


Introduction
Health technology assessment (HTA) plays an important role in Taiwan’s healthcare system by providing scientific, economic, and ethical evidence to inform coverage decisions under the National Health Insurance (NHI). As the NHI covers more than 99 percent of the population (1), assessing the effectiveness, value, and budget impact of new technologies is crucial for equitable access and long-term sustainability (Reference Kao, Huang, Wu and Gau2;Reference Chiu, Pwu and Gau3).
Taiwan’s HTA activities are led primarily by the Center for Drug Evaluation (CDE), commissioned by the NHI Administration (NHIA) to conduct independent assessments of comparative effectiveness and economic evaluation. Initially focused on new drug reimbursements, the HTA system has expanded to include policy-oriented HTA projects commissioned by the Ministry of Health and Welfare (MOHW) and its affiliated agencies, medical device assessment, digital health technologies, and major NHI coverage reforms (Reference Kao, Huang, Wu and Gau2).
Over the past 15 years, the HTA framework has evolved to meet emerging healthcare needs by adopting international best practices and developing approaches suited to Taiwan’s context. Recent reforms, including the Taiwan Cancer Drugs Fund (TCDF) (4), parallel reviews, new draft HTA guidelines for real-world evidence (RWE) and precision medicine, and formalized patient involvement, mark a new stage of system development. Together with ongoing health technology reassessment (HTR), these measures have enhanced the system’s capacity for timely, evidence-based, and value-oriented decision-making (5).
This article synthesizes the evolution and current landscape of HTA in Taiwan, with particular attention to key developments from 2024 to 2025. The analysis integrates historical trends, annual HTA performance data, methodological frameworks, and major policy initiatives to capture Taiwan’s progress toward a sustainable and learning-oriented HTA ecosystem. Taiwan’s HTA development has been shaped through iterative policy learning, drawing on international HTA experiences while adapting them to the institutional context of the NHI system. These experiences have informed the refinement of HTA processes, including evidence assessment, managed entry arrangements, RWE generation, and mechanisms for stakeholder and patient engagement.
Institutional foundations and evolution
Establishment and governance
The CDE, established in 1998 under the MOHW and formally commissioned to conduct HTA in 2008, comprises multidisciplinary experts in medicine, epidemiology, health economics, biostatistics, and public health. Its HTA activities cover new drug reimbursement, indication expansions, high-impact medical devices, and policy-level health and welfare programs (Reference Kao, Huang, Wu and Gau2). HTA reports led by the CDE HTA Division serve as key reference documents for deliberations of the Pharmaceutical Benefits and Reimbursement Scheme (PBRS) Joint Committee, the NHI’s principal advisory body for benefit listing and pricing (Reference Kao, Huang, Wu and Gau2;6).
Standardized HTA workflow and timelines
Taiwan implements a transparent timeline for HTA (7). Rapid HTA reports are typically completed within 42 days after receipt of the full submission dossier, followed by a 7-day period for manufacturers to provide comments, and an additional response period when needed (7). For broader policy-oriented HTA projects, which often involve population-level policy analysis or health system evaluation, the analytical timeline is ~6–12 months, with more complex studies occasionally requiring longer than 1 year. Clinical experts are regularly consulted during HTAs to provide insights into local clinical practice, treatment pathways, and the interpretation of clinical evidence. Their input helps ensure that HTAs appropriately reflect real-world clinical practice and patient needs in Taiwan. All finalized HTA reports are released simultaneously to the National Health Insurance Administration (NHIA) and manufacturers, supporting transparency, early dialogue, and consistent evidence use. Manufacturers are given the opportunity to review the reports and submit comments if they have concerns regarding the interpretation of evidence or other aspects of the assessment process (8–Reference Oortwijn, Husereau and Abelson10).
HTA reports are also publicly available on the NHIA and CDE webpage, where documentation – including assessment rationales and evidence summaries – is accessible, although largely in Mandarin. This disclosure mechanism enhances stakeholder engagement, increases accountability, and aligns Taiwan’s HTA system with international expectations for openness and transparency (8–Reference Oortwijn, Husereau and Abelson10).
