


Introduction
With fewer than 50 reported cases, maternal physiologic support after brain death (MPS-BD) with the intent to maintain a previable fetus is rare.Reference Dodaro1 In cases of MPS-BD, health care professionals (HCPs) provide prolonged intensive support to a pregnant decedent while the fetus continues to gestate. These scenarios present profound, interconnected, and sometimes conflicting ethical, legal, and clinical questions.Reference Cartolovni and Habek2 Considerations include optimal medical management, whether the pregnant decedent indicated antemortem preferences about organ donations or MPS-BD, who acts as the surrogate decision-maker, the legal framework regarding MPS-BD, and who bears financial responsibility for medical expenses incurred by providing MPS-BD.
Since the US Supreme Court overturned the constitutional right to abortion in Dobbs v. Jackson Women’s Health Organization, restrictive and often vague abortion statutes and fetal personhood laws, which vary state by state, add further complexity to these already nuanced and multifaceted circumstances.Reference Curhan3 We introduce a theoretical case to explore the ethical, legal, and clinical dilemmas raised in cases of MPS-BD. After a brief review of the clinical factors involved in MPS-BD, we describe the complex legal environment in which such cases arise, and delve into the ethical principles used to make decisions for cases of MPS-BD. Finally, we propose an institutional framework for navigating decision-making in these situations.
Theoretical Case
Miranda Jones is 7 weeks pregnant when she experiences a stroke and is declared dead by neurologic criteria: brain death (BD). She lives in a state that prohibits abortion after embryonic cardiac activity is detected, which generally occurs around the sixth week of gestation.Reference Schoenwolf4 The state also has a fetal personhood law, which establishes legal personhood for “any member of the species Homo sapiens at any stage of development who is carried in the womb” and invalidates advance directives during pregnancy.5 Because Miranda was unmarried, the father of the fetus has no legal decision-making authority regarding her health care, per state law. Since she had not identified a health care proxy, a person identified in legal documents to make decisions if the patient is incapacitated, her parents legally serve as surrogate decision-makers. Her parents report that Miranda had wished to terminate her pregnancy. Her partner was aware and in agreement. Additionally, she had not consented to postmortem organ donation and verbalized that she would not want to be dependent on mechanical ventilation if she had no hope of recovery. She did not, however, write a living will detailing her end-of-life care preferences and had never discussed such preferences in the context of pregnancy. The HCPs must determine how to navigate potential incongruencies between Miranda’s known values, the legal landscape, and the fetus’s potential interests.
Clinical Background
Brain Death
In the United States, HCPs declare death either when circulatory and respiratory functions irreversibly cease (circulatory death) or when all functions of the entire brain, including the brain stem, irreversibly stop (BD).Reference Aas6 After lawmakers codified BD in the Uniform Determination of Death Act (UDDA), medical organizations, including the American Academy of Neurology (AAN), published guidelines to standardize determinations and uphold ethical integrity.Reference Kirschen7 These guidelines affirm the permanence of BD: brain function will not return irrespective of medical intervention for a BD individual.Reference Greer8 Pursuant to these guidelines, a pregnant individual can be declared brain-dead by standard criteria, and pregnancy status should not preclude a BD exam if otherwise indicated.Reference Lewis9 While there is controversy surrounding whether consent should be required for BD testing, AAN guidelines state that HCPs do not need consent to evaluate a patient for BD unless otherwise required by institutional policies or state law.10 Once an individual is declared brain-dead pursuant to clinical criteria, the person is also considered legally dead, and ongoing somatic function reflects medically-supported physiologic activity rather than life. This distinction underscores the ethical, legal, and medical difference between maintaining biological processes and preserving life.Reference Magnus11
While HCPs typically discontinue interventions that provide physiologic and technologic support after BD, a small number of states recognize religious objections and allow accommodations.Reference Johnson12 Accommodations recognized by two states (California and Illinois) do not change the clinical or legal status of the decedent or prohibit an HCP from performing a brain death exam.13 Rather, they address institutional process and shield hospitals from liability for continuing physiologic support for a reasonable period beyond BD. Only New Jersey prohibits the declaration of BD if it would violate an individual’s religious beliefs. Under such circumstances, cardiorespiratory criteria must be used to affirm death.Reference Bernat14 In other situations, HCPs may maintain short-term physiologic stability to permit organ procurement and transplantation, including in a pregnant individual, with input from the multidisciplinary team and surrogate decision-makers.Reference Kantor and Hoskins15 However, a pregnant decedent raises an additional question: whether to continue physiologic support for fetal benefit to achieve live birth.
Miranda lives in a state that has codified the UDDA’s definition of BD. In Miranda’s case, the family agrees to a BD exam, although consent was not required by the health care institution or state law. After completing this testing, the neurologist declares Miranda dead by neurologic criteria.
MPS-BD for Fetal Sustenance in Practice
Not long after the UDDA’s adoption, the first case of MPS-BD with the intent of continuing gestation was reported.16 Three weeks after the individual was declared brain-dead, the HCPs delivered a live infant at 27 weeks’ gestation. Since that publication, additional cases of MPS-BD have resulted in outcomes of either live birth or fetal demise.17 Discussions and decisions about MPS-BD often focus on the decedent’s antemortem preferences, if known, and on fetal risks and benefits. Depending on the gestational age and circumstances, options include (1) discontinuing physiologic support with demise of the fetus, (2) immediate delivery of the fetus (if viable, beginning at around 22 weeks’ gestation in high-resource medical settings)Reference Battarbee18 with subsequent discontinuation of physiologic support for the decedent, and (3) continuing physiologic support at least until the fetus reaches viability.
