

Introduction
The Japanese medical community often perceives the anticipated childcare and familial responsibilities of female physicians as inherent impediments to their professional advancement. (Reference Matsui, Sato, Kato and Nishigori1; 2) Female doctors inadvertently perpetuate this stereotype, allowing traditional notions of women’s roles in Japanese society to be mirrored within the medical sector. Consequently, these notions remain unchallenged by both female physicians and the prevailing system. There’s a pervasive reluctance among women to confront these gender biases, with many adopting a passive stance towards their medical profession. (Reference Takahashi, Nin, Akano, Hasuike, Iijima and Suzuki3)
Contributing factors include extensive working hours and a scarcity of childcare facilities. Prior research suggests that the resulting fatigue diminishes their capacity to counteract such stereotypes. The extensive working hours and lack of childcare facilities underscore a palpable lack of work-life balance. (Reference Nomura, Yamazaki, Gruppen, Horie, Takeuchi and Illing4) Additionally, while the representation of female assistant professors and lecturers has seen a yearly rise, the ascendancy of these female professionals to professorships and other pivotal roles remains challenging. (Reference Kono, Watari and Tokuda5) Barriers persist in rectifying gender disparity within the Japanese medical domain. In this chapter, we initially elucidate the challenges Japan encounters, as derived from literature reviews, and subsequently delve into specific instances.
Gender in Japanese Society
In a detailed analysis of Japan’s gender dynamics as of January 2020, the population stood at 60.94 million men and 64.36 million women, reflecting a nearly balanced sex distribution. Yet disparities emerge in the workforce: men outnumber women by roughly 2:1 in full-time roles, while the ratio inverts to about 1:2 for non-regular and part-time positions, constraining women’s participatory role in the labour market. Consequently, women’s average income remains significantly subdued, approximately 40% lower than that of their male counterparts. (6)
Cultural Background
A detailed description of changes in women’s roles in Japan’s cultural context in recent years follows. Historically, Japan endorsed practices such as ‘retirement upon marriage’ or ‘retirement by age 30’, exclusively applying to female employees. (7) This unequal employment condition was seen as a problem; thus, the Labour Standards Law was enacted in 1947. This law was designed to consider the physiological and physical characteristics unique to women and establish the ‘principle of equal pay’, which prohibits gender-based wage disparities. Between 1985 and 1999, the following labour laws were enacted: the Equal Employment Opportunity Law (1986), which prohibited dismissal due to pregnancy, childbirth, or maternity leave; the Convention on the Elimination of All Forms of Discrimination against Women (1985); and the Child Care Leave Law (1991), which supports workers with nursing or childcare so that they can smoothly balance responsibilities and continue work (now the Child Care and Family Care Leave Act, 1999). (Reference Iki8)
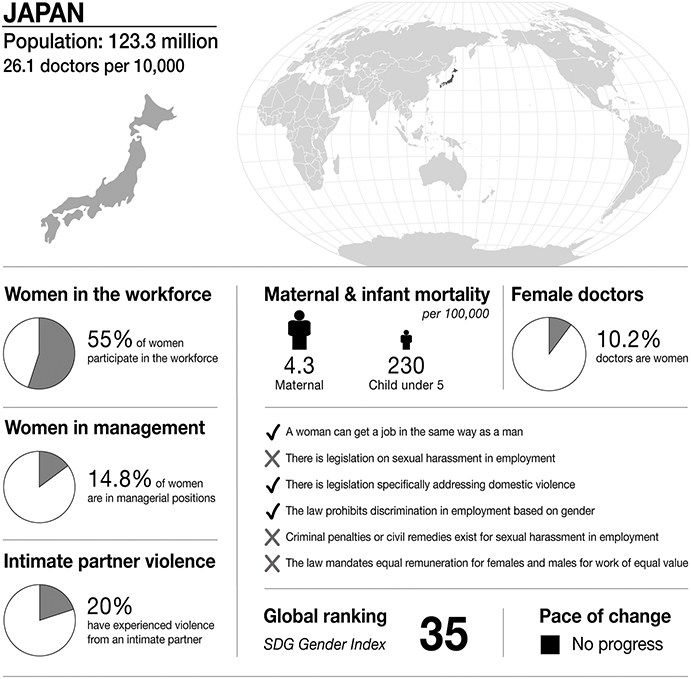
Infographic Japan. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.
