


Introduction
Acute care cardiology is a relatively new subspecialty within the field of paediatric cardiology, though it has grown rapidly in recognition and adoption since inception of the Paediatric Acute Care Cardiology Collaborative (PAC3). PAC3 was established in 2014 with aim of improving the quality, value, and experience of inpatient cardiac care outside of the ICU. The structure and practices of early adopters of the acute care cardiology model were previously described based on findings of the initial PAC3 Hospital Survey in 2017. Reference Hoerst, Bakar and Cassidy1 However, since this comprehensive description, the growth and continued variability of acute care cardiology practice across North America have not been formally reassessed.
The initial PAC3 Hospital Survey included data from 31 North American PAC3 institutions. As of March 2025, there are 50 North American PAC3 member centres, a 60% increase since inception. PAC3 supports collaborative learning and improvement through its clinical data registry, quality improvement work, educational programming, and professional society for acute care cardiology providers, nurses, and ancillary staff.
The PAC3 Hospital Survey has been conducted four times on a biennial basis. The survey’s goal is to identify practice variation across disciplines important to acute care cardiology, as PAC3 nears its 10-year anniversary of supporting the field. We aim to share the current state of acute care cardiology and highlight notable changes in the specialty since the initial report in 2017. Finally, with this current work, we have identified important data points that may inform further quality improvement in our field.
Materials and methods
A panel of PAC3 members with diversity of institution geography, programme size and type, and pediatric cardiology content expertise was convened in Fall 2022 to design this survey. Survey authors reviewed the prior PAC3 Hospital Survey to assess for continued relevance and clarity of questions. Questions were removed if no longer relevant, revised for clarity or data granularity, or added for additional data capture.
The PAC3 Hospital Survey 4.0 was ultimately comprised of eight sections with 214 total stem questions. With branching logic, the survey includes a total of 454 fields. There were seven previously established sections including Demographics, Staffing, Resources and Therapies, Transitions and Escalations in Care, Standards of Care, Discharges, Quality improvement, and a new section for Equity, Diversity, and Inclusion.
The survey was administered to clinical champions at participating PAC3 centres between September and December 2023 via REDCap. Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2 Only one survey was completed per centre, though clinical champions were encouraged to discuss the questions with members of the multidisciplinary team to provide the most accurate representation of their centre’s practices. The survey required approximately 60 minutes to complete. Missing data fields were reconciled by the PAC3 project coordinator who contacted individual centres to clarify questions and obtain the response that most closely reflected their centre’s practices.
Basic statistical analysis was performed. Categorical variables were summarised as frequencies and percentages and compared using chi-square or Fisher’s exact test. Continuous variables were reported as medians with interquartile ranges and compared using the Wilcoxon rank-sum test or Kruskal–Wallis test. All statistical tests were two-sided, with significance defined as p < 0.05. McNemar’s test was used to compare paired binary outcomes between survey versions. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC). Changes over time were assessed only relative to centres who answered both the 2017 and 2023 survey.
Results
There were 47 centres that participated in this 2023 edition of the Hospital Survey, representing a 100% response rate of PAC3 member centres at time of survey administration. This is an increase of 16 centres compared to the 2017 report, with 94% of those centres included again in 2023 (29/31).
Demographics
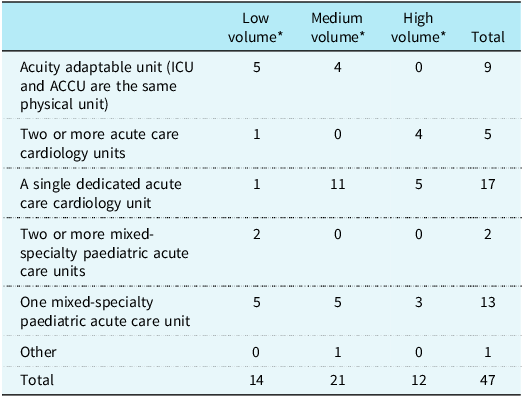
Unit composition showed diversity in care models across the collaborative (Table 1). The number of acute care cardiology beds varied widely between centres, with a median of 24 (interquartile range 15–32). The largest number of acute care beds at a given centre was 54. Centres report that most rooms are private (40, 85%), have their own restroom (45, 96%), and all have the ability for a parent to sleep overnight (47, 100%). Most (35, 74%) acute care units are near the cardiac ICU with 13 contiguous with ICU (28%), 19 on the same floor (40%), and 3 within one floor (above or below) the cardiac ICU (6%). The median number of admissions to acute care units within the collaborative during 2023 was 707 (interquartile range: 517, 1077). Medicaid was the insurance provider for 50% of patients in most (27, 57%) centres.
