


Introduction
Enlarged vestibular aqueduct (EVA) is the most common inner ear malformationReference Germiller, Wetmore and Bell1 seen in hearing loss. Approximately 82 per cent of EVA patients present by the age of five years with either congenital or delayed onset hearing loss while the remainder present later, even in adulthood.Reference Jackler and De La Cruz2 Enlarged vestibular aqueduct syndrome (EVAS) is characterised by hearing loss, often bilateral and mixed, with characteristic imaging findings of unilateral or bilateral enlarged vestibular aqueducts. Hearing outcomes vary from stable hearing in 51 to 67 per cent of patients,Reference Mori, Westerberg, Atashband and Kozak3 progressive hearing loss in 10 to 70 per cent of patientsReference Jackler and De La Cruz2, Reference Madden, Halsted, Benton, Greinwald and Choo4 and sudden hearing loss in up to 60 per cent of patients.Reference Okumura, Takahashi, Honjo, Takagi and Mitamura5 Negative prognostic factors described in a systematic reviewReference Saeed, Kenth, Black, Saeed, Stivaros and Bruce6 of literature include presence of hearing loss at 250 Hz,Reference Greinwald, DeAlarcon, Cohen, Uwiera, Zhang and Benton7 vestibular aqueduct midpoint size,Reference Ascha, Manzoor, Gupta, Semaan, Megerian and Otteson8 head traumaReference Noguchi, Fukuda, Fukushima, Gyo, Hara and Nakashima9 and the presence of biallelic SLC26A4 mutations.Reference Greinwald, DeAlarcon, Cohen, Uwiera, Zhang and Benton7 A meta-analysis found that patients with sudden hearing loss were more likely to experience another sudden hearing loss episode, as well as hearing loss after minor head trauma.Reference Noordman, van Beeck Calkoen, Witte, Goverts, Hensen and Merkus10 Sudden hearing loss may or may not recover to baseline, and can be catastrophic in patients with pre-existing severe hearing loss as it can result in complete loss of hearing not amenable to amplification, which we term an EVAS crisis. Sudden sensorineural hearing loss (SSNHL) has further devastating impact on the paediatric population. Studies have widely demonstrated that SSNHL may lead to delays in speech and language acquisition, which may result in difficulties in comprehension and communication.
Steroids and hyperbaric oxygen therapy (HBOT) are the main treatment options in the guidelines for the management of idiopathic SSNHL in patients more than 18 years of age.Reference Chandrasekhar, Tsai Do, Schwartz, Bontempo, Faucett and Finestone11 Two systematic reviews cum meta-analysesReference Alter, Hamiter, Han, Leu, Usseglio and Lalwani12, Reference Joshua, Ayub, Wijesinghe and Nunez13 have found higher chances of recovery of SSNHL when HBOT is used in combination with medical treatment, than medical treatment (usually steroids) alone. To date, there are no guidelines or large studies on the management of EVAS crisis. In a meta-analysis of thirteen studies on paediatric SSNHL,Reference Wood, Shaffer, Kitsko and Chi14 only two studies reported findings of EVA,Reference Dedhia and Chi15, Reference Chen, Jiang, Zong and Wu16 of which one patient received steroids with no improvement.
Given the uncertainty in pre-existing literature, and the importance of addressing paediatric hearing loss, a comprehensive summary of evidence is clinically relevant and timely. This systematic review aims to investigate the appropriate treatment options for patients with EVAS crisis and their success rates.
Methods
Our study methodology was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The study was registered on PROSPERO (CRD24021261072) prior to data collection. The PRISMA checklist is included in Supplementary Table 1.
Study selection
Embase, Ovid MEDLINE and Web of Science databases were searched from inception to 19 August 2024 for studies reporting the effect of various treatment options for EVAS. The search terms were generated with the help of a medical librarian and are published in Supplementary Table 2.
Based on the Population, Intervention, Comparators, and Outcomes (PICO) framework, the inclusion criteria were as follows: Publication in English. Foreign-language journals were screened when an English abstract was available. Participants: EVA patients of all ages with sudden hearing loss. Intervention: Treatment administered to improve sudden hearing loss. Comparison: Participants that did not receive any treatment. Outcomes: Degree of hearing improvement (dB HL) and return to baseline hearing. Study design: Case reports and case series were included. Articles reporting EVA with gradual hearing loss and surgical management of EVA-related sudden hearing loss, duplicates, reviews, meta-analyses, animal studies and studies with incomplete data were excluded.
