


Introduction
Re-experiencing symptoms are a key component of post-traumatic stress disorder (PTSD; Ehlers et al., Reference Ehlers, Hackmann and Michael2004). Flashbacks are a form of re-experiencing and can be understood as intrusive multi-sensory memories (Hellawell and Brewin, Reference Hellawell and Brewin2004; Whalley et al., Reference Whalley, Kroes, Huntley, Rugg, Davis and Brewin2013) which are experienced as uncontrollable and as though they are happening again in the present moment (Ehlers et al., Reference Ehlers, Hackmann and Michael2004). Flashbacks are thought to exist on a continuum, ranging from a fleeting intrusive memory of a traumatic event to dissociative experiences whereby a person loses orientation to time and place for periods of minutes or more (Brewin, Reference Brewin2015). They have been found to differ from standard autobiographical memories in that flashback memories have been associated with higher levels of arousal, such as increased heart rate (Chou et al., Reference Chou, La Marca, Steptoe and Brewin2018). Whilst it has been proposed that differences are due to traumatic memories being encoded, organised, and retrieved differently from non-traumatic memories (Ehlers and Clark, Reference Ehlers and Clark2000), research into the underlying mechanisms of flashbacks remains limited. Existing research is also dominated by exploration of the visual component (i.e. what people see) of flashbacks (Brewin et al., Reference Brewin, Gregory, Lipton and Burgess2010; Pearson, Reference Pearson2019).
Somatic flashbacks can be understood as those in which somatosensory sensations, such as touch or physical pain, experienced during the traumatic event are re-experienced in the present. Whilst existing literature recognises that flashbacks are rich in sensory information (Berntsen et al., Reference Berntsen, Willert and Rubin2003; Brewin, Reference Brewin2014; Brewin et al., Reference Brewin, Gregory, Lipton and Burgess2010; Crespo & Fernández-Lansac, Reference Crespo and Fernández-Lansac2016; Malaktaris and Lynn, Reference Malaktaris and Lynn2019), research into somatic flashbacks is in its infancy. Current research is limited to a single prevalence study (Macdonald et al., Reference Macdonald, Salomons, Meteyard and Whalley2018) and four case reports (Mellman and Davis, Reference Mellman and Davis1985; Salomons et al., Reference Salomons, Osterman, Gagliese and Katz2004; Schreiber and Galai-Gat, Reference Schreiber and Galai-Gat1993; Whalley et al., Reference Whalley, Farmer and Brewin2007), all of which focus exclusively on the somatic re-experiencing of pain.
Research has found that treatment that specifically addresses flashbacks is associated with better outcomes (Nijdam et al., Reference Nijdam, Baas, Olff and Gersons2013). Despite this, no empirical research exists which investigates the therapeutic treatment of somatic flashbacks. The present study explores the feasibility of a novel therapeutic treatment for somatic flashbacks, using imagery rescripting (ImRs).
ImRs is a therapeutic technique that uses mental imagery to update the meanings associated with traumatic memories and reduce re-experiencing and emotional distress (Arntz, Reference Arntz2012). The term ‘mental image’ is used to describe imagery that can contain one or more of the five senses (Kosslyn et al., Reference Kosslyn, Ganis and Thompson2001). Although ImRs is not explicitly named within the current UK clinical guidelines for the treatment of PTSD (National Institute for Health and Care Excellence, 2018), it is often integrated into the recommended trauma-focused therapies, cognitive therapy for PTSD (CT-PTSD) and eye movement desensitisation and reprocessing (EMDR) therapy (Arntz, Reference Arntz2011; Ehlers et al., Reference Ehlers, Hackmann and Michael2004). Over the last 30 years, ImRs has been used successfully as an intervention for PTSD amongst veterans ( Alliger-Horn et al., Reference Alliger-Horn, Zimmermann and Schmucker2016), asylum seekers and refugees (Arntz et al., Reference Arntz, Sofi and Van Breukelen2013; Steel et al., Reference Steel, Young, Akbar, Chessell, Stevens, Vann and Arntz2023), survivors of childhood abuse (Boterhoven de Haan et al., Reference Boterhoven de Haan, Lee, Fassbinder, van Es, Menninga, Meewisse, Rijkeboer, Kousemaker and Arntz2020; Jung and Steil, Reference Jung and Steil2012; Jung and Steil, Reference Jung and Steil2013; Raabe et al., Reference Raabe, Ehring, Marquenie, Olff and Kindt2015; Raabe et al., Reference Raabe, Ehring, Marquenie, Arntz and Kindt2022; Smucker and Niederee, Reference Smucker and Niederee1995; Steil et al., Reference Steil, Jung and Stangier2011), survivors of workplace injuries (Grunert et al., Reference Grunert, Weis, Smucker and Christianson2007), people experiencing survivor guilt (Murray et al., Reference Murray, Medin and Brown2021), people with a co-morbid eating disorder (Napel-Schutz et al., Reference Napel-Schutz, Vroling, Mares and Arntz2022), and people with co-morbid symptoms of psychosis (Clarke et al., Reference Clarke, Kelly and Hardy2022; Paulik et al., Reference Paulik, Steel and Arntz2019). A recent meta-analysis of 17 randomised control trials (Kip et al., Reference Kip, Schoppe, Arntz and Morina2023) demonstrated ImRs can effectively treat a variety of mental health difficulties, and produced similar treatment effects to other evidence-based interventions; potentially in fewer sessions.