Acute care cardiology unit (ACCU) composition, 2023

Table 1 Long description
The table presents the composition of acute care cardiology units across various centers in 2023, categorized by low, medium, and high volume. It includes five unit types: acuity adaptable unit, two or more acute care cardiology units, a single dedicated acute care cardiology unit, two or more mixed-specialty pediatric acute care units, and one mixed-specialty pediatric acute care unit. The table has five rows and four columns, with column headers being Low volume, Medium volume, High volume, and Total. Row 1: Acuity adaptable unit (ICU and ACCU are the same physical unit) with 5 in low volume, 4 in medium volume, 0 in high volume, and a total of 9. Row 2: Two or more acute care cardiology units with 1 in low volume, 0 in medium volume, 4 in high volume, and a total of 5. Row 3: A single dedicated acute care cardiology unit with 1 in low volume, 11 in medium volume, 5 in high volume, and a total of 17. Row 4: Two or more mixed-specialty pediatric acute care units with 2 in low volume, 0 in medium volume, 0 in high volume, and a total of 2. Row 5: One mixed-specialty pediatric acute care unit with 5 in low volume, 5 in medium volume, 3 in high volume, and a total of 13. The final row shows the totals: 14 in low volume, 21 in medium volume, 12 in high volume, and a grand total of 47. The table highlights the diversity in care models and the distribution of acute care cardiology beds across different centers.
*Based on total cardiac admissions in 2022; Low: 600, Medium: >600–900, High: >900.
Admission to the acute care cardiology unit requires a cardiac indication or specific cardiac diagnosis in most centres (39, 83%). Most (25, 53%) have policies regarding admission criteria for the acute care cardiology unit, with indications including: recent cardiac surgery (32, 68%), single ventricle physiology regardless of stage (31, 66%), systemic to pulmonary artery shunts and single ventricle physiology prior to stage 2 (36, 77%), single ventricle physiology prior to stage 3 (32, 68%), unrepaired moderate to large post-tricuspid shunts (26, 55%), unrepaired cyanotic heart disease (37, 79%), repaired with haemodynamically significant residual lesions (36, 77%), heart transplant (29, 62%), and ventricular assist device (27, 57%). Few centres (5, 10%) aimed to admit all acute care level patients with CHD to the acute care cardiology unit. Patients with observation status after same-day procedures (i.e. cardiac catheterisation) are commonly admitted to the acute care cardiology unit (38, 81%).
Pulmonary hypertension patients are admitted to the acute care cardiology unit in most centres (33, 70%), most often under the general cardiology service (31, 66%) with a pulmonary hypertension consultation available in 23 centres. A primary pulmonary hypertension team exists in six centres under either cardiology or pulmonology.
Heart transplants were performed at most PAC3 centres (44, 94%). These patients are almost universally permitted to be admitted to the acute care cardiology unit (42, 96%) with a specialty transplant service as the primary provider at 28 (60%) centres, under the general cardiology team in 13 (28%) centres, and on the cardiothoracic surgery team post-operatively in one (2%) centre. Dual organ transplants were offered at 20 (43%) of PAC3 centres with heart combined with kidney (16 centres), liver (13 centres), lung (eight centres), or bowel (two centres).
The care of acute care cardiology unit patients varies widely: 20 (43%) centres reported acute care cardiology unit patients are routinely admitted to the unit, 12 (26%) centres have restrictions based on diagnosis, and seven (15%) refer all adult patients to adult facilities.