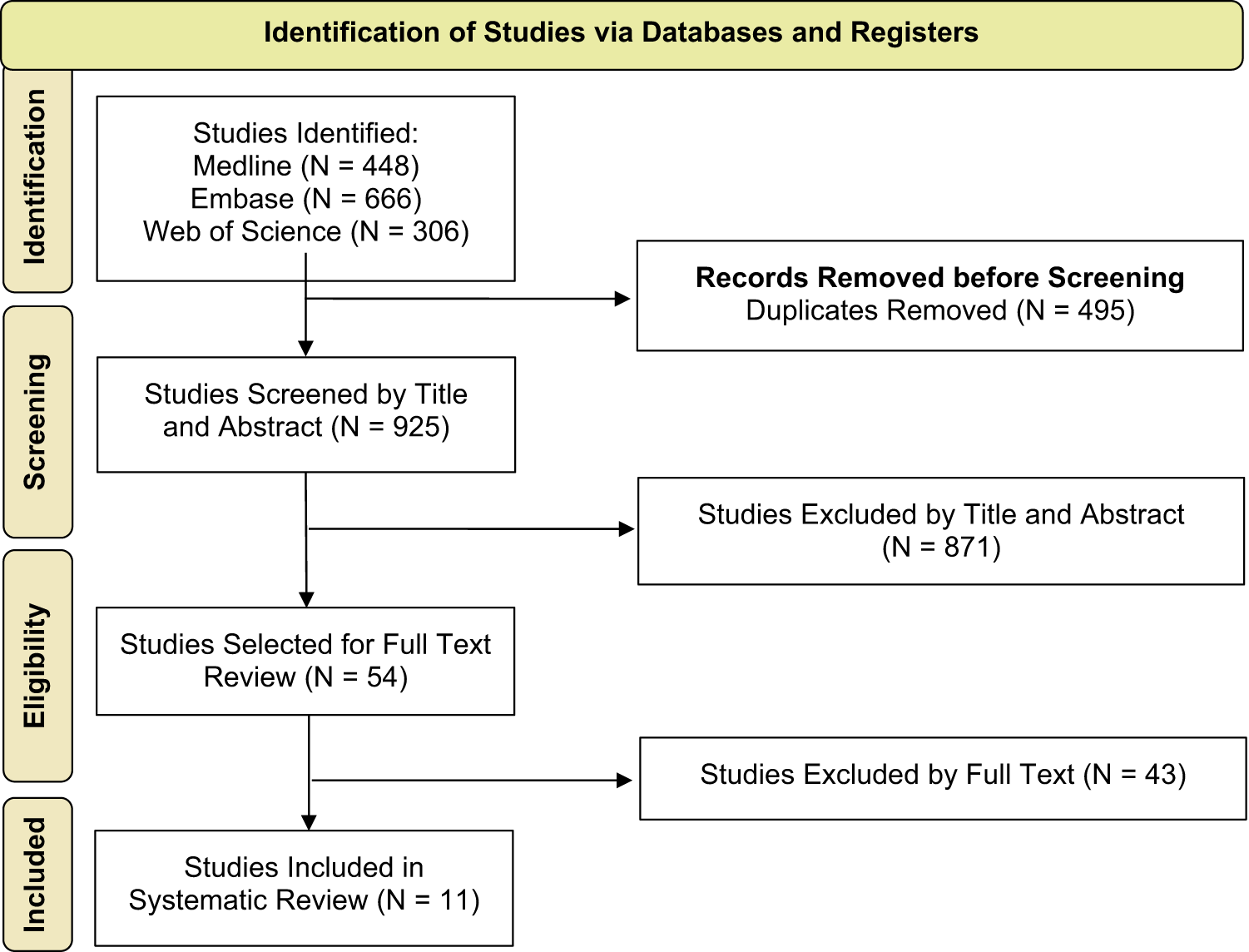
The references for the articles were uploaded into Rayyan.Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid17 Two independent reviewers (C.Y.C. and J.N. during the first search, C.Y.C. and S.X.L.S. during the second search) blindly reviewed all identified titles and abstracts, followed by their full texts to check the eligibility for inclusion. The articles were divided into include, exclude, and maybe categories based on the inclusion criteria. Upon completion of the individual review, blinding was removed. In the event of conflicts and or all articles in the maybe category by any reviewer, a consensus was reached after discussion. The study selection process can be found in Figure 1.