MPS-BD requires intensive clinical management and creates the potential for multiple complications. Medical management typically requires intensive care unit-level support, with continuous monitoring of multiple physiologic parameters. Complications include infections (urinary tract infections, pneumonia, sepsis); circulatory instability; diabetes insipidus; thermal variability; and panhypopituitarism.19 Management may include preservation of uterine/placental blood flow, respiratory support to maintain adequate oxygenation and ventilation, cardiovascular support, hormonal regulation, management of diabetes insipidus, thermoregulation, nutritional support through total parenteral nutrition, and aggressive treatment of infections.20 The complications and required treatments may all have implications for the fetus.
The medical challenges of the decedent’s body, fetal monitoring, and fetal assessment guide the duration and intensity of MPS-BD, with the goal of achieving sufficient fetal maturity to optimize neonatal outcomes while balancing the maternal physiologic deterioration that inevitably occurs despite maximal medical support. In a review by Dodaro and colleagues, the most common indications for delivery were maternal cardiocirculatory instability (38%) and non-reassuring fetal testing (35%).21
Fetal viability currently begins near 22 weeks’ gestation in high-resource settings, and neonatal outcomes improve with each advancing week thereafter.22 Although data are limited, some reports suggest the risk of fetal demise and neonatal death or morbidity decreases as the gestational age at the time of brain death increases.23 The lack of oxygen to the fetal brain that may occur prior to initial stabilization of the pregnant decedent’s organs, subsequent medical complications during MPS-BD that may affect the fetus, and premature birth all can impact neonatal morbidity and mortality. Multidisciplinary HCPs should counsel the family so that they comprehend the process and range of expected outcomes and the multiple factors that impact outcomes when making decisions.
When MPS-BD is pursued, the clinical risks and benefits of the timing of delivery necessitate careful ethical reflection. Gestational age, maternal physiologic stability, and family preferences play a role. The family and medical team intend to maximize fetal well-being while avoiding unnecessary prolongation of physiologic support.Reference Mallampalli and Guy24 For some families, this creates pressure to continue MPS-BD until near term, if possible. The decision becomes more complex as the decedent’s physiology deteriorates with time. Maternal-fetal specialists, intensivists, and the neonatal team, together with the family, determine the best timing for delivery.Reference Feldman25
MPS-BD and the Law
A complex web of state laws may influence or constrain the clinical approach to MPS-BD. Because MPS-BD is not directly addressed with current legislation, interested parties must extrapolate from laws related to advance directives, fetal personhood, and abortion. Without clear guidance at the federal or state level, institutions have variable approaches to maternal BD, the ability to forgo MPS-BD, and the permissibility of prolonging MPS-BD.26 After Dobbs, regulatory authority over abortion returned to individual states, but statutes that focus on restricting abortion for living pregnant individuals or establishing fetal personhood as an additional means to restrict abortion do not address MPS-BD.27 Legal considerations extrapolated from laws governing advance health care directives, including living wills and health care powers of attorney, do not directly apply to someone who is brain dead. These laws are meant to pertain to living patients without capacity and only extend to decedents in the context of anatomical gifts. For example, the Uniform Health-Care Decisions Act of 2023 and Michigan’s patient advocate law require explicit authorization for anatomical gifts in order for the agent’s power to extend beyond death.28 Further complicating matters, many states have pregnancy override statutes that limit decision-making regarding the cessation of life-sustaining measures for living pregnant patients, including by invalidating a pregnant person’s living will either for the entire duration of pregnancy or after fetal viability.Reference DeMartino29 Specifically, the majority of states that invalidate or restrict end-of-life decisions for pregnant patients do so through (1) complete invalidation of a living will during pregnancy; (2) invalidation at the point of fetal viability; (3) presumptive validity unless withdrawal of intensive care would cause harm to the fetus; and (4) invalidation unless the patient has given specific instructions to apply the living will during pregnancy.Reference Segal30 These laws, however, govern decisions about continuing medical interventions in a patient who is still alive, not after BD.
Published court cases involving MPS-BD are few, but in a 2014 Texas case — Munoz v. John Peter Smith Hospital — the court emphasized the distinction between medical care for living patients without capacity and interventions performed on deceased individuals.31 In Munoz, the hospital continued MPS-BD against the family’s wishes, citing a state law restricting withdrawal of life-sustaining therapy during pregnancy. The court held that this law governs only living patients, not decedents, and that once BD is established, further interventions require appropriate consent.Reference Pope32 The decedent, Marlise Munoz, was subsequently removed from physiologic support, resulting in fetal demise.Reference Hellerman33 The trial court found that the Texas pregnancy override statute requiring life-sustaining treatment for a pregnant patient (Section 166.049 of the Texas Health and Safety Code) did not apply because Mrs. Munoz was legally dead.34 This decision was predicated on the difference between an incapacitated living patient and a brain dead individual.