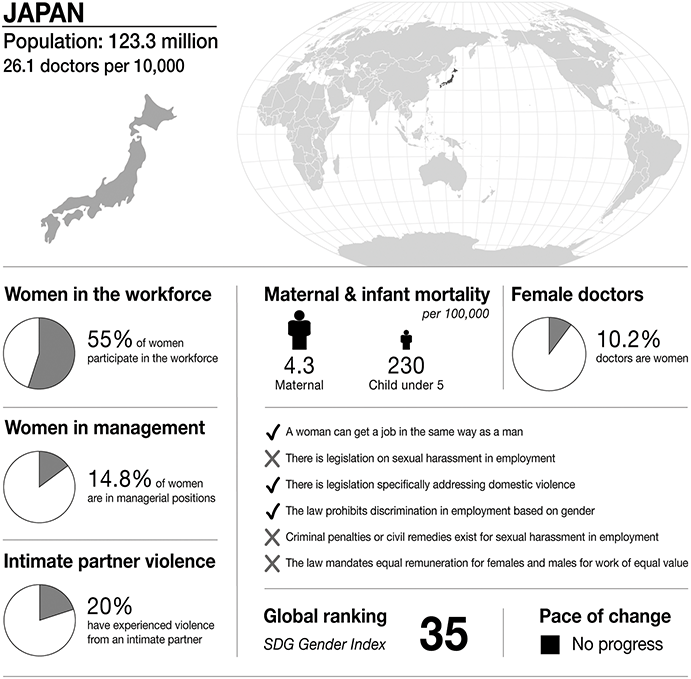
Figure 23.1 Long description
The infographic provides information about Japan, with a population of 123.3 million and 26.1 doctors per 10,000 people. It highlights several gender-related statistics. 55 per cent of women participate in the workforce. 14.8 per cent of women are in managerial positions. 20 per cent of women have experienced intimate partner violence. Maternal mortality is 4.3 per 100,000. Infant mortality under 5 is 230 per 100,000. 10.2 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In (country):
– a woman can get a job in the same way as a man- the law prohibits discrimination in employment based on gender.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– there is no legislation on sexual harassment in employment.
– criminal penalties or civil remedies for sexual harassment in employment do not exist.
– there is no law mandating equal remuneration for females and males for work of equal value.
S D G Gender Index global ranking is 35, and is stable.
Awareness about discrimination against women has also gradually increased. Between 1999 and 2022, there has been a shift in policies for women to improve gender equity. The Basic Act for a Gender Equal Society (1999) and the Law for the Promotion of Women’s Activities (2015) have been enacted, and the policy axis today insists on gender equality, inclusive of both men and women, rather than only for women. (Reference Iki8)
Changes in the Status of Women
Statistical data indicates changes in the status of Japanese women in recent years. It suggests that the number of women in the workforce has been increasing steadily, (10) and the percentage of female full-time employees (27.2%) has also increased. (9) However, the percentage of women in management positions remains low. (10) According to the Global Gender Gap Report 2021, women hold 14.7% of managerial positions, 9.9% of parliamentarian positions, and only 10% of all ministerial positions, with a score of 0.061 for ‘politics’ (0 being complete inequality and 1 being full equality). (11; 12) In 2016, the first female governor of Tokyo was finally elected, but there is yet to be a female prime minister in Japan. (13; 14)
Selective Dual-Surname System
A recent case highlights the issues Japanese women face: the selective dual-surname system. Under the current Civil Code, married couples are required to have the same family name when they marry, and to our knowledge, Japan is the only country in the world with such a requirement. (15) Hence, most women change their family names upon marriage. (16) With the advancement of women in the workforce, some advocate for the need to introduce a selective separation of the family names of married couples. However, the Supreme Court did not approve such a system. (17)
While the prevailing Japanese stereotype dictating that women should predominantly remain at home has evolved since the 1950s, gender-based discrimination persists. Women’s societal participation remains markedly unequal. Consequently, it is challenging to assert that Japan has achieved gender parity.