PRISMA flowchart of included studies. PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.

Figure 1 Long description
The flowchart outlines the process of identifying studies via databases and registers. It begins with ′Identification′ where studies are identified from Medline (448), Embase (666) and Web of Science (306). Next, ′Records Removed before Screening′ shows 495 duplicates removed. In ′Screening′, 925 studies are screened by title and abstract, with 871 excluded. ′Eligibility′ involves selecting 54 studies for full text review, with 43 excluded. Finally, ′Included′ shows 11 studies included in the systematic review.
Data extraction and synthesis
Relevant information from each included article was extracted to Microsoft Excel (Microsoft Corporation 2016) by C.Y.C. The types of information extracted were year of publication, first author, article title, type of study, number of patients, sex, side of involvement, age at diagnosis, treatment instituted (if any), treatment window, baseline hearing thresholds (dB HL), degree of hearing deterioration (dB HL), hearing after treatment (dB HL), degree of hearing improvement (dB HL), recovery to baseline (none, partial or full recovery) after first treatment, salvage treatment, type of salvage treatment, salvage treatment window, hearing thresholds after salvage treatment (dB HL), degree of hearing improvement after salvage treatment (dB HL) and recovery to baseline (none, partial or full recovery) after salvage treatment. We defined full recovery as a return to the baseline hearing, partial recovery as a recovery of 10 dB or more but not to baseline and none when the improvement was less than 10 dB, in line with that described by Furuhashi et al.Reference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18
Risk of bias assessment and evaluation of overall evidence
The risk of bias of included studies was evaluated using the Joanna Briggs Institute (JBI) Critical Appraisal Tool (Supplementary Material 3). As outlined by the JBI tool, distinct criteria were applied depending on the study design of each included study. For each domain accessed, a point may be awarded if the criteria were met, while no point would be allocated if the study did not meet the criteria or if it was unclear whether they were met. The total aggregate score for each study was converted to a percentage of the total possible score. We classified studies as high, moderate and low risk of bias if they scored less than 50 per cent, 50–80 per cent or greater than 80 per cent, respectively. The overall certainty of evidence was evaluated using the Grading Recommendations Assessment, Development and Evaluation (GRADE) approach.