State statutes defining fetal personhood further complicate matters. Such laws grant some degree of legal recognition and protection to the fetus as a person, with a range of potential implications. Even prior to Dobbs, some states adopted personhood language throughout their legal codes, including criminal codes that allow prosecutors to bring criminal charges of fetal abuse and fetal homicide.Reference Shachar35 Post-Dobbs, state statutes diverge widely, but some include personhood or “personhood-adjacent” language.36 These legal definitions encroach upon religious, philosophical, bioethical, and scientific definitions and individual conceptions of personhood. Extending personhood to fetuses can curtail pregnant patients’ autonomy before and after death, expose pregnant patients or third parties to criminal and civil liability, and, in some jurisdictions, compel HCPs to initiate or continue life-sustaining treatment for extremely preterm infants. Indeed, while fetal personhood laws are often directed toward restricting abortions, they have repercussions for a variety of other health care services, including miscarriage management, infertility treatment, contraception, MPS-BD, and more.
Statutes attributing fetal personhood as a reason to restrict abortions should not, however, control MPS-BD. Withholding or withdrawing technologic support from a pregnant decedent does not constitute an abortion. While the precise definitions vary, abortion statutes govern living pregnant patients, not decedents.37 Moreover, many laws restricting or banning abortion require the act of pregnancy termination to be taken with the purpose of terminating a pregnancy unless certain exceptions exist, such as to result in a live birth, to save the life or health of the mother, or in the case of fetal demise.Reference Colgrove38 The act of withdrawing support from a BD pregnant decedent is intended to allow the natural progression after death, not to terminate the pregnancy. The legal and moral intent is to refrain from prolonging bodily functions artificially after death has occurred. Nevertheless, there is a risk that, in the absence of clear legal authority (court opinion, explicit statutory language, and/or other official state guidance) establishing that the withdrawal of physiologic support from a BD pregnant decedent does not violate state abortion law, HCPs or other stakeholders may fear running afoul of abortion restrictions and maintain MPS-BD for this reason alone. In the context of a brain-dead decedent whose antemortem wishes would preclude MPS-BD, fear of legal action under state abortion or fetal personhood laws creates a legal-ethical dilemma for HCPs: honor a patient’s end-of-life wishes and risk civil or criminal liability for declining MPS-BD, or carry out MPS-BD in violation of the decedent’s preferences.Reference Cortezzo39 Defining nonviable fetuses as legal persons has the potential to elevate fetal claims while compromising the posthumous rights of the pregnant decedent.
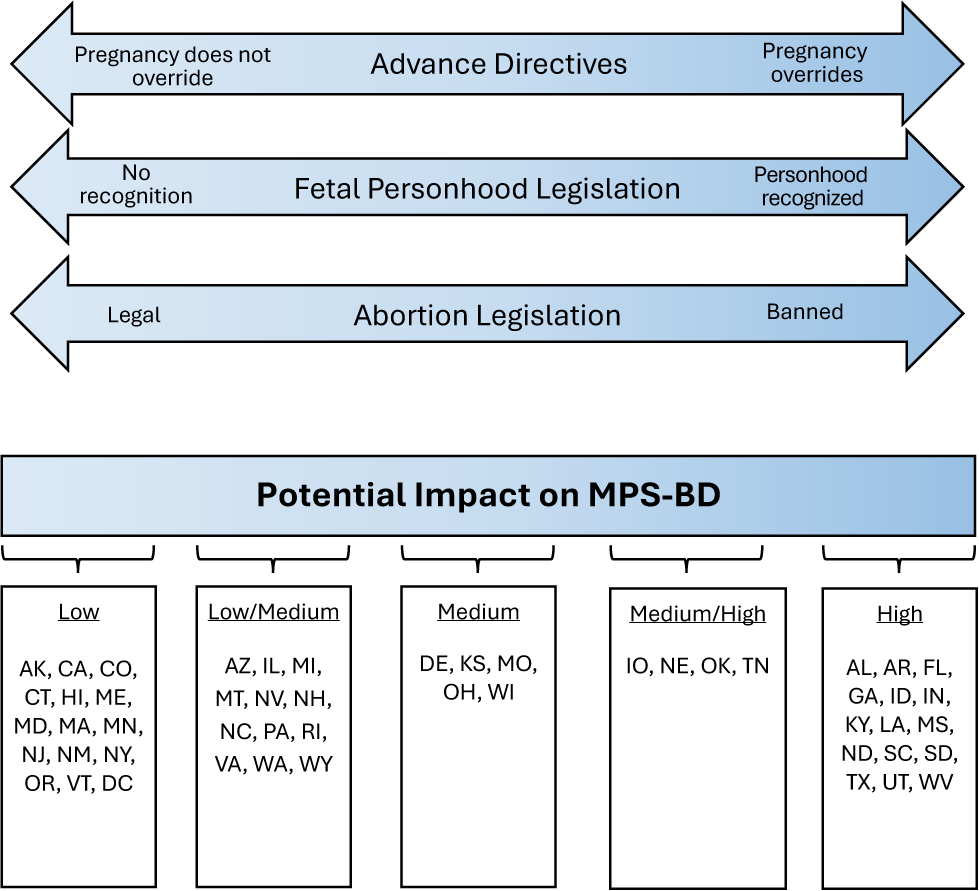
In the absence of clear guidance, HCPs must rely on ethical principles, case law, extrapolation from abortion, fetal personhood, pregnancy override statutes, and substituted judgment to navigate these situations. In some circumstances, hospitals or family members may seek court involvement to protect HCPs, institutions, and/or loved ones. Laws governing advance directives in pregnancy, fetal personhood, and abortion may independently and collectively affect decisions about MPS-BD, even though they govern living people and not decedents. For example, legislation that invalidates advance directives during pregnancy may increase the perceived need to provide MPS-BD; limited overrides of advance directives that allow the cessation of life-sustaining treatment in some cases (for example, prior to viability) may exert a more moderate influence; and the absence of restrictions on end-of-life decision-making during pregnancy is likely to have a minimal effect on MPS-BD decisions. Similarly, codification of fetal personhood may substantially shape decisions about MPS-BD, whereas its absence is unlikely to do so. Finally, in states with bans or severe restrictions on abortion, the expectation to preserve fetal life irrespective of clinical context may impact HCP and health care institutions’ policies regarding whether physiologic support can be discontinued. Where abortion remains legal, such laws are less likely to affect MPS-BD decisions. Legislation across these domains exists on a spectrum, and within a single state the legislation, and interpretation thereof, may be incongruent. Figure I illustrates how each factor, alone and in combination, may influence MPS-BD. Based on our state-by-state review, we propose relative impact categories: low, low-to-medium, medium, medium-to high, or high.