ImRs protocols fall into two categories: those in which the client relives a traumatic memory and is invited to change the ending of it, to meet their needs, e.g. for a child in danger to be rescued by a valued adult (Arntz and Weertman, Reference Arntz and Weertman1999; Smucker et al., Reference Smucker, Dancu, Foa and Niederee1995); and those in which a new mental image is constructed to capture the ‘antidote’ cognitions, emotions, and meanings needed to counteract the distress associated with a ‘toxic’ image (Holmes et al., Reference Holmes, Hales, Young and Di Simplicio2019; Steil et al., Reference Steil, Jung and Stangier2011). An example of the latter would be creating a mental image in which someone can see all of their skin cells regenerating to reduce the feeling of being contaminated following a sexual assault (Steil et al., Reference Steil, Jung and Stangier2011).
The current study aims to contribute to the existing evidence base for ImRs in PTSD by developing an ImRs intervention to specifically target somatic flashbacks. It addresses the gap in knowledge around the feasibility of using ImRs in the treatment and management of somatic flashbacks in PTSD. An effective ImRs intervention for somatic flashbacks could complement existing therapies and lead to more effective treatment protocols for a specific symptom that has been overlooked in the existing literature. As the majority of existing research focuses on imagery re-scripting for visual flashbacks, the current study aims to provide guidance to an adaptation to imagery re-scripting for somatic flashbacks, which may be less intuitive to clinicians.
The primary aim of the present study is to investigate the feasibility, safety, and acceptability of the intervention. Given that research suggests that re-experiencing symptoms reduce following successful PTSD treatment (Ehlers et al., Reference Ehlers, Hackmann and Michael2004), the secondary aim of this study is to explore if the intervention leads to any differences in participants’ experience of somatic flashbacks and their global symptoms of PTSD. It was hypothesised that ratings of somatic flashbacks and global PTSD symptoms would reduce following the intervention.
Method
Participants
Seven participants were recruited from two National Health Service (NHS) out-patient specialist PTSD services between October 2023 and April 2024. Inclusion criteria were: (1) age 18 and above, (2) DSM-5 (American Psychiatric Association, 2013) diagnosis of PTSD or ICD-11 (World Health Organization, 2022) diagnosis of complex PTSD. PTSD and complex PTSD were diagnosed during participants’ assessments into their respective services. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) (Weathers et al., Reference Weathers, Bovin, Lee, Sloan, Schnurr, Kaloupek, Keane and Marx2018) and the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5; Weathers et al., Reference Weathers, Litz, Keane, Palmieri, Marx and Schnurr2013) were administered at this stage to assess for PTSD symptoms, (3) currently experiencing somatic flashbacks, and (4) to have completed the first phase of those services’ phase-based model of treatment for PTSD (Robertson et al., Reference Robertson, Blumberg, Gratton, Walsh and Kayal2013). Phase 1 involves providing psychoeducation about common symptoms of PTSD and techniques on how to manage re-experiencing symptoms, including flashbacks, nightmares, and dissociation.
Exclusion criteria were: (1) currently receiving another trauma-focused intervention, (2) active suicidal intent or recent (past 8 weeks) suicide attempt, (3) currently abusing substances (substance abuse was not clinically measured; if substance use was disclosed by a participant, clinical judgement, supervision, and discussion with the participant was used to understand if current substance use was impacting the participant’s ability to engage and benefit from the intervention), (4) participation in the study is not considered in the best interest of the prospective participant by the clinical team responsible for the participant’s care, (5) participants who do not consent to the intervention sessions being recorded, and (6) participants who do not consent to their assessment information being made available to the trainee clinical psychologist carrying out the intervention.
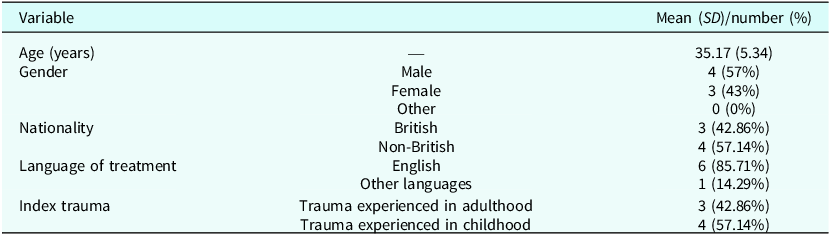
One of the NHS services was unable to provide funding for interpreters, and therefore, eligible clients who did not speak English could not be recruited. See Table 1 for sample demographics. Due to the small sample size, nationality was recorded in place of ethnicity to protect participants’ anonymity. No participants shared the same racial or ethnic identity, and all non-British participants had refugee status.
Sample characteristics

Design
A non-randomised feasibility study design was used.
Instruments
Primary outcome measures
Feasibility. Feasibility was assessed by recording eligibility rates, recruitment rates and completion rates.
Safety. Safety was assessed through monitoring and assessing adverse events for severity, expectancy, and relatedness to study procedures. Examples of adverse events include suicide attempts, serious violent incidents, and hospital admissions. As in Clarke et al. (Reference Clarke, Kelly and Hardy2022), supervisors determined the event severity and expectancy based on participants’ current and past context and the relatedness of an event to the study.
Acceptability. Acceptability was measured using the Treatment Acceptability and Adherence Scale (TAAS; Milosevic et al., Reference Milosevic, Levy, Alcolado and Radomsky2015). The TAAS is a 10-item self-report instrument that measures participants’ perceived treatment acceptability and anticipated adherence to psychological interventions for anxiety and related disorders (e.g. ‘I will be able to complete this treatment’). Items were rated on a 7-point Likert scale ranging from 1 (‘disagree strongly’) to 7 (‘agree strongly’), with total scores ranging from 10 to 70. As recommended on the TAAS measure, questions in the TAAS were modified to reflect the point at which the participant was completing the scale (e.g. after completing a treatment session, or after completing a treatment component). Higher scores indicate higher acceptability and anticipated adherence to an intervention. The TAAS has demonstrated high internal consistency of 0.87 and 0.88 (Milosevic et al., Reference Milosevic, Levy, Alcolado and Radomsky2015). This questionnaire was delivered after the final intervention session.