Results
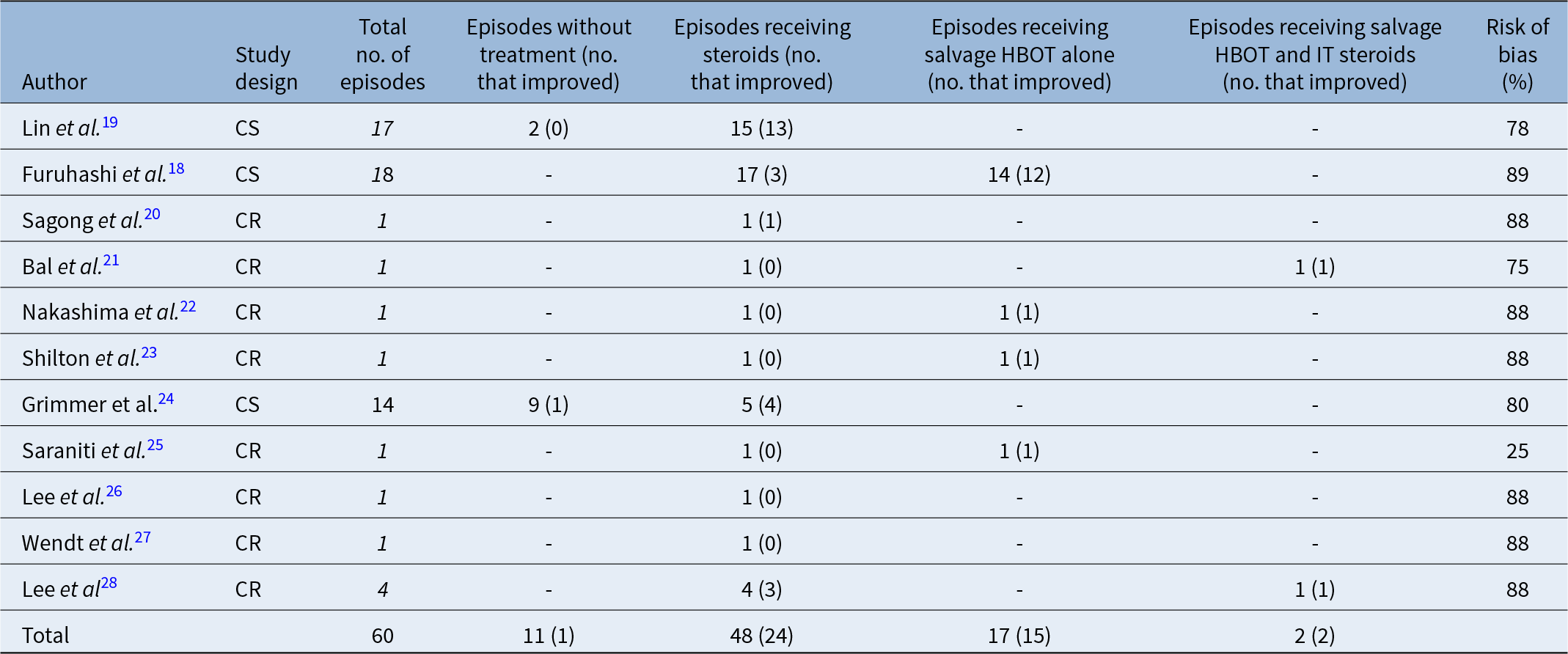
A systematic search generated 1,420 articles, of which 925 remained after the removal of duplicates. Ultimately, 11 studiesReference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18–Reference Lee, Kim, Kwek and Chan28 were included in the final analysis (Figure 1), of which three studiesReference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Lin, Lin, Kao and Wu19, Reference Grimmer, Hedlund and Park24 were case series and eightReference Sagong, Seok, Kwon, Kim, Lee and Lee20–Reference Shilton, Hodgson and Burgess23, Reference Saraniti, Di Franco, Maggio, Martines and Martines25–Reference Lee, Kim, Kwek and Chan28 were case reports. There were 60 episodes of EVAS crisis affecting 39 patients, of which 11 patients experienced two or more episodes in the same ear or the contralateral ear. The maximum recorded number of SSNHL in a single patient was seven, and patients with multiple episodes received multiple courses of steroids and salvage HBOT. The key characteristics extracted from included studies are summarised in Table 1. Of note, improvement was noted in 1 of 11 episodes (9.1 per cent) that did not receive any treatment, 24 of 48 episodes (50.0 per cent) that received steroids and 17 of 19 episodes (89.5 per cent) that received salvage HBOT. The risk of bias assessment of included studies using the JBI critical appraisal tool can be found in Supplementary Tables 3-4. There were twoReference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Grimmer, Hedlund and Park24 case series with a low risk of bias and one case seriesReference Lin, Lin, Kao and Wu19 with a moderate risk of bias. Separately, there were sixReference Sagong, Seok, Kwon, Kim, Lee and Lee20, Reference Nakashima, Ueda, Furuhashi, Yasue, Beppu and Ogawa22, Reference Shilton, Hodgson and Burgess23, Reference Lee26–Reference Lee, Kim, Kwek and Chan28 case reports with a low risk of bias, one with a moderate risk of biasReference Bal, Ismi, Bucioglu, Vayısoğlu and Gorur21 and one with a high risk of bias.Reference Saraniti, Di Franco, Maggio, Martines and Martines25 The overall certainty of evidence was determined by GRADE can be found in Supplementary Table 5.