Growth into policy-oriented HTA
In 2024, Taiwan’s HTA system conducted 196 rapid HTA reports covering new molecular entities, relative effectiveness and budget impact analyses, new formulations or routes of administration, and applications for expanded indications or reimbursement scope revisions. In addition, twelve HTA assessments were conducted for medical devices. Beyond these evaluations, the HTA system also informs broader health policy areas, including cancer screening, digital health and artificial intelligence (AI), NHI reimbursement and payment system reforms, and healthcare resource allocation. In the same year, the CDE HTA team completed five major policy evaluations commissioned by the MOHW and eight studies supporting reforms of NHI benefit mechanisms. HTA findings may inform policy planning, support policy development, or be directly adopted and implemented in policy.
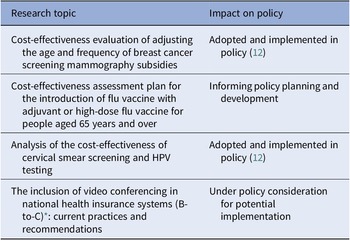
Among the five commissioned evaluations, four have informed policy development or implementation, and the corresponding reports have been publicly released online (Table 1) (11).
Overview of policy-oriented HTA projects supporting health system reform in 2024 (11)

* Note: B-to-C (Business-to-Consumer) refers to telemedicine services delivered directly from healthcare providers to patients via video consultation platforms.
Embedding evidence into decision-making
Taiwan’s HTA system integrates clinical evidence, economic value, and local relevance to inform coverage decisions. Assessments draw on comparative effectiveness evidence, real-world data (RWD), and local clinical input, with particular attention to high clinical impact. Economic and budget impact analyses consider disease severity, unmet needs, affordability, and long-term system sustainability under the global budget.
Given that clinical practice patterns and treatment pathways may differ from those in international settings, Taiwan’s HTA places strong emphasis on local applicability to ensure that reimbursement decisions reflect real-world outcomes. This includes consideration of Taiwanese clinical guidelines, population-specific factors influencing treatment response or safety, local adverse event profiles, and real-world utilization within the NHI system.
Taiwan’s earlier national experience with immune checkpoint inhibitors (ICIs) illustrates the value of integrating local RWD into HTA (6;7). ICIs were selected as a case study because they represented one of the earliest high-cost oncology therapies in Taiwan, where reimbursement decisions were accompanied by structured post-listing evidence generation. Given the substantial clinical uncertainty and financial impact associated with these therapies, the NHIA established a national registry to systematically collect real-world treatment outcomes and utilization data.
Evidence generated from this registry enabled evaluation of treatment effectiveness in routine clinical practice and supported reassessment of reimbursement decisions. For example, RWE collected during the first year of implementation demonstrated that treatment outcomes for certain indications were more limited than expected, prompting expert review and policy discussions regarding reimbursement adjustments and potential cost-effectiveness agreements with manufacturers.
This experience demonstrates how locally generated RWD can complement clinical trial evidence, support life cycle HTA, and strengthen evidence-based decision-making in Taiwan (6;7).
Policy impact
Taiwan’s HTA has expanded from evaluating individual technologies to guiding system-level reforms across prevention, service coverage, and resource allocation. This broader application reflects the increasing role of the HTA as a foundation for evidence-based health policies and long-term NHI sustainability.
Resource optimization and real-world effectiveness evaluation
In 2024, the CDE reassessed both pharmaceuticals and medical devices to optimize resource allocation. Drug-related evaluations included taxane and pyrimidine analog chemotherapies, immunoglobulin, and albumin, along with immune checkpoint inhibitors requiring RWE. Device and procedure reassessments included three-dimensional ablation catheters, ventricular assist devices, and rib fixation systems, examining clinical outcomes, safety, budget impacts, and patterns of use. Supported by RWD from the NHI database, these analyses refine benefit specifications, reduce low-value care, and ensure that coverage decisions align with contemporary clinical practice (13).
These system-level HTA applications extend impact beyond individual appraisals and reinforce their central role in Taiwan’s healthcare delivery, cost-effectiveness-informed reimbursement policies, and evidence-driven resource allocation.
Novel access pathways
Taiwan has introduced novel mechanisms to balance timely patient access, budgetary control, and evidentiary uncertainty in the adoption of new medical technologies. These include the parallel review system, managed entry agreements (MEAs), and temporary reimbursement through the TCDF. Together, these pathways form a framework that supports timely access while maintaining rigorous evaluation and financial sustainability.
