal pro-brain natriuretic peptide in the diagnosis of pediatric heart failure. Determining serum N-terminal pro-brain natriuretic peptide levels may guide the early detection of cardiac involvement in Duchenne muscular dystrophy patients and help in timing treatment options during follow-up.
In a study involving 78 adult patients diagnosed with Duchenne muscular dystrophy, where cardiac biomarkers N-terminal pro-brain natriuretic peptide and troponin I were evaluated with cardiac magnetic resonance imaging findings, N-terminal pro-brain natriuretic peptide emerged as a biomarker associated with cardiopulmonary failure-related deaths. Reference Soslow, Xu and Slaughter30 However, no such study has been conducted in children.
In another study by Sheybani et al. Reference Irwing, Azeka and Adorisio15 in 2022, involving 61 Duchenne muscular dystrophy children with an average age of 13 and 18 healthy control children with an average age of 14.5, N-terminal pro-brain natriuretic peptide was found to be related to indexed left ventricular end-diastolic volume and left atrium volume according to body surface area by cardiac magnetic resonance imaging. Our study demonstrated no relationship between serum N-terminal pro-brain natriuretic peptide levels and left ventricular volumes measured by real-time three-dimensional echocardiography. This difference may be due to the younger age of our patients or technical differences between two different imaging techniques.
In a study investigating the value of N-terminal pro-brain natriuretic peptide in predicting dilated cardiomyopathy, conducted between 2002 and 2005, involving 143 patients aged 8–70 years (primarily adults) with Duchenne muscular dystrophy, Becker muscular dystrophy, and 219 carriers of these diseases, 78 % of the participants had N-terminal pro-brain natriuretic peptide levels above the upper limit of the laboratory kit (95 pg/ml). Reference Mu, Echouffo-Tchugui and Ndumele16 This study found no significant relationship between N-terminal pro-brain natriuretic peptide and dilated cardiomyopathy. Although the sensitivity of N-terminal pro-brain natriuretic peptide in detecting dilated cardiomyopathy was found to be 85%, its specificity was very low at 23%. The frequency of dilated cardiomyopathy in the subjects was 17%. In their study, the diagnostic criteria for dilated cardiomyopathy were defined according to the World Health Organization’s guidelines as an enlarged left ventricle accompanied by global left ventricular systolic dysfunction or a fractional shortening of 28% or less. Since our study only included patients with Duchenne muscular dystrophy, even though our patients were younger, 31% of them had dilated cardiomyopathy with an ejection fraction of less than 55%. In our study, similar to that study, no relationship was found between N-terminal pro-brain natriuretic peptide and ejection fraction.
In a study conducted by Mori et al. Reference Mori, Manabe, Nii, Hayabuchi, Kuroda and Tatara31 in 2002, which included 63 patients diagnosed with Duchenne muscular dystrophy, with ages ranging from 8 to 21 years and an average age of 15.8 years, the relationship between serum atrial natriuretic peptide and brain natriuretic peptide levels and left ventricular ejection fraction was investigated. No relationship was found between these biomarkers and ejection fraction. Brain natriuretic peptide levels increased dramatically in patients with an ejection fraction below 15%. It was concluded that brain natriuretic peptide levels were not sensitive for the early stages of heart failure but were significant for the later stages. In our study, N-terminal pro-brain natriuretic peptide levels were measured, and our patients were younger. Similarly, no relationship was found between N-terminal pro-brain natriuretic peptide and ejection fraction.