EVAS crisis: summary of included studies

Table 1 Long description
The table summarizes 11 EVAS studies (case series and case reports) by author, number of hearing-loss episodes, treatments used, number improved, and risk-of-bias percentage. Overall there were 60 episodes: 11 had no treatment with 1 improvement, and 48 received steroids with 24 improvements. Salvage hyperbaric oxygen therapy alone was reported for 17 episodes with 15 improvements, suggesting higher improvement counts than steroids or no treatment in the episodes where it was used. Salvage hyperbaric oxygen therapy combined with intratympanic steroids was reported for 2 episodes with 2 improvements. Larger case series include Lin (17 episodes; 13 improved with steroids; none improved without treatment) and Furuhashi (18 episodes; 3 improved with steroids; 12 improved with salvage hyperbaric oxygen therapy alone). Risk-of-bias ratings vary widely, from 25 percent to 89 percent, and most evidence comes from single-episode case reports, so comparisons across treatments are limited and may reflect selection and reporting differences rather than treatment effect.
Note: Values presented as number of events.
CS = case series; CR = case report; EVAS = enlarged vestibular aqueduct syndrome; HBOT = hyperbaric oxygen therapy.
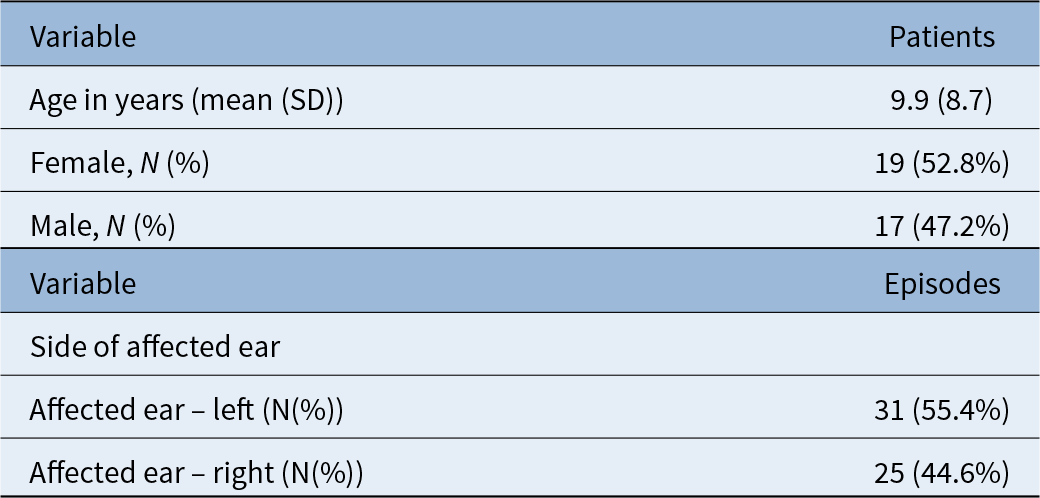
The demographic data of patients are presented in Table 2. The mean age of participants was 9.9 +/- 8.7 years old, of which the youngest HBOT recipient was 4 years old. Where data were reported, 52.8 per cent of participants were female. The majority of sudden hearing loss episodes occurred in the left ear (55.4 per cent), while the right ear was affected in 44.6 per cent of cases.
Demographic data of EVAS patients

Table 2 Long description
The table summarizes patient demographics and episode characteristics for individuals with enlarged vestibular aqueduct syndrome. Mean age was 9.9 years with a standard deviation of 8.7 years. Sex distribution was nearly even, with 19 females (52.8 percent) and 17 males (47.2 percent). For episodes, the affected ear was more often the left ear, reported in 31 episodes (55.4 percent), compared with 25 episodes (44.6 percent) involving the right ear. Percentages for sex are based on patients, while percentages for ear side are based on episodes, so the two sections should not be directly compared as the same denominator.
EVAS = enlarged vestibular aqueduct syndrome; HBOT = hyperbaric oxygen therapy.
