


Introduction
Preventing surgical site infections (SSIs) depends on the timely administration of effective, perioperative, antimicrobial prophylaxis. Cefazolin is widely recommended as first-line prophylaxis for many clean and clean-contaminated procedures because of its activity spectrum, safety profile, and cost. Reference Bratzler, Dellinger and Olsen1,2 However, patients with a beta-lactam antibiotic allergy label often receive alternative, prophylactic agents, such as clindamycin and vancomycin. Reference Blumenthal, Ryan, Li, Lee, Kuhlen and Shenoy3 Inappropriate labeling is associated with the avoidance of first-line beta-lactam agents for treatment and prophylaxis, which increases the risk of SSI, Reference Blumenthal, Ryan, Li, Lee, Kuhlen and Shenoy3 rate of infections by antimicrobial-resistant organisms and C. difficile, Reference Blumenthal, Lu, Zhang, Li, Walensky and Choi4 duration of hospitalization, and healthcare costs. Reference Powell, Honeyford and Sandoe5 For these reasons, appropriately assessing patients’ information about antibiotic allergy is crucial to effective antimicrobial stewardship. Reference Powell, Honeyford and Sandoe5,Reference Trubiano, Chen and Cheng6
Antibiotic allergy labels are commonly recorded in electronic health records (EHR). When patients self-report an antibiotic allergy, this information is typically entered into their EHR by a physician, nurse or pharmacist. However, this information is often documented without sufficiently evaluating the specific symptoms, timing or clinical course. Indeed, many of the labels are in fact of nonallergic adverse drug reactions or historical events that are no longer clinically relevant. Reference Moskow, Cook and Champion-Lippmann7,Reference Shenoy, Macy, Rowe and Blumenthal8 The clinical impact of an allergy label depends not only on its availability, but also on the thoroughness of the information documented, such as the name of the causative agent, reaction phenotype, timing, recency, and whether the label has been assessed or re-evaluated. Reference Moskow, Cook and Champion-Lippmann7,Reference Shenoy, Macy, Rowe and Blumenthal8 In the perioperative setting, incomplete or ambiguous information about patients’ allergies may lead to a precautionary avoidance of certain agents as first-line prophylaxis. Reference Blumenthal, Ryan, Li, Lee, Kuhlen and Shenoy3
Evidence of the epidemiology and downstream effects of the beta-lactam allergy label is generally quite robust in the Western countries but remains limited in Asia, where the reported prevalence and assessment methods vary. Reference Mak, Yeung, Wong, Chiang and Li9 Given the differences in patterns of antimicrobial use, EHR systems, and access to allergologists, data are needed from each relevant region to inform a tailored approach to perioperative prophylaxis and antimicrobial stewardship. In Japan, there are scant data on the quality of antibiotic allergy-related documentation in EHR and real-world methods of perioperative assessment. In particular, it remains unclear how often the key elements of the documentation are missing, how frequently clinicians document assessment results or seek evaluation by a specialist, and to what extent these factors are associated with the use of non-first-line, prophylactic regimens.
The present study therefore had the three-fold aim of characterizing the completeness of antibiotic allergy labels in the EHR of patients undergoing surgery for which cefazolin was recommended as first-line prophylaxis; quantifying the frequency and content of documented clinical assessments and specialist evaluations of those labels; and describing the perioperative, prophylactic regimens actually administered (cefazolin vs non-first-line alternatives) in relation to the recorded labels.
Methods
Study setting and patient selection
This retrospective observational study was conducted at the Institute of Science Tokyo Hospital (ISTH, formerly Tokyo Medical and Dental University Hospital), an 813-bed tertiary teaching hospital with 19 surgical departments located in Tokyo, Japan. The study period was April 2021 through March 2023.