Secondary outcome measures
Target trauma memory ratings. Ratings of the target trauma memories were measured using a visual analogue scale (VAS). The VAS is a 4-item self-report measure used to assess ‘frequency’, ‘intensity’, ‘distress’, and ‘coping’ with somatic flashbacks. Items were rated on a 10-point Likert scale ranging from 0 (‘not frequent all’) to 100 (‘extremely frequent’), with total scores ranging from 0 to 400. The VAS was used at three time points to track changes in somatic flashbacks. Higher ‘frequency’, ‘intensity’, and ‘distress’ scores indicate more severe re-experiencing symptoms. Lower ‘coping’ score indicates a poorer sense of coping with re-experiencing symptoms. A similar measure was used in an existing pilot study exploring imagery rescripting for feelings of being contaminated (Steil et al., Reference Steil, Jung and Stangier2011).
The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5; Weathers et al., 2013). The PCL-5 is a 20-item self-report measure that assesses the 20 DSM-5 (American Psychiatric Association, 2013) symptoms of PTSD in the past month. Items were rated on a 5-point Likert scale ranging from 0 (‘not at all’) to 4 (‘extremely’), with total scores ranging from 0 to 80. Higher scores indicate more severe PTSD symptoms. It has demonstrated high internal consistency (0.94) (Roberts et al., Reference Roberts, Kitchiner, Lewis, Downes and Bisson2021).
Procedure
Participants were recruited through two NHS clinical teams. Participants had typically been referred to these specialist PTSD treatment services by their GP or other secondary mental healthcare teams. Participants recruited into the study were all on a waiting list to receive trauma-focused therapy and remained on the waiting list whilst taking part in the ImRs intervention. The following screening question was used to identify potential participants: ‘In the last 14 days, have you experienced any physical sensations in or on your body which resemble, in quality and location, the physical sensations experienced during the traumatic event (e.g. internal or external pain, tension, sensations of touch, pressure, warmth, coldness)?’. This question was either posed at assessment, by an assessing clinician in the service, or during initial symptom management sessions.
Eligible participants were provided with an information sheet about the study by their assessing clinician or by the lead clinician on the study. At least 48 hours were given to clients to allow time to read through the participant information sheet and ask questions about the study. Prospective participants were then contacted by telephone to confirm if they would like to take part in the research and provide informed consent. Where participants did not speak English, interpreters were used to translate the content of the consent form. Participants were made aware that opting in or out of the study would not impact their care within their respective NHS service. Participants who did not consent to take part in the study were not contacted beyond this stage.
Once recruited, all research procedures and therapy sessions were completed by one researcher (J.C.) under the clinical supervision of the other researchers (L.O. and F.B.). Weekly clinical supervision was available to discuss any questions. Each participant attended a pre-intervention session to complete the VAS, PCL-5, and to confirm the target somatic flashback. All participants then received two ImRs intervention sessions. At the end of the second ImRs session, participants completed the VAS, PCL-5, and the TAAS. The ImRs sessions occurred a week apart. Up to 90 minutes were allocated to complete each session.
At a 4-week follow-up session, participants completed the VAS, PCL-5 and were asked if any external events had impacted their symptoms of PTSD during the 4 weeks between intervention and follow-up. At the 4-week follow-up, participants also received a verbal and written debrief about the aims of the study.
Intervention
The protocol was developed drawing upon existing ImRs protocols (Holmes et al., Reference Holmes, Hales, Young and Di Simplicio2019; Jung and Steil, Reference Jung and Steil2012; Jung and Steil, Reference Jung and Steil2013; Muller-Engelmann and Steil, Reference Muller-Engelmann and Steil2017; Steil et al., Reference Steil, Jung and Stangier2011) and with the support of an NHS patient involvement group. An ImRs protocol which did not require imaginal exposure to the trauma was selected as it was felt this could be less intrusive and distressing for participants. Participants were supported to activate or develop a self-generated, strong, multi-sensory image that encapsulated the target somatic flashback (e.g. the moment they were physically assaulted). If participants reported multiple somatic flashbacks, a target flashback from a specific memory was agreed upon.