The Potential Impact of Current Legislation on Providing MPS-BD.
This figure depicts how legislation related to pregnancy override of advance directives, fetal personhood, and abortion may each independently and collectively impact decisions about MPS-BD. The authors analyzed whether the collective legislation from each state may have a low to high impact on MPS-BD.

In Miranda’s case, her unwritten preferences expressed before death hold questionable legal weight, especially in states with restrictive abortion laws or laws with strong fetal personhood language. Moreover, even if she had a living will or other legal document expressing her wishes against MPS-BD, HCPs and hospital attorneys in states with pregnancy override statutes may ignore such preferences in favor of maintaining fetal life.
Ethical Analysis
Clinical risks and benefits and an evolving legal landscape give rise to several complicated ethical dilemmas for HCPs, patients, and patients’ families who face the prospect of MPS-BD.
Autonomy and Substituted Judgment
Autonomy is one of the four main principles of biomedical ethics as articulated by Beauchamp and Childress in Principles of Biomedical Ethics, originally published in 1979.Reference Beauchamp and Childress40 In clinical ethics, autonomy emphasizes the patient’s right to make their own decisions about their medical care free from coercion and with an understanding of relevant information that advises their decision-making.
Although a decedent cannot exercise autonomy, a person who is alive can exercise autonomy by expressing preferences regarding the disposition of their remains. Failure to adhere to their antemortem wishes may, therefore, constitute a posthumous harm to their autonomy.Reference Wicclair41 For example, MPS-BD against a decedent’s expressed or implied preferences prior to death would constitute using their body for the benefit of another — the fetus. It also injures the family, who is unable to carry out their loved one’s wishes. In such a case, MPS-BD disregards the principle of autonomy and treats the decedent as an object — a mere means to an end. Interests formed and decisions made while alive about issues such as organ donation, disposition of remains, and estate planning all persist and are legally enforceable after death. That is, decedents still have morally salient interests.42
Even if a pregnant decedent had a living will that would otherwise govern treatment choices during pregnancy under institutional policy or state law, the decedent may not have expressed wishes regarding MPS-BD. Without a written mandate from the decedent, substituted judgment appropriately replaces autonomous decision-making. In substituted judgment, the health care surrogate bases their decision on the decedent’s values and known preferences, asking what the patient would have wanted if they could tell the surrogate decision-maker. If the surrogate has little or no information about a patient’s prior wishes, they decide using the best interests standard.Reference Torke43
Miranda clearly stated a desire to terminate her pregnancy, avoid prolonged ventilation without hope of recovery, and forgo organ donation. The nuanced discussions between her family and HCPs review the concept of substituted judgment and examine the effect of MPS-BD for Miranda and her fetus. The family concludes Miranda would not want MPS-BD for the sake of the fetus. Meanwhile, the HCPs recognize that allowing Miranda’s organs to cease functioning, the physiologic consequence of death, would result in fetal demise, as distinct from an abortion. Yet they worry that state law might construe withdrawal of physiologic support as “abortion.”Reference Lewis44 The hospital’s ethics team and legal department are both consulted. The ethics team concludes that it is ethically permissible to withdraw physiologic support so Miranda’s family can bury her and respect what her family believes she would have wanted, with the caveat to consult with the legal team. The hospital’s legal counsel, concerned about liability for the HCPs and the hospital, seeks judicial guidance. Although the medical team agrees with the ethics team’s analysis, the institution’s legal advice constrains their actions. They continue MPS-BD while awaiting the court’s decision.