Gender in Medicine
In 2018, the total number of Japanese physicians was approximately 300,000, of which 21.9% were women. (18) The percentage of female physicians in Japan is the lowest in the OECD, (19) and many of them work as part-time or short-term regular employees rather than full-time employees. (20) As for the composition of each specialty by gender, the percentage of men engaged in internal medicine was 20.6%, orthopedics 8.5%, and surgery 5.3%, while the percentage of women engaged in internal medicine was 14.9%, pediatrics 8.9%, and ophthalmology 7.6%. (21) Men are more engaged in surgical specialties. (Reference Burgos and Josephson22)
Women Leaders in the Medical Community
According to Dr Kono et al., the number of female assistant professors has increased to 30% between 1980 and 2018, while the number of female professors has remained stagnant at less than 10%. (Reference Kono, Watari and Tokuda5) According to a 2011 survey by the Japanese Surgical Association, women comprised 14.6% of physician medical subcommittees and 6.3% of surgical societies. The current situation reveals the difficulties women face in getting promotions. It is rare for women to take on leadership roles in business or the medical world.
Sexual Harassment and Abuse in the Medical Community
In 2021, the Japanese Surgical Association conducted a sexual harassment survey among its female members. (23) Results showed that 50% of the respondents had been sexually harassed; 62% of female physicians had received negative comments about their pregnancies; and 28% had resigned or changed jobs because of pregnancy or the birth of their first child. (Reference Kawase, Nomura and Nomura24) In addition, 25% of female doctors had experienced sexual harassment, according to a survey by the National Doctor Union. (25)
According to a commercial physician membership platform Medical Restoration (m3.com), run by a private entity, 8.8% of male physicians and 60.9% of female physicians have indicated experiences of sexual harassment. Our study from April 2023 (n=430, response rate 80.4%, forthcoming) involving newly graduated resident physicians revealed that 28.7% of residents experienced some form of sexual harassment during their clinical clerkships; this comprised 17.2% encountering gender harassment and 9.0% facing unwanted sexual attention. Although no incidents of sexual violence or physical harm were reported, the potential for underreporting remains a concern.
Sexual Harassment in Hospitals
According to Japanese surveys, nurses, administrative staff, and doctors answered that they had ‘sometimes’ been sexually harassed. (26) Thus, the frequency of sexual harassment occurring in hospitals varies for several types of health care workers. Nurses tend to be more susceptible to sexual harassment, as compared to other health care workers. (Reference Amano27) Female physicians in Japan face both sexual harassment and pressure to sacrifice their jobs (their careers) because of life events such as marriage, pregnancy, childbirth, and child rearing. Therefore, it is difficult for female physicians to maintain an excellent work-life balance in Japan.