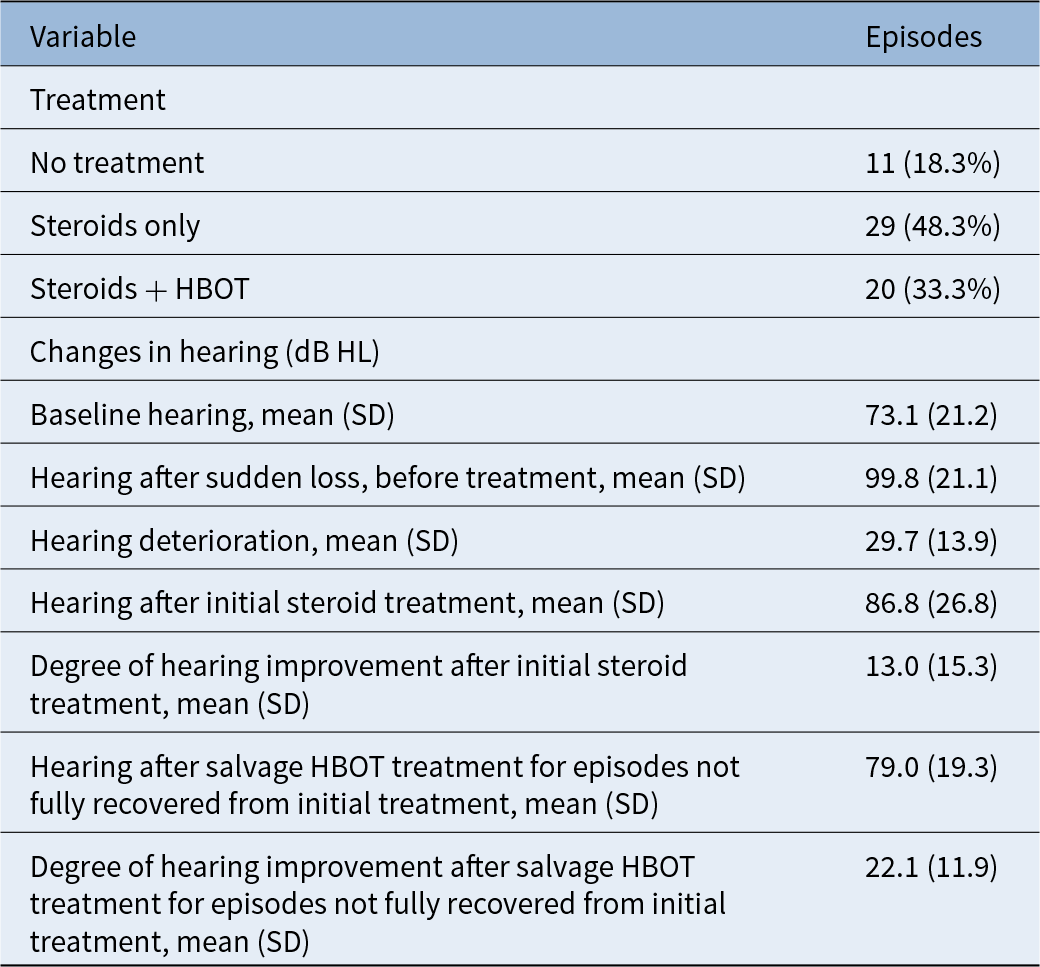
Table 3 provides an overview of the treatments administered to patients with EVAS and the corresponding changes in their hearing outcomes. The degree of hearing deterioration ranged from 11 to 67 dB HL. Eleven of the episodes of EVAS crisis did not receive any treatment, while the initial treatment in the remaining 49 episodes were systemic steroids (oral or intravenous). The average baseline hearing function of EVAS patients was 73.1 +/- 21.2 dB. Administration of initial steroids improved hearing by 13.0 +/- 15.3 dB on average. However, 20 patients did not regain their baseline hearing levels following systemic steroid treatment and subsequently underwent salvage HBOT. For these patients, HBOT was initiated approximately seven days after steroid therapy, typically involving 15 sessions. The hearing function of these patients improved by 22.1 ± 11.9 dB on average with salvage HBOT, resulting in a mean hearing function of 79.0 ± 19.3 dB.
Management of EVAS patients with hearing loss

Table 3 Long description
The table summarizes treatment choices and average hearing level changes across episodes in patients with enlarged vestibular aqueduct syndrome. Treatment distribution was 11 episodes with no treatment (18.3%), 29 with steroids only (48.3%), and 20 with steroids plus hyperbaric oxygen therapy (33.3%). Mean baseline hearing was 73.1 dB HL, worsening to 99.8 dB HL after sudden loss before treatment, for an average deterioration of 29.7 dB HL. After initial steroid treatment, mean hearing improved to 86.8 dB HL, corresponding to an average improvement of 13.0 dB HL. For episodes not fully recovered after steroids, salvage hyperbaric oxygen therapy was associated with mean hearing of 79.0 dB HL and an average additional improvement of 22.1 dB HL. Values are reported as means with standard deviations, so individual responses may vary and the table does not indicate statistical testing or outcomes for untreated episodes beyond treatment counts.