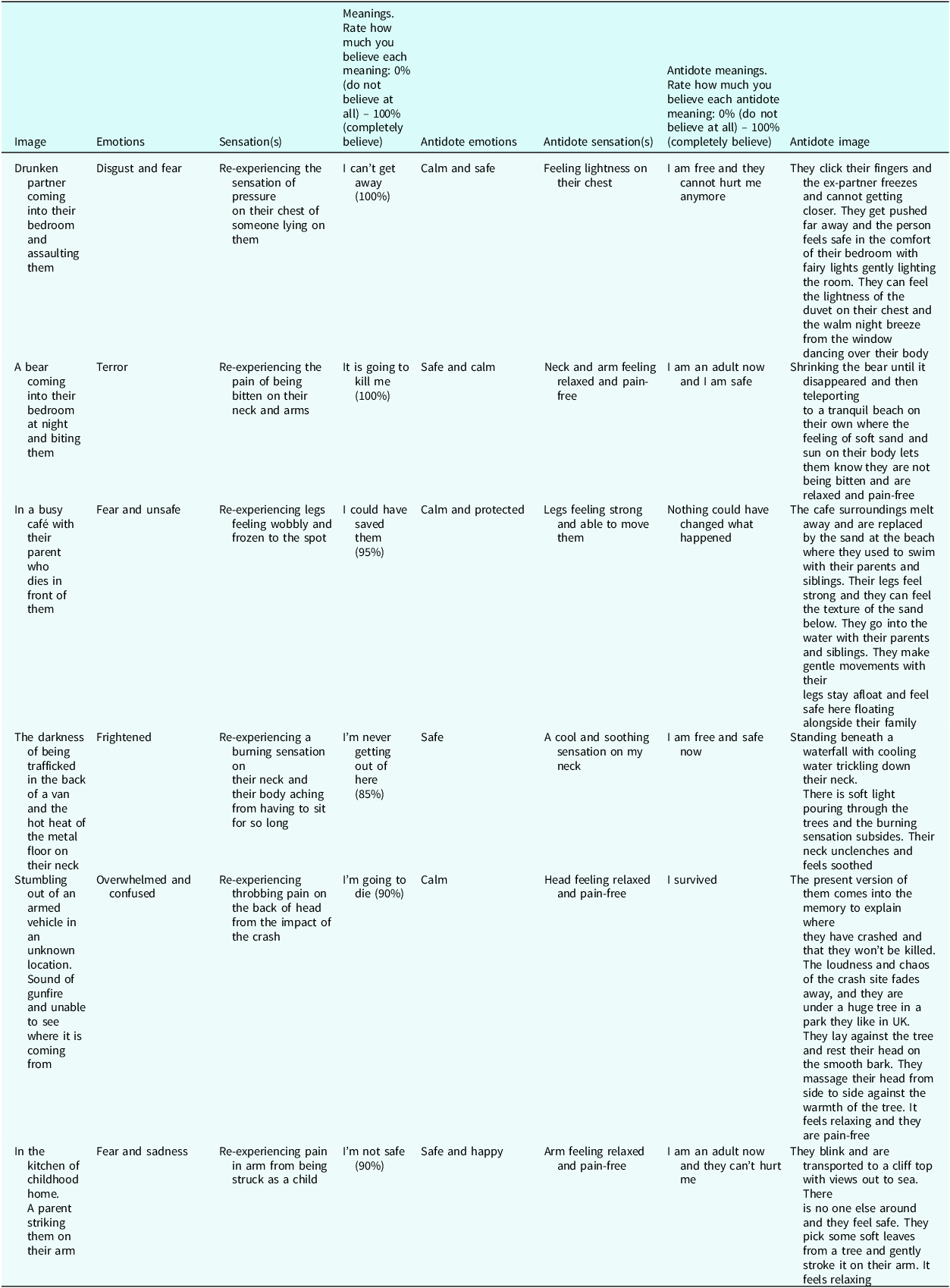
To develop the multi-sensory new image, the researcher gathered information about the participant’s ‘toxic’ emotional experiences, somatosensory experiences, and beliefs (e.g. feeling scared, a hot sharp pain on their face, and believing they will die). Following this, a participant-generated, multi-sensory rescript was created, which encapsulated the participant’s desired ‘antidote’ emotion, somatosensory experience, and beliefs at the time of the traumatic event (e.g. feeling safe, coolness and relaxation on their face, and believing they are no longer in danger). Participants were able to include whatever they felt would be useful within their rescript and were told this did not need to be realistic (for example, flying to a serene beach where the water cooled down the feeling of heat in their body). Table 2 details anonymised imagery rescripts. The order the cases are presented within the table have been randomised.
Overview of imagery rescripts

Data analysis
Feasibility, safety, and acceptability were evaluated through inspection of descriptive data and the TAAS. VAS scores were evaluated through inspection of descriptive data. PCL-5 scores were evaluated through inspection of descriptive data, reliable change index (RCI) and clinically significant change (CSC). RCI was calculated using thresholds reported by Marx et al. (Reference Marx, Lee, Norman, Bovin, Sloan, Weathers, Keane and Schnurr2022). Given the small sample size of the present study, the more conservative threshold of ≥18 point reduction in within-person PCL-5 scores was applied. Clinically significant change was defined as post-intervention score of ≤28.
Results
Primary outcomes
Feasibility
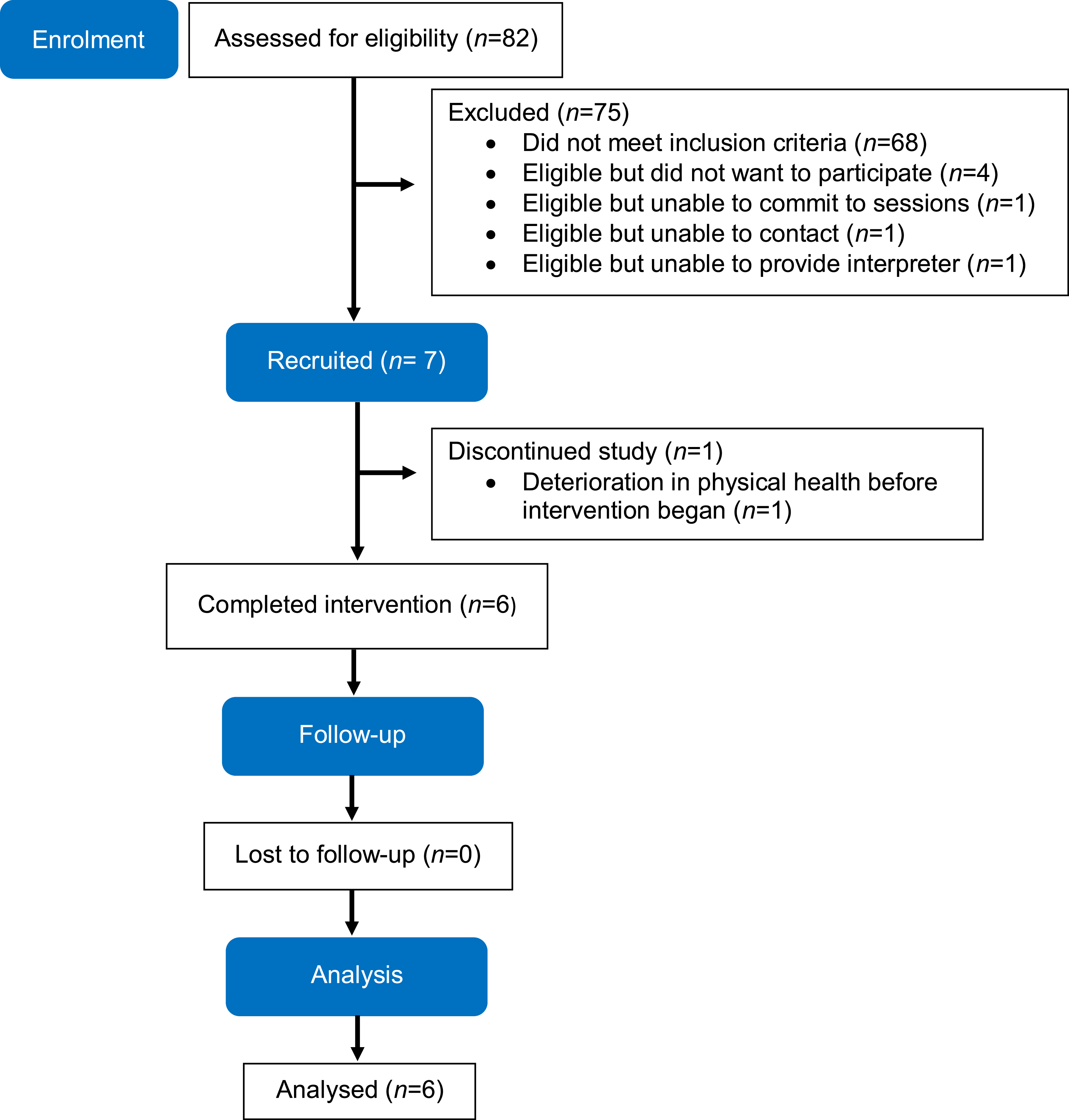
Figure 1 presents an overview of recruitment and participation. In total, 82 people were screened for eligibility for this study. Of these, 14 (17.07%) were eligible for participation. Seven (50%) of these people were recruited into the study. Reasons for not participating were declining to take part in research (n=4), feeling unable to commit to the sessions due to current employment demands (n=1), and being uncontactable by the researcher (n=1). In addition, one client who was eligible but did not speak English could not be recruited in the NHS service which was unable to fund interpreters.
Overview of recruitment and participation.