Staffing: physicians and advanced practice providers
Acute care cardiology units utilise multidisciplinary teams to care for their patients, including attending physicians, advanced practice providers, hospitalists, fellows, and residents. There is an average of 9.8 attendings per centre in the pool for weekday coverage (13.6 for weekend coverage). The average number of service weeks per attending is 8 weeks (range: 1–26). Very few centres (3, 6%) employ an in-house attending overnight, only one of which utilises an acuity adaptable model.
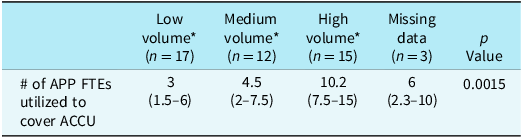
A minority of programmes utilise hospitalists without formal cardiology training (8, 17%), while most utilise advance practice providers (41, 87%) to provide frontline care for acute care cardiology unit patients. Centres average 6.8 acute care cardiology-dedicated advance practice provider full time equivalents (range: 1–23), however when evaluated by centre volume there are significant differences in dedicated full time equivalent (Table 2). Most centres’ acute care cardiology advance practice providers are dedicated to the acute care cardiology unit without clinic or consult responsibilities (27, 57%). Most centres utilise cardiology fellows in their care model (34, 72%), and 22 programmes have a fellow in-house on weeknights while 19 programmes have a fellow in-house on weekend nights. 79% of centres utilise residents as front-line providers (37), with half utilising upper-level paediatric residents and the other half using interns. Residents care for all acute care cardiology unit patients in 61% of programmes, whereas 18% exclude postoperative patients and 8% exclude heart failure patients. Overnight front-line provider coverage is primarily by paediatric residents (31, 66%), whereas fewer centres utilise advance practice providers (16, 34%), fellows (10, 21%), and hospitalists (4, 9%).
Advance practice provider full time equivalent (FTE) by centre volume

Table 2 Long description
The table presents data on the number of advance practice provider full-time equivalents (FTEs) utilized to cover the acute care cardiology unit (ACCU) across different center volumes. It includes four columns: Low volume, Medium volume, High volume, and Missing data, with corresponding FTE ranges. The Low volume centers (n=17) utilize 3 FTEs (range 1.5-6), Medium volume centers (n=12) utilize 4.5 FTEs (range 2-7.5), and High volume centers (n=15) utilize 10.2 FTEs (range 7.5-15). Missing data for 3 centers show a range of 2.3-10 FTEs. The p-value for this data is 0.0015, indicating significant differences in FTE utilization based on center volume.
APP: advance practice provider; FTE: full-time equivalent.
*Based on total cardiac admissions in 2022; Low: 600, Medium: >600–900, High: >900.
Staffing: nursing and multidisciplinary staff
Most centres (70%) use a 3:1 nursing ratio with flexible ratios based on patient acuity (42, 89%), and with the addition of a resource nurse in 27 centres (57). Some centres (12, 26%) have a fully cardiac ICU cross-trained nursing staff; of these, 7 utilise an acuity adaptable model of care. Many types of multidisciplinary staff/services are available at most centres (Figure 1).
Multidisciplinary staff utilization across participating centers. Pharm: pharmacist; RD: registered dietician; RT: respiratory therapist; OT: occupational therapist; SLP: speech language pathologist; SW: social worker.

Figure 1 Long description
The bar graph compares the utilization of various multidisciplinary staff across participating centers. The x-axis lists different staff roles, including Vascular Access, Pain Service, Pharm, RD, Lactation, RT, PT, OT, SLP, Case Manager, SW, Chaplain, Psychologist, and Interpreter. The y-axis represents the percentage of staff utilization, ranging from 0% to 100%. The graph uses a stacked bar format with four colors: teal for staff dedicated to the unit, red for staff shared with other cardiac services, purple for staff shared with other units, and blue for staff not available. Each bar is divided into segments representing the percentage of staff in each category. Notable trends include high utilization of Vascular Access and Pain Service staff dedicated to the unit, while roles like Interpreter and Psychologist show significant portions of staff shared with other units or not available. The color scheme effectively differentiates the various categories of staff utilization.
