



Impact statement
Sub-Saharan Africa also hosts the largest population of refugees, at 5.4 million, renowned for being among the most vulnerable to suicide, and concurrently comprises 48 of the 108 low- and middle-income countries that registered the highest suicide rates in 2021. This is evidence of the need to implement more suicide prevention efforts across Africa, one of which is the promotion of adaptive coping for all refugees with a history of suicidal ideation or attempts. Suicide follows episodes of suicidal ideation and attempts, which, if poorly or maladaptively coped with, allow progression to suicide. Thus, coping mechanisms, which are behaviors or thoughts adopted to manage stressful conditions that can be external or internal, are significant for suicide prevention. However, the assessment of coping mechanisms, while extensively conducted before, has not included refugees, especially those with a history of suicide attempts. This is also true in Uganda, which hosts Africa’s largest refugee population, with a substantial suicide rate, which might proliferate even more if the transition from a suicide attempt to suicide is not prevented through education on how to cope adaptively with the consequences of a suicide attempt. We believe that this study is among the first to assess coping mechanisms adopted following a suicide attempt in a refugee context, and it could be significant for mental health and psychosocial support programs, particularly if published in the Cambridge Prisms journal and is widely accessed. Consequently, the findings might indicate a new angle that can be taken by MHPSS programs in Uganda and other host countries in their efforts to curb suicide in humanitarian settings. Even better, international organizations such as UNHCR, the Danish Refugee Council, and the Jesuit Refugee Service might also base their MHPSS programming models on the findings, including a component for promoting adaptive coping.
Introduction
A suicide occurs every minute (World Health Organization [WHO], 2025), making it a significant public health challenge that warrants more attention than it currently receives. Moreover, the global suicide rate has not decreased significantly over the past 20 years; during that period (between 2000 and 2021), the rate decreased by 35%, translating to approximately 1.7% per year. The smallest reduction occurred between 2022 and 2023 (Ritchie, Reference Ritchie2026), when the rate remained almost stationary. A mean suicide reduction rate of 1.7% per year will not be sufficient to achieve indicator 3.4.2 (33% reduction in the suicide rate by 2030 compared with 2015) of target 3.4 (reduction of premature mortality from non-communicable diseases) (WHO, 2026). Previous evidence indicates that the age-standardized suicide rate decreased from 9.0 per 100,000 people in 2019 to only 8.9 per 100,000 people in 2021 (International Association for Suicide Prevention [IASP], 2022), a difference of only 0.1%. Regionally, most suicide deaths occur in Eastern Europe (19.2 deaths per 100,000), followed by Southern Sub-Saharan Africa (16.1 per 100,000), and Central Sub-Saharan Africa (14.4 per 100,000) (Weaver et al., 2025). Sub-Saharan Africa reported the highest suicide mortality in 2021 and hence significantly contributes to the global suicide burden. The fact that Sub-Saharan Africa comprises 48 of the 108 (44%) countries in the low- and middle-income country categorization also implies that it significantly contributes to the reported 547,500 annual cases of suicide registered in those countries. Given the social stigma and cultural concerns that lead to concealment, the number of suicide cases may be higher than previously reported (Dattani et al., Reference Dattani, Rodés-Guirao, Ritchie, Roser and Ortiz-Ospina2023). Another alarming fact is that sub-Saharan Africa is home to the world’s second-largest population, estimated at 1.54 billion people (World Population Review, 2026). It is also host to the largest population of refugees, at 5.4 million, renowned for being among the most vulnerable to suicide (Cogo et al., Reference Cogo, Murray, Villanueva, Hamel, Garner, Senior and Henschke2022; Bevione et al., Reference Bevione, Panero, Abbate-Daga, Cossu, Carta and Preti2024). This is further evidence for the implementation of more suicide prevention efforts in Africa, which can take several routes. Among the most important yet usually sidelined of those is the promotion of adaptive coping for all refugees with a history of suicidal ideation or attempts. This is premised on evidence that suicide follows episodes of suicidal ideation and attempts (Weissman et al., Reference Weissman, Stapper, Valmadrid, Appelbaum and Daskalakis2026), which, if poorly or maladaptively coped with (using emotion-based coping), can allow progression to suicide. Coping mechanisms refer to thoughts, perceptions, emotions and behaviors that are adopted by a given individual to reduce the effects or manage internal or external stressful conditions or situations (Folkman and Moskowitz, Reference Folkman and Moskowitz2004; Ruvalcaba et al., Reference Ruvalcaba, Kim, Ndaba, Cele, Swana, Bosire and Moolla2023; Algorani and Gupta, Reference Algorani and Gupta2023). Some authors (Cooper et al., Reference Cooper, Katona, Orrell and Livingston2006) have categorized coping mechanisms into problem-focused (adaptive) and emotion-focused (maladaptive) mechanisms. Problem-focused coping involves active adoption of activities that aim at directly tackling the problem/stressor. Emotion-focused coping, on the other hand, involves the use of emotional support, religion, avoidance, and humor to try to reduce the effects of the stressor, without necessarily removing the stressor (Baloran, Reference Baloran2020; Nurunnabi et al., Reference Nurunnabi, Hossain, Chinna, Sundarasen, Khoshaim, Kamaludin, Baloch, Sukayt and Shan2020; Savitsky et al., Reference Savitsky, Findling, Ereli and Hendel2020; Garcini et al., Reference Garcini, Rosenfeld, Kneese, Bondurant and Kanzler2022). In essence, emotional coping following a suicide attempt does not enable one to address the explanatory cause of the previous suicide attempt, but rather lets it remain prominent, to the extent of causing further suicidal ideation. That is why it is called maladaptive coping, since it does not allow for growth of adaptive capacity to deal with the previous stressor and prevent its progressive effect of suicidal ideation and inclination toward another potentially successful suicide attempt (Garg et al., Reference Garg, Chauhan, Singh and Bansal2022; Okechukwu et al., Reference Okechukwu, Ogba, Nwufo, Ogba, Onyekachi, Nwanosike and Onyishi2022). This denotes the significance of promoting the adoption of adaptive coping mechanisms among all refugees with a suicide attempt history, especially in countries like Uganda, which hosts Africa’s largest refugee population. Besides hosting such a large refugee population, the country has perennially registered high suicide rates, especially in Northern Uganda (Athumani, Reference Athumani2021; UNHCR, 2023; UNHCR, 2025). However, the promotion of coping mechanisms requires that evidence is generated indicating the status of coping among refugees with suicide attempt history. But, despite the extensiveness of studies on refugees and their suicidal behaviors, even in Uganda (e.g., Kizza et al., Reference Kizza, Knizek, Kinyanda and Hjelmeland2012; Athumani, Reference Athumani2021; Bukuluki et al., Reference Bukuluki, Wandiembe, Kisaakye, Besigwa and Kasirye2021), there were barely any that assessed coping mechanisms adopted following a suicide attempt. This study was conducted to assess the coping mechanisms adopted following suicidal ideation and suicide attempts among refugees in humanitarian settings in Northern Uganda.
