


Introduction
Breastfeeding self-efficacy is a mother’s confidence in her ability to breastfeed her infant rather than her actual practice that improves breastfeeding outcomes (Dennis, Reference Dennis1999; McGovern et al., Reference McGovern, O’Toole, Laws, Skinner, McAuliffe and O’Reilly2024).
Globally, over two-thirds of child deaths in the first year of life are often related to poor exclusive breastfeeding practices (UNICEF, 2017). Around 41% of global deaths due to poor breastfeeding practices were from Sub-Saharan Africa (Woldie, Reference Woldie2014; Saqib and Qazi, Reference Saqib and Qazi2018). In Ethiopia, 270,000 malnutrition-related deaths among children under the age of five were due to a lack of exclusive breastfeeding (Jarso et al., Reference Jarso, Workicho and Alemseged2015). The evidence revealed that approximately 21.9% of women were introduced to additional foods before six months (Kasahun et al., Reference Kasahun, Wako, Gebere and Neima2017). To tackle the low breastfeeding rates, breastfeeding self-efficacy (BFSE) should be an important determinant of breastfeeding initiation, duration, and patterns (Kingston et al., Reference Kingston, Dennis and Sword2007). According to the WHO, breastfeeding self-efficacy is modifiable, has positive results on exclusive breastfeeding (WHO & UNICEF, 2017), and reduces the number of women who stop breastfeeding, especially in the first few months (Borona et al., Reference Borona, Gualdana, Maga, Del Bo, Arrigoni, Brigante, Daniele, Caruso and Magon2023; McGovern et al., Reference McGovern, O’Toole, Laws, Skinner, McAuliffe and O’Reilly2024).
Across the world, the magnitude of breastfeeding self-efficacy ranged from 38.8% to 90.2% (Mirghafourvand et al., Reference Mirghafourvand, Malakouti, Mohammad-Alizadeh-Charandabi and Faridvand2018; Hemiyanty et al., Reference Hemiyanty, Wandira and Suwendro2022; Vaithilingan and Johnson, Reference Vaithilingan and Johnson2023). The evidence indicated that high levels of breastfeeding self-efficacy increased breastfeeding initiation and duration, improved problem-solving, and reduced stress and anxiety around breastfeeding, promoting maternal well-being (Awaliyah et al., Reference Awaliyah, Rachmawati and Rahmah2019; Brani et al., Reference Brani, Mrvoljak-Theodoropoulou, Pechlivani, Gourounti, Iliadou, Palaska, Antsaklis, Drakakis and Dagla2024).
Low self-efficacy can precipitate the early cessation of breastfeeding, with mothers perceiving breastfeeding as painful and challenging, leading to negative experiences and feelings of guilt (De Sá Vieira Abuchaim et al., Reference De Sá Vieira Abuchaim, Caldeira, Di Lucca, Varela and Silva2016; Titaley et al., Reference Titaley, Dibley, Ariawan, Mu’asyaroh, Alam, Damayanti, Do, Ferguson, Htet, Li, Sutrisna and Fahmida2021). According to the studies, more than half of women with children under 6 months have low breastfeeding self-efficacy (Economou et al., Reference Economou, Kolokotroni, Paphiti-Demetriou, Kouta, Lambrinou, Hadjigeorgiou, Hadjiona and Middleton2021; Titaley et al., Reference Titaley, Dibley, Ariawan, Mu’asyaroh, Alam, Damayanti, Do, Ferguson, Htet, Li, Sutrisna and Fahmida2021). A mother who had low breastfeeding confidence in their ability was 2 to 3 times more likely to stop breastfeeding earlier than the recommended period (Awaliyah et al., Reference Awaliyah, Rachmawati and Rahmah2019).
The various studies showed that education level, working outside the home, receiving breastfeeding advice, young maternal age, income, number of pregnancies, lack of breastfeeding experience, breastfeeding problems, cesarean section delivery, and social and partner support were associated with breastfeeding self-efficacy (Schwartz et al., Reference Schwartz, D’Arcy, Gillespie, Bobo, Longeway and Foxman2002; Taveras et al., Reference Taveras, Capra, Braveman, Jensvold, Escobar and Lieu2003; O’Brien et al.,, Reference O’Brien, Buikstra and Hegney2008; Pelt et al., Reference Pelt, Massar and Eem2020; Topuz et al., Reference Topuz, Duman, Uysal and Öcalan2021).
The evidence revealed that the lack of breastfeeding self-efficacy has several consequences, such as early cessation of breastfeeding, reduced lactation, motivation & low mother-to-baby bonding, reduced mother’s mood, and increased level of her anxiety and interference with the cognitive abilities, negative effects on maternal feeling and performance (Glassman et al., Reference Glassman, McKearney, Saslaw and Sirota2014; De Sá Vieira Abuchaim et al., Reference De Sá Vieira Abuchaim, Caldeira, Di Lucca, Varela and Silva2016; Maleki-Saghooni et al., Reference Maleki-Saghooni, Barez, Moeindarbari and Karimi2017).
Moreover, breastfeeding self-efficacy is crucial to preventing early weaning, which leads to infant morbidity and mortality, particularly in developing countries that do not have adequate medical equipment and resources (Hinic, Reference Hinic2016; Awaliyah et al., Reference Awaliyah, Rachmawati and Rahmah2019). Furthermore, the evidence revealed that promoting breastfeeding requires addressing prevalent myths, knowledge gaps, and awareness of certain aspects of breastfeeding (Kumari and Jain, Reference Kumari and Jain2024). It is a critical factor influencing whether mothers initiate breastfeeding, persist through challenges, and achieve their breastfeeding goals (Zeng et al., Reference Zeng, Zheng, Wang, Liu, Liu, Lin and Guo2024). Again, as far as searching capacity is concerned, the principal investigator could not find evidence that the study was conducted in a study setting on breastfeeding self-efficacy and its determinant factors among postnatal mothers. Therefore, this study aimed to assess breastfeeding self-efficacy status and determinant factors among postnatal women in Gurage Zone public hospitals, Central Ethiopia.