Conventional echocardiography evaluates the heart in two dimensions and does not evaluate regional contractility in patients with regional contractile disorders such as Duchenne muscular dystrophy. Left ventricular volume measurements and global contractility can be assessed in three dimensions with the introduction of real-time three-dimensional echocardiography in recent years. With speckle-tracking echocardiography, strain measurements can be performed to evaluate global and regional contractility disorders. Many studies have shown that Duchenne muscular dystrophy patients with normal ejection fraction and fractional shortening have impairment in both global and regional strain.,Reference Song, Zhang, Wang, Zhang, Sun and Yu32,Reference Amedro, Vincenti and De La Villeon33 Therefore, myocardial strain measured by speckle-tracking echocardiography is an important marker for early detection of cardiac involvement. Most of these studies were conducted with two-dimensional speckle-tracking echocardiography. However, one study was conducted using the more advanced technology of three-dimensional speckle-tracking echocardiography. Reference Irwing, Azeka and Adorisio15
A meta-analysis conducted in 2020, which reviewed eight separate studies involving 269 patients diagnosed with Duchenne muscular dystrophy and 299 healthy controls, predicted that the measurement of ejection fraction might be insufficient for evaluating cardiac systolic function in this patient group. Reference Song, Zhang, Wang, Zhang, Sun and Yu32 It has been suggested that regional left ventricular dysfunctions can be detected by measuring strain using speckle-tracking echocardiography before the left ventricular ejection fraction is affected. However, these studies were conducted in different age groups, and there are inconsistencies in their results. This meta-analysis stated that global longitudinal strain shows longitudinal contractions as a whole and is helpful in the early detection of cardiac involvement. They did not make any comment on regional contraction abnormalities due to insufficient data in this meta-analysis.
In a 2016 study by Amedro et al. Reference Amedro, Vincenti and De La Villeon33 , which was included in this meta-analysis, 36 Duchenne muscular dystrophy patients with a mean age of 11 years, all younger than 18, and 72 healthy controls in a similar age group were examined by two-dimensional speckle-tracking echocardiography. The basal inferolateral and anterolateral regions were the most affected. Additionally, many longitudinal segments were affected. Similarly, our study found a relationship between N-terminal pro-brain natriuretic peptide and basal inferolateral and anterolateral longitudinal and radial strains.
In the study published by Mertens et al. Reference Mertens, Ganame and Claus34 in 2008, the examination of 3–12-year-old Duchenne muscular dystrophy patients with a mean age of 7.9 years and 29 healthy controls with a mean age of 7.7 years using two-dimensional speckle-tracking echocardiography showed that despite normal ejection fraction, basal inferolateral and anterolateral longitudinal and radial strains were impaired. Our study found an association between N-terminal pro-brain natriuretic peptide and myocardial strain values of the same regions.
In our study, the reference threshold value for N-terminal pro-brain natriuretic peptide was accepted as 125 pg/ml. Patients were divided into two groups (<125 pg/ml and ≥125 pg/ml) and compared based on this threshold. Among all the global and regional strain measurements obtained by conventional, real-time three-dimensional echocardiography and speckle-tracking echocardiography, only the longitudinal strain in the basal anterolateral region was significantly impaired in the group with N-terminal pro-brain natriuretic peptide ≥125 pg/ml. This finding supports the relationship between N-terminal pro-brain natriuretic peptide and regional contractility.
The strength of the study lies in the inclusion of 38 patients collected in a single centre, despite Duchenne muscular dystrophy being a rare disease. Also, this study is the first to evaluate the relationship between serum N-terminal pro-brain natriuretic peptide levels and regional contraction function obtained by three-dimensional speckle-tracking echocardiography in children with Duchenne muscular dystrophy. However, there are some limitations of this study. The study is cross-sectional, and the study population is small, with both a narrow range of patient age and disease severity. Another limitation is the fact that some of the patients were under medication. Twenty-one patients were regularly using corticosteroids, and only 6 patients were receiving angiotensin-converting enzyme inhibitor therapy. These sample sizes are insufficient to adequately satisfy the assumptions required for reliable regression modelling, and subgroup analyses would result in very small groups with limited statistical power and an increased risk of unstable or misleading estimates.
In conclusion, the relationship between N-terminal pro-brain natriuretic peptide and regional contraction data holds promise for its value as a biomarker in detecting subclinical cardiac dysfunction. Prospective studies with a larger population with a broader range of disease severity are necessary to demonstrate the importance of serum N-terminal pro-brain natriuretic peptide levels to predict subclinical cardiac dysfunction in patients with Duchenne muscular dystrophy.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126112062.
Acknowledgements
We kindly thank the patients and their families for participating in the study.
Financial support
No funding was received for conducting the study.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical standard
All procedures contributing to this work comply with the ethical standards of the national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study has been approved by Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine Ethics Committee (E-83045809-604.01.01-790905 on September 26, 2023). Written informed consent was taken from all participants or their legal guardians.




 Open access
Open access