Methodology
Overview of study methodology
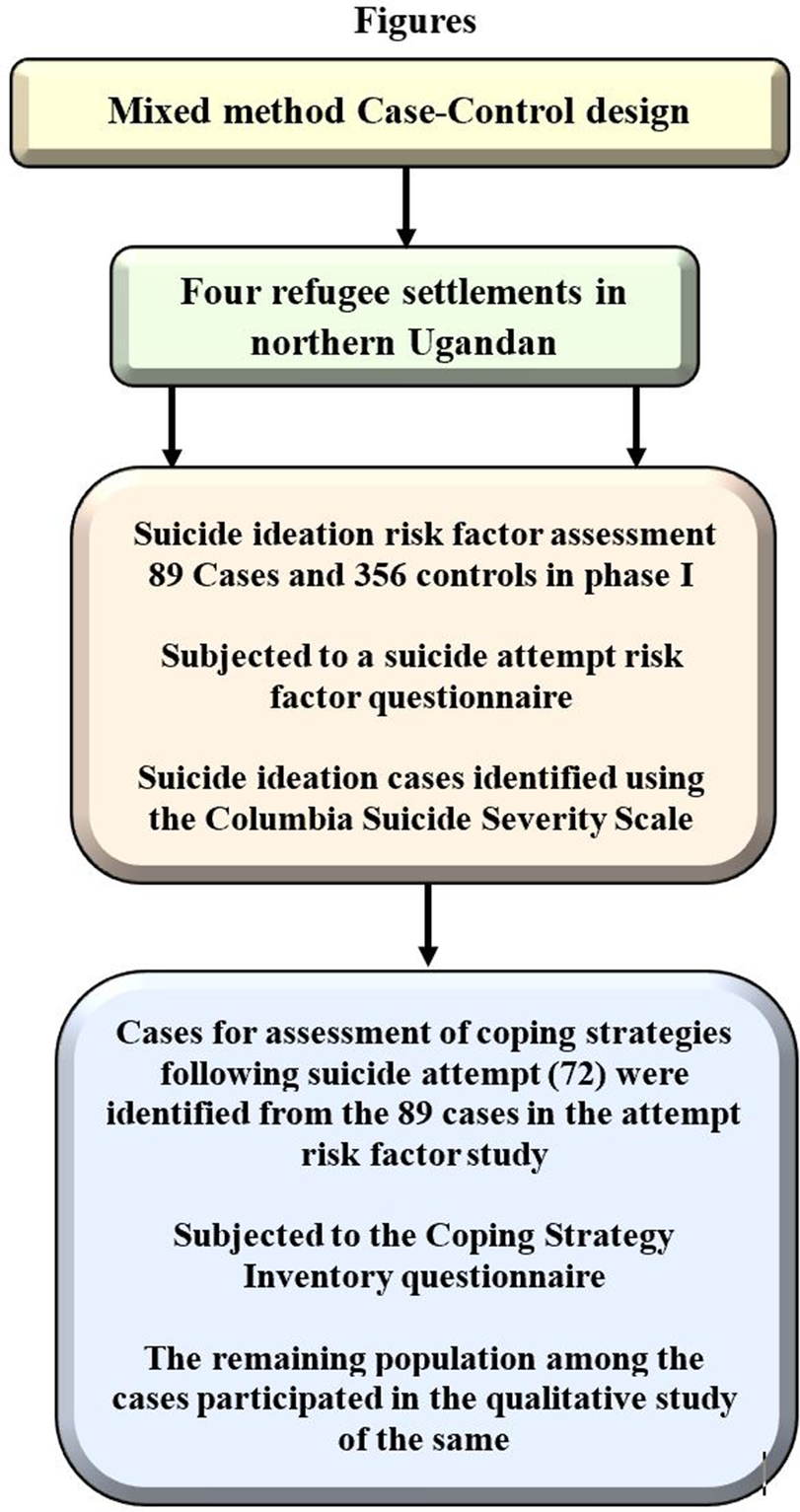
This study is a sequel to a mixed-method case–control study that was conducted to assess the risk factors and coping mechanisms adopted following suicidal ideation and attempts among refugees in four refugee settlements in the northwest Nile, Uganda (Rhino camp, BidiBidi, Palorinya, and Nyumanzi refugee settlements). Initially, activities to collect data for the assessment of suicide attempt risk factors were mounted. Each of the four settlements was stratified by zone, allowing for a simple random sampling of villages and systematic random sampling of households within each village (Figure 1). Quantitatively, 89 cases and 356 controls of suicide attempts were identified and studied for the risk factor assessment with the help of the Columbia Suicide Severity Scale, which has already demonstrated high reliability in screening for suicidal behaviors (Posner et al., Reference Posner, Brown, Stanley, Brent, Yershova, Oquendo, Currier, Melvin, Greenhill, Shen and Mann2011; Nam et al., Reference Nam, Um, Jeong, Rodriguez and Lardier2024). Thus, in the current study on coping following a suicide attempt, 89 suicide attempt cases were the population size used to compute the number of refugees required. This calculation, performed using the Krejcie and Morgan formula, yielded 72 suicide attempts that were subjected to the Coping Strategy Inventory questionnaire for quantitative coping strategy assessment (Figure 1). Some of the remaining cases that did not participate in the quantitative assessment of the coping strategy for suicidal ideation were purposively sampled to participate in the qualitative segment of the study.
Overview of study methodological approach.

Figure 1. Long description
The flowchart consists of four sequential boxes connected by downward-pointing arrows.
1. The top box is yellow and labeled Mixed method Case-Control design.
2. An arrow points down to a light green box labeled Four refugee settlements in northern Ugandan.
3. Two arrows point down to a large beige box describing Phase I. It contains three points: Suicide ideation risk factor assessment 89 Cases and 356 controls in phase I; Subjected to a suicide attempt risk factor questionnaire; and Suicide ideation cases identified using the Columbia Suicide Severity Scale.
4. A final arrow points down to a large light blue box detailing the assessment of coping strategies. It contains three points: Cases for assessment of coping strategies following suicide attempt 72 were identified from the 89 cases in the attempt risk factor study; Subjected to the Coping Strategy Inventory questionnaire; and The remaining population among the cases participated in the qualitative study of the same.
Study design and area
This study adopted a concurrent mixed-method design, characterized by the collection of both quantitative and qualitative data, albeit not in a sequence. The quantitative component of this study involved the assessment of coping mechanisms among 72 refugees with a history of suicide attempts. The qualitative component involved exploring the coping mechanisms adopted by the 17 cases not included in the quantitative assessment. The qualitative data were collected using a phenomenological approach, since coping mechanisms are lived experiences of persons with a history of attempted suicide (Giorgi, Reference Giorgi1985; Boss et al., Reference Boss, Dahl, Kaplan, Sprenkle and Moon1996; Bassett, Reference Bassett and Bassett2004). This design was used to conduct a study across four refugee settlements in Northern Uganda, where South Sudanese refugees settled. They included Imvepi, Parolinya, Bidi Bidi, and Rhino Camp refugee settlements, all of which registered more than 70% of suicide attempt cases that were reported between January 2023 and August 2023 in Uganda (UNHCR, 2023). These settlements were chosen as study areas because while refugees in Uganda have been reported to register a high prevalence of suicide, most of those cases are contextual to refugee settlements in Northern Uganda (UNHCR, 2020; Athumani, Reference Athumani2021; UNHCR, 2023).
Study participants
The study population consisted of adult *refugees of South Sudanese origin who had a history of suicide attempt, as earlier identified in the suicide attempt risk factor study. Those refugees participated in both the quantitative and qualitative arms of the study, wherein they responded to an exploration of coping mechanisms for suicide attempts. The study included adult refugees who declared (verbatim) willingness to have a suicide history assessed during the consent process. Only such refugees were included in this study because those who were free to divulge accurate information about their attempt history ensured the study’s high credibility and reliability. Qualitative study participants who were uncomfortable with their responses being digitally recorded were excluded because voice recording is the only way to validate and comprehensively capture qualitative study responses (Lee, Reference Lee2004; Al-Yateem, Reference Al-Yateem2012; Nordstrom, Reference Nordstrom2015).
Sample size determination
For the quantitative study, the required sample size was determined using the formula by Krejcie and Morgan (Reference Krejcie and Morgan1970), as the population size (N) of suicide ideation cases had already been established. The formula is given by s = X2N P (1 − P)/d2 (N − 1) + X2 P (1 − P), which was true when s = required sample size; X 2 = the table value of chi-square for one degree of freedom at the desired confidence level (3.841), N is the population size = number of refugees who had suicidal ideations, as identified in the ideation risk factor study = 96; P = the population proportion (assumed to be 0.50, as this would provide the maximum sample size); and d is the degree of accuracy expressed as a proportion (0.05). This yielded a sample size of 72 refugees with a history of suicide attempts. However, in a qualitative study, data saturation was used to determine the number of respondents who were to be included in the qualitative exploration of coping mechanisms, as per Guest (Reference Guest, Bunce and Johnson2006). In-depth interviews were conducted until data saturation was reached, as indicated by response overlap (Morse, Reference Morse1995; Guest et al., Reference Guest, Bunce and Johnson2006; Morse, Reference Morse2015). With this approach, saturation occurred at the 14th in-depth interview.
Sampling procedures
Given that this assessment required 72 participants for the quantitative assessment of coping mechanisms adopted following a suicide attempt, across the four settlements, consecutive sampling was used to sample the respondents. Consecutive sampling was used because the sample size of refugees with a history of suicide attempt required in this study was about 80% of the population size earlier predetermined, implying that the use of random sampling was impractical. Random sampling, despite being renowned for reducing sampling bias, involves probabilistic elimination and requires larger population sizes to be used. Consecutive sampling is the least biased of all the qualitative sampling methods (Polit and Beck, Reference Polit and Beck2017) and does not involve probability sampling, meaning that it could allow for the obtainment of the required sample size, with respect to the small population size available. Consecutive sampling involves the inclusion of any respondent for as long as they meet the inclusion criteria of the study (Polit and Beck, Reference Polit and Beck2017). The sampling was applied following the establishment of the number of refugees that was required from each settlement, by proportioning the sample size (72) according to the population size of the cases in each settlement.