Methods and materials
Study area and period
In central Ethiopia, Gurage is an administrative Zone. Wolkite Town is the capital of the Gurage Zone. The distance between the Gurage zone and Addis Ababa, the capital of Ethiopia, is 153 km southwest. The Gurage zone has 1,279,646 residents, overall, 657,568 of whom are women and 622078 of whom are men, according to the 2007 national household census. (Ethiopia, Reference Ethiopia2007) It has 14 districts and 5 town administrations. The Zone has four hospitals and 72 health centers. All hospitals provided maternal health care services to mothers, including antenatal care, labor and delivery, and postpartum care. The study was conducted from February 15 to March 15, 2025.
Study design
A multicenter facility-based cross-sectional study with a concurrent mixed approach was employed from February 15 to March 15, 2025.
Source population
All postnatal women in Gurage Zone public hospitals, Central Ethiopia.
Study population
All postnatal women in public hospitals during the data collection period.
Eligibility criteria
Inclusion criteria
All postnatal women who received postnatal care and were willing to participate during the data collection period.
Exclusion criteria
Postnatal women who have severe medical illness, breast complications, complementary feeding, and have known mental illness were excluded.
Sample size determinations
The sample size was determined using a single population proportion formula by considering a population proportion of 50% with a 95% confidence interval and a 0.05 margin of error.
 ${ n}={({ Z}{\alpha }/{2}){2}{ p}({1}-{ p}) \over { d}{ 2}}$
${ n}={({ Z}{\alpha }/{2}){2}{ p}({1}-{ p}) \over { d}{ 2}}$
With the assumptions of 95% CI, estimated breastfeeding self-efficacy status among postnatal women at 50% (P = 0.5), the formula yields 384. To calculate the final sample size, use the single population proportion formula: n = 1.96.2 (0.5) (1–0.5)/(0.05)2 = 384.16 ≈ 384. Adding a 10% non-response rate leads to a final sample size of 422.
For the qualitative data, a thematic qualitative approach was implemented. A total of four focus group discussions were conducted. Each focus group consisted of six mothers. The qualitative sample size was determined using the principle of data saturation.
Sampling techniques and procedures
For quantitative data, four public hospitals were founded in the Gurage Zone. All four hospitals were included. The average number of clients who were followed up on postnatal care at each facility over two months was approximately 860 (N). The number of respondents in each hospital was proportionally allocated based on the average number of mothers who received maternity care at each hospital. Following this, systematic random sampling was used to select the study participants in each hospital, as K = N/n = 860/422 = two (2). The interview was conducted after selecting the first respondent randomly by lottery methods from the women who attended the maternity care unit on the first day of data collection, and each respondent corresponding to the skip interval was chosen after that.
For the qualitative component, postnatal mothers were purposively selected from the postnatal unit through maternity healthcare providers to participate. Data were collected through four focus group discussions (FGDs), each consisting of six mothers, to explore in depth individual experiences regarding breastfeeding self-efficacy. Data collection continued until saturation was achieved, and a few additional discussions were conducted to confirm that no new information was emerging from respondents across the focus group discussions. All FGDs were conducted in facility-based venues that were convenient, neutral, and ensured privacy and confidentiality for the participants.
Operational definitions
Exclusive breastfeeding
If a mother feeds her infant exclusively breast milk for the entire 6 months, she should not feed her infant any other liquids or solids other than vitamins, mineral supplements, or medications.
Breastfeeding self-efficacy
Breastfeeding self-efficacy refers to a mother’s confidence in her capacity to breastfeed her baby (Dennis, Reference Dennis1999; McGovern et al., Reference McGovern, O’Toole, Laws, Skinner, McAuliffe and O’Reilly2024).
Perceived social support
refers to an individual’s belief that emotional, informational, and practical help will be available from their social network, such as family, friends, or other significant persons, when needed (Scarapicchia et al., Reference Scarapicchia, Amireault, Faulkner and Sabiston2017).
Study variable
Dependent variable
Breastfeeding self-efficacy status
Independent variables
Sociodemographic characteristics
Maternal age, residence, religion, maternal education status, marital status, occupation, husband’s educational status, husband’s occupation, and income
Obstetrics-relation questions
Parity, ANC follow-up, pregnancy intention, gestational age, number of children, mode of delivery, sex of the current baby
Personal related factors
Perceived social support (friends support, family support, other significant supports), having breastfeeding information, breastfeeding experience, and plan to breastfeed
Data collection tools and measurements
The data collection tool was adapted from similar research on the outcome of interest and used for collecting data (Uyar Hazar and Uzar Akça, Reference Uyar Hazar and Uzar Akça2018; Gizaw et al., Reference Gizaw, Sopory and Morankar2022; Abageda et al., Reference Abageda, Jena and Belachew2024; Brani et al., Reference Brani, Mrvoljak-Theodoropoulou, Pechlivani, Gourounti, Iliadou, Palaska, Antsaklis, Drakakis and Dagla2024). The questionnaire was prepared in an English version. Then, it was translated into the Amharic version and then to the Guragigna language by a language expert. After, it was translated back to the English version to check its consistency. Postpartum mothers’ sociodemographic information, obstetrics-related factors, personal-related factors, and Breastfeeding Self-Efficacy Scale Short Form (BSES-SF) were included in the tool. To ensure reliability and consistency, the tool was checked by a panel of experts, and a reliability test was conducted. The data was collected by trained nine diploma nurses, and four BSc nurses supervised by holding nurses who are fluent in the local language.
Regarding BFSE measurement
Breastfeeding self-efficacy was measured using the Breastfeeding Self-Efficacy Scale Short Form, which was published in different reputable journals (Uyar Hazar and Uzar Akça, Reference Uyar Hazar and Uzar Akça2018; Gizaw et al., Reference Gizaw, Sopory and Morankar2022; Abageda et al., Reference Abageda, Jena and Belachew2024; Brani et al., Reference Brani, Mrvoljak-Theodoropoulou, Pechlivani, Gourounti, Iliadou, Palaska, Antsaklis, Drakakis and Dagla2024). We used the BSES-SF, a 14-item questionnaire with a five-point Likert scale developed to measure breastfeeding confidence in Amharic that was translated from validated English questionnaires from various studies, to assess the mother’s self-efficacy in her ability to breastfeed. All of the items are preceded by the phrase ‘I can always’ and are anchored with a 5-point Likert scale, with one indicating no confidence at all and five indicating very confident.