Of the seven participants who were recruited, six completed the intervention. It was agreed with one participant that they would not continue in the study after session 1 (pre-intervention session) due to a deterioration in their physical health. This was discussed in supervision. The six remaining participants all completed the intervention (in person) and follow-up session (four participants attended this session virtually). All participants reported being able to use the rescript between sessions.
Safety
No serious adverse events were reported during the study.
Acceptability
Overall, on the TAAS (Milosevic et al., Reference Milosevic, Levy, Alcolado and Radomsky2015), participants rated the study as highly acceptable, with an average rating of 58.17 out of a maximum of 70 (SD=10.89, range 40–70). No participants dropped out of the intervention after receiving their first ImRs session and all participants reported practising the intervention between sessions, which implies the intervention was tolerated well and that participants found the content relevant and useful.
Protocol adherence
One participant required two sessions to complete the pre-intervention measures due to arriving late to their initial session. This meant they attended five sessions in total instead of four. Whilst the protocol aimed for the intervention to be completed over 7 weeks, the average duration of the intervention was 9 weeks (ranging from 8 to 11 weeks). Reasons for delays included participant sickness, unplanned leave of treating clinician, public holidays, childcare difficulties and social stressors. On average, the first ImRs intervention session took 60 minutes to complete and the second ImRs intervention session took 45 minutes to complete. Supervision was provided to the clinician delivering the intervention to all participants. No other drifts from the protocol occurred during the study.
Secondary outcomes
Due to the design and sample size of the current study, the following analysis is exploratory. Any changes observed are intended to guide developments for sufficiently powered future studies. Data from the discontinued participant was excluded.
Frequency, intensity, and distress of somatic flashbacks and ability to cope
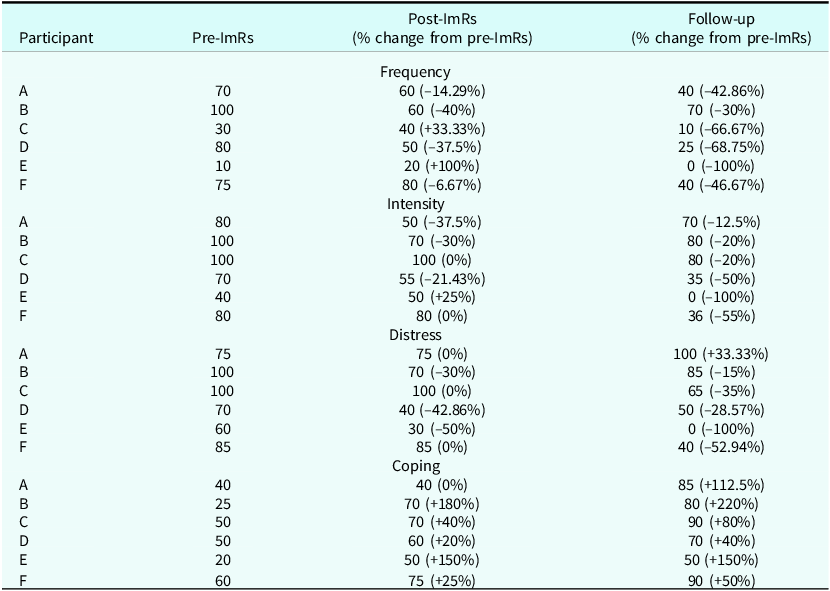
Based on previous research, changes in frequency, intensity, distress, and ability to cope VAS score (Steil et al., Reference Steil, Jung and Stangier2011) are reported. Table 3 shows participants’ VAS scores for each item and percentage change in scores at each time point.