For the qualitative study, whose available population size was predetermined as being 17, purposive sampling was used to sample three participants per refugee settlement. This strategy was used to ensure that at the point of data saturation, at least all four refugee settlements would be represented. It happened that data saturation was not reached until the time when 12 in-depth interviews had been held across the four settlements (first round of interviews). Therefore, another round was conducted, in which data saturation was reached when three interviews were conducted in Rhino camp, making a total of 15 interviews that had been conducted by the time data saturation set in.
Data collection techniques
Structured interviews were conducted to collect data for the quantitative assessment of coping mechanisms. These interviews were ideal for the quantitative study because the adapted Coping Strategies Inventory (CSI) was structured, requiring administration in a standardized manner. Qualitative data, on the other hand, were collected using in-depth interviews, which are conducted one-on-one and are well suited to exploring sensitive issues, such as coping mechanisms following suicidal ideation. The principal investigator moderated all in-depth interviews to increase the likelihood of accurately detecting data saturation. Responses from structured interviews were captured using a structured questionnaire comprising items from the CSI, which contains 71 items (Speyer et al., Reference Speyer, Morgenstern, Hayashino, Kerr, Rayner, Robinson and Pisoni2016). The CSI identifies emotion-focused engagement, emotion-focused disengagement, problem-focused engagement, and problem-focused disengagement. The CSI has demonstrated acceptable internal consistency (α = 0.56–0.80) in countries such as the United Kingdom (UK), the United States (US), Australia, Sweden, and Germany, making it suitable for assessing coping strategies. The CSI tool was translated into Juba-Arabic and Dinka, two of the most widely spoken and understood languages among South Sudanese refugees in Uganda. Qualitative data generated from in-depth interviews were captured using an in-depth interview guide and were also audio-recorded.
Measurement of coping strategies and suicide attempt
The participants in this study had earlier been screened for suicide attempt history in the attempt risk factor study, wherein Columbia Severity Rating Scale (C-SRS) was used. The C-SSRS has already demonstrated high reliability in screening for suicidal behaviors (Posner et al., Reference Posner, Brown, Stanley, Brent, Yershova, Oquendo, Currier, Melvin, Greenhill, Shen and Mann2011; Nam et al., Reference Nam, Um, Jeong, Rodriguez and Lardier2024). Posner et al. (Reference Posner, Brown, Stanley, Brent, Yershova, Oquendo, Currier, Melvin, Greenhill, Shen and Mann2011) reported that the C-SSRS tool showed very high divergent and convergent validity with other suicidal behavior screening scales, along with a very high level of specificity and sensitivity. Nam et al. (Reference Nam, Um, Jeong, Rodriguez and Lardier2024) recently concluded that the Cronbach’s alpha of the C-SSRS ranged from 0.74 to 0.89, proving its reliability.
Coping strategies were measured using 72 indicators as prescribed in the CSI tool, each of which had attributes that represented adaptive or maladaptive coping inclinations. Adaptive coping represented problem-focused coping practice adoption, while maladaptive coping represented more emotion-focused coping practice adoption. The responses per question were Not at all, A Little, Somewhat, Much, and Very much, which were scored 1, 2, 3, 4, and 5, respectively. However, that scoring was for problem-focused assertions; for emotion-focused assertions, the scoring was reversed, as Not at all = 5, A Little = 4, Somewhat = 3, Much = 2, Very much = 1. The reverse scoring was premised on the fact that emotion-focused coping is discouraged as it breeds further depression and increases progression to suicide volition. For problem-focused assertions, the responses which showed satisfactory coping frequency were “much and very much,” while for emotion-focused coping, the responses which showed satisfactory frequency of adopting a given coping activity were “Not at all” and “A Little.” In essence, the minimum score for a refugee to be deemed as having adaptively coped was 288 (4 × 72), with the maximum score being 360 (5 × 72), implying that the refugee had to score between 288 and 360 to be considered as being an adaptive coper of suicide attempt history.
Statistical and qualitative data analysis
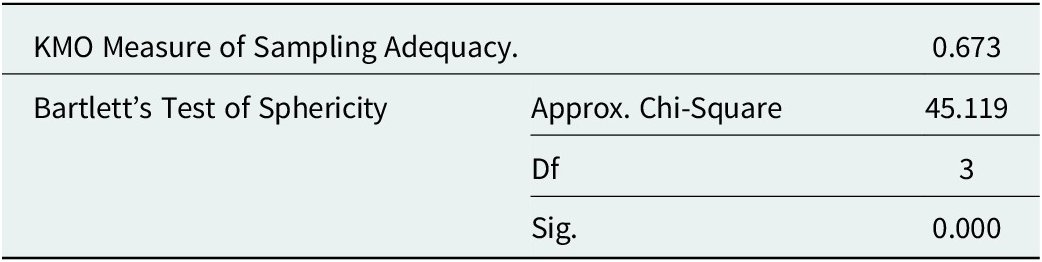
Quantitative data management and analyses were performed using SPSS version 25. Descriptive analysis was performed using frequency distributions, followed by principal component and cluster analyses. Principal component and cluster analyses were performed to identify the most important components defining coping mechanisms, given that the questionnaires used to assess both variables had numerous items that needed to be dimensionally reduced. To determine whether the data on coping mechanisms, as obtained from the assessment with the CSI, met the assumptions for analysis using principal component analysis (PCA), the Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity were run first. This test, as shown below, turned out to be statistically significant (p < 0.05), with the KMO measure of Sampling Adequacy being above the acceptable limit of 0.6, at 0.673. This confirmed that the data were suitable for dimensionality reduction, and it was hence subjected to PCA.

Table 1. Long description
The table contains two main sections of statistical data. The first row shows the K M O Measure of Sampling Adequacy with a value of 0.673. The second section covers Bartlett’s Test of Sphericity, which includes three specific metrics: an Approx. Chi-Square value of 45.119, degrees of freedom (D f) of 3, and a significance (Sig.) value of 0.000.
PCA was performed using the varimax method with orthogonal rotation (Jolliffe, Reference Jolliffe and Cadima2016). All variables with eigenvalues exceeding one were considered principal components. However, to ascertain the distribution of the 11 principal components that were identified from PCA, cluster sampling was performed using K-means cluster analysis (Lloyd, Reference Lloyd1957; MacQueen, Reference MacQueen, Le Cam and Neyman1967), with which the number of clusters required was set at two (2), with 10 maximum iterations. The distance between cases and cluster centers was set using the simple Euclidean distance. This resulted in the establishment of the largest cluster of refugees with a given set of coping mechanisms (previously identified as principal components). Each principal component was then cross-tabulated with the cluster to determine the distribution of the principal components in the largest cluster and the coping mechanisms adopted by the majority of respondents who had ideated or attempted suicide. These characteristics in the largest cluster defined the coping mechanisms among the studied suicidal ideation cases.
Qualitative data generated from the exploration of coping mechanisms were analyzed using Braun and Clarke’s (Reference Braun and Clarke2006) thematic analysis approach. The analysis was conducted through a six-phase process, which was preceded by transcription of recorded responses to text by the principal investigator. This was then followed by familiarization with the data in Phase 1, generation of initial codes in Phase 2, search for themes in Phase 3, review of themes in Phase 4, and definition and naming of themes in Phase 5. For each theme generated, the principal investigator conducted a detailed analysis of the quotes therein, identifying the story each theme told (Braun and Clarke, Reference Braun and Clarke2006) and adding a narrative. This was done to show what each theme was about and how it was interlinked with other themes and the study.