The scale’s score was calculated by taking the average of all items. A higher total score indicates that the mother is more confident in her ability to breastfeed. All items are presented positively, and scores are summed to produce a range from 14 to 70. In this study, BFSE-SF was operationalized as participants with scores equal to or more than the mean were considered to have high breastfeeding self-efficacy, and those with scores below the mean were considered to have low breastfeeding self-efficacy. A higher total score indicates that the mother is more confident in her ability to breastfeed (Poorshaban et al., Reference Poorshaban, Pakseresht, Khalesi, Kazem and Leili2017; Abageda et al., Reference Abageda, Jena and Belachew2024). In this study, a Cronbach’s α value of BFSE-S is 0.93.
Regarding social support measurement
In this study, perceived social support was assessed using the tool developed by Zimet et al., Reference Zimet, Dahlem, Zimet and Farley1988, the multidimensional perceived social support scale (MSPSS), which consists of 12 items with three subscales: family, friend, and significant others (Zimet et al., Reference Zimet, Dahlem, Zimet and Farley1988). The lowest score that can be obtained from the subscales is 4, and the highest score is 28. For the whole scale, the lowest possible score is 12, and the highest is 84. Based on these scores, perceived social support can be categorized into low, moderate, and high levels. A high score indicates high perceived social support. The original reliability test showed a Cronbach’s α value of 0.88, and in this study, it was 0.89 (Konukbay et al., Reference Konukbay, Öksüz and Guvenc2024).
Qualitative data were collected using FGDs to supplement the quantitative data. The focus group discussion guides were structured into sections covering key thematic areas related to breastfeeding self-efficacy. Each section included open-ended questions with probes to explore participants’ experiences in detail. The FGDs lasted 90 minutes each to explore in detail breastfeeding self-efficacy. Four BSc nurses with prior experience in qualitative data collection conducted the focus group discussions. Each session was audio-recorded after obtaining written informed consent from the participants. The place and time of discussion were selected to be convenient for the study participants. The principal investigator and supervisors selected the participants, and the discussions were conducted until saturation of ideas occurred. The supervisors moderated the discussions, while the data collectors took notes and recorded all the information from the focus group discussions.
Data quality control
To ensure data quality, language experts translated the questionnaire into Amharic and Guragigna. The tool was pre-tested on 21 postpartum mothers at Gubre Health Center before actual data collection to ensure clarity, consistency, cultural relevance, and completeness. Data collectors and the supervisor received two days of training on the study’s objectives, questionnaire clarification, sampling strategy, and data collection process and supervision. The principal investigator and supervisor guided, facilitated, and checked data completeness, ensuring the overall activities were effectively managed throughout the data collection process. Data was coded, entered, and rechecked during data entry into the computer software before analysis. Simple frequencies and a box plot were used to look for missing values and outliers, respectively.
For qualitative data, field notes were taken during the focus group discussions, and a tape recorder was used to support accurate transcription. After each session, the recordings and notes were reviewed to ensure completeness, consistency, and clarity of data. Furthermore, the trustworthiness of the study was ensured following Guba and Lincoln’s criteria (Guba and Lincoln Reference Guba and Lincoln1985). Credibility was enhanced through member checking and triangulation, dependability through an audit trail, confirmability through reflexive notes, and transferability by providing detailed descriptions of the study objectives.
Statistical analysis
After ensuring the questionnaire’s completeness, the data were checked, coded, and entered into the EPI data 4.1 statistical packages before being analyzed with SPSS version 26 software. Binary and multivariate logistic regressions were used to identify the relationships between predictors and outcome, and variables with a p-value of less than 0.25 at a 95% confidence interval were considered for multivariable logistic regression analysis. This approach is widely recommended in the literature to avoid excluding potentially important variables that may not show a strong association in bivariable analysis but could be significant in the multivariable model after adjusting for confounders. An odds ratio with a 95% confidence interval was used to determine the association between dependent and independent variables. Significant associations are defined as p-values <0.05.
Multicollinearity was checked to see the linear correlation among the associated independent variables by using the variance inflation factor (VIF) and standard error. A VIF of >10 or a standard error of >2 was considered suggestive of multicollinearity. For all independent variables, the multicollinearity effect was checked by co-linearity diagnostic statistics via VIF and tolerance test with a maximum value of 1.20 and a minimum value of 80.8%, respectively. In multivariable analysis, the multivariable logistic regression model was used to control the confounders. The Hosmer–Lemeshow goodness-of-fit test was done to check for model fitness with a p-value of 0.775, which indicates the model was fitted. Adjusted Odds Ratio (AOR) with a 95% confidence interval was estimated to demonstrate the strength of the association between the independent variables, after controlling for the effects of confounders. The results were considered statistically significant at a P-value < 0.05.
For qualitative data, thematic analysis approaches were conducted. The audio-taped qualitative data were transcribed verbatim and translated into English. The transcripts were read repeatedly by the principal investigator and research team to gain familiarity with the data and to identify initial patterns. Then, codes or terms were identified and tallied to develop categories, which were later used to establish themes based on the objectives of the study. Proper coding and categorization of data were maintained to ensure the quality of the analysis. To ensure reliability and validity, coding and theme development were independently performed and then compared; discrepancies were discussed and resolved through consensus. Furthermore, findings were presented to sampled participants to confirm that the themes accurately reflected their breastfeeding self-efficacy and its determinants. Audit trails were maintained throughout the analysis to enhance the transparency of the research process. Finally, the findings were triangulated with the quantitative results by comparing survey outcomes with themes emerging from focus group discussions, allowing the study to elaborate, complement, and contextualize the results on breastfeeding self-efficacy.
Results
Among a total sample of 422 study participants, 419 were interviewed and gave a response rate of 99.3%, and the results were presented as follows under subheadings.