Participant VAS scores and percentage change (VAS scores range from 0 to 100)

Frequency of somatic flashback VAS scores
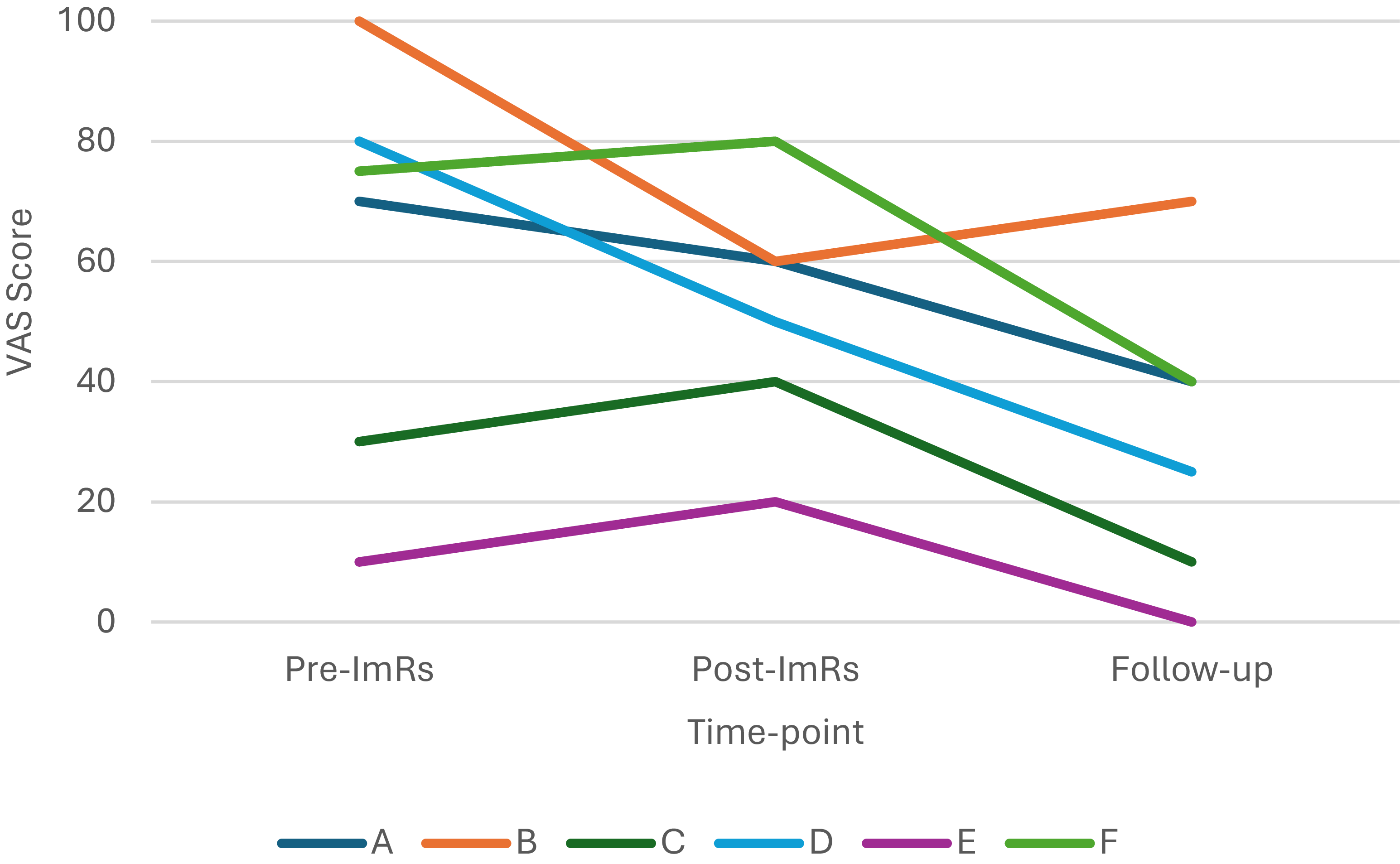
Between the pre-ImRs session and the follow-up session, participants’ mean frequency VAS scores (range 0–100) reduced by 30 (SD=15.17, range 10–55). This represents a mean reduction of 59.16% across the six participants. See Fig. 2 for frequency VAS scores at pre-intervention, post-intervention, and follow-up.
Participant frequency VAS scores (scores range from 0 to 100).