Results
Sociodemographic characteristics of respondents in the quantitative assessment of coping mechanisms adopted following a suicide attempt
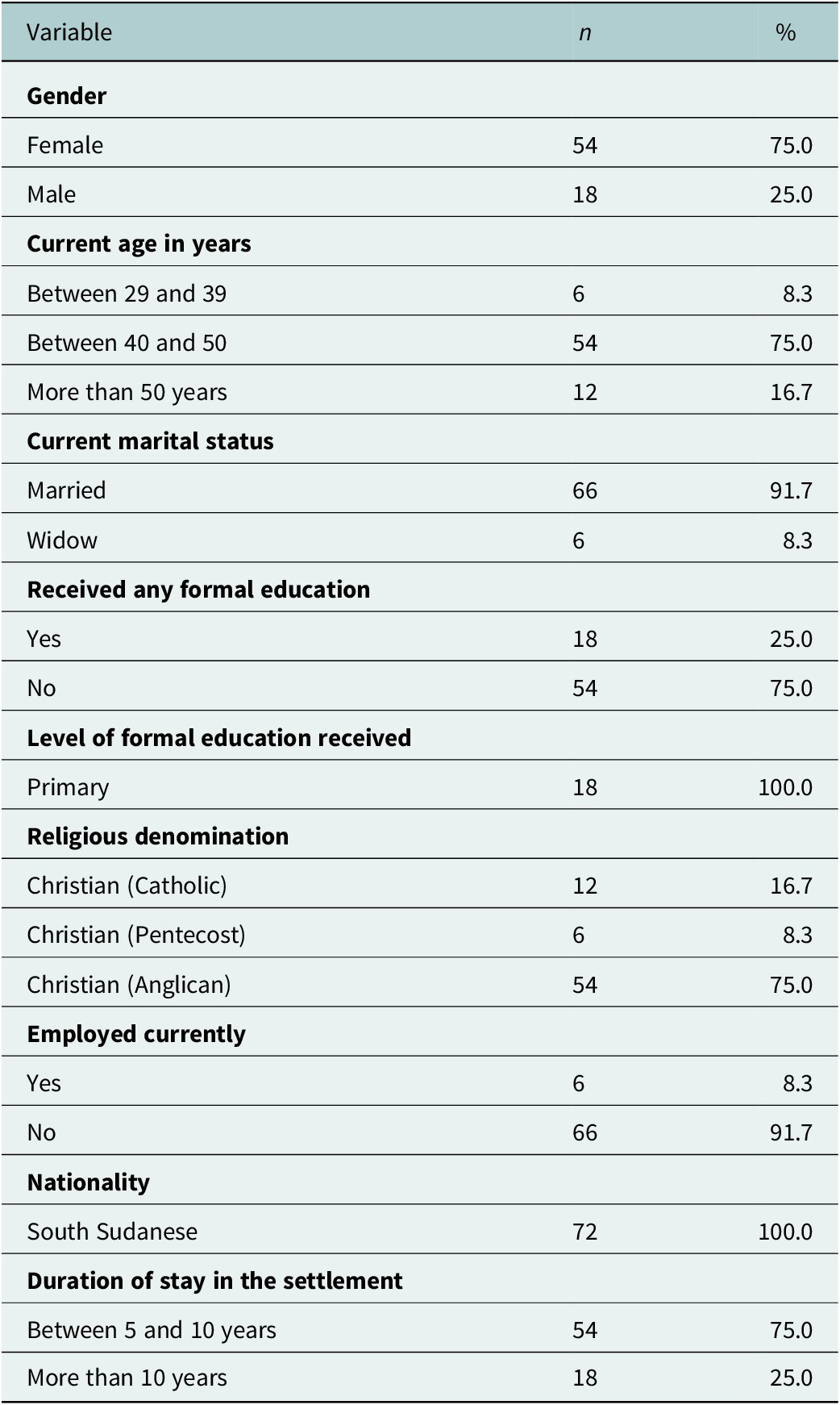
Table 2 shows that three-quarters 54 (75.0%) of the refugees were female and were aged between 40 and 50 years (54, 75.0%). Almost all refugees were married (66, 91.7%), although the majority had not received any formal education (54, 75.0%). Among those who had received formal education, 18 (100.0%) had completed primary education. Most of the refugees were Christian (Anglican), 54 (75.0%); not currently employed, 66 (91.7%); and had stayed in their respective settlements for 5 to 10 years, 54 (75.0%).
Sociodemographic characteristics of participants in the assessment of coping strategies following suicide attempt

Table 2. Long description
The table consists of three columns: Variable, n, and percent.
* Gender: Female 54 (75.0 percent), Male 18 (25.0 percent).
* Current age in years: Between 29 and 39 is 6 (8.3 percent), Between 40 and 50 is 54 (75.0 percent), More than 50 years is 12 (16.7 percent).
* Current marital status: Married 66 (91.7 percent), Widow 6 (8.3 percent).
* Received any formal education: Yes 18 (25.0 percent), No 54 (75.0 percent).
* Level of formal education received: Primary 18 (100.0 percent).
* Religious denomination: Christian Catholic 12 (16.7 percent), Christian Pentecost 6 (8.3 percent), Christian Anglican 54 (75.0 percent).
* Employed currently: Yes 6 (8.3 percent), No 66 (91.7 percent).
* Nationality: South Sudanese 72 (100.0 percent).
* Duration of stay in the settlement: Between 5 and 10 years is 54 (75.0 percent), More than 10 years is 18 (25.0 percent).
Classification of coping mechanisms in the assessment of coping mechanisms adopted following a suicide attempt
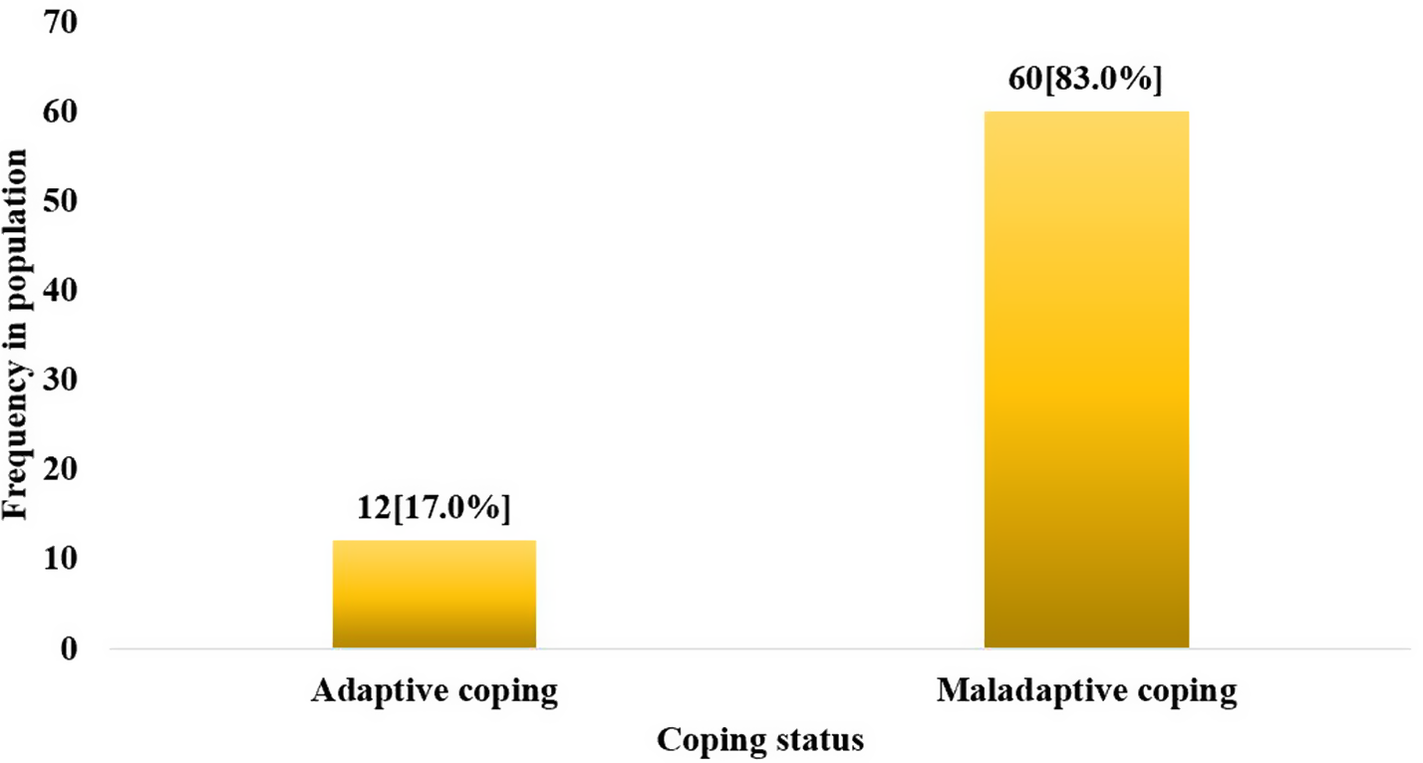
Figure 2 shows that the assessment of coping mechanisms using the coping strategy inventory revealed that less than a quarter (17%, n = 12) of refugees who had attempted suicide coped adaptively.