Resources and therapies
Certain resources and therapies on are of variable presence on acute care cardiology units. Centres with dedicated acute care cardiology units administer high-risk medications more often than centres with acuity adaptable or mixed-specialty non-cardiac acute care models (Figure 2A). When evaluating inotropes specifically, acute care cardiology units offer more types of inotropic support than acuity adaptable and mixed specialty units (Figure 2B), though there was no statistical difference in the number of each type of centre offering each medication (p > 0.05).
Variation in use of medications. iNO: inhaled nitric oxide; IV PC: intravenous prostacyclin; SQ PC: subcutaneous prostacyclin; Inh PC: inhaled prostacyclin; Anti-Arrh: anti-arrhythmic medications; Sys. Vasodil: systemic vasodilators.

Figure 2 Long description
The image contains two bar graphs. The first bar graph, titled 'Medication Use by Center Type,' compares the use of various medications across three types of centers: Mixed Specialty Acute Care Unit, Acute Care Cardiology Unit, and Acuity Adaptable Unit. The medications include iNO, IV PC, SQ PC, Inh PC, Anti-Arrh, Sys. Vasodil, PGE, and Inotrope. The second bar graph, titled 'Inotropic Medications by Center Type,' focuses specifically on the use of inotropic medications across the same three center types. The inotropic medications include Combined Infusions, Epinephrine, Dobutamine, Dopamine, and Milrinone. Each bar represents the frequency of medication use, with different colors indicating different medications. The graphs show variations in medication use across different center types, highlighting differences in clinical practices.
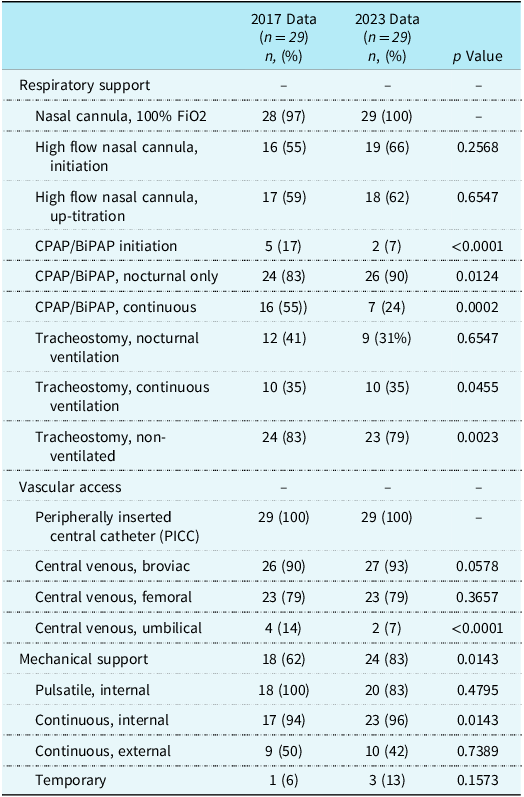
Equipment availability is variable as well and relatively stable since the initial Hospital Survey in 2017 (Table 3). Importantly, there was a significant increase in the number of centres using ventricular assist devices (VADs) on the acute care cardiology unit (18 versus 24; p = 0.01) between 2017 and 2023. However, of the entire 2023 cohort, only 31 (66%) centres provide VAD therapy on the acute care cardiology unit.
Variation in equipment availability on the ACCU, 2017 versus 2023

Table 3 Long description
The table compares equipment availability on the acute care cardiology unit (ACCU) between 2017 and 2023. It includes data for 29 centers in each year, focusing on respiratory support, vascular access, and mechanical support. Key trends include increased use of high flow nasal cannula, CPAP/BiPAP, and mechanical support. Notable changes are observed in the use of tracheostomy for ventilation and non-ventilated cases. Vascular access methods such as peripherally inserted central catheters (PICC) and central venous lines are also detailed. Mechanical support data includes the use of pulsatile and continuous internal and external support devices.