Sociodemographic characteristics of the participants
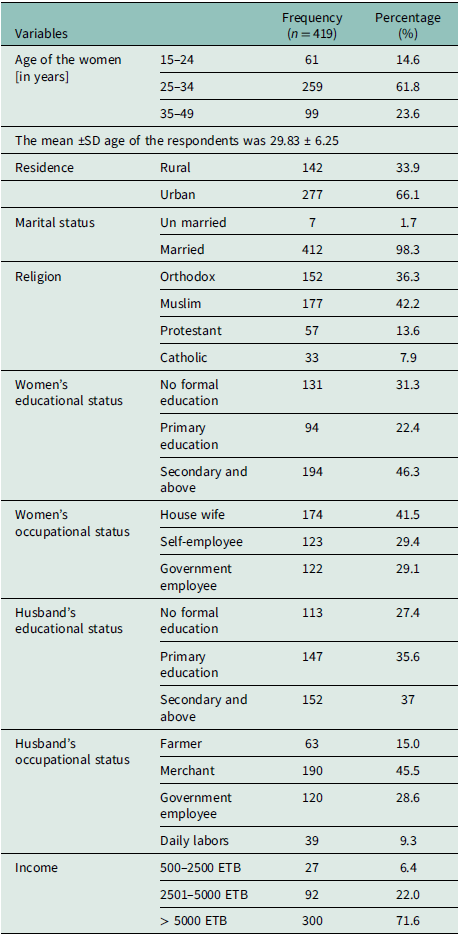
More than half, 259 (61.8%), of the participants were in the age group 25–34 years. The mean age of the respondents was 29.83 (± 6.25 SD) years. Two hundred seventy-seven (66.1%) of the study participants were urban residents. Nearly half of the study participants, 177 (42.2%), were followers of the Muslim religion.
Among the study participants, 412 (98.3%) were married. More than half of the women, 288 (68.7%), attended formal education, and 152 (36.3%) of them reported that their husbands’ educational status was secondary and above. One hundred seventy-four (41.5%) of the women were housewives, and 45.5% of them reported that their husbands’ occupation was merchant (Table 1).
Socio-demographic characteristics of the study participants in the Gurage Zone public hospitals, Central Ethiopia, 2025 (n = 419)

ETB: Ethiopian birr.
Obstetrics characteristics of the participants
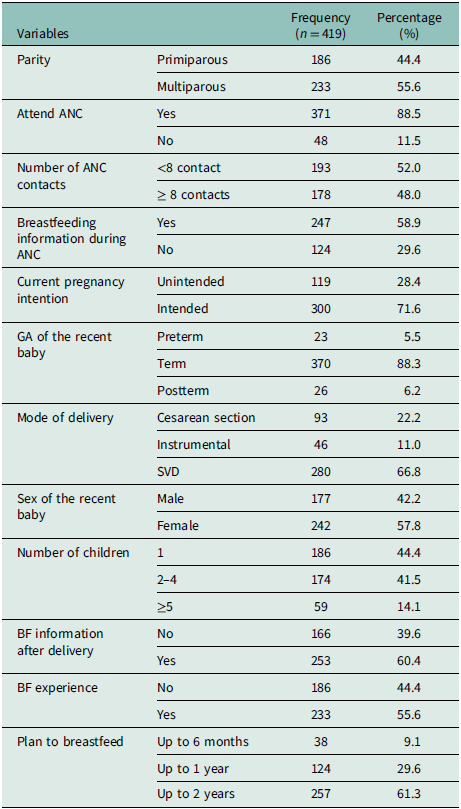
Of the total study participants, 371 (88.5%) attended antenatal care; from these, 178 (48%) women had eight or more antenatal care contacts. In addition, two hundred thirty-three (55.6%) of the study participants were multiparous. Regarding pregnancy intention, 300 (71.6%) had an intended pregnancy. Furthermore, 233 (55.6%) had previous breastfeeding experiences. Moreover, among the total study participants, 257 (61.3%) had a plan to breastfeed their newborn up to 2 years (Table 2).
Obstetrics characteristics of the study participants in the Gurage Zone public hospitals, Central Ethiopia, 2025 (n = 419)

Note: ANC: Antenatal care, BF: Breastfeeding, SVD: Spontaneous Vaginal Delivery, GA: Gestational age.
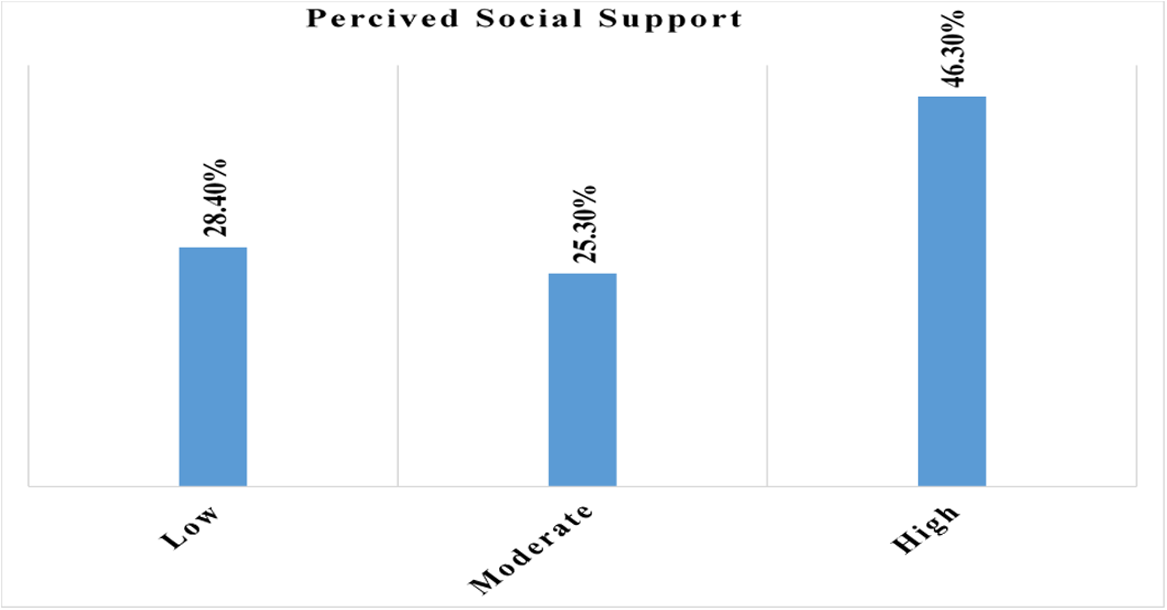
Of 419 study participants, 194 (46.3%) had high perceived social support regarding breastfeeding self-efficacy (Figure 1), and 215 (51.3%) of the study participants had support from their husbands during breastfeeding their babies.