Distribution of coping status among suicide survivors.
![Bar chart showing Frequency in population by Coping status. Adaptive coping has a frequency of 12 [17.0%] and Maladaptive coping has a significantly higher frequency of 60 [83.0%].](https://static.cambridge.org/binary/version/id/urn:cambridge.org:id:binary:20260709034737174-0319:S2054425126102635:S2054425126102635_fig2.png?pub-status=live)
Identification of the most important coping mechanisms (PCA)
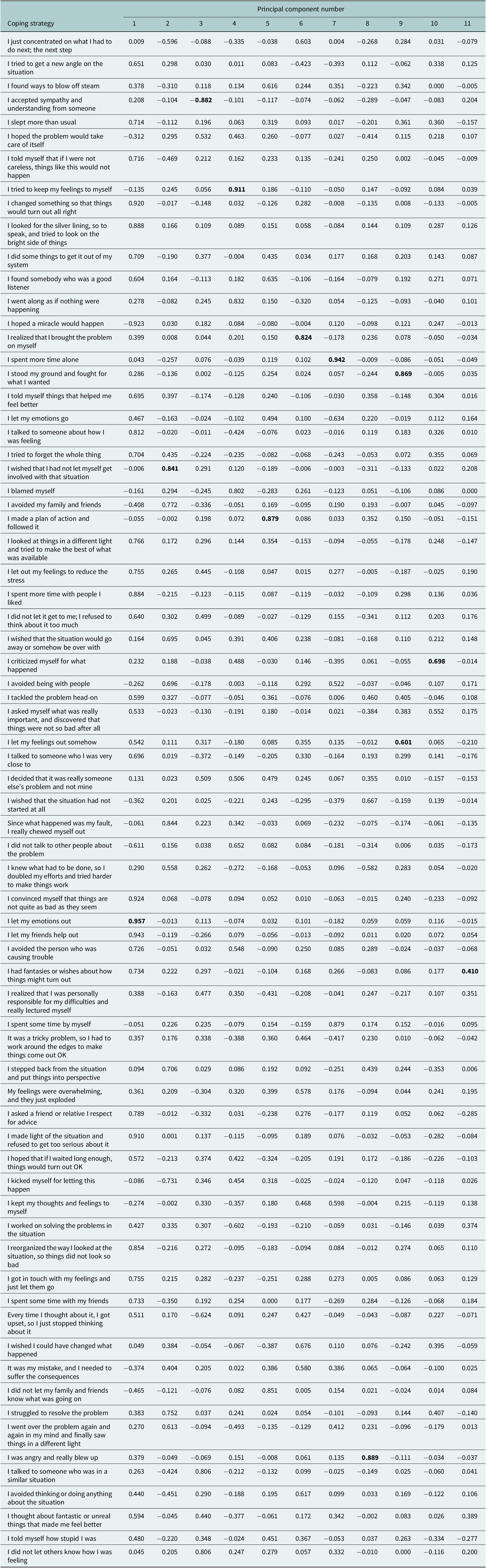
PCA was performed on the 71 coping strategies reported by the refugees to determine which of those were most correlated and, hence, could indicate a definitive picture of how refugees cope after a suicide attempt. This process resulted in the identification of 11 principal components (Table 3), that is, those with eigenvalues of 1 and above. These components were letting their emotions out (coef. 0.957), wishing that they had not let themselves become involved in the situation (coef. 0.841), accepting sympathy and understanding from others (coef. −0.882), trying to maintain feelings of the self (coef. 0.911), making a plan of action, and following it (coef. 0.879), indicating that one had brought problems to oneself (coef. 0.824), and spending more time alone (coef. 0.942), being angry or really blowing up (coef. 0.889), standing ground, and fighting what one wants (coef. 0.869), criticizing oneself for what has happened (coef. 0.698), and having fantasies or wishes about how things might turn out (coef. 0.410).
Rotated matrix from the PCA of coping strategies adapted following a suicide attempt

Table 3. Long description
The table presents a rotated matrix from a Principal Component Analysis P C A. The header row lists Principal component numbers from 1 to 11. The first column lists 66 specific coping strategy statements. Each row contains numerical factor loadings for that strategy across the 11 components.
Key high-loading values (bolded in the source) include:
* I accepted sympathy and understanding from someone: -0.882 in component 3.
* I tried to keep my feelings to myself: 0.911 in component 4.
* I realized that I brought the problem on myself: 0.824 in component 6.
* I spent more time alone: 0.942 in component 7.
* I stood my ground and fought for what I wanted: 0.869 in component 9.
* I wished that I had not let myself get involved with that situation: 0.841 in component 2.
* I made a plan of action and followed it: 0.879 in component 5.
* I criticized myself for what happened: 0.698 in component 10.
* I let my feelings out somehow: 0.601 in component 9.
* I was angry and really blew up: 0.889 in component 8.
* I let my emotions out: 0.957 in component 1.
* I had fantasies or wishes about how things might turn out: 0.410 in component 11.
Values range from approximately -0.923 to 0.957, representing the strength and direction of the relationship between each strategy and the underlying principal components.
The bold values indicate the highest coeficient in each of the principal component columns, indicating the adjacent variable that was identified as the textual descriptor of the given component.
Determination of the largest cluster to which the respondents belonged
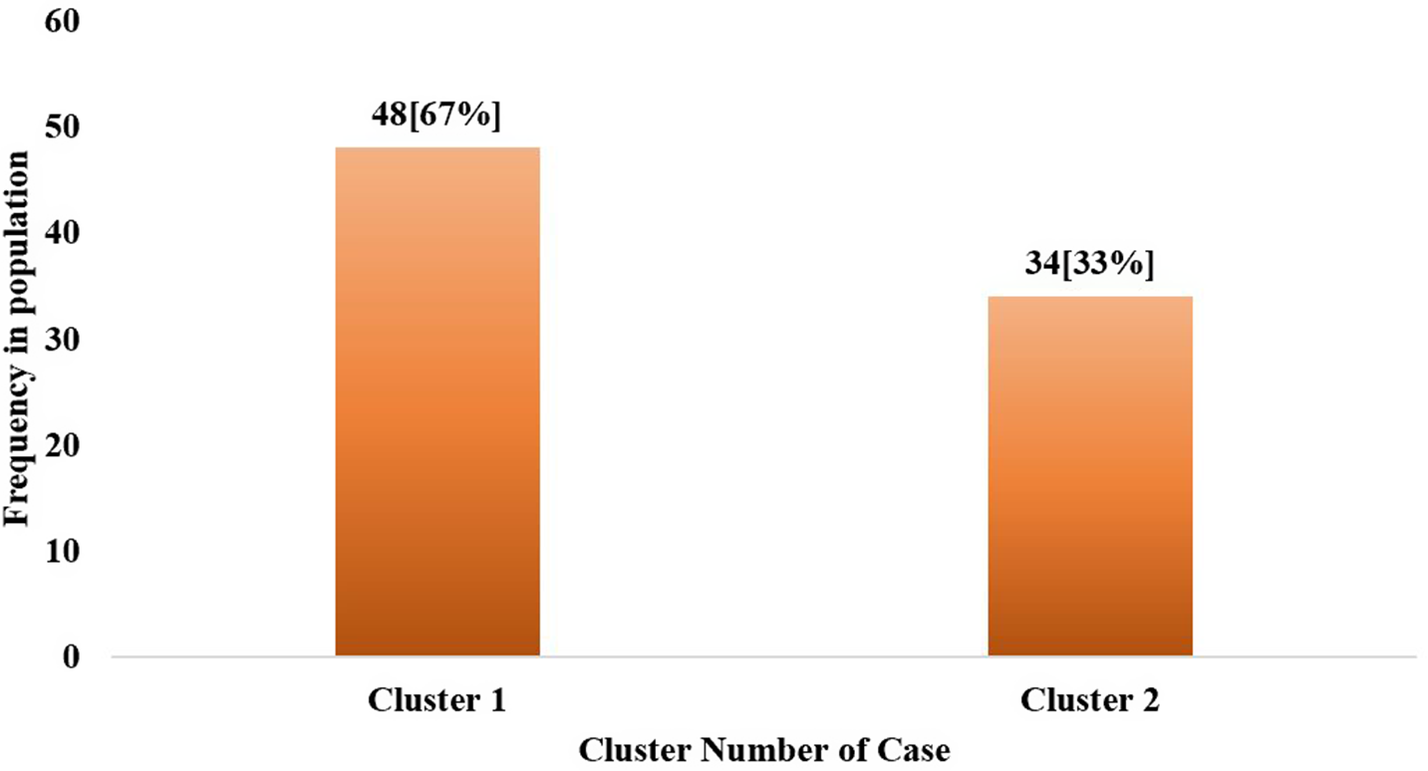
Using the K-means clustering approach, cluster analysis (Figure 3) revealed that refugees who participated in the quantitative assessment of coping mechanisms adopted after a suicide attempt belonged to two clusters. The largest of these clusters was Cluster 1, comprising 48 (67%) of them (Figure 3). Therefore, this study aimed to determine the coping mechanisms adopted by refugees in the largest cluster. It is the coping mechanism in the largest cluster that was taken as representative of most refugees and, hence, the most definitive.