EVAS = enlarged vestibular aqueduct syndrome; HBOT = hyperbaric oxygen therapy.
Adverse effects
One patient experienced otalgia when the HBOT chamber had to be rapidly depressurised because another patient had difficulty equalising ear pressure. There were no side effects of HBOT or steroids reported in the other studies.
Discussion
To our knowledge, this is the first systematic review investigating the success of steroids and salvage HBOT in the treatment of EVAS crisis. Our results show that first line treatment of EVAS crisis with steroids may be associated with improvement in hearing thresholds and likelihood of full recovery. Likewise, we show that salvage HBOT in steroid non-responders is associated with improvement in hearing thresholds and likelihood of full recovery.
Steroid administration
The clinical practice guidelines for sudden sensorineural hearing loss recommend oral prednisone at 1 mg/kg/day or equivalent dosing of methylprednisolone or dexamethasone with tapering regimes for 10 to 14 days.Reference Chandrasekhar, Tsai Do, Schwartz, Bontempo, Faucett and Finestone11 The included studies in our review had differing modes of steroid administration. Lin et al.Reference Lin, Lin, Kao and Wu19 dosed prednisone at 1 to 2 mg/kg/day, or equal doses of dexamethasone for two weeks. Furuhashi et al.Reference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18 described giving daily intravenous steroids (details unknown), adenosine triphosphate and vitamin B12 for up to seven days. Other regimes included oral prednisone at 0.5 to 1 mg/kg/day for one to three weeks,Reference Grimmer, Hedlund and Park24 oral methylprednisolone at 1 mg/kg/dayReference Bal, Ismi, Bucioglu, Vayısoğlu and Gorur21 and intravenous hydrocortisone 150 mg/day with alprostadil 5 μg/day for seven days.Reference Nakashima, Ueda, Furuhashi, Yasue, Beppu and Ogawa22 None of the studies described intratympanic steroids as first line treatment. Due to the small number of studies with varying steroid administration regimes, we cannot identify the ideal regime. We are also unsure of the impact of adjunctive treatments on hearing.
HBOT protocol and utility of concurrent steroid administration
The HBOT protocol also varied slightly amongst the studies. Most described patients undergoing 15 sessions where the air pressure was compressed and maintained at 2 atm for 60 to 90 minutes.Reference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Nakashima, Ueda, Furuhashi, Yasue, Beppu and Ogawa22, Reference Shilton, Hodgson and Burgess23 Of the sixReference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Bal, Ismi, Bucioglu, Vayısoğlu and Gorur21–Reference Shilton, Hodgson and Burgess23, Reference Saraniti, Di Franco, Maggio, Martines and Martines25, Reference Lee, Kim, Kwek and Chan28 reports using salvage HBOT, four prescribed HBOT alone after initial failure of systemic steroids.Reference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Nakashima, Ueda, Furuhashi, Yasue, Beppu and Ogawa22, Reference Shilton, Hodgson and Burgess23, Reference Saraniti, Di Franco, Maggio, Martines and Martines25 Two reportsReference Bal, Ismi, Bucioglu, Vayısoğlu and Gorur21, Reference Lee, Kim, Kwek and Chan28 used intratympanic steroids together with salvage HBOT. The clinical practice guidelines for SNNHL recommend initial or salvage therapy with HBOT combined with steroid therapy as an option.Reference Chandrasekhar, Tsai Do, Schwartz, Bontempo, Faucett and Finestone11 However, the fourReference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18, Reference Nakashima, Ueda, Furuhashi, Yasue, Beppu and Ogawa22, Reference Shilton, Hodgson and Burgess23, Reference Saraniti, Di Franco, Maggio, Martines and Martines25 reports using salvage HBOT alone show improvement in the hearing thresholds even without concurrent steroid administration. This suggests that HBOT itself improves the hearing outcome, but cannot conclude whether a second course of steroids (oral or intratympanic) given at the time of HBOT further enhances hearing recovery when treating EVAS crisis.