Parallel review: accelerating access without sacrificing rigor
Implemented in 2024, the parallel review system enables simultaneous assessment of regulatory documentation and reimbursement evidence by evaluation and insurance agencies. This coordinated approach shortens time-to-access for priority and high-impact therapies while maintaining the rigor of HTA. Previously, reimbursement evaluation generally began only after regulatory approval had been granted, which could result in delays of ~1 year or longer before reimbursement listing. Under the parallel review mechanism, regulatory and reimbursement evaluations can proceed concurrently, with the policy objective of enabling reimbursement implementation within ~6 months after marketing authorization.
Eligible products include priority review and accelerated approval therapies, high clinical impact treatments, pediatric rare-disease medicines, domestically developed novel ingredients, drugs sold internationally for at least 5 years but newly introduced or manufactured locally, and technologies that improve effectiveness or lower cost relative to NHI-covered alternatives (5).
In its first year, the parallel review system completed eighteen eligibility assessments for the parallel review pathway and contributed to reducing the time between regulatory approval and reimbursement listing for priority therapies. It has become a core mechanism aligning regulatory evaluation with reimbursement decisions, forming a key component of Taiwan’s strategy to enable timely, evidence-informed access to novel medical technologies. Its interaction with adaptive reimbursement tools, such as MEAs, supports a coherent, life cycle-based approach to market entry and coverage decisions (5).
Managed entry agreements
Since 2019, Taiwan has implemented a structured MEA framework to address clinical and economic uncertainties.
MEAs have become essential policy tools for managing uncertainties tied to novel or high-cost therapies. These agreements take various forms, including outcome-based arrangements (e.g., survival, response, or progression-linked payments), financial-based agreements (e.g., expenditure caps and price–volume arrangements), and hybrid models combining financial safeguards with clinical performance requirements. MEAs enable conditional access to therapies with uncertain benefits, incentivize manufacturers to generate RWE, and allow future price or coverage adjustments based on observed performance. They play a key role in facilitating timely access to oncological treatments, rare disease therapies, and high-cost biologics within Taiwan’s NHI system.
Temporary reimbursement and the Taiwan cancer drugs fund
To address rapidly growing cancer drug expenditure and urgent patient needs, and having learned from the NICE experience (14), Taiwan established the TCDF as a structured, multiphase, and temporary reimbursement policy (15). This design separates high-impact oncology spending from routine NHI financing while enabling conditional access under evidence development. The TCDF separates high-impact oncology expenditure from routine NHI financing and enables conditional access under evidence development. As of June 2025, twenty-four drugs were temporarily reimbursed. The scheme provides early access while generating RWE to inform final reimbursement decisions, supported by transparent governance, mandatory data submission, periodic reassessment, and financial safeguards such as expenditure caps and claw-backs. Its implementation relies on coordination among NHI, MOHW, CDE, and clinical networks, alongside the development of an integrated precision oncology RWD ecosystem linking next-generation sequencing (NGS), cancer registry, pathology, and claims data to support life cycle HTA.
Overall impact
The integration of parallel reviews, MEAs, and the TCDF represents a major reform in Taiwan’s reimbursement system. These pathways enable rapid, responsible access to high-cost and high-clinical impact therapies, link reimbursement to continuous evidence generation, and support the financial sustainability of NHI. They also enhance the national HTA system’s capacity to manage clinical and economic uncertainty, aligning Taiwan with international best practices for adaptive and life cycle-based reimbursements (5).
Building the evidence ecosystem
Taiwan’s HTA framework is evolving into a learning system, focusing on RWD, precision medicine evaluation methodologies, and systematic health technology reassessment (HTR). These components bridge evidence gaps, manage uncertainty, and optimize coverage decisions. To anticipate future budget pressures and support proactive policy planning, Taiwan has also strengthened its horizon scanning and forward-looking evaluation mechanisms. These activities identify emerging high-impact technologies, estimate timelines to market entry, project potential budget implications, and flag candidates that may require MEAs or temporary reimbursement. Enhanced horizon scanning enables the NHIA and CDE to better prepare for innovations such as CAR-T therapies, gene therapies, and advanced medical devices, ensuring that reimbursement strategies remain adaptive and aligned with rapid scientific and clinical advances. Temporary reimbursement mechanisms, including the TCDF and MEAs, play a central role in life cycle HTA. TCDF requires 2–3 years of RWD generation (extendable to 5 years), after which final reimbursement decisions are made. As highlighted in regional policy discussions, TCDF forms part of Taiwan’s broader strategy to reduce the cancer burden through integration with precision medicine and digital transformation. By linking evidence generation to funding conditions, Taiwan enables earlier access to high-need therapies while managing uncertainty and safeguarding the long-term sustainability of the NHI system (5).