Cluster membership of the 10 principal components.

Determination of coping mechanisms in the largest cluster of refugees
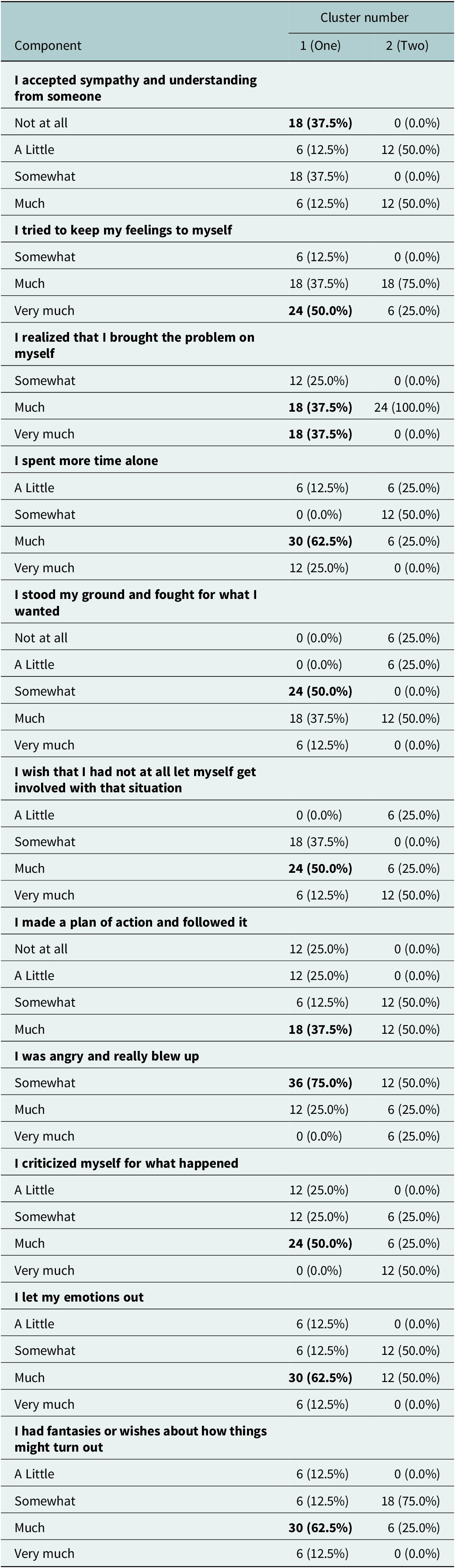
To determine the coping mechanisms adopted by most refugees, a cross-tabulation of each of the 11 principal components identified with the two clusters was conducted (Table 4). The findings in Table 3 show that in the largest cluster of refugees who had attempted suicide, the largest proportion coped by rarely accepting sympathy and understanding from (18 [37.5%]), frequently trying to keep their feelings to themselves (24 [50.0%]), realizing that they brought the problem to themselves (18 [37.5%]), spending more time alone (30 [62.5%]), standing on their ground and fighting for what they wanted (24 [50.0%]), wishing that they had not allowed themselves to get involved with the situation (24 [50.0%]), and making a plan to action followed by (18 [37.5%]). Many of them were angry and really blowing up (36 [75.0%]), criticizing themselves for what happened 24 (50.0%), letting their emotions out (30 [62.5%]), and having fantasies or wishes about how things might turn out (30 [62.5%]).
Disaggregation of the 11 principal components into the largest cluster

Table 4. Long description
The table consists of three columns: Component, Cluster number 1 (One), and Cluster number 2 (Two).
1. I accepted sympathy and understanding from someone: Cluster 1 peaks at Not at all and Somewhat (both 18, 37.5 percent). Cluster 2 peaks at A Little and Much (both 12, 50.0 percent).
2. I tried to keep my feelings to myself: Cluster 1 peaks at Very much (24, 50.0 percent). Cluster 2 peaks at Much (18, 75.0 percent).
3. I realized that I brought the problem on myself: Cluster 1 is split between Much and Very much (both 18, 37.5 percent). Cluster 2 is 100 percent at Much (24).
4. I spent more time alone: Cluster 1 peaks at Much (30, 62.5 percent). Cluster 2 peaks at Somewhat (12, 50.0 percent).
5. I stood my ground and fought for what I wanted: Cluster 1 peaks at Somewhat (24, 50.0 percent). Cluster 2 peaks at Much (12, 50.0 percent).
6. I wish that I had not at all let myself get involved with that situation: Cluster 1 peaks at Much (24, 50.0 percent). Cluster 2 peaks at Very much (12, 50.0 percent).
7. I made a plan of action and followed it: Cluster 1 peaks at Much (18, 37.5 percent). Cluster 2 is split between Somewhat and Much (both 12, 50.0 percent).
8. I was angry and really blew up: Cluster 1 peaks at Somewhat (36, 75.0 percent). Cluster 2 peaks at Somewhat (12, 50.0 percent).
9. I criticized myself for what happened: Cluster 1 peaks at Much (24, 50.0 percent). Cluster 2 peaks at Very much (12, 50.0 percent).
10. I let my emotions out: Cluster 1 peaks at Much (30, 62.5 percent). Cluster 2 is split between Somewhat and Much (both 12, 50.0 percent).
11. I had fantasies or wishes about how things might turn out: Cluster 1 peaks at Much (30, 62.5 percent). Cluster 2 peaks at Somewhat (18, 75.0 percent).
The bold values indicate the highest coeficient in each of the principal component columns, indicating the adjacent variable that was identified as the textual descriptor of the given component.