Dignity and Bodily Integrity
Maintaining a pregnant decedent on medical technology for weeks or months after a declaration of BD raises questions about defacement, desecration, and harms related to dignity and bodily integrity, concerns that families and HCPs experience as deeply distressing.45 Every person deserves to die with dignity, which extends to honorable treatment after death.46 As with physiologic support after BD for organ donation, MPS-BD demands decency and dignity.Reference Montag47 Treating the decedent with respect, honoring previously expressed or known wishes, and recognizing the sensitivities of loved ones regarding death offer dignity for the decedent. The concept of bodily integrity requires avoidance of unnecessary procedures and respecting the individual’s cultural, religious, and ethical values about treatment of the body after death. MPS-BD may be perceived as a form of bodily exploitation or violation of the decedent’s dignity, particularly if it conflicts with antemortem preferences or substituted judgment.Reference Flamm48
Laws prohibiting bodily defacement or abuse of a corpse present challenges to MPS-BD.Reference Fleming49 Such laws could be interpreted to prevent some of the very acts that HCPs would have to engage in when providing MPS-BD.Reference Warren50 Invasive medical procedures and interventions necessary in MPS-BD may include establishing access for intravenous catheters or central lines, placing a tracheostomy, inserting a feeding tube, administering medications and blood products, drawing blood, and performing routine daily care to the decedent. Even when legal exceptions for health care exist, moral tensions remain.51
Medical students learn early in their education that the cadavers they dissect deserve respect. The students treat them with esteem and care, valuing the opportunity for education. Similarly, HCPs must treat the bodies of decedents receiving MPS-BD with respect and dignity. The organ donation system supports this concept.52 Once consent is obtained, HCPs maintain physiologic support only until organ procurement, typically for hours or a few days. For a brain-dead pregnant decedent, the physiologic support could last for seven to eight months. While both MPS-BD and organ donation after BD raise concerns of dignity and challenge the moral justification for continued intervention without consent, MPS-BD is distinct from organ donation by both length and degree of physiologic support.
Whether the decedent would have wanted MPS-BD has a bearing on dignity. The International Federation of Gynecology and Obstetrics’ Committee for the Ethical Aspects of Human Reproduction and Women’s Health endorses the rights of the pregnant decedent over those of the fetus.53 Some suggest that because the dead cannot feel pain, their interests cannot be supported.54 Yet instrumentalizing the body contrary to the person’s antemortem wishes is a violation of dignity and bodily integrity. Ethical practice requires careful deliberation about whether MPS-BD aligns with the decedent’s values while avoiding treatment driven by family desires or societal pressure alone.55 This may cause moral constraint or distress if restrictive legislation dictates a care path that does not align with these principles.
Moral Status of the Pregnant Decedent and the Fetus
Moral status reveals the standing or value of an individual, which compels that their interests be treated as morally significant.Reference Jaworska and Tannenbaum56 Whether dead persons retain or fetuses possess moral status has generated much discussion.Reference DeGrazia57 Some contend that loss of physiologic function entails loss of moral standing.Reference Veatch58 However, as evidenced by the standard of honoring decision-making related to organ donation, there is still a precedent to respect and abide by an individual’s antemortem wishes. Disregarding these interests without moral justification disregards the principle of autonomy. We argue that respect for the decedent remains important regardless of one’s pregnancy status.
Further complexity arises in MPS-BD, where two entities, the decedent and the fetus, have degrees of moral status. Brain death extinguishes traditional concepts of personhood — rationality, self-awareness, and relational capacity.59 The fetus likewise lacks these attributes. This raises questions about whether either the decedent or the fetus can embody personhood in the ethically relevant sense, or, more broadly, if personhood is even a requirement to extend moral standing to an individual.
Theories of personhood vary widely and garner much debate. Some traditional approaches base personhood upon a psychological method and consider memory, self-awareness, and rational thought.Reference Locke60 John Locke, for example, characterized the infant as a blank slate and accordingly denied it the status of personhood. Others rely upon attributes such as consciousness, reasoning ability, mental states, self-awareness, and ability to experience, features lacked by fetuses.Reference Blumenthal-Barby61 More recently, bioethical concepts of personhood based on moral theories aim to clarify the fundamental wrongs of harming a person regardless of the above psychological factors.Reference Holm and Lewis62 For a fetus, this concept of nonmaleficence may be applied at any number of points in gestation: Some assign personhood at fertilization, others at viability, others at the point when a fetus can experience sensations as either agreeable or disagreeable, and others when the pregnant patient personally confers moral status upon the fetus.Reference Campo-Engelstein and Andaya63 These definitions may be rooted in religious beliefs, moral theories, social systems, and/or biology. This wide variation in the basis for assigning personhood translates to a lack of a universal definition of personhood. Deliberations about the meaning of personhood therefore continue, influencing not only the abortion debate but also discussions and decisions about MPS-BD.
Moral standing, however, does not rest solely upon personhood. In the case of MPS-BD, the decedent’s moral standing can rest on their interests, expressed prior to death, in gestating a fetus, organ donation, or disposition of remains.64 The fetus’s moral standing begins at some point in gestation, a point that has been variably defined, and increases along the gestational continuum due to sentience and viability. Even a nonviable fetus may have relative moral standing, but DeGrazia and others argue that the moral standing of a future person is not the same as that of a person, even one who has died.Reference Feinberg, Beauchamp and Regan65 In particular, we argue that the pregnant decedent has greater moral status than that of the previable fetus.
Decisions about MPS-BD should therefore be guided by the pregnant patient’s expressed beliefs and wishes about what should happen to their body after death, and, if known, their ideas about fetal personhood. Though few pregnant individuals discuss MPS-BD, their expressed thoughts about organ donation, dignity of the decedent, desire for parenthood, and disposition of the body can give some insight into their thinking. The extended medical team, together with the family, must evaluate each case of possible MPS-BD to determine the ethically appropriate course of action.
Miranda’s body functions through physiologic support while her fetus develops. The well-recognized posthumous rights and interests of the deceased confer moral standing. Due to a lack of a written living will explaining Miranda’s antemortem choices, her parents use substituted judgment and ask to end physiologic support, a decision they believe is supported by Miranda’s desire to terminate this pregnancy and her desire to not be placed on mechanical ventilation if she had no hope of recovery. Miranda’s partner is supportive of this decision.