Health technology reassessment: ensuring sustainability
HTR is a core component of Taiwan’s HTA strategy, designed to systematically reevaluate existing covered technologies, identify low-value or outdated interventions, adjust benefit coverage and payment levels, and respond to evolving clinical and economic evidence. In 2024, Taiwan implemented a comprehensive HTR program encompassing pharmaceuticals, high-cost medical devices, and medical services. Medical service reassessments covered areas such as high-flow oxygen therapy, stroke care, robot-assisted surgery, CT-based diagnostic imaging, and diabetes management under the Family Physician Program. Across these domains, HTR integrates structured evidence review, cost-effectiveness analysis, and the use of RWD – applied flexibly according to the specific characteristics and policy needs of each case – to inform adjustments to benefit specifications, payment mechanisms, and coverage scope. Reassessments included major oncology medicines – such as immune checkpoint inhibitors evaluated using national RWD – as well as targeted reviews of selected drugs and high-impact technologies, including transcatheter aortic valve implantation, cardiac ablation devices, and bariatric surgery technologies. Through standardized reassessment procedures combining clinical and economic evidence, the 2024 HTR program supported refinements in benefit design, cost-effectiveness-informed reimbursement policies, renegotiation of managed entry agreements, and decisions on the modification or continuation of temporary reimbursement. Collectively, these efforts strengthened the alignment of reimbursement policies with contemporary clinical value and reinforced the long-term sustainability and accountability of Taiwan’s NHI system.
Patient and patient organization involvement
Strengthening patient engagement has become central to HTA reforms in Taiwan. Since the 2013 amendment of the NHI Act, Taiwan has institutionalized mechanisms to ensure that patient experiences, lived realities, and value preferences meaningfully contribute to HTA deliberations and reimbursement decision-making. Patient participation is embedded across assessment and PBRS processes, reflecting a shift toward transparency, inclusiveness, and patient-centered policy (Reference Chen, Huang and Gau16).
Systematic integration of patient perspectives
Patient input is systematically collected and integrated into HTA through structured mechanisms, including a national submission platform and mandatory synthesis of patient perspectives within HTA reports for PBRS deliberation. Patient evidence is used to contextualize unmet needs, disease burden, and treatment goals – particularly for chronic, rare, and oncologic conditions – and is publicly disclosed to enhance transparency. These processes ensure that patient perspectives complement clinical and economic evidence in decision-making (Reference Chen, Huang and Gau16).
Pre-meeting mechanisms and stakeholder engagement
Since 2019, the CDE has convened twenty-nine pre-PBRS patient engagement meetings with patient groups, insured representatives, and caregivers. The insured representatives participating in these meetings are the formal representatives of the PBRS Joint Committee.
These efforts aim to clarify key uncertainties and unmet needs, consolidate patient input, prepare patient representatives for PBRS participation, and facilitate dialogue between HTA assessors and patient organizations to ensure accurate representation of patient evidence (Reference Chen, Huang and Gau16). During these meetings, the CDE HTA team also presents how patient submissions collected through the NHIA platform have been synthesized and incorporated into HTA reports and reimbursement deliberations, allowing patient groups to review the summaries and confirm whether any perspectives have been missed or whether additional input should be included.
From May 2015 to October 2024, seventy-five technologies (forty-five oncology, twenty-eight non-oncology, and two medical devices) incorporated patient input before the PBRS review. This cumulative figure spans multiple years and is not directly comparable to the number of HTA assessments conducted in 2024. These interactions show a process that is structured and adaptive, evolving from early patient submissions to more sophisticated inputs gathered by patient organizations through surveys, focus groups, and community networks.
Ongoing challenges and areas for future improvement
Despite the substantial progress described above, several challenges have accompanied the development of Taiwan’s HTA system. As HTA has become increasingly central to reimbursement and policy decision-making under the NHI, expectations from multiple stakeholders – including clinicians, industry, policymakers, and patients – have also increased. Balancing timely access to novel technologies with financial sustainability and evidence-based decision-making remains an ongoing policy challenge. As HTA activities expand, maintaining constructive dialogue with clinicians, industry, and other stakeholders is essential to address differing perspectives on access, evidence requirements, and reimbursement priorities.