The proportion of perceived social support among postnatal women in Gurage Zone public hospitals, Central Ethiopia, 2025 (n = 419).

Breastfeeding self-efficacy status of the postnatal women
In this study, the overall breastfeeding self-efficacy status was 51.3 % (95% CI: 47, 56) (Figure 2).
The overall breastfeeding self-efficacy status among postnatal women in Gurage Zone public hospitals, Central Ethiopia, 2025 (n = 419).

Qualitative findings regarding breastfeeding self-efficacy status
The qualitative findings from the focus group discussions data revealed three interrelated themes and several subthemes describing how postnatal women and their communities experience breastfeeding self-efficacy. These themes are low breastfeeding self-efficacy among postnatal mothers, determinants undermining breastfeeding confidence, and determinants enhancing breastfeeding confidence.
Low breastfeeding self-efficacy among postnatal mothers
The majority of the discussants reported that their confidence in breastfeeding their babies after birth was not as expected. This shows a lack of understanding of the benefit of confidently breastfeeding their babies, even during challenges.
Primiparous mothers expressed further breastfeeding challenges. First-time mothers often reported low confidence in their ability to breastfeed, particularly when family advice conflicted with health recommendations.
“This is my first baby, and I have no experience breastfeeding confidently. I wanted support, but my husband was too busy… my mother-in-law told me to feed the baby butter in addition to breast milk. I was not confident in this challenge, so I decided to give butter as my mother-in-law recommended, even though I know complementary feeding is not advised up to six months” (A 21-year-old primiparous mother, FGD).
These reflect mothers’, particularly primiparous mothers’, challenges of breastfeeding confidence.
Determinants undermining breastfeeding confidence
Postnatal mothers described several factors that reduced their confidence in breastfeeding. Women’s work responsibilities and limited social support significantly undermined some mothers’ breastfeeding confidence.
“This is my second baby. I do not feel confident about breastfeeding because I am busy with work during the day, and at night, I have no support; rather, I must cook for my first child, my husband, and my family. Unlike my best friend, I do not plan to breastfeed my baby for up to two years. Even though I know it may be wrong, I have a plan to stop breastfeeding before six months.” (24-year-old FGD participant).
This indicated how work responsibilities and social support significantly influence the mothers’ breastfeeding self-confidence.
Community beliefs and myths also influence breastfeeding self-efficacy. In this study, the majority of the mothers described community myths around breastfeeding created feelings of shame and fear, leading to early cessation of breastfeeding their babies.
A 31-year-old FGD participant said, “This is my third baby. I have a plan to start additional food after three months because I am not confident breastfeeding in front of other people, even my extended family. In our community, there is a belief that bad spirits can affect breast milk production and babies’ comfort. Because of this, I do not feel confident breastfeeding when people are around me.”
These beliefs and myths make the mothers emotionally not ready to breastfeed their babies.
During the focus group discussion, some mothers raised the gender preference and mistreatment as barriers to breastfeeding confidence.
“This is my six baby. My husband and my mother-in-law were expecting a boy, but my baby was a girl. Because of her sex, they hate me and interrupt me while I am breastfeeding. Even the community does not like me, because they believe that at least one baby should be male. Because of this, I fear that my baby’s development is less than expected for her age, and I am not confident in breastfeeding my baby girl.” (A 39-year-old FGD multiparous mother).
These revealed that cultural preferences for male children and family mistreatment undermined breastfeeding confidence.
Determinants enhancing breastfeeding confidence
FGD mothers also described factors that strengthened their breastfeeding confidence. At the time of focus group discussions, participants shared that family support builds confidence to breastfeed their babies.
A 23-year-old primiparous mother said,” This is my first baby. I gave birth in this hospital, and now I am with my grandmother. I had antenatal care for this baby, and I am confident that breastfeeding exclusively up to six months without complementary food. My grandmother showed me how to breastfeed based on her experience, and my husband also helps me at night. I am happy and confident to breastfeed, and I plan to continue up to two years.”
This showed that support from family, particularly experienced relatives are essential in building and increasing mothers’ confidence.
Furthermore, prior counseling and health education also played a significant role in breastfeeding self-efficacy. At the time of focus group discussions, participants also shared that prior counseling had built confidence to breastfeed their babies.
“This is my second baby. I gave birth in this hospital, and now I am with my relative, who is a health extension worker. I had antenatal care for this baby, and I am confident about breastfeeding exclusively up to six months without complementary food. My relative showed me and taught me how to breastfeed based on her experience. I am happy and confident to breastfeed up to two years.” (26-year-old FGD mother).
These indicated that antenatal counseling and exposure to breastfeeding education positively reinforced self-efficacy.