Patient identification and eligibility criteria
This study included adult patients (aged ≥ 18 yr) who had undergone surgery in any one of the following surgical departments: orthopedic, obstetrics and gynecology, peripheral vascular surgery, thoracic surgery, breast surgery, cardiac surgery, general surgery, and cardiology. These departments were chosen for analysis because they administered a cefazolin-based prophylaxis as the first-line regimen for most procedures in accordance with departmental protocol and accounted for most of the eligible surgeries during the study period. Cardiology was included because certain invasive procedures at the study center are managed within the cardiology department and follow the same perioperative prophylaxis workflow. Eligible cases were identified by linking operating room and procedural scheduling records with those of perioperative medication administration to capture prophylactic antibiotic use. These cases were then cross-referenced with a dedicated EHR allergy module to identify patients with antibiotic allergy label ≥1. The exclusion criteria were age <18 years and change in the recommended prophylactic regimen due to intraoperative conversion or procedural modification resulting in the exclusion of cefazolin as the recommended first-line agent.
Recommendations for institutional prophylaxis
Procedures for which cefazolin was recommended as first-line prophylaxis were those described as such by the Japanese guidelines for perioperative antimicrobial prophylaxis 10 and the corresponding, institutional prophylaxis protocol. The latter dictates the use of clindamycin or vancomycin as an alternative, prophylactic regimen when a beta-lactam allergy label is present.
Data elements and definitions
The study center uses a commercial EHR system (HOPE/EGMAIN-GX, Fujitsu, Japan). Antibiotic allergy labels are entered into a dedicated allergy module that records the causative drug (selected from a list of drug names) and a free-text description of the reaction details. Structured fields for timing and severity are available but not mandatory, and the module does not distinguish immune-mediated allergies from nonallergic adverse drug reactions at the time of entry.
The term, “antibiotic allergy label” was used to refer to any antibiotic agent recorded in the allergy module regardless of whether the recorded event represented a true, immune-mediated allergy or a nonallergic adverse reaction. The following information was extracted from each label: (1) causative antibiotic agent or drug class; (2) symptoms and findings; (3) timing of symptom onset (categorized as <10 yr, ≥10 yr or unknown); (4) evidence of clinical assessment by a physician (ie, any documentation indicating a review or reinterpretation of the label); (5) record of a specialist’s evaluation (consultation with a dermatologist or infectious diseases specialist to evaluate the label, including documentation of assessment items, whenever available); and (6) perioperatively administered antibiotic agents.
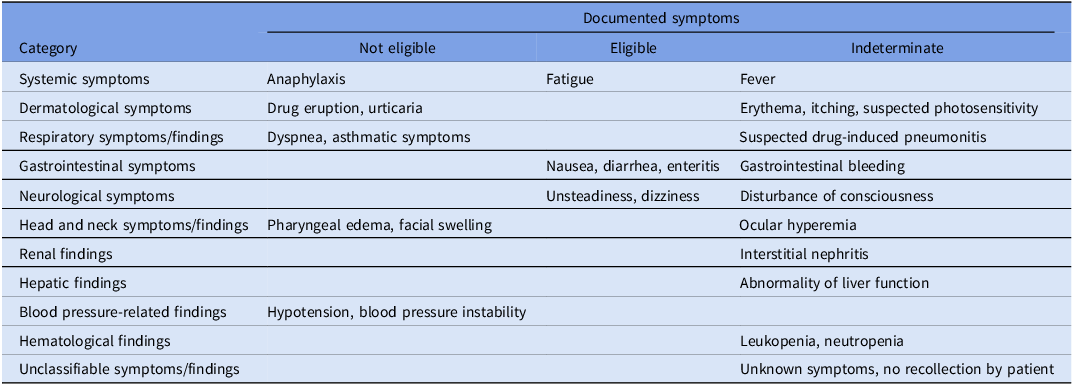
Symptoms and findings were categorized a priori into clinically meaningful groups, and eligibility for re-administration was assessed on the basis of the documented symptoms and findings: (1) not eligible, reactions indicating a severe, immune-mediated mechanism (eg, an immediate hypersensitivity reaction to a cephalosporin or penicillin, or a severe cutaneous adverse reaction); (2) eligible, a reaction attributable only to antibiotics other than cephalosporins and penicillins, or nonspecific intolerance to cephalosporins or penicillins unlikely to represent a severe, immune-mediated mechanism; and (3) indeterminate, cases in which the mechanism or severity could not be determined from the medical record alone. Table 1 shows the detailed mapping by category.