When considering monitoring of acute care cardiology unit patients, nearly all units provide centralised heart rhythm (98%) and pulse oximetry (91%) monitoring. Approximately half (53%) of acute care cardiology unit’s have monitor alarms sent electronically to the bedside nurse, typically (84%) with an algorithm to escalate alarms that are not acknowledged by the bedside. Only 40% of centres have monitoring systems that are staffed continuously without interruption; of these, the system is staffed by nurses with additional training in rhythm detection in 16%, nurses without such additional training in 16%, and technicians trained in rhythm detection in 63%. Few acute care cardiology units (12, 26%) provide near-infrared spectroscopy monitoring.
Standards of care
Protocolised or standardised care models are commonly used in healthcare to reduce practice variation, decrease human error, and improve outcomes. Reference Elwadhi, Panda and Tyagi3,Reference Balamuth, Weiss and Fitzgerald4 However, only one-third of responding centres (16, 34%) reported having written pathways or protocols for postoperative care after benchmark cardiac procedures. Among these, there are differences related to which lesions or procedures have protocolised care; single ventricle palliation postoperative care is the most likely to be protocolised (Norwood 13, 57%; Glenn 12, 52%, Fontan 16, 100%). Of centres that utilise protocols, a minority audit adherence to these protocols (6, 38%). Many centres indicate a high level of consistent practice related to postoperative testing despite lack of a written protocol, but do not track the frequency/timing of postoperative chest radiography, echocardiography, electrocardiography, and laboratory evaluations.
There is significant variability in pacing wire removal with 57% of centres (27) without standardisation. Contrastingly, chest tube removal is more consistent across the collaborative, with only 18 centres (38%) indicating lack of standardisation. Several other topics were assessed with regard to protocolisation, defined as a written accessible document or a process driven by shared order sets, versus standardisation, defined as a practice used 95% of the time without a written policy (Figure 3). Notably, transition in care of these clinical issues from the acute care cardiology unit to outpatient settings is not commonly addressed within protocols.
Prevalence of written protocols and standardized practices utilized 95% of the time. NEC: necrotizing enterocolitis; VAD: ventricular assist device.

Figure 3 Long description
The bar graph titled Prevalence of Protocols and Standard Practice compares the prevalence of written protocols and standard practices across various medical procedures. The x-axis represents the percentage prevalence, ranging from 0 to 40. The y-axis lists different medical procedures, including Diuretics, Fontan Complications, Pain Management, Hematochezia/NEC, Heart Failure, Lesion Specific Pathway, Pulse Loss, Chest Tube Removal, VAD, Infant Feeding, Single Ventricle, and Chylothorax. Each procedure has two horizontal bars: one for written protocols in blue and one for standard practices in red. The graph shows that Single Ventricle and Chylothorax have the highest prevalence of both written protocols and standard practices, while Diuretics have the lowest. Notable trends include a higher prevalence of standard practices compared to written protocols for most procedures. All values are approximated.
Escalations and transitions of care
There is variability in how patients transition from the cardiac ICU to the acute care cardiology unit, and how they are monitored for escalated care needs. When transferring care from the cardiac ICU, a minority of centres use written processes for care handoff (13, 28%). Of these, the most common included topic is personnel involved, whereas checklists for communication, documentation processes, time of day, and location are less commonly specified. Communication for transfer of care is rarely according to a script (7, 15%) or checklist (2, 4%) and more likely to occur by organ system (19, 40%) or variable delivery (19, 40%). Front-line providers from the acute care cardiology unit and cardiac ICU are the most common personnel present at handoff of care, followed by acute care cardiology unit and cardiac ICU attending physicians. Nursing handoff commonly occurs separate from medical team sign out (35, 75%). Very few centres have specific protocols or criteria addressing transfer readiness (5, 11%), though more reported standard practices (15, 32%).
Most centres (28, 60%) employ early warning scoring systems to predict clinical deterioration, and most have a mechanism to identify at-risk patients (32, 68%). For these at-risk populations, 47% (15) have formal, population-specific protocols. Cardiac rapid response teams are present in most centres (29, 62%), and include cardiologists, respiratory therapists, and nurses at all centres. Nearly all centres (97%) perform reviews of rapid response teams to assess clinical effectiveness and patient safety. Most centres have separate processes to review emergent transfers to the cardiac ICU (71%) and cardiac ICU readmissions (56%).