Quantitative findings regarding determinant factors
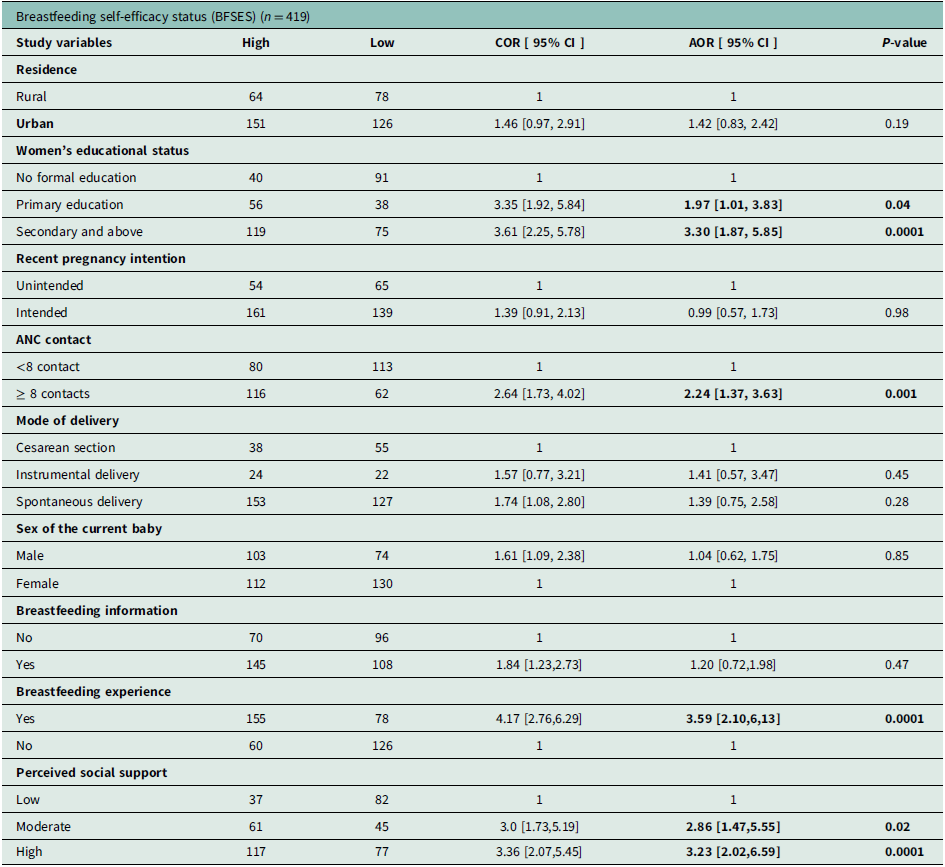
Bivariate logistic regression analysis showed that residence, women’s educational status, recent pregnancy intention, ANC contact, mode of delivery, sex of current baby, having breastfeeding information, breastfeeding experience, and perceived social support were found to be candidate variables (p < 0.25) for multivariable analysis.
In multivariable analysis, women’s educational status, ANC contact, breastfeeding experience, and perceived social support were significantly associated with breastfeeding self-efficacy (p < 0.05).
In the present study, women with higher educational status (AOR = 1.97; 95% CI: 1.01, 3.83) and (AOR = 3.30; 95% CI: 1.87, 5.85) were more likely to have the ability to confidently breastfeed their baby as compared to those with no formal education. Women who attended 8 or more ANC contacts were 2.24 times (AOR = 2.24; 95% CI: 1.37, 3.63) more likely to be confident in breastfeeding as compared to women who attended fewer than 8 contacts.
Women who had previous breastfeeding experience were three times more likely to have breastfeeding self-efficacy as compared to those who had no previous experience (AOR = 3.59; 95% CI: 2.10, 6.13). Those study participants who had high and moderate perceived social support regarding breastfeeding were 3.23 (AOR = 3.23; 95% CI: 2.02, 6.59) and 2.86 times (AOR = 2.86; 95% CI:1.47,5.55 more likely to have confidence to breastfeed their baby as compared with those women who did not have low perceived social support, respectively (Table 3).
Bivariate and multivariable analysis of determinant factors of breastfeeding self-efficacy status among postnatal women in Gurage Zone public hospitals, Central Ethiopia, 2025

Note: AOR: Adjusted Odds Ratio, ANC: Antenatal Care, BFSE: Breastfeeding Self-Efficacy, COR: Crude Odds Ratio, CI: Confidence Interval, 1: Reference category.
Discussion
Breastfeeding self-efficacy is a mother’s confidence in her ability to breastfeed her infant. A mother’s belief in her ability to breastfeed strongly determines whether she initiates, persists, and successfully sustains breastfeeding, especially when facing challenges, according to Bandura’s Self-Efficacy Theory (Bandura, Reference Bandura1997). In the present study, the overall prevalence of breastfeeding self-efficacy was 51.3% (95% CI: 47, 56). The finding indicates nearly half of the participants in the study population lacked confidence in their ability to successfully breastfeed, which leads to difficulties in achieving optimal breastfeeding practices. Self-Efficacy Theory indicated that low confidence reduces the motivation and coping ability of mothers, making them more vulnerable to early breastfeeding cessation (Dennis, Reference Dennis2003). The findings highlight the necessity for specific programs, including health education, social support, and counseling, to enhance maternal confidence for better breastfeeding outcomes.
The prevalence observed in this study is in line with a study conducted in the southern Ethiopian region (48%) (Nigussie et al., Reference Nigussiee, Demeke, Bagilkar, Firetsidk, Abageda and Belachew2025). In contrast, this study is lower than studies conducted in Australia (72%) (Bourne et al., Reference Bourne, Brown, Haines, Truong and Smith2013), Brazil (82.35%) (Souza and Fernandes, Reference Souza and Fernandes2014), Thailand (70.3%) (Lynn and Chuemchit, Reference Lynn and Chuemchit2024), Indonesia (90.2%) (Hemiyanty et al., Reference Hemiyanty, Wandira and Suwendro2022), Greece (65%) (Brani et al., Reference Brani, Mrvoljak-Theodoropoulou, Pechlivani, Gourounti, Iliadou, Palaska, Antsaklis, Drakakis and Dagla2024), and Uganda (60.2%) (Nankumbi et al., Reference Nankumbi, Mukama and Ngabirano2019). The possible explanation for this variation may be that healthcare infrastructure differences, combined with limited access to skilled maternal care, strongly affect BFSE. Australia and Brazil maintain advanced breastfeeding support networks with professional lactation experts and organized postnatal programs that many Ethiopian regions lack (Passanha et al., Reference Passanha, Benício, Venâncio and Dos Reis2013; Burns et al., Reference Burns, Duursma and Triandafilidis2020; Zegeye et al., Reference Zegeye, Gebrehana, Bezabih, Mengistu, Adane and Lakew2024). In addition to this, cultural beliefs and social norms of countries like Indonesia and Brazil have strong cultural norms supporting exclusive breastfeeding, which enhance breastfeeding self-efficacy as compared to Ethiopian mothers (Agrina et al., Reference Agrina, Wahyuni, Misrawati, Suyanto, Dewi and Guna2025). Furthermore, the discrepancy may also be explained by variations in the timing of evaluation, sampling techniques, and sample size.