Medical Education
Undergraduate Training
In Japan’s university system, after high school graduation and six years of medical school education, students can take the National Medical Examination to obtain a medical licence. (28) However, private universities do not offer sufficient career support in undergraduate education as compared to public medical schools. According to Nagano et al., female physicians in private medical schools receive notably less career support, with only 20.7% being provided position support compared to 43.1% for men, and 20.7% receiving support for other job dimensions, as opposed to 70.6% for men. (Reference Nagano, Watari, Tamaki and Onigata29) Furthermore, female medical students are confronted with concerns regarding work-life balance, particularly in relation to matrimony and childbirth. (30) During entrance interviews, interviewers, who are physicians, often probe these students about life milestones such as marital plans. (30) Disturbingly, in 2018, discriminatory practices against female candidates were identified in four private medical school admissions processes. (31; Reference Kenji, Kunio and Takehisa32) The Ministry of Education, Culture, Sports, Science and Technology (MEXT) pointed out problems in medical school admissions and subsequently surveyed to clarify the status of improvement at each university. (31)
Postgraduate Training
After obtaining a medical licence, for specialization, doctors undergo two years of initial training under the Ministry of Health, Labour, and Welfare programme, followed by three to five years of postgraduate training. (28) The resident’s supervising physician conducts a clinical evaluation, (33) for submission to the hospital’s clinical training management committee, to decide the resident’s completion of training. Three primary issues exist. Firstly, when a resident’s supervisor is the perpetrator of harassment, it jeopardizes the resident’s training completion, thus inhibiting open discussion about the issue within psychological safety. Secondly, institutional guidelines predominantly focus on post-harassment actions, with a conspicuous absence of nationally standardized preventive measures or interventions. Lastly, the foundational guidelines for managing harassment prevention within Japan’s post-graduate education remain rudimentary, thereby relegating the decision-making process to the discretion of individual training centres.
Medical students and female doctors often ignore problems they are aware of because they do not want to get involved in further trouble. In fact, according to a survey by Medical Restoration (m3.com), 52.7% of those who said they had felt sexually harassed said it was by their immediate supervisor. (26) Female physicians are reluctant to speak up in the educational field because they do not want to make things awkward, with faculty members or senior doctors making it difficult for them to work.
Japanese Laws for Women
Laws such as the Equal Employment Opportunity Law (1972) and the Child Care and Family Care Leave Law (1992) contribute to the prevention and management of harassment for life events such as pregnancy and childbirth. (34) These laws also prohibit dismissal and other disadvantageous treatment due to pregnancy, childbirth, and childcare, and have been promoted to provide an environment where women can easily take appropriate leave. In addition, victims can also ask a neutral third-party organization to resolve harassment disputes against the offenders. With the enforcement of the revised Law for the Comprehensive Promotion of Labour Policies (i.e. the Power Harassment Law) (2018), employers’ measures against harassment have become an obligation. Companies are obligated to set up consultation services and implement measures to prevent recurrence. (35; 36) These laws are similar in their form to those of many developed countries in this area.
Operation of the Law on Sexual Harassment
While establishing a department dedicated to addressing harassment is commendable, the conservative cultural milieu of East Asia frequently hinders consultations from yielding prompt resolutions. Victims require tremendous bravery to approach the counseling department, and there have been instances where they faced unjust dismissals. (37) For instance, the number of consultations on the Equal Employment Opportunity Law (1972), the Part-Time Work Law, and the Child Care and Family Care Leave Law (1992) was 19,595, of which 7,323 (37.4%) (2019) were on sexual harassment. (38) Very few consultations led to disciplinary action such as transferring the perpetrators of sexual harassment to a different workplace. The recorded consultations are a small proportion of the actual number of sexual harassment cases occurring in the workplace.
According to a brochure disseminated by the Equal Employment Opportunity Office, a national governmental entity, sexual harassment is characterized in two primary categories. The first pertains to verbal manifestations, encompassing behaviours such as soliciting information about one’s sexual history, intentionally disseminating sexual rumours, making sexual innuendos or jests, repeatedly inviting individuals to meals or outings with romantic implications, and openly discussing one’s own sexual experiences. The second domain addresses physical and direct sexual actions, including coercion into sexual activities, unwarranted physical contact, circulating or displaying explicit imagery, forced lascivious behaviours, and rape.
From this delineation, it is evident that there are legislative efforts to categorize and perhaps manage manifestations of sexual harassment. However, a salient deficiency exists: while specific indecorous behaviours and unwarranted solicitations of sexual engagements are delineated, no overarching statute explicitly bans sexual harassment in its entirety. Until there is a legal provision that categorically proscribes sexual harassment, a comprehensive solution remains elusive. Thus, it is imperative for future legal frameworks to explicitly interdict sexual harassment (39).