Intensity of somatic flashback VAS scores
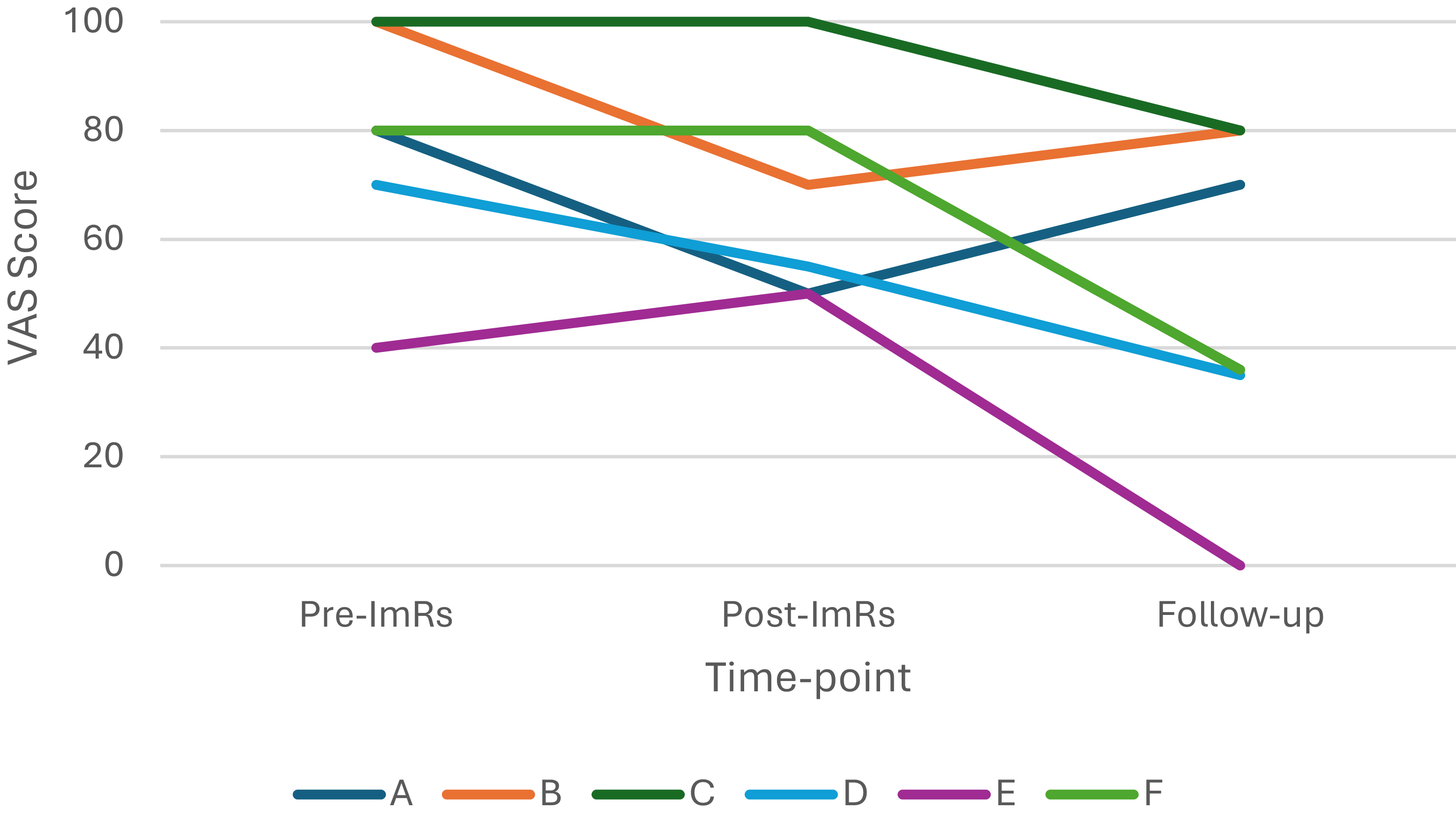
Between the pre-ImRs session and the follow-up session, participants’ mean intensity VAS scores (range 0–100) reduced by 28.17 (SD=13.42, range=10–44). This represents a mean reduction of 42.92% across the six participants. See Fig. 3 for intensity VAS scores at pre-intervention, post-intervention, and follow-up.
Participant intensity VAS scores (scores range from 0 to 100).

Distress due to somatic flashback VAS scores
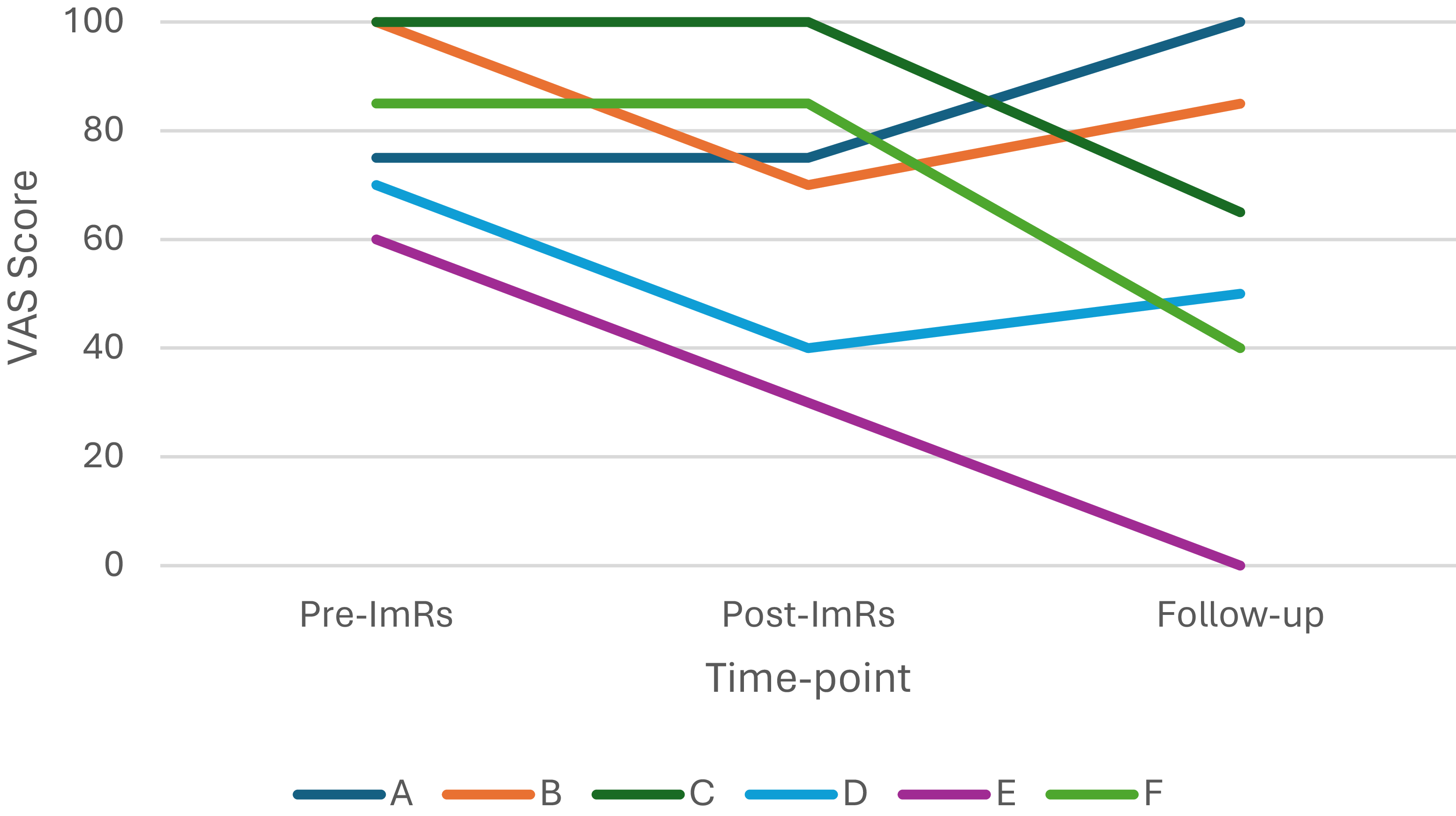
Between the pre-ImRs session and the follow-up session, participants’ mean distress VAS scores (range 0–100) reduced by 25 (SD=29.50, range –25–60). This represents a mean reduction of 33.03% across the six participants. See Fig. 4 for distress VAS scores at pre-intervention, post-intervention, and follow-up.