Qualitative findings from the assessment of coping mechanisms adopted following a suicide attempt
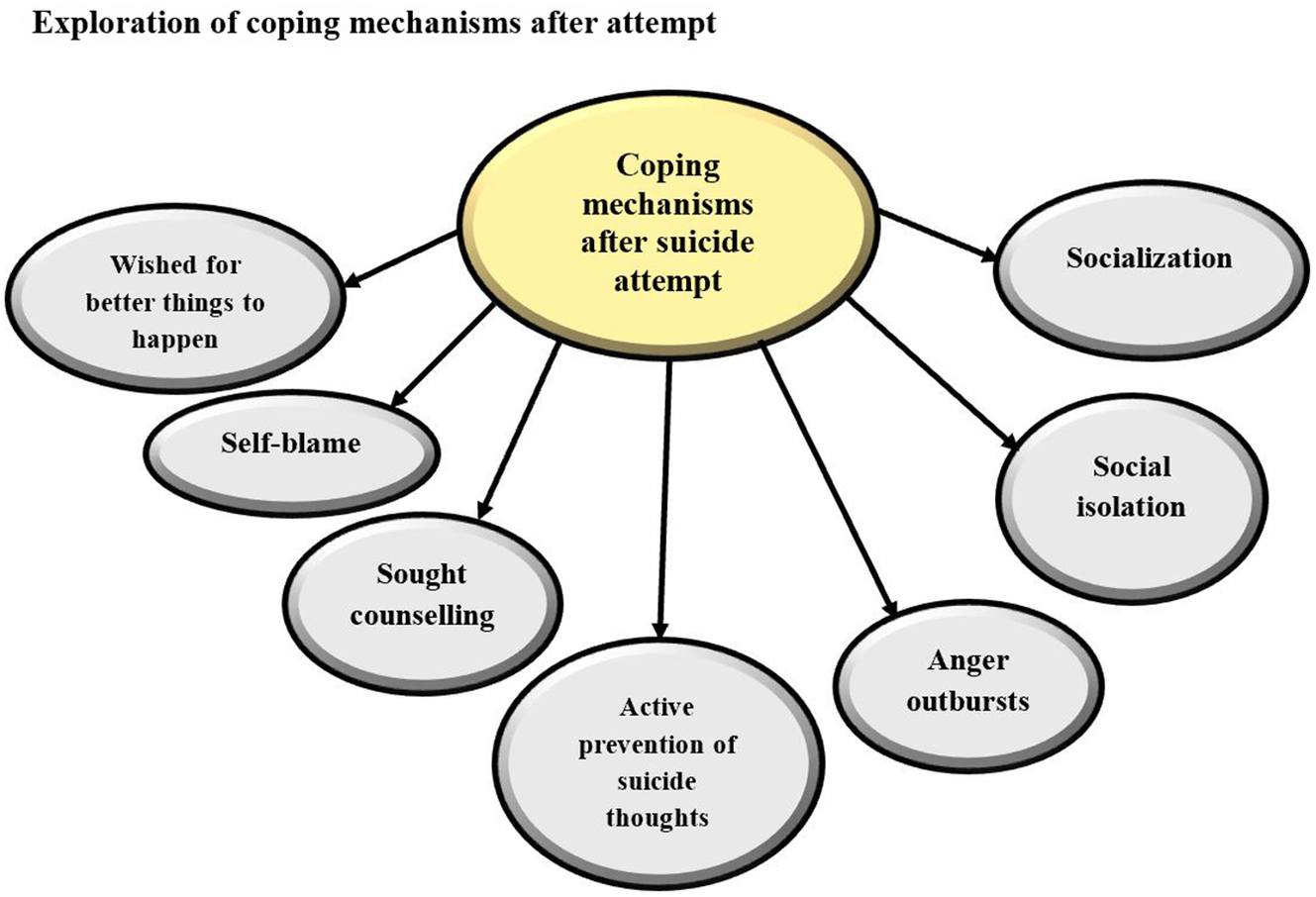
Figure 4 shows the findings from the exploration of coping mechanisms adopted following a suicide attempt, revealing four key themes: self-isolation, self-blame, active prevention of suicidal thoughts, and anger outbursts. Nonetheless, a few participants mentioned that they had adopted more coping mechanisms following their suicide attempts, as discussed below.
Thematic tree showing emergent themes from the analysis of coping mechanism adopted after a suicide attempt.

Self-isolation
Many refugees tried to cope with their suicide attempts by isolating themselves from others. Most of them noted that they realized that being around people had made them internalize stigma and could exacerbate their ideations and inclinations to attempt suicide.
………………I have kept to myself since; I do not like being around people because some of them got to know that I almost killed myself, and they stigmatize me, so I decided that I should not be around them, since it would make me get angry or more depressed. Male, In-depth interview 7, Parolinya.
Some participants mentioned that staying away from other people in the community enabled them to heal, especially toxic people who had contributed to their suicidal nature.
……………To a great extent, staying away from people is what has enabled me to get along since I attempted suicide. One of the things that made me attempt to take my life was being around toxic people, so I have decided to isolate myself whenever I can, for peace of mind. Female, in-depth interview 12, Rhino camp.
Self-blame
Self-blame was a rampantly mentioned coping mechanism that nearly all participants adopted. Most seemed to judge themselves for the suicide attempt they had made earlier, and decided to face any consequences henceforth.
……………you see, I am the one who attempted suicide, so I have learnt to blame myself, and blame me, so that I feel guilty and try to heal, so that I do not attempt to commit suicide again. Male, In-depth interview 8, Parolinya.
Active prevention of suicidal thoughts
Many participants also mentioned that they chose to prevent their suicidal thoughts actively. Some went ahead and mentioned the things they did to ensure that they practically or behaviorally tackled suicidal ideation and attempts. The practices they employed included cessation of alcohol consumption, seeking counseling, and many other factors that predisposed them to suicidality.
………….For me, if it had not been for practically fighting suicidal thoughts and trying to engage the things that caused my suicidal ideation and attempt last time, I would have killed myself by now. I was an alcoholic last time, thinking that the alcohol would enable me to reduce the depression, but it got worse, so, to prevent any further bad things from happening, I have chosen to withdraw from alcohol consumption, and other things that I think might predispose me to being suicidal again. Male, In-depth interview 9, Nyumanzi refugee settlement.
Anger outbursts and venting
Similar to coping mechanisms for suicidal ideation, many refugees mentioned that they coped by letting out their anger and quarreling most of the time. One of the refugees with such an approach to coping mentioned that letting out their anger made them feel better, and ideated or planned to attempt suicide less.
……………I have coped by being free to do what I want, especially by getting angry and showing that I am actually angry, through letting my voice be heard and quarreling. It actually sounds weird, but letting out my feelings has made me cope with the fact that I attempted suicide; it could be that the last time, I was keeping all my emotions in, and it made me get more depressed. Female, in-depth interview 6, BidiBidi refugee settlement.
Discussion
In summary, this study found that less than a quarter (17%) of the suicide attempts coped adaptively. Most refugees coped emotionally by rarely accepting sympathy and understanding from 18 (37.5%), frequently trying to keep their feelings at themselves 24 (50.0%), self-blame 24 (50.0%), self-isolation 30 (62.5%), making a plan to action, followed by 18 (37.5%), bursting out in anger and other emotions 36 (75.0%), and having fantasies or wishes about how things might turn out 30 (62.5%). These coping mechanisms were congruent with those identified in the qualitative exploration. For illustration, the 11 quantitatively identified coping mechanisms were categorizable into Isolation (frequently trying to keep their feelings to themselves, realizing that they brought the problem to themselves, and spending more time alone), Actively preventing attempt causes (standing on their ground and fighting for what they wanted), and Self-blame (wishing that they had not allowed themselves to get involved with the situation, and making a plan to action followed by, and having fantasies or wishes about how things might turn out). This was significantly congruent with the five qualitatively identified emergent coping mechanisms including self-isolation, self-blame, active prevention of suicidal thoughts, and anger outbursts. Therefore, this confirms the imperativeness of assessing coping mechanisms with a pragmatic research philosophy lens, as opposed to only qualitatively. That is because a pragmatic approach provides a bidirectional complementary value to quantitative and qualitative findings.