Registered symptoms, classification of antimicrobial allergies and adverse effects, and criteria for re-administration

Outcomes
The primary outcomes were the proportions of labels documenting the reaction phenotype and documenting timing or recency. Secondary outcomes were the proportions of labels documenting clinical assessment, the proportion of patients receiving specialist evaluation, and labeled patients receiving perioperative cefazolin. Clinical outcomes included surgical site infection (SSI) within 30 days, Clostridioides difficile infection (CDI) within 90 days, and perioperative adverse drug reactions.
To assess the potential effect of labeling on the choice of prophylactic agent, the use of non-first-line prophylaxis was evaluated in patients with labels limited to (1) cephalosporins, (2) penicillins, and (3) both cephalosporins and penicillins.
Statistical analysis
Descriptive statistics were used for analysis. Categorical variables were expressed as a number and a percentage, and continuous variables were expressed as the median and a range. All analyses were performed at the patient and label levels, as appropriate. This study was approved by the Institutional Review Board of Institute of Science Tokyo Hospital (approval number M2024-035). The requirement for patient consent was waived in accordance with the Declaration of Helsinki because the study was retrospective. This study was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Results
Patient characteristics
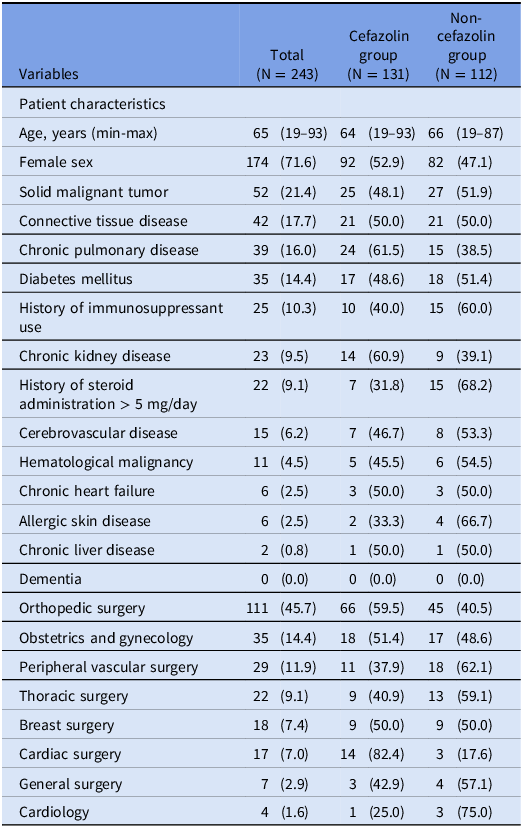
During the study period, 2,402 adult patients underwent a procedure in one of the eight included departments, of whom 253 (10.5%) had antimicrobial allergy labels. Of the 2,402, 1,981 (82.5%) underwent a procedure for which the institutional protocol recommended cefazolin as first-line perioperative prophylaxis. After excluding patients aged <18 years and those whose regimen was changed due to intraoperative conversion or substantial procedural modification, 243 patients (10.1%) remained for the final analysis. The median age was 65 years (range: 19–93), and 174 (71.6%) were female. The most common underlying conditions were solid malignancies (21.4%), autoimmune diseases (17.7%), and chronic lung diseases (16.0%) (Table 2).
Demographic data of patients with registered antimicrobial allergies

Details of antibiotic allergies
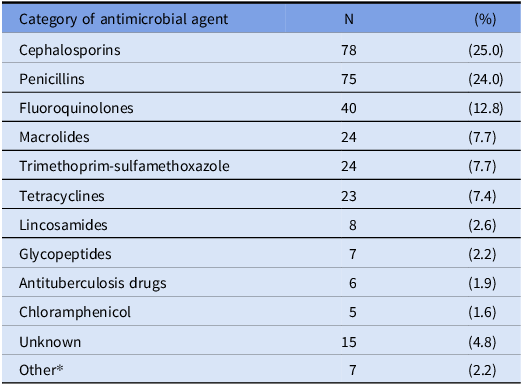
In total, 312 antimicrobial agents were registered in the 243 patients, with the median being one registered agent per patient (range: 1–8) (Table 3). The most frequently recorded antibiotic classes were cephalosporins (78/312; 25.0%) and penicillins (75/312; 24.0%), followed by fluoroquinolones (40/312; 12.8%). Third-generation agents accounted for the largest proportion of the cephalosporin labels (35/78; 44.9%), followed by first-generation agents (29/78; 37.1%) and fourth-generation agents (5/78; 6.4%); the remainder consisted of other cephalosporins.