Justice and Resource Allocation
Prolonged MPS-BD raises broader ethical concerns beyond the individual patient, family, and HCPs. Such care creates substantial financial burdens that raise important questions about health care resource allocation. These cases often require weeks to months of care in an intensive care unit (ICU) and, if the fetus is born alive, in a neonatal ICU. The cost of such care can reach hundreds of thousands of dollars or, in some instances, over a million dollars.66 Insurance coverage varies substantially in the United States. Most policies exclude care after BD.Reference Liao and Ito67 When not covered by insurance, the hospital may assume costs or negotiate with families resulting in the estate shouldering the fees.Reference Howard68 Institutions must also consider the costs of dedicating ICU beds and specialized staff for a dead patient when those resources could serve critically ill patients with potential for recovery. The prospect of a favorable neonatal outcome complicates a simple cost-benefit analysis. Some institutions have developed specific protocols and designated resources for these cases to minimize impact on other patient care. Importantly, these decisions related to justice and resource allocation should be made based on hospital or state policy rather than at the bedside.
In Miranda’s case, insurance does not cover care after BD. If courts mandate MPS-BD, the medical bill for the remainder of gestation will be extraordinary. Will Miranda’s estate be responsible for the medical bills even though she and her family opposed continued support, or would the hospital cover the costs?69 If Miranda’s estate is insufficient to cover the medical debt, who will pay for care? Would it matter if the family were the ones requesting ongoing intensive care? What if the ICU is at capacity and no beds are available for additional patients?
Timing of Delivery and Family Disagreements
When physiologic support continues, decisions about timing of delivery involve competing indications.Reference Farragher and John70 The goal for delivery may begin at the lower limits of viability, 22 to 24 weeks, but morbidity decreases and survival increases with advancing gestation. Should delivery be delayed to improve neonatal outcome? What if the decedent’s physiologic stability fails before that point? HCPs must weigh the benefits of greater survival and lower morbidity with the risks of fetal demise should the decedent’s physiologic stability fail. Families and HCPs must navigate this uncertainty together.
This article has thus far focused on a theoretical scenario in which family members are aligned about their desires surrounding MPS-BD and what they think the decedent would have wanted, but the decision to withdraw physiologic support is constrained by institutional policy and state law. While it is beyond the scope of this paper to fully consider the legal and ethical dilemmas that arise when family members disagree, we acknowledge that disagreements will heighten the ethical, legal, and emotional stakes. Disagreements may occur between the decedent’s partner and parents, among siblings, or across generations. Differing interpretations of what the decedent would have wanted, religious beliefs, and cultural values contribute to these conflicts. HCPs must traverse these disputes with family members while maintaining therapeutic relationships and remaining neutral about their personal preferences. They should seek mediated resolution with social workers, spiritual care professionals, and ethicists. When that fails, the named surrogate decision-maker or the legal default surrogate would decide. In some jurisdictions, an unmarried partner would not prevail without a valid health care power of attorney.71 If the default surrogate and the unmarried father cannot agree, the latter will have to go to court to petition for decision-making authority.
In Miranda’s case, her parents are the legal surrogates and align with the father of the fetus in prioritizing Miranda’s values.
Additional Considerations for the Family and HCPs
The above sections illuminate the profound ethical dilemmas that challenge fundamental principles of medical ethics and human dignity created by the intersection of BD, pregnancy, law, and ethics. The dilemmas and consequences of MPS-BD, whether freely chosen or forced by law, extend beyond the deceased pregnant patient and gestating fetus to the patient’s family, support systems, and HCPs.
MPS-BD can complicate the family’s grief, particularly when choices about whether to pursue MPS-BD are constrained by law. While no studies focus on grief in the context of MPS-BD, many examine grief in families of brain dead decedents maintained for organ donation.Reference Friedrich72 In their review, Kerstis and Widarsson summarize family member’s experiences when their brain dead relative receives support for organ procurement.73 Families report shock, denial, powerlessness, rage, and anxiety after an unexpected death. Many families do not understand whether intensive care treats the decedent or preserves transplantable organs. Decisions about donation evoke mixed responses: For some, saving others’ lives imparts meaning; for others, the process amplifies stress. Additional studies note that the ambiguity of the decedent appearing alive on physiologic support yet having been pronounced dead, and the difficulty of accepting the BD diagnosis, may complicate grief and worsen depressive symptoms.Reference Kentish-Barnes74
While studies are lacking, we expect that families of MPS-BD decedents would have a more exaggerated experience than families of those whose period of physiologic support is limited to facilitating organ donation. Families must witness the body of their loved one, whom they may have already begun to mourn, maintained on machines in a hospital bed, in a liminal state between death and burial. The persistence of physiologic support may impede their acceptance of death, as their loved one’s body remains physically present. Prolonged invasive procedures and visible physical changes as the body breaks down can seem disrespectful, further complicating grief. They may experience “ambiguous loss,” in which the lingering biological activity of a dead body prevents the normal mourning process and hinders the acceptance of death.Reference Boss75 Postponing rituals such as burial, cremation, memorials, and religious ceremonies delays closure.
Even if a family looks forward to welcoming a new baby (assuming the infant’s survival), MPS-BD can cause complicated and conflicting emotions. They may worry about the implications of MPS-BD on fetal health: feeling overwhelmed by the prospect of a long NICU stay and an uncertain prognosis that may include lifelong disability. If the fetus or premature infant dies, regret, guilt, and anger may intensify.