Medical Regulation
Registration and Revocation System for Physicians
It is necessary to register as a doctor in Japan after passing the National Medical Practitioners Examination. The Ministry of Health, Labour, and Welfare (MHLW) manages details such as the name and legal domicile of the person who has obtained a medical licence. Second, the administrative punishment of physicians is outlined in the Medical Practitioners Law wherein the MHLW can issue a warning, suspend medical practice for three years, or revoke the licence of the offender. However, the MHLW must obtain the permission of the Medical Ethics Council before taking any action. (40)
Punishment of Doctors
According to ‘The concept of administrative punishment for doctors and dentists’ (41) of the Medical Ethics Subcommittee of the Medical Ethics Council, the degree of administrative punishment is determined by referring to the amount of punishment for judicial punishment. For example, indecent behaviour that takes advantage of one’s position as a doctor or dentist is considered a malicious act that betrays the public’s trust and will result in severe punishment. In other words, if doctors engage in sexual harassment or severe obscenity during medical treatment misusing their position, the harassment is likely to be illegal. (42) This will result in their suspension from medical practice or revocation of their medical licences.
However, the proceedings of the Medical Ethics Council, which examines and reviews the actions of doctors, are closed to the public and lack transparency. The names of doctors who have been suspended in practice are never made public. (43) The rights of doctors are overly protected despite inappropriate behaviour, and the opacity of the disciplinary and punishment processes is problematic. Another problem is that no specific punishment is mentioned for indecent behaviour towards peers (female doctors) in the hospital, and it is left up to each hospital and facility to decide what action needs to be taken. As a result, sexual harassment of female doctors by male colleagues is sometimes overlooked, (Reference Toshiko44) and male doctors are likely to continue medical practice without adequate punishment.
Therefore, clarifying the disciplinary process for physicians, stipulating clear disciplinary measures for sexual harassment of peers (female physicians) in the hospital, and ensuring that hospitals and facilities protect individuals (Reference Akihito45) are considered essential for improving gender bias.
Case Study
The following is a composite case of several people based on interviews. This illustrates how sexual harassment may be experienced and managed in Japan.
Setting
The characters are a male attending doctor A and a female Resident B, Resident C and Attending D. Attending A is educated, conscientious, and trusted by the residents. Among the three female residents, Resident B was particularly well supervised by Attending A. Neither Resident B nor others felt that this was a problem.
After one of my study sessions, Resident B received a message on social media from Attending A, saying that she was attractive and wanted to meet her in an empty room.
As soon as Resident B received this message, she discussed it with her trusted resident classmate C and her attending doctor D. When she did not reply to the message, she received another message from Attending A, saying that he did not want her to worry about it, and things were fine. After that, she did not receive any messages from Attending A.
Later, this incident became known to the others. Colleagues and junior staff made fun of Resident B, saying that she was invited because she was beautiful, that she must have been flirting with Attending A, and that Attending A was a womanizer, contrary to appearances. There were no other female residents in the room except Resident B. She felt frustrated that she could not say anything back and could only laugh along with them.
Prelude
There is a latent perception that men are superior in ability and position in a male-dominated environment in terms of numbers and status, and in a hierarchical relationship between attending doctors and residents. Such perceptions foster a culture in which women are evaluated not for their abilities but based on their appearance and charm.
Resident B thought that she had been treated by Attending A without any arbitrary intentions. However, from Attending A’s point of view, Resident B’s behaviour might have made him think that she loved him. She tried to remember each of their interactions to pinpoint which behaviour made him think so, but nothing came to mind.
Assault
Resident B was not physically harassed by Attending A. However, she was psychologically and socially harassed. She was afraid of what Attending A might do to her if she met him behind closed doors, and she was worried that her future career would be negatively affected if she rejected her supervisor. In addition, the comments of her colleagues and junior staff who found this incident amusing made Resident B feel uncomfortable at work and angry with them.
Some people may say that this is not sexual harassment because nothing was done. However, sexual harassment can cause indelible psychological scars on its victims, regardless of whether they are physically harmed.