Discharge
One of the most important transitions in care for acute care cardiology unit patients is the transition to home. Roughly half of participating centres allow chest tube and pacing wire removal (49% and 53%, respectively) on the day of discharge. All centres require a pre-discharge echocardiogram for postoperative patients, and fewer require discharge electrocardiograms (72%). Most centres (91%) allow for discharge with nasogastric tubes in place, but only 74% of these centres allow for interstage infants to discharge with an nasogastric tube. Many fewer centres discharge with nasoduodenal tubes (43%) or with total parenteral nutrition (49%).
Family education processes are variable. Few centres (23%) provide medication education to all acute care cardiology unit patients and families upon discharge. Education for specific medications is more common (15, 32%), including anticoagulation (12), immunosuppression (10), anti-arrhythmic medications (7), neurosedation (5), and medications in the setting of polypharmacy (>6 medications; 5). Cardiopulmonary resuscitation education is provided to all patients and families in 34% of centres and to select patients at 57% of centres. Most (87%) centres provide specific newborn care education when discharging home from the acute care cardiology unit for the first time after birth. Car seat testing is performed in 70% of centres, though elements of such testing are unknown (i.e. cardiorespiratory monitoring during testing, duration of testing) based on available survey data. Discharge education is provided by a variety of roles (Figure 4).
Variable disciplines of providers of discharge education across participating centers.

Figure 4 Long description
The bar graph compares the number of providers of discharge education across different categories. It features six vertical bars, each representing a different category of providers. The x-axis lists the categories: Bedside R N, Discharge Educator, Discharge Class Teacher, Care Managers, Frontline Provider, Attending, and Other. The y-axis indicates the number of providers, ranging from 0 to 50. The Bedside R N category has the highest number of providers at 46, followed by Frontline Provider at 38. Attending has 22 providers, Care Managers have 18, Discharge Educator has 16, and Discharge Class Teacher has 10. The Other category has the fewest providers at 6. All values are approximated.
Family engagement around discharge can be fostered by rooming-in, which is quite variable. Most centres (83%) require a period of rooming-in for “select” patients, most commonly interstage patients (30, 64%), complex care patients (19, 40%), those with new medical equipment (12, 26%), and those with “social concerns” (12, 40%). Finally, 21 centres perform post-discharge calls to assess patient and family re-assimilation to the outpatient environment (45%). Of these, 11 centres call all families (52%).
Quality improvement
PAC3 continues to have a strong emphasis on quality improvement with a well-described improvement structure that is shared with Cardiac Networks United. Reference Bates, Madsen and Lyren5 Most centres (37, 78%) have a dedicated quality improvement director within the heart centre; 26 centres (55%) describe additional support from the institution outside of heart centre efforts. When asked if “existing data sources allow us to easily pull data needed for quality improvement,” 27 (57%) centres responded positively (somewhat agree or agree); however, most (40, 85%) report employing staff dedicated to the collection and analysis of data for quality improvement work. 26 (55%) centres describe multidisciplinary teams for most/all quality improvement projects.
Multiple support mechanisms exist within PAC3 for quality improvement. Regarding quality improvement initiatives in the past 2 years that utilised PAC3 resources, 34 (72%) centres used registry data, 24 (51%) used networking opportunities, and 18 (38%) participated in conferences, among other offerings. To date there have been 5 multicentre quality improvement initiatives sponsored by PAC3 and 34 (72%) centres reported actively participating or adapting local improvement efforts based on these projects. 35 (74%) “agree” or “strongly agree” PAC3 provides important quality improvement resources and training.