Patients’ families may experience feelings of helplessness, guilt, confusion, or betrayal. These emotions may be amplified if the families are inadequately involved in decision-making; not informed of treatment plans or potential complications; or denied decision-making power due to state laws governing abortion, fetal personhood, or living wills for pregnant persons. They may fear legal and societal repercussions if they make the “wrong” choice. Disagreement among the family may create additional strife and shatter support structures during a time when they are needed most.
For HCPs, navigating these sensitivities requires balancing respect for the family’s wishes with the obligation to honor the decedent’s body and uphold ethical standards. HCPs should facilitate compassionate communication, provide psychosocial support, and ensure transparency to aid families in understanding the complex medical and moral issues involved.76 HCPs who are constrained to perform MPS-BD by their institutions and/or interpretation of state law should seek and support the empowerment of family members to honor the decedent’s body in ways that are meaningful to them. In this way, HCPs can support healthier coping and grief.
HCPs may face their own moral distress when providing intensive care and performing invasive procedures on a pregnant decedent, particularly when the law seemingly requires them to do so against family wishes or known or presumed patient values.Reference Hamric and Blackhall77 Medical teams must perform invasive procedures, manage complications, and provide intensive interventions not for the benefit of the decedent receiving them but solely for the developing fetus who has an unknown chance of survival. This can create profound cognitive dissonance, particularly when the likelihood of bringing the pregnancy to viability is low, when the fetus shows signs of compromise, or when the process requires weeks or months of intensive care resources. Some HCPs may feel complicit in what they perceive as instrumentalizing a human body, while others struggle with the emotional toll of caring for a corpse in ways typically reserved for living patients.
The prolonged nature of care amplifies moral distress as staff members may develop emotional attachments to the deceased patient, the fetus, and the family while simultaneously questioning the clinical and moral appropriateness of the care provided.Reference Diehl78 Moral distress can lessen or alternatively increase when the pregnancy becomes visible or when fetal imaging provides a view of the fetus. A visible, live fetus inside a dead mother may intensify conflict and ambiguity about who the patient is. Health care institutions should offer counseling, ethics consultations, and opportunities for staff to express concerns.Reference Austin79
Miranda’s family wants to bury her. While the hospital pursues a court order, she remains on physiologic support. The family feels guilty for what is happening to Miranda’s body, despite not requesting MPS-BD or initiating the legal action. They do not feel supported by the institution. Moreover, they fear legal and social repercussions. While some of the family would love to welcome a new baby under other circumstances, they cannot make peace with forcing Miranda’s corpse to gestate a fetus she did not want to gestate while she was alive.
The medical staff likewise has difficulties caring for Miranda’s body while awaiting the court order. HCPs are continually reminded that their patient is dead as they do not use pain relief or symptom management for invasive treatment. Her body goes into cardiac arrest and requires cardio-pulmonary resuscitation. The doctors, nurses, and respiratory therapists feel they are desecrating her body. Knowing that she did not want to stay pregnant makes every physical interaction anguished. Offering emotional support to her bereaved family proves painful and difficult.
The Complexity of Ethics and the Law
While they often converge, the law is not necessarily bound to ethical principles, and what is ethical may fall outside the limits of the law. MPS-BD during pregnancy poses an ethically and legally complex scenario where ethical principles and legal requirements may diverge. We maintain that MPS-BD is ethically permissible but not obligatory, and, in some cases, ethical principles may in fact weigh against MPS-BD, such as in cases where the decedent’s express or implied wishes suggest they would not have wanted MPS-BD, or when their surrogate decision-maker chooses withdrawal of physiologic support over MPS-BD. Yet the law may challenge the prerogative of a decedent (via preferences expressed during life), surrogate, or health care team to forgo MPS-BD even when ethics permits or demands doing so. Decisions regarding who may act as surrogate for the fetus, the duration of support, and acceptable medical interventions may lead to conflicts between what clinicians ethically perceive as appropriate and what the law or institutional policy permits.Reference Barr80 Statutes directly addressing MPS-BD are nonexistent. In the absence of clear legal requirements, hospitals rely on institutional policies, ethics committees, and hospital attorneys to aid decision-making. Some hospital attorneys and HCPs extrapolate from fetal personhood, abortion, and pregnancy overrides in advance directive laws; others do not, resulting in variability in practice.
The intersection of ethics, law, and clinical practice in MPS-BD highlights several areas of tension. Clinically, somatic support is technically feasible; ethically, supporting the fetus may or may not be justified; legally, frameworks are silent or ambiguous at best. Resource allocation, emotional burden on families, and risk of medical complications regarding the decedent and the gestating fetus further impact decision-making.Reference Kass and Rachel81 Given these complexities, there is a compelling need for structured institutional protocols and legal clarity. Ethical and legal clarity can help standardize practice, reduce HCP distress, and protect maternal dignity and the rights of surrogate decision-makers. Interdisciplinary institutional guidelines, explicit maternal advance directives in pregnancy, and transparency of laws regulating postmortem bodily integrity are critical to support evidence-based, ethically sound, and legally defensible decision-making in these rare but consequential scenarios.