Resident B suffered double sexual harassment, not only from Attending A but also from her colleagues and juniors who treated her unkindly. Since this incident was a one-time event, it is not worth remembering for the person who perpetrated this sexual harassment. However, for the victim, the suffering continues even now, and any trigger can suddenly recall the memory of the event.
Limbo
Resident B immediately consulted her trusted attending doctor and peers after receiving Attending A’s message. She knew she would not be able to resist Attending A if he harmed her behind closed doors. She also knew she would not be able to ignore what he did and continue working. However, she did not want all her colleagues or juniors to know about this. It was enough for Resident B to confide in someone who understood her suffering. She did not know how people found out about it later, but Resident B thought that she could confide in someone she trusted and then continue her work without telling anyone the whole story, and she did just that.
Exposure
When her name became known at work, and she saw her trusted colleagues talking about her with amusement, she was disappointed. She lost her trust in them and became angry.
How do I cope with this sense of betrayal when colleagues talk about me behind my back? At that time, she had to laugh it off. She did not want to say anything back to her colleagues or juniors and worsen her relationship with them.
Are the critics correct? Am I to blame? Resident B does not think so. While there was a comment that Resident B might have invited her superior, she did not remember misleading Attending A. She almost thought she was at fault, but she did not feel guilty. She did not feel guilty about what she had said or done, but she did not want to blame Attending A.
How do I keep working when everyone is talking about me? Resident B tried to think of the people who were likely to gossip or talk about her behind her back. She worked to keep a psychological distance from them by not socializing with them beyond work.
Aftermath
Resident B is now a senior resident working at a different hospital. Attending A continues to work in the same hospital. She positively reflected that she would now be able to deal with similar events if they occur in the future. She also thought that she would be able to advise other female doctors or medical students with similar experiences.
For Resident B, this incident triggered a strong desire to not want other women to go through the same thing. Rather than going public with her own experiences, she would first help the women near her.
Discussion
Current Problems
Society
In Japanese society, stereotypical ideas about gender roles such as ‘women are supposed to stay at home’ are still prevalent, making it difficult for women to change the way they work. (Reference Matsui, Sato, Kato and Nishigori1) It has been pointed out that this stereotypical way of thinking persists even among women. It is not difficult to change the system and rules. However, it is more challenging and time-consuming to change the culture, ‘the one that we women doctors embody’ through our education and cultural background. Studies from outside Japan have shown that family and national culture significantly influence women’s career advancement. (Reference Alers, Verdonk, Bor, Hamberg and Lagro-Janssen46; Reference Alwazzan and Rees47) As of 2022, women are still not playing an equal role in society, and the current situation in Japan is far from gender equal (Japan ranks 120th in a 2021 gender gap report). (12)
Medical Community
In the Japanese medical community, female doctors are more likely to be sexually harassed and sacrifice their careers because of their life events. (Reference Takahashi, Nin, Akano, Hasuike, Iijima and Suzuki3) There is a keen sense of not wanting to be in awkward situations with senior doctors, and even if there is a problem, action is often challenging. It is difficult for female doctors in Japan to have a proper work-life balance.
Laws
There are laws aimed at achieving gender equality and dealing with sexual harassment. (48) However, these laws are incomplete as far as specific consultation statistics and responses are concerned. The lack of laws prohibiting the act of sexual harassment is itself a significant problem. (49)
Regulation of Doctors
In the current situation, the punishment of doctors is unclear, and they are overly protected even if they are the cause of the problem.
Causes of Failure to Achieve Gender Equality
Unconscious Stereotypes
There are a deep-rooted stereotypical ideas about the division of labour in Japan, with women doing the housework and men doing the work outside the home. As a result, female physicians tend to leave the workforce after marriage to enter the home. The following are three studies and examples of stereotypes:
A questionnaire survey of female medical students reported that they accepted the inevitability of this forced choice of childcare and housework. (Reference Takahashi, Nin, Akano, Hasuike, Iijima and Suzuki3) Female medical students see this situation as inevitable and natural, and unconsciously give in to it. (Reference Ozaki50)
A study reported that ‘the process of integrating personal and professional identities of female doctors is greatly influenced by gender stereotypes that emphasize marriage, childbirth, and having a family, and prioritize the domestic role of wife and mother after marriage’. (Reference Matsui, Sato, Kato and Nishigori1) This study shows that the stereotype of female doctors being family oriented is deeply rooted.