According to the transactional model of stress and coping, a person who faces a stressor, such as suicidal ideation and attempt, adopts coping mechanisms by default in an attempt to minimize the impact of that stressor. This was true among refugees who had ideations and attempted suicide, which is consistent with the findings of Al-Dajani et al. (Reference Al-Dajani, Horwitz and Czyz2022), Liang et al. (Reference Liang, Kõlves, Lew, De Leo, Yuan, Abu Talib and Jia2020), Stanley et al. (Reference Stanley, Martínez-Alés, Gratch, Rizk, Galfalvy, Choo and Mann2021), Cao et al. (Reference Cao, Wei, Zhu, Duan, Geng, Hong, Jiang, Zhao and Zhu2020), Cai et al. (Reference Cai, Tu, Ma, Chen, Fu, Jiang and Zhuang2020), and Muller et al. (Reference Muller, Hafstad, Himmels, Smedslund, Flottorp, Stensland, Stroobants, Van Velde and Vist2020), Parcesepe et al. (Reference Parcesepe, Filiatreau, Gomez, Ebasone, Dzudie, Pence, Wainberg, Yotebieng, Anastos, Pefura-Yone, Nsame, Ajeh and Nash2023). Thus, as expected, refugees who had attempted suicide endeavored to minimize the consequences of their actions and, perhaps, avoid transition to graver outcomes such as suicide. However, worryingly, the majority of them maladaptively coped; the findings showed that less than a quarter (17%, n = 12) of refugees who had attempted suicide coped adaptively. This finding implies that only about two in every ten refugees who ideate or attempt suicide adopt problem-focused coping strategies or coping strategies that are proactive and involve focus on minimizing the effect of the stressor. In other words, most refugees in Northern Uganda adopt emotion-focused coping following a suicide attempt, characterized by stressor avoidance, which exacerbates the stressor and puts them at risk of transitioning to a suicide attempt. Although very few studies have assessed coping after suicide attempts among refugees, generic studies have confirmed a high prevalence of emotion-focused or maladaptive coping among persons with a history of suicide attempts (Konkan et al., Reference Konkan, Erkuş, Güçlü, Şenormanci, Aydin, Ülgen and Sungur2014; Sun et al., Reference Sun, Li, Wang and Li2021; Ge and Tolmie, Reference Ge and Tolmie2025). Coping was performed by self-blaming, self-isolation, and bursting out in anger, which are typical of emotion-focused coping (Nurunnabi et al., Reference Nurunnabi, Hossain, Chinna, Sundarasen, Khoshaim, Kamaludin, Baloch, Sukayt and Shan2020; Savitsky et al., Reference Savitsky, Findling, Ereli and Hendel2020; Garcini et al., Reference Garcini, Rosenfeld, Kneese, Bondurant and Kanzler2022) and are usually associated with subsequent substance abuse and impulsive behaviors (Jahan and Burgess, Reference Jahan and Burgess2023; Otache et al., Reference Otache, Ezenwosu, Ossai, Nwobi, Abah and Uzochukwu2023). This is because, with emotion-focused coping, one simply sits back and presumes that the ideations will somehow subside on their own; they become more introverted, which gives room for intense loneliness, which only makes suicidal ideation and urges for suicide attempts more severe (Hernandez-Vasquez et al., Reference Hernandez-Vasquez, Vargas-Fernandez, Daaz-Seijas, Tapia-Lapez and Bendezu-Quispe2019; Zhang et al., Reference Zhang, Lei, Song, Lu, Duan and Prochaska2019; Bračič et al., Reference Bračič, Roškar and Kocjan2019). Recent evidence also indicates that without good emotion regulation, suicidal ideation persists, increasing the risk of suicide attempts (Stetsiv et al., Reference Stetsiv, Wilks and Carpenter2026), which can progress to suicide. One of the key outcomes or cardinal signs of emotion-focused coping is self-isolation, the outcome of which includes more intense distress (D’Amico et al., Reference D’Amico, Grazzi, Bussone, Curone, Di Fiore, Usai, Leonardi, Giovannetti, Schiavolin and Raggi2015; Fried et al., Reference Fried, Prohaska, Burholt, Burns, Golden, Hawkley, Lawlor, Leavey, Lubben, O’Sullivan, Perissinotto, van Tilburg, Tully and Victor2020; Lui et al., Reference Lui, Young, Ebbert, Rosedahl and Philpot2020), which are renowned precursors of psychological distress and suicidal ideation. Longstanding loneliness is associated with a greater likelihood of engaging in impulsive behaviors, such as substance use, as a secondary coping strategy (Rhew et al., Reference Rhew, Cadigan and Lee2021; Otache et al., Reference Otache, Ezenwosu, Ossai, Nwobi, Abah and Uzochukwu2023; Walsh and Schlauch, Reference Walsh and Schlauch2024). This further aggravates suicidal ideation severity, guaranteeing an effective transition from a suicide attempt. Only a few refugees were protected from these outcomes, and they included those who spent time with friends, though, on their own admission, they did so infrequently. The findings of the quantitative assessment of coping strategies largely concurred with those from the qualitative exploration. With the widespread maladaptive coping approaches used by suicidal refugees, it comes as no surprise that the number of suicide cases registered in Uganda coincided with the number of suicide attempt cases. The most recent analysis of suicide incidents among refugees and nationals in Uganda indicated that 27% of all suicide attempts by 2025 resulted in suicide (United Nations High Commissioner for Refugees, 2025). More concerning is the fact that there were nearly twice as many repeat suicide attempts (45) as first-time suicide attempts (25) among refugees (United Nations High Commissioner for Refugees, 2025), which is symbolic of maladaptive coping among refugees with a history of suicide attempts.
Conclusion/implications
Most of the refugees (8 in every 10) with a history of attempted suicide maladaptively coped with the aftermath of their mental health challenges, implying that they are at a high risk of repeated suicide attempts and potentially suicide, given that they are not coping with the cause of the problem. The largest proportion of them cope by rarely accepting sympathy and understanding from someone frequently trying to keep their feelings to themselves, realizing that they brought the problem to themselves, spending more time alone, standing on their ground and fighting for what they wanted, wishing that they had not let themselves get involved with the situation, and making a plan to act and following it, being angry and really blowing up criticizing themselves for what happened, letting their emotions out, and having fantasies or wishes about how things might turn out. It is almost certain that without enabling more adaptive coping for all refugees with a history of suicide attempt, other psychosocial support interventions may be less effective. Thus, available mental health and psychosocial support interventions and those planned in the future, targeting refugees with an attempt history, ought to emphasize the need for education and support aligned toward enabling the adoption of more problem-focused coping. Such refugees should be dissuaded from blaming themselves for their predicament and self-isolation, and encouraged to address the root cause by seeking support and means to minimize triggers.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10263.
Data availability statement
The data on which the findings in this study are based are available upon reasonable request from the principal investigator.
Acknowledgements
I am sincerely grateful to my supervisors at Gent and Makerere universities, namely Wouter Vanderplasschen and Rosco Kasujja, and Benjamin Alipanga, respectively, for all the guidance they accorded in the conduct of this study. I will be forever grateful to the refugees in Parolinya, Bidibidi, Imvepi, and Rhino camp refugee settlements for allowing us to participate in this study unconditionally. Special thanks go to refugees with a history of suicide attempt, who agreed to be involved in a second series of interviews about their coping mechanisms; the views you provided are invaluable.
Author contribution
M.M. conceptualized the study, wrote the manuscript, collected and analyzed data, and reviewed the manuscript. G.P. analyzed data, supervised the study, and reviewed the manuscript. R.J. analyzed data, supervised the study, and reviewed the manuscript. B.A. analyzed data, supervised the study, and reviewed the manuscript. I.D. analyzed data, supervised the study, and reviewed the manuscript. W.V. wrote the manuscript, analyzed data, supervised the study, and reviewed the manuscript.
Financial support
The study received some financial support from Bijzonder Onderzoeksfonds(BOF), the Special Research Fund.
Competing interests
The authors declare no conflict of interest whatsoever.
Ethics statement
Approval to conduct this study, among refugees settled in refugee settlements within northern Uganda, and permission to access them, subsequently, was obtained from the institutional review boards at Makerere University School of Health Sciences Research Ethics Committee (Appendix S), under number MAKSHSREC-2024-729 on the 20/08/2024, and the Uganda National Council of Science and Technology, under number SS3111ES on the 8/10/2024. Permission to conduct the study within refugee settlements of interest was obtained from the Prime Minister’s Office in Uganda. Permission granted by the Office of the Prime Minister was used to obtain final clearance from the commandant of each sampled refugee settlement. Each refugee was first given details about the study, including its purpose, procedures, risks, benefits, and the ethics observed, such as confidentiality and voluntary participation. Consent was obtained from each refugee before inclusion in the study. Anonymity, privacy, confidentiality, and voluntary participation were maintained in accordance with the Declaration (World Medical Association, 2001).

 Open access
Open access
Comments
Dear Editor
Sub-Saharan Africa reported the highest suicide mortality in 2021 (Yan et al., 2024). It significantly contributed to the deaths that make low- and middle-income countries (LMICs) the most affected, registering 73% of the global suicide burden. Sub-Saharan Africa is also host to the largest population of refugees, at 5.4 million, renowned for being among the most vulnerable to suicide (Bevione et al., 2024; Cogo et al., 2022). This is further evidence for the need to implement more suicide prevention efforts in Africa, which can take several routes, perhaps the most important yet usually sidelined being the promotion of adaptive coping for all refugees with a history of suicidal ideation or attempts. This is premised on evidence that suicide follows episodes of suicidal ideation and attempts (Weissman et al., 2026), which, if poorly or maladaptively coped with, allow progression to suicide. Thus, coping mechanisms, which are behaviors or thoughts adopted to manage stressful conditions that can be external or internal (Folkman & Moskowitz, 2004), are significant in suicide prevention. However, the assessment of coping mechanisms, while extensively done before, has not included refugees, especially those with a history of suicide attempt. That is also true in Uganda, which hosts Africa’s largest refugee population, with quite a substantial suicide rate (UNHCR, 2025), which might proliferate even more if the transition from suicide attempt to suicide is not prevented through education on how to cope with the consequences of a suicide attempt adaptively. We believe that this study is among the first that have assessed coping mechanisms adopted following a suicide attempt, in a refugee context, and it could be significant for mental health and psychosocial support programmers, particularly if published in the Cambridge Prisms: Global Mental Health Journal, and widely accessed. Our assumption is that going forward, programmers and implementers of mental health and psychosocial support programs may, as informed by the findings in this study, include coping mechanism augmentation interventions in their routine support activities for suicidal persons.