Counterarguments and Synthesis
We argue that the moral standing — and thus the rights — of the pregnant decedent outweigh those of a fetus with regard to MPS-BD. We acknowledge, however, ongoing debate about this and related issues. Others argue that the interests of the fetus create an independent moral obligation that always justifies MPS-BD and that HCPs owe beneficence to the fetus.82 They claim that if a limited period of physiologic support could bring the fetus to viability, withholding MPS-BD harms a vulnerable potential life and outweighs the harm to the decedent. Yet while beneficence towards the fetus carries moral weight, it should not override the decedent’s antemortem wishes and posthumous interests in the absence of consent. The lesser moral status of the fetus relative to the pregnant decedent, together with the lack of a general duty to use one’s body for others, challenges arguments for forced physiologic support.
Some authors suggest that with MPS-BD, the benefits to the fetus outweigh the harms experienced by the decedent.83 This may be true physically but not morally. As discussed above, mandated MPS-BD can generate significant moral harms. It also undermines the family’s ability to grieve appropriately, prolonging distress. Moreover, if the patient expressed the antemortem wish not to subject themself and/or their fetus to MPS-BD, maintaining support contravenes their right to determine the disposition of their body and their right to refuse treatment, rights recognized in both law and ethics.Reference Chervenak and McCullough84 In this sense, the harm of overriding the patient’s or surrogate’s wishes is significant, outweighing speculative benefits to the fetus when antemortem preferences clearly oppose such use of the maternal corpse.
No statute coerces the use of a decedent’s body for the sake of another, which is why organ donation requires consent.85 Even when a child needs a life-saving transplant, organ donation by their brain-dead parent cannot be compelled. In such situations, the living child holds indisputable personhood and moral authority, unlike the fetus. In the context of pregnancy, the pregnant decedent has no duty to physiologically support the fetus.
The court orders that Miranda’s antemortem wishes must be respected. MPS-BD is discontinued at 12 weeks’ gestation, allowing the family to bury Miranda’s body with her fetus in utero.
Practical and Policy Implications
When HCPs declare a pregnant patient brain-dead, they, with institutional support, should follow a set policy that allows enough flexibility to meet the needs and wishes of the individual decedent and family. A practical approach is outlined in Table I. First, HCPs should evaluate for clinical feasibility of MPS-BD. An interdisciplinary team comprised of intensivists, maternal-fetal medicine specialists, neonatologists, social workers, palliative care specialists, ethicists, and spiritual health advisors should meet with the family to discuss the meaning and implications of BD. They should elicit the family’s reaction and understanding and redescribe BD, as families often have difficulty accepting BD as real death. The hospital should conduct a resource evaluation, and the legal team should analyze institutional policies and state law for any relevant guidance or restrictions on the care options that are available. The health care institution should have a written policy for how to handle disagreements with family members and vague or conflicting laws. This policy should seek to adhere to the law without sacrificing principles of medical ethics and standards of care.
A Practical Approach for Considering and Enacting MPS-BD

Subsequently, the care team should inform the family about MPS-BD and elicit and document the decedent’s antemortem preferences, if known. They should identify the appropriate surrogate and discuss the surrogate’s knowledge of the decedent’s end-of-life wishes, feelings about the current pregnancy, views regarding fetal personhood, and any other relevant considerations that may illuminate what the decedent would have wanted in the case of brain death while pregnant. The medical team should clearly explain the expected course and potential medical complications of MPS-BD for the decedent’s corpse, the risks of injury to the fetus, and the potential outcomes for the fetus under the unique clinical circumstances that led to the pregnant person’s death. The surrogate’s role, absent specific documented wishes regarding MPS-BD, is to make the choice they believe the decedent would choose under these circumstances. The HCPs should document the decision of the surrogate with the rationale.
If the family chooses MPS-BD, the care team should hold multiple multidisciplinary meetings involving maternal-fetal specialists, obstetricians, neonatologists, palliative care specialists, nurses, ethicists, social workers, spiritual health advisors, and the family. The care plan should take into account the status of the decedent, timing of delivery of the fetus, social support, and bereavement assistance. HCPs should document regular communication with the family. Hospital lawyers should be available to discuss indications for court involvement if conflict arises. In addition, the hospital should develop mechanisms of support and counseling for family as well as staff.
In summary, institutions can use a screening process to consider MPS-BD if all the following criteria are present: (1) antemortem consent or persuasive substituted judgment grounded in the patient’s values; (2) a care plan with milestones such as delivery at specific gestational age if clinical stability persists; (3) a care plan in the event of cardiac arrest or significant physiologic instablilty; (4) a plan for staffing, beds, staff support, and funding that does not create unjust displacement of other patients; and (5) a plan for social and psychological support of both family and health care team given the moral, ethical, and emotional burden of MPS-BD. MPS-BD may not proceed if any of these conditions are missing and irremediable.
Conclusion
MPS-BD remains rare but raises serious ethical, legal, and clinical issues. Autonomy and dignity of the decedent remain paramount. Fetal interests, though morally relevant, do not override antemortem wishes or substituted judgment. In the absence of consent, HCPs should withdraw physiologic support, honor the pregnant decedent’s posthumous interests, and support families and staff.
Institutions must develop protocols to guide these cases, protect families, and support staff. They must take into consideration the legal constraints in their state while ensuring they parse whether and how specific laws apply to the living and the dead. With the rapidly evolving medicolegal climate, hospital attorneys must stay abreast of current legislation and guide HCPs as to how, if at all, they apply to these unique circumstances. Future research should include empirical data on outcomes, development of consensus guidelines, and national-level discussions on how to ethically manage MPS-BD. As medical technology advances, so too should our consideration of this difficult yet salient ethical problem.
Disclosures
The authors have nothing to disclose.


 Open access
Open access