Equity, diversity, and inclusion
Most centres have an institution-wide equity, diversity, and inclusion committee (45, 96%), with far fewer heart centre-specific committees (11, 23%). More commonly, there is a heart centre equity, diversity, and inclusion champion/sponsor/representative or equivalent (16, 34%). Acute care cardiology unit-specific equity, diversity, and inclusion champions are rare (5, 11%). Active heart centre equity, diversity, and inclusion work is occurring in 18 centers (38%), with rarer acute care cardiology unit-specific work (8, 17%). A minority of centres are routinely reviewing their PAC3 data using race/ethnicity filters available on the reporting platform to evaluate for disparities (14, 30%).
Social determinants of health screening are common in heart centres (28, 62%), with 71% of those centres (20) performing this screening on the acute care cardiology unit. Limited English proficiency identification occurs at most centres (40, 85%), and in-person interpreter services are available universally, with video (45) and telephone (44) services also commonly available. Routine interpretation services are utilised most commonly for discharge instructions (44, 94%), teaching (43, 91%), clinical updates (41, 87%), admission processes (40, 85%), and least commonly during family-centered rounds (28, 60%). One-third of centres offer a written translation service (17, 36%).
Discussion
Significant variability exists in the practice of acute care cardiology related to unit structure, staffing models, equipment, resources, and more. When evaluating the evolution of factors important to acute care cardiology, there are several salient changes and a number of areas where expected change has not occurred. Most centres that participated in both (2017 and 2023) surveys kept the same unit structure and no centres shifted to an acuity adaptable model. It is important to note the diversity of unit structure of centres that have joined PAC3 since inception, specifically the addition of more acuity adaptable models and mixed specialty units since 2017. While admission criteria have largely stayed consistent since 2017, there has been an increase in dedicated heart transplant services on acute care cardiology units, and there has been a significant increase in the number of centres that provide VAD therapy on acute care cardiology units. Despite a generally acknowledged increase in the ACHD population, there was not a notable difference in the number of centres admitting these patients to paediatric acute care cardiology units in 2023.
Acute care cardiology unit staffing models, though relatively stable from prior surveys, are ripe for change. In 2023, acute care cardiology unit practice relied heavily on paediatric residents which is currently in jeopardy given the 2025 changes in Accreditation Council for Graduate Medical Education (ACGME) curricula. 6 Acute care cardiology practice will likely rely increasingly on advance practice providers and hospitalists to care for our patients, especially as front-line providers at night. Attending physician workforce composition is notable, with increasing recognition of the necessity of acute care cardiologists as distinct specialists due to the complexity of our patients, nature of inpatient care, emphasis on high quality of care to promote shorter length of stay (LOS), and aims for smooth transitions to outpatient care. Despite precedent in adjacent specialties such as hospital medicine and critical care, a clear definition of an “acute care cardiologist” remains lacking.
Finally, it is important to recall that the Hospital Survey has been administered every two years with results transparent to participating institutions. Yet only 19% of centres indicate impacts of PAC3 participation on the resources and therapies available in their acute care cardiology units. Interestingly, protocol presence does not reflect the same pattern. There is a high prevalence of protocols for chest tube management, which may be attributable to prior PAC3 work on the topic; Reference Bates, Connelly and Khadr7,Reference Sheth, Tignor and Connelly8 similarly, prevalence of chylothorax protocols may be attributable to other Cardiac Networks United work. Reference Lion, Winder and Amirnovin9 This raises several questions regarding the role of protocols on the acute care cardiology unit that may be different from physical resources and therapies. Are they most important for rare conditions where clinicians might have less experience? Or, are they more worthwhile for common situations where even slight practice variability will compound given frequency of the clinical event? Or, are they most important for clinical areas where multidisciplinary input is most important but difficult to achieve daily? Answers to these questions relative to this survey will aid acute care cardiologists and multicenter collaborators within PAC3 to determine next steps for protocol development and standardisation based in evidence or expert consensus.
Limitations
The PAC3 Hospital Survey is self-reported and not based on patient-level data. Thus, there is possibility of inherent bias from the survey respondents related to their views of the acute care cardiology unit. Based on survey methodology, there is no manner by which we can confirm answers.
Future work
Inherent in PAC3’s mission is a desire for continued improvement, and thus the answers to the Hospital Survey ignite ideas within the collaborative, and form the basis for upcoming interdisciplinary and multicenter work within the growing field of acute care cardiology.