While in medical school, Dr Uchida was told by male classmates that ‘being a doctor is hard work and not a woman’s job’ and ‘you can’t give birth or raise children’. (51) This statement shows that stereotypes take root among women and men. (Reference Izumi, Nomura and Higaki52)
From the above three cases, gender stereotypes about women’s roles which persist in Japan are likely to lead to difficulties at work and sexual harassment for female workers. Inadequate education on gender equality in educational institutions and clinical workplaces may also evoke unconscious stereotypes.
Social System with Poor Work-Life Balance
The second reason is that the Japanese social system does not allow women to have a good work-life balance. The following are three concrete examples of a poor work-life balance:
It has been pointed out that female doctors give up medical practice due to concerns such as working hours and lack of childcare facilities. (Reference Nomura, Yamazaki, Gruppen, Horie, Takeuchi and Illing4; Reference Nomura and Gohchi53)
In a survey about work-life balance promotion, nearly half the respondents answered that they did not think the relationship between themselves and their spouse/partner was equal in terms of childcare. (54) For female physicians with the heavy burden of childcare and housework, systems such as reduced work hours are beginning to be established through the Work-Life Balance Charter, (55) but they remain insufficient.
Female doctors experience a sense of inequality in the support system. (Reference Ono56) People in society find it challenging to have a good work-life balance because men and women have not achieved equality.
These three examples illustrate that the lack of work-life balance clearly makes it difficult for female doctors to concentrate on their work. It is essential to consider this issue as a problem for both female and male doctors.
Few Female Leaders and Educators in the Medical Field
The third cause of gender inequity is the lack of female leaders and educators in the field of medicine. Three concrete examples follow:
It has been reported that promotion of female doctors is hindered in Japanese universities and that there is a glass ceiling. (Reference Hashimoto57) The percentage of female physicians has increased from 10.0% to 21.1% over the past forty years, while female professors remained stagnant at less than 10% in 2004. (Reference Kono, Watari and Tokuda5)
According to Dr Nagano, the actual proportion of female doctors declines dramatically as academic rank increases in Japan, with only 4.7% women at the professor level. And the proportion of women in senior positions was significantly higher in private medical schools (28.2%) than in public medical schools (25.4%). (38) The percentage of women in senior positions, although higher in the private sector, is still low compared to men.
Studies have reported that fewer female organizers in meetings and conferences result in fewer female speakers. This study also suggests that if there are fewer women in leading positions, such as organizing the meeting or conference, fewer women are selected to speak. (Reference Homma, Motohashi and Ohtsubo58)
These three studies show few opportunities for women to take on leadership roles in the medical field. Furthermore, it is also clear that there is little likelihood that women will be appointed without more women leaders.
Insufficient Education around Gender Equality
In Japanese medical education, there is little education on gender issues, before or after graduation. According to Dr Nagano, (Reference Nagano, Watari, Tamaki and Onigata29) public medical schools provided more support for women in terms of positions and other job-related matters than private medical schools (exclusive positions for women in career advancement and research support: public 43.1% vs. private 20.7%, p = 0.043; regular employment available for shorter working time than full-time: public 70.6% vs. private 20.7%, p < 0.001). However, according to this study, more than half the medical schools do not support women. (Reference Nagano, Watari, Tamaki and Onigata29) A US study has shown that physicians are educated in several ways to deal with gender discrimination. As a result of this, female associate professor numbers increased, prejudice against women became apparent, and salary disparity improved. (Reference Fried, Francomano and MacDonald59) We should create facilities for better gender education in medical schools, hospitals, and facilities in Japan.
Because of these barriers, it is not surprising that fewer female physicians stay in the medical field.

 Open access
Open access