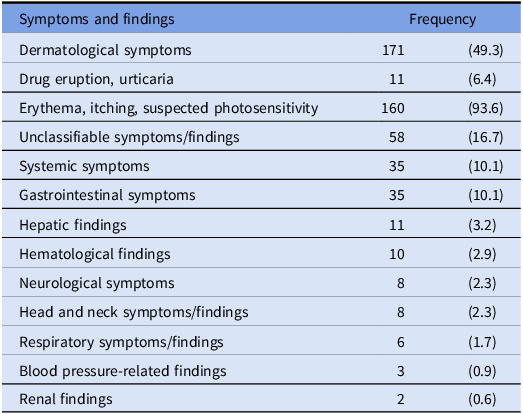
In total, 347 symptoms were recorded for the 312 registered antimicrobial agents (Table 4). Dermatological symptoms were the most common (171 events, 49.3%), with reactions suggesting a severe immune-mediated mechanism, including drug eruption and urticaria, in 11 cases (6.4%); these were followed by systemic (35; 10.1%) and gastrointestinal symptoms (35; 10.1%). A substantial proportion lacked details (eg, “unknown” or “no recollection”; 57 registrations, 16.7%), hampering risk stratification. Anaphylaxis was documented in 17 patients (5.5%). Documentation of timing and recency was frequently incomplete: symptom onset was not documented for 233/312 labels (74.7%), and where available, was within 10 years for 41/312 (13.1%) and ≥10 years for 38/312 (12.2%).
312 antimicrobial agents registered as those of an antimicrobial allergy (multiple entries allowed) in the 243 patients

* Other categories included carbapenems in 3 patients (1.0%); fosfomycin in 2 patients (0.6%); aminoglycosides and nitroimidazoles in 1 patient each (0.3%).
347 Symptoms and findings registered as an antimicrobial allergy (multiple entries allowed) in the 243 patients

Note: Data are presented as a number (%) unless otherwise specified.
Clinical assessment by a physician was documented in only 28/312 labels (9.0%). Assessments by a specialist were uncommon: documentation of dermatological consultations for the pre or postoperative assessment of antibiotic allergies was available for 15/243 patients (6.2%), and documentation of consultations with an infectious diseases specialist was available for 2/243 patients (0.8%).
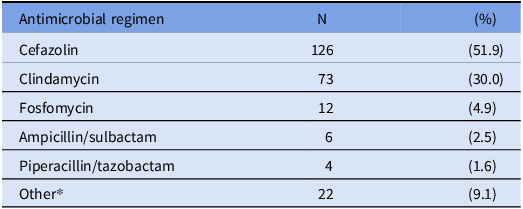
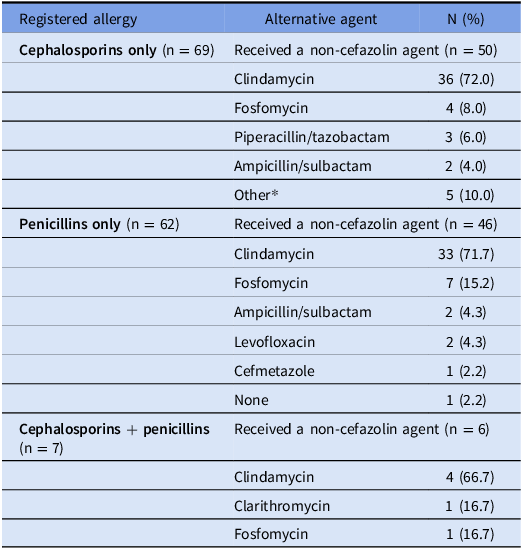
Among the patients with a registered antimicrobial allergy, the most frequently administered, perioperative antimicrobial agent was cefazolin (126 patients; 51.9%), followed by clindamycin (73 patients; 30.0%) and fosfomycin (12 patients; 4.9%) (Table 5). Non-first-line prophylaxis was frequently used even in the patients with only a penicillin label. Among 69 patients with only a cephalosporin label, non-cefazolin prophylaxis was administered to 50 patients (72.5%). Of 62 patients with only a penicillin label, non-cefazolin prophylaxis was administered to 46 patients (74.2%). In seven patients with a label limited to a penicillin and a cephalosporin, non-cefazolin prophylaxis was administered to six patients (85.7%). (Table 6). In this study, patients with a history of immunosuppressant use, history of steroid administration >5 mg/day, and allergic skin disease were more common in the group that did not receive cefazolin for perioperative prophylaxis (40.0% vs 60.0%, 31.8% vs 68.2%, and 33.3% vs 66.7%). Reactions to each antimicrobial agent recorded in the 243 patients were assessed using prespecified criteria for re-administration. Overall, 106 patients (43.6%) were classified as eligible, 24 (9.9%) as not eligible, and 113 (46.5%) as indeterminate. As clinical outcomes, we observed no SSI or CDI. However, perioperative adverse drug reactions were observed in 7 patients; dermatological symptoms in 5 patients (71.4%), followed by blood pressure-related events in 1 patient (14.3%) and hematological events in 1 patient (14.3%).