This study found a higher prevalence compared to Brazil (35%) (de Abreu et al., Reference de Abreu, Filipini, da Costa Aguiar Alves, da Veiga and Fonseca2018) and India (38.8%) (Vaithilingan and Johnson, Reference Vaithilingan and Johnson2023). The possible explanation may be due to the conduct of the studies, and the characteristics of the participants may explain the differences. The study in Brazil focused only on mothers 12–72 hours after birth and used non-probability sampling, whereas this study focused on the early postpartum period, and the study participants were selected by using the probability sampling method. Moreover, regarding the educational status of the respondents, the higher educational attainment of study participants in the Brazil study was only 16%, as compared to this study, in which 46.3% of study participants had a high educational status (de Abreu et al., Reference de Abreu, Filipini, da Costa Aguiar Alves, da Veiga and Fonseca2018). On the other hand, the Puducherry, India, study included only first-time mothers, while our study included both first-time and experienced mothers, making it more representative (Vaithilingan and Johnson, Reference Vaithilingan and Johnson2023). Also, the larger sample size in our study may have given more accurate results than the smaller-sample-size studies.
This study further identified the determinants of breastfeeding self-efficacy among postnatal women in central Ethiopia. The determining factors of breastfeeding self-efficacy included women’s educational status, ANC contact, breastfeeding experience, and perceived social support.
In this study, women’s educational status had a strong association with breastfeeding self-efficacy status; women who completed primary education and secondary or higher were 1.97 and 3.30 times more likely to have the ability to confidently breastfeed their baby, as compared to those with no formal education. These findings are supported by qualitative findings, as mothers with limited education or first-time mothers often reported low confidence in breastfeeding, particularly when family advice conflicted with health recommendations. These findings are consistent with studies conducted in Saudi Arabia (Al-Thubaity et al., Reference Al-Thubaity, Alshahrani, Elgzar and Ibrahim2023), Greece (Economou et al., Reference Economou, Kolokotroni, Paphiti-Demetriou, Kouta, Lambrinou, Hadjigeorgiou, Hadjiona and Middleton2021), Iran (Poorshaban et al., Reference Poorshaban, Pakseresht, Bostani Khalesi and KazemNejad Leili2017), and Indonesia (Titaley et al., Reference Titaley, Dibley, Ariawan, Mu’asyaroh, Alam, Damayanti, Do, Ferguson, Htet, Li, Sutrisna and Fahmida2021). The possible explanation might be that as educational status increases, access to information and awareness regarding breastfeeding confidence also increase. Moreover, the evidence shows that, as educational attainment increases, mothers’ ability to handle challenges, make informed decisions, and be more prepared and confident in their ability to breastfeed also increases (Si and Mao, Reference Si and Mao2024; Nigussiee et al., Reference Nigussiee, Demeke, Bagilkar, Firetsidk, Abageda and Belachew2025).
In these findings, antenatal care contact was significantly associated with breastfeeding self-efficacy status. Mothers who attended 8 or more ANC contacts were 2.24 times more likely to be confident in breastfeeding compared to women who attended fewer than 8 contacts. The results are supported by qualitative findings, as mothers who had ANC contact and prior counseling expressed higher confidence in breastfeeding. These findings are similar to studies conducted in China (Yang et al., Reference Yang, Gao, Ip and Sally Chan2016), Turkey (Topuz et al., Reference Topuz, Duman, Uysal and Öcalan2021), and southern Ethiopia (Gizaw et al., Reference Gizaw, Sopory and Morankar2022). A possible justification is that increased frequency of antenatal care contacts enhances women’s access to information, counseling, and guidance on proper breastfeeding practices from healthcare personnel. In addition, breastfeeding education as a routine component of ANC contacts empowers mothers by increasing awareness, dispelling myths about breastfeeding, and boosting breastfeeding confidence (Öztürk et al., Reference Öztürk, Ergün and Özyazıcıoğlu2022; Kumari and Jain, Reference Kumari and Jain2024; Tello et al., Reference Tello, Hernández, Dueñas-Espín and Tejera2025). The qualitative findings indicated that antenatal counseling and exposure to breastfeeding education positively reinforced self-efficacy.
This finding revealed the strong association between breastfeeding experience and breastfeeding self-efficacy status. Women who had previous breastfeeding experience were three times more likely to have breastfeeding self-efficacy compared to those who had no previous experience. These findings are supported by studies conducted in Malaysia (Johari and Abdul Hamid, Reference Johari and Abdul Hamid2021), Saudi Arabia (Al-Thubaity et al., Reference Al-Thubaity, Alshahrani, Elgzar and Ibrahim2023), China (Yang et al., Reference Yang, Gao, Ip and Sally Chan2016), and Thailand (Lynn and Chuemchit, Reference Lynn and Chuemchit2024). The possible reason is that the experiences of breastfeeding positively enhance mothers’ confidence to breastfeed their babies. Furthermore, breastfeeding experiences enhance mothers’ intention to breastfeed and confidence, directly contributing to a strong sense of self-efficacy that supports successful breastfeeding practices (Huang et al., Reference Huang, Ouyang and Redding2019). The qualitative findings indicated that mothers with prior breastfeeding experience reported higher confidence compared to first-time mothers. This finding is supported by social cognitive theory, which states that prior mastery experiences, such as previous breastfeeding, enhance self-efficacy and mothers’ confidence in breastfeeding (Bartle and Harvey, Reference Bartle and Harvey2017).