Acute care cardiology units are heterogenous units that are becoming more common in paediatric hospitals. PAC3 will continue to facilitate discussion regarding unit characteristics (i.e. populations for admission, team structures, and unit locations) that promote the best outcomes for paediatric heart disease. Importantly, the staffing models of multidisciplinary teams required to care for our complex patient population vary widely across the collaborative. Though there is precedent in hospital medicine and critical care, Reference Fromme, Ruch-Ross, Marks, Barone and Shaugnessy10,Reference Ettinger, Loscalzo, Liu, Griffis, Mack and Agus11 there is no current definition of an attending full time equivalent in paediatric cardiology, much less acute care cardiology. Complicating this, most acute care cardiologists, even those who are primarily dedicated to inpatient acute care cardiology unit care, have other clinical duties such as outpatient clinic or echocardiography. Survey data stratified in multiple ways to assess factors like acuity and volume may allow PAC3 to contribute to defining a single full time equivalent in paediatric acute care cardiology. This survey also shows that acute care cardiology currently relies heavily on paediatric residents. However, given the recent changes in ACGME curricula for paediatric residents, 6 most centers will need to adapt team structure to provide safe care day and night. PAC3 as a multidisciplinary group can monitor any impacts to patient care quality and consistency.
While some resources and therapies have increased in availability on acute care cardiology units, others have become less common or remained stable. The optimal balance of resources for acute care cardiology has not been defined since patient populations, conditions treated, acuity, and staffing models are quite variable. The launch of the Hospital Survey Visualisation Dashboard in 2022 allows centers to transparently evaluate similar centers’ practices. Thus far, however, there have not been many notable changes in deployed resources and therapies on acute care cardiology units across the collaborative outside of increase in VAD use. PAC3 will continue to foster conversations between similar centers to share optimal systems and practices and understand barriers to expanding resource availability.
Wide variability in the presence of protocols for common diagnoses in acute care cardiology presents opportunities for PAC3 to support centres in standardising care informed by new clinical practice guidelines. While protocols must acknowledge differences in resources, compiling evidence-based approaches that meet the needs of many centre types is beneficial. PAC3 has begun protocol work with recent publication of a clinical practice guideline for pain management, Reference Gal, Clyde and Colvin12 with ongoing work regarding bacterial endocarditis, anticoagulation, and necrotising enterocolitis. PAC3’s culture of transparency and collaboration can accelerate improvement work. Impact of protocols should gauge staff burden, parental stress, cost, or iatrogenic harm, and evaluate for outcome disparities.
Finally, given that transitions in care are a vulnerable time for patients and families, we must use the information available within this survey to optimise these periods. Currently, there is no clear early warning score that meets the unique needs of acute care cardiology patients, and centres instead utilise scoring systems made for other patient populations. Creation and validation of an early warning system for acute care cardiology would have profound impacts when considering prevention of acute events outside of the ICU. Regarding transition to home, there are widely disparate practices and poorly defined, subjective populations for which rooming-in is required. Acute care cardiology units would benefit from creating a standardised approach for rooming-in practices to remove biases that may be present. Finally, PAC3 can assist with creation of standardised discharge instructions for common acute care cardiology unit discharge needs in languages most commonly utilised across the collaborative in order to narrow gaps that are described in centres without robust interpreter support.
Conclusion
The state of the acute care cardiology unit and the practice of acute care cardiology continue to be widely variable, owing likely to the heterogeneity of patient populations and hospital systems within which this care is delivered. While systems in acute care cardiology must exist within the constraints of existing hospital systems, identification of similarities where they exist and opportunities for optimal care delivery are facilitated by our efforts to conduct the biennial PAC3 Hospital Survey.
Acknowledgements
We would like to recognise the many outstanding PAC3 clinical and data champions for their contributions to this dataset. We would also like to recognise all clinical staff, patients, and families across participating PAC3 centres without whom this study would not be possible.
Financial support
This work received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
The authors declare none.





 Open access
Open access