Antimicrobial agents actually administered during the perioperative period in patients with a documented allergy (N = 243)

* Other regimens included levofloxacin in 3 patients (1.2%); cefazolin + clindamycin; cefazolin + vancomycin in 2 patients each (0.8%); vancomycin; ceftriaxone; cefepime; meropenem; ampicillin; clarithromycin; cefmetazole; piperacillin; aztreonam + vancomycin; vancomycin + meropenem; ceftriaxone + vancomycin; cefepime + vancomycin; daptomycin + cefazolin; clindamycin + gentamicin; and none in 1 patient each (0.4%).
Alternative antimicrobial agents administered perioperatively in patients with a registered cephalosporin or penicillin allergy

* Other agents included levofloxacin; ampicillin; cefepime; ceftriaxone + vancomycin; aztreonam + vancomycin in 1 patient each (2.0%).
Discussion
This retrospective, single-center study evaluated the prevalence and characteristics of antibiotic allergy labels in the EHR, as well as the extent of the clinical assessment of these labels in patients in a Japanese university hospital undergoing a procedure for which cefazolin was recommended as the first-line perioperative prophylactic agent. Approximately 10% of the eligible patients had an antibiotic allergy label. Cephalosporins were the most frequently labeled class, followed by penicillins and fluoroquinolones. Among the patients with an antibiotic allergy label, roughly half received a cefazolin; however, an alternative agent was used in the remaining cohort. Clindamycin was the most common alternative, and cefazolin was often avoided even in patients labeled as having an allergy only to penicillin. The quality of the documentation was suboptimal, and both primary-team assessment and specialist consultation for allergy evaluation in this group were infrequent.
The prevalence of antibiotic allergy labels in this study (10.1%) was comparable to previous reports of self-reported penicillin allergy in other countries (approximately 8%) Reference Macy11 and the findings of a previous, Japanese, single-center study of patients who had received infectious diseases consultation (approximately 13%). Reference Adachi, Katayama and Tanaka12 The predominance of cephalosporin labels was also consistent with Japanese data on pregnant patients. Reference Hirai, Ishikawa and Takeda13
Our findings highlighted the frequent use of clindamycin as an alternative to cefazolin for perioperative prophylaxis. The Japanese guidelines recommend clindamycin or vancomycin as alternatives for patients with a beta-lactam allergy label. 10 In our cohort, clindamycin was administered to approximately 70% of patients with a penicillin and/or cephalosporin allergy label, suggesting it is widely perceived as a standard substitute with perioperative timing and workflow similar to cefazolin. However, current evidence indicates that cross-reactivity between penicillins and cephalosporins is substantially lower than historically assumed, especially when side-chain structures differ. Reference Campagna, Bond, Schabelman and Hayes14 Cefazolin in particular is structurally distinct from many other beta-lactam agents and is considered to have a low risk of cross-reactivity based on side-chain considerations. Reference Trubiano, Stone and Grayson15 Importantly, the use of non-first-line alternatives (including clindamycin and/or vancomycin) in patients labeled penicillin-allergic has been associated with a higher rate of SSI. Reference Norvell, Porter and Peck16 When eligibility for re-administration was assessed from the recorded symptoms, approximately 40% of cases were likely eligible. These data suggest that systems enabling appropriate identification of patients who can safely receive cefazolin could improve both antimicrobial stewardship and patient outcomes. Because the cohort also included patients with allergies to antimicrobials other than beta-lactams, physicians may have individually reviewed the allergy history before selecting cefazolin.