Regarding social support, this study discovered that participants with high and moderate perceived social support for breastfeeding were 3.23 and 2.86 times more likely, respectively, to have confidence in breastfeeding their baby compared with women who had low perceived social support. The qualitative findings described mothers who had social support from family members as strengthened breastfeeding self-efficacy. These findings suggest that social interventions are important for improving mothers’ confidence in breastfeeding. This finding is supported by studies conducted in different countries, such as China (He et al., Reference He, Yimyam and Namprom2022), Turkey (Konukbay et al., Reference Konukbay, Öksüz and Guvenc2024), Brazil (De Sá Guimarães et al., Reference De Sá Guimarães, Conde, Gomes-Sponholz, Oriá and Dos Santos Monteiro2017), Iran (Mirghafourvand et al., Reference Mirghafourvand, Malakouti, Mohammad-Alizadeh-Charandabi and Faridvand2018), Uganda (Miller et al., Reference Miller, Collins, Boateng, Widen, Natamba, Achoko, Acidri, Young and Martin2022), and Southern Ethiopia (Gizaw et al., Reference Gizaw, Sopory and Morankar2022). A possible justification for this association might be that mothers who receive social support, especially from healthcare personnel, partners, and families, tend to have higher breastfeeding self-efficacy and greater breastfeeding continuation rate. Perceived social support can be greatly used as a predictor by enhancing self-perception, lowering stress, and boosting sustained confidence in breastfeeding (Can et al., Reference Can, Bulduk, Can and Ayşin2025; Gopal et al., Reference Gopal, Venkatnarayan, Gopal, Sharma, Kumar and Lahariya2025). This aligns with social cognitive theory, which highlights the role of helpful surroundings in shaping health behaviors (Islam et al., Reference Islam, Awal, Mazumder, Munni, Majumder, Afroz, Tabassum and Hossain2023). The evidence showed that breastfeeding support is a key strategy for improving newborn survival, child health outcomes, and the effectiveness of primary healthcare (Kumari and Jain, Reference Kumari and Jain2024; Thacker et al., Reference Thacker, Singh and Grange2025).
These findings show important gaps in knowledge regarding breastfeeding self-efficacy status among mothers in the Gurage Zone, Central Ethiopia. The results suggest that improving health education during antenatal care and postnatal care is essential. Enhancing the quality of antenatal care contact, women’s educational status, the provision of counseling and awareness-creating on breastfeeding, and good social support could significantly improve breastfeeding self-efficacy, which has the potential to reduce neonatal complications and morbidity in the study area. Moreover, the qualitative findings discovered social norms, beliefs, and cultural effects on breastfeeding confidence. These findings have implications for policy and practice in contexts beyond the local setting. Improving breastfeeding self-efficacy globally, especially in culturally distinct areas, supportive social norms shape infant feeding practices. Policymakers are encouraged to integrate culturally sensitive breastfeeding counseling into national maternal and child health guidelines, promote community-based supports, and strengthen health workers to address misconceptions regarding breastfeeding practices. In addition, global health institutions are expected to design interventions on modifiable factors to enhance mothers’ confidence in breastfeeding practices.
Strengths and limitations of the study
Strength of the study
In this study, women’s breastfeeding self-efficacy status was assessed using a mixed study design that included both first-time and experienced women. To the knowledge of the investigator, no previous study has been conducted in this setting. Potential biases were minimized by using clear objectives and research questions, pretested questionnaires, training for data collectors and supervisors, a random sampling method, an ideal sample size, and statistical adjustments (multivariable regression) to account for confounding variables. Finally, ethical guidelines were followed to ensure unbiased participation.
Limitations of the study
In this study, self-reported data on breastfeeding self-efficacy may have introduced recall bias and social desirability biases, leading to possible over- or under-reporting. To minimize this, structured questionnaires with specific prompts and clear pretested tools were used to help participants accurately recall their experiences. Furthermore, facility-based sampling may limit the generalizability of the findings to the wider population. Since this is a cross-sectional study, it does not show cause-and-effect relationships.
Conclusion and recommendations
Conclusion
The present findings indicated that 48.7% of women lacked breastfeeding self-efficacy. The educational status, breastfeeding experience, antenatal contact, and perceived social support were significantly associated with breastfeeding self-efficacy. Mothers’ breastfeeding confidence is essential to improve maternal and child health outcomes. Mothers who have high breastfeeding self-efficacy initiate and continue exclusive breastfeeding, which reduces the risk of malnutrition, neonatal infections, and infant morbidities. Enhancing maternal confidence in breastfeeding can lead to progress toward global nutrition and improved child health outcomes. As a result, the study concludes that by intervening in the modifiable factors, postpartum women’s awareness regarding breastfeeding self-efficacy can be increased.
Recommendations
The following recommendations were given based on the findings to the concerned bodies:
To Gurage Zone public hospitals and health care providers: It is encouraged to provide targeted health education on breastfeeding and its benefits during antenatal care (ANC) contact by using simple, culturally appropriate materials to improve women’s awareness regarding breastfeeding self-efficacy. At the community level, it is encouraged to design community-based awareness campaigns focusing on women with lower educational status and those who have no experience. In addition, encourage health extension workers and community health volunteers in disseminating information at the household and community levels regarding the importance of social support to enhance breastfeeding self-efficacy.
To policymakers and the healthcare system: The study findings show gaps in breastfeeding self-efficacy, ANC contact, and social support. Strengthening the integration of breastfeeding self-efficacy into maternal and child health programs at all levels of the healthcare system aligns with existing maternal and child health policies that promote universal access to maternal health services. Additionally, enhancing maternal confidence in breastfeeding can lead to progress toward global nutrition and improved child health outcomes.
For the researcher: A longitudinal study needs to be done to gain a better understanding of women’s breastfeeding self-efficacy.
Data availability statement
Data that support the findings are available from the corresponding author upon a reasonable request.
Acknowledgements
The authors would like to thank Wolkite University for giving us the opportunity to conduct the research and for granting ethical approval. Authors also extend our gratitude to the study participants, data collectors, and the supervisor for their unreserved efforts and willingness to participate in this research study.
Author contribution
MA and ABD wrote the proposal, participated in data collection and supervision, analyzed the data, and drafted the paper. MA, AB, and ABD approved the proposal with some revisions, participated in data analysis, and revised subsequent paper drafts. KNM, ASA, and MOG commented on the final paper and manuscript. All authors read and approved the manuscript.
Funding statement
The author(s) received no financial support for this article’s research, authorship, and/or publication.
Competing interests
There is no potential conflict of interest concerning the research, authorship, and/or publication of this article.
Ethical standards
Ethical clearance was obtained from the Wolkite University, Institutional Review Board with reference number IRB/037/25). A formal letter of permission was obtained from Wolkite University to the Zonal Health Office and the hospitals to allow the execution of the research. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. An ethical letter was written to the Gurage Zone public hospitals to obtain permission for data collection. The purpose of the study and participants’ right to refuse were explained to the study participants, and informed written consent was obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of all minors (under 18 years old) participants before enrollment. Coding was implemented to remove respondents’ names and other personal identifiers throughout the study to ensure participant confidentiality.
Consent for publication
Not applicable.


 Open access
Open access