The introduction of adaptive policy tools, such as managed entry agreements and temporary reimbursement mechanisms, has also required continuous institutional learning and coordination across regulatory, payer, and clinical stakeholders. Another key challenge has been strengthening the infrastructure for RWE generation to support life cycle HTA and reassessment. As novel and high-cost therapies increasingly enter the healthcare system, the ability to generate and use RWD to inform coverage decisions and policy adjustments has become increasingly important. Taiwan has addressed these challenges through gradual policy reforms, capacity building, and enhanced stakeholder engagement mechanisms, including transparent HTA processes.
At the institutional level, the expansion of HTA activities has increased the workload of the HTA agency. Over time, the scope of HTA has expanded beyond new drug assessment to include policy evaluations, medical devices, reassessments, and evidence generation initiatives. To support these developments, the HTA workforce has gradually expanded, accompanied by structured training programs and a clearer division of responsibilities across multidisciplinary teams. Standard operating procedures have been established to guide the HTA workflow and ensure consistent, transparent, and efficient assessment processes.
Despite these mechanisms, challenges remain in broadening awareness and participation. Patient input is still evolving in scope and impact, partly due to limited awareness of the platform and resource constraints among patient organizations. Additionally, the PBRS Joint Committee agenda is typically published ~7 days before the meeting, leaving limited time for patient representatives to gather and synthesize input on multiple technologies.
To address these issues, the CDE HTA team has drawn on international best practice, including tools developed by the Health Technology Assessment International (HTAi) Patient and Citizen Involvement in HTA Interest Group (PCIG). With the support of NHIA, the patient submission platform has been progressively refined to improve usability and better capture patient experiences. These improvements aim to facilitate more meaningful participation and strengthen the integration of patient perspectives into HTA deliberations.
International collaboration
International collaboration has been central to the evolution of Taiwan’s HTA system. With sustained support and exchange through global networks such as HTAi and the International Network of Agencies for Health Technology Assessment (INAHTA), Taiwan has strengthened its methodological capacity and policy impact. Over the past decade, Taiwan has actively contributed to international discussions by sharing practical experience and learning from peers. Through participation in HTAi activities, including the 2023 Asia Policy Forum, Taiwan presented its approaches to adaptive pathways and reimbursement of new medical technologies, contributing to regional dialogue on balancing timely access with evidentiary uncertainty. These collaborations have supported the maturation of Taiwan’s HTA system and enhanced its role in helping the government expand access to effective and sustainable healthcare for the population (17).
Establishment of the Center for Health Policy and Technology Assessment
A key institutional milestone was reached on 27 December 2023, with the establishment of the Center for Health Policy and Technology Assessment (CHPTA) under the NHIA to strengthen evidence-based decision-making in Taiwan. According to the NHIA, the CHPTA functions as a national think tank that integrates HTA, payment reform research, and policy evaluation to support long-term NHI sustainability (18).
CHPTA’s mandate covers three core functions: (i) scientific assessment of medical technologies, RWE, and population outcomes; (ii) evaluation of health policies and payment mechanisms, including novel reimbursement approaches; and (iii) policy advice to support NHI strategy and system sustainability. Building on these functions, CHPTA advances HTA methods, strengthens evidence-based decision-making, supports temporary reimbursement and MEAs, integrates RWD and precision medicine into life cycle HTA, and lays the groundwork for a future independent national HTA institution. Together, these roles reinforce Taiwan’s commitment to evidence-informed policymaking and international HTA collaboration (1 8).
Conclusion
Over the past 15 years, Taiwan has developed an HTA system to support evidence-based and sustainable decision-making under the NHI. Initially focused on new drug assessment, the system has gradually expanded to include novel access pathways, RWE generation, precision medicine evaluation, and systematic health technology reassessment. Recent reforms reflect ongoing efforts to balance timely access to new medical technologies with long-term affordability through phased implementation. The increasing use of RWD and formal reassessment processes suggests a gradual transition toward a learning health system. Taiwan’s experience may offer relevant insights for countries developing HTA systems within constrained fiscal and administrative contexts.
Acknowledgments
The authors thank the Ministry of Health and Welfare (MOHW) and National Health Insurance Administration (NHIA) for financial support.
Competing interests
The authors declare none.

 Open access
Open access