This study also identified limitations in EHR functionality and workflow: allergy labels and nonallergic adverse drug reactions were not clearly distinguishable in the EHR, raising the possibility that nonallergic events were recorded as an allergy, leading to unnecessary avoidance of first-line agents. In addition, key elements required for risk stratification—the identity of the causative agent, details of the reaction phenotype, and timing—were frequently missing, making subsequent clinical assessment challenging, as also noted in previous studies. Reference Moskow, Cook and Champion-Lippmann7,Reference Shenoy, Macy, Rowe and Blumenthal8 These findings underscore the need to improve both EHR design and local documentation practices, such as standardizing entry of causative agents, recording reaction details, and establishing a chronology of events. Patients with a history of immunosuppressant use, steroid administration >5 mg/day, or allergic skin disease were significantly more common in the group that did not receive cefazolin. Atopic predisposition has been reported as a predictor of hypersensitivity reactions to beta-lactam antimicrobials, and clinicians may have avoided cefazolin in light of these findings; however, the extent to which they are recognized in routine clinical practice remains unclear. Reference Epstein-Rigbi, Ziv, Bulanenkova, Bouganim, Tal-Jasper and Marchaim17 Additionally, allergy labels were also more common in women than in men; previous studies have similarly reported that antimicrobial allergy labels, particularly beta-lactam labels, are more frequent among female patients, which may have contributed to the higher proportion of women in this cohort. Reference Park, Matesic, Markus and Li18
Recent studies have reported that structured assessment and de-labeling interventions led by trained clinicians (including pharmacists and physicians) can improve the quality of allergy documentation and increase the appropriate use of beta-lactam agents. Reference Turner, Wrenn and Sarubbi19 The Centers for Disease Control and Prevention’s Global Antibiotic Stewardship Evaluation Tool also positions antibiotic allergy assessment as an important component of inpatient antimicrobial stewardship. 20 Establishing a feasible, context-appropriate evaluation pathway, potentially involving an allergy assessment team, may therefore be a key step in improving the accuracy of antibiotic allergy information and optimizing perioperative prophylaxis. In particular, preoperative assessment clinics provide an effective opportunity to reassess and remove inappropriate penicillin allergy labels before surgery, and pharmacist-led interventions have been reported to enable de-labeling in a larger number of patients. Reference Wade and Marshall21
This study has several limitations. First, it was a retrospective analysis at a single academic hospital; thus, its findings may not be generalizable to other settings in Japan. Second, the cohort was restricted to patients undergoing a procedure for which cefazolin was recommended as first-line prophylaxis; patterns may differ for other procedures and specialties. Third, because the EHR allergy module could not distinguish allergic reactions from other adverse events, the proportion of genuine, immunologically mediated allergies could not be determined. Finally, the clinical appropriateness of each perioperative regimen was not directly evaluated at the individual patient level, as the labeled antibiotics included agents other than cefazolin.
In conclusion, antibiotic allergy labels in the EHR were often incomplete and infrequently assessed, partly due to the avoidance of first-line prophylaxis in a substantial proportion of the cohort. Improving the design of EHR to enable allergies to be distinguished from nonallergic adverse events; standardizing the documentation format; and implementing a clinically workable assessment pathway may increase appropriate cefazolin use, advance antimicrobial stewardship, and potentially improve patient outcomes.
Acknowledgments
We thank James R. Valera for his assistance with editing this manuscript.
Author contribution
YE and YT designed the study protocol and drafted the first version of the manuscript. YE collected and analyzed the clinical data and composed the figures. KO revised the manuscript, and all the authors contributed to the final version of the manuscript for submission.
Financial support
None.
Competing interests
The authors declare no conflicts of interest and have submitted the ICMJE form for the Disclosure of Potential Conflicts of Interest.

 Open access
Open access