Practically, it is difficult for patients to adhere to daily HBOT and undergo intratympanic injections at the same time because the services may be located in different regions. Also, since most of the affected patients are children, general anesthesia is necessary to perform intratympanic injections, and they may not be able to meet the therapy schedule at the HBOT center on the same day.
Other treatments
During our review, we encountered two articles describing exploratory tympanotomy as a treatment option in EVAS crisis. One patient presented with recurrent hearing loss, tinnitus and aural fullness with a history of head trauma, while the other experienced hearing loss after head injury. Both were found to have perilymphatic fistula and were repaired. Though head trauma appears to be the common factor in these two cases, the data were extremely limited, and we cannot conclude that exploratory tympanotomy is indicated in all EVAS crisis.
Strengths and limitations
The pre-determined protocols of systematic searching, risk of bias evaluation and quality grading were rigorously adhered to, which enhance the credibility of the findings in this systematic review. However, there are several appreciable limitations of our study. First, results should be interpreted with a degree of caution due to underlying limitations of systematic reviews consisting of case reports and case series. Given that clinical data were collected and reported for the purposes of case reports and case series, many fall short of the requisite precision needed for quantitative analysis. There is also potential publication bias, reports with positive outcomes are more likely to be published. Second, potential confounders were not adjusted for due to insufficient reporting among included studies. Third, it was not possible to determine an ideal treatment regime because of the heterogeneity of steroid regimens and adjunct treatments in the studies. Fourth, the inclusion criteria of sudden hearing loss were not consistent across all studies. While some studies defined a decrease of 10 dB on pure tone audiogram to fulfil the criteria of sudden hearing loss,Reference Furuhashi, Sato, Nakashima, Miura, Nakayama and Mori18 others required patients to also have reduced speech discrimination.Reference Lin, Lin, Kao and Wu19 Similarly, the definitions of partial and full recovery were not defined in all studies, but we were able to overcome this as most studies included the hearing thresholds. Only seven episodes with documented improvement in hearing did not have baseline thresholds, and we were unable to determine if partial or full recovery was achieved. Fifth, bias with regards to the timing of treatment and selection of patients for HBOT may affect the interpretation of results. While it is unlikely for large sample sizes to exist considering the low overall incidence of EVA crisis in populations with easy access to HBOT, future observational studies with larger sample sizes, or multi-center randomised control trials dividing patient into the various treatment groups, may be beneficial in providing a more accurate pooled estimate of the overall effect size of outcomes. Additionally, future studies may consider investigating how the timing and dosing of steroid prescription affects outcomes.
Conclusion
Our results found initial steroids and salvage HBOT may be associated with improvements in hearing and full recovery. We recommend using steroids as first line treatment, and if available, to consider salvage HBOT for EVAS crisis in steroid non-responders to give patients the best chance at a functional hearing outcome. Steroid therapy should be initiated as soon as possible after confirmation of hearing deterioration and HBOT promptly instituted when there is no or partial recovery after systemic steroids.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0022215126105088.
Data availability
All articles in this manuscript are available from Embase, Ovid Medline, and Web of Science.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors”.
Competing interests
The authors declare none.
Author contributions
All authors have made substantial contributions to all the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted. No writing assistance was obtained in the preparation of the manuscript. The manuscript, including related data, figures and tables, has not been previously published and that the manuscript is not under consideration elsewhere. C.Y.C had full access to all the data and takes full responsibility for the integrity of the data. C.Y.C and J.G. conceived and designed the study. C.Y.C., J.N., B.S.Y.Y and S.X.L.S selected the articles and extracted data. B.S.Y.Y was responsible for statistical analysis. C.Y.C and B.S.Y.Y wrote the first draft of the manuscript. C.Y.C, B.S.Y.Y, S.X.L.S and J.G. contributed to critical revisions of the article. All authors approved this study for publication. The corresponding author attests that all listed authors meet authorship.
Acknowledgements
Miss Amy Bergeron, Librarian, McConnell Resource Centre, Medical Library; Ramanakumar Agnihotram and Frédéric Lamonde Biostatistics Consulting Unit, Research Institute of the McGill University Health Centre.



 Open access
Open access