Participant distress VAS scores (scores range from 0 to 100).

Coping with somatic flashback VAS scores
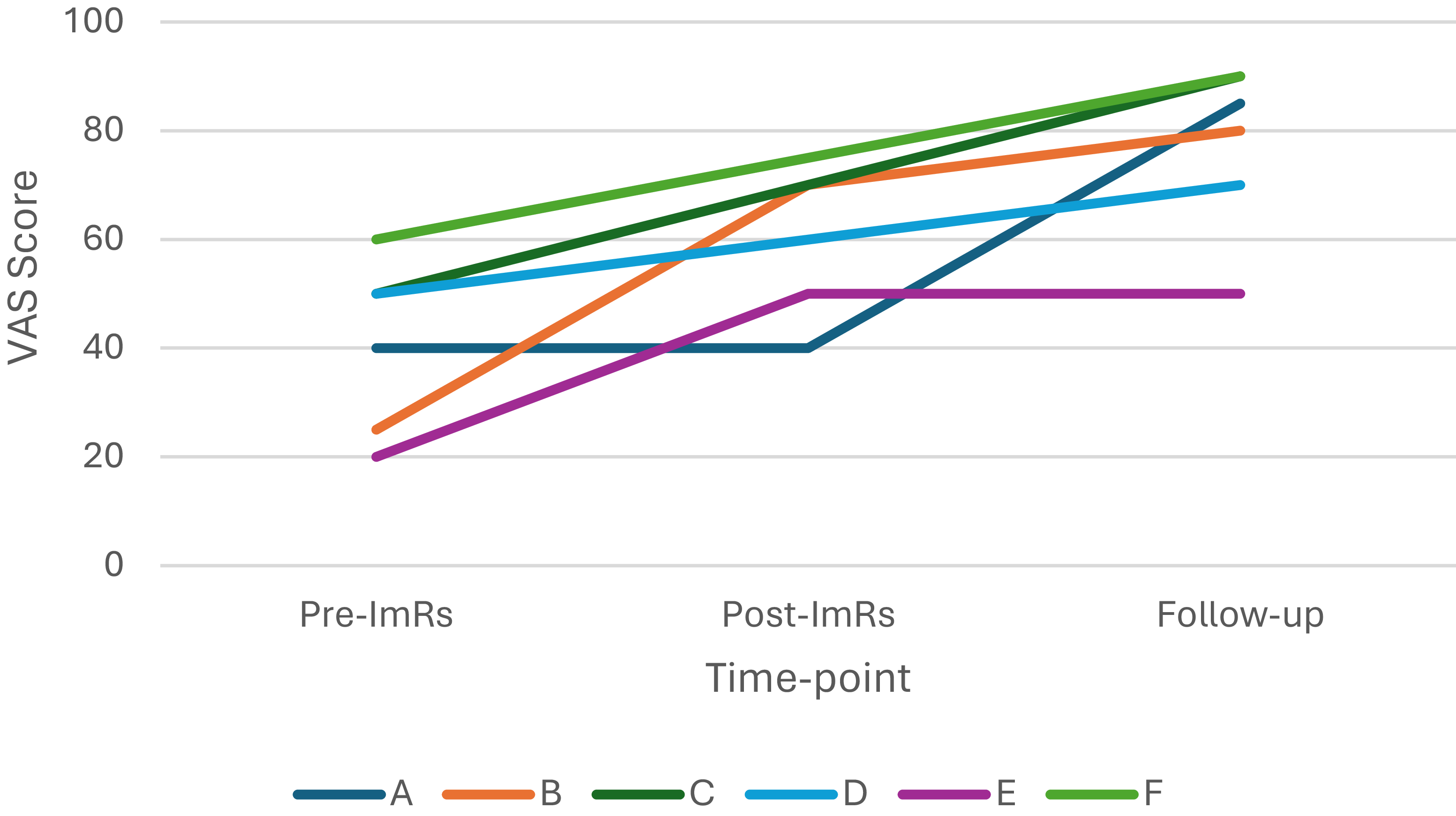
Between the pre-ImRs session and the follow-up session, participants’ mean coping VAS scores (range 0–100) increased by 36.67 (SD=12.52, range 20–55). This represents a mean increase of 108.75% across the six participants. See Fig. 5 for coping VAS scores at pre-intervention, post-intervention, and follow-up.
Participant coping VAS scores (scores range from 0 to 100).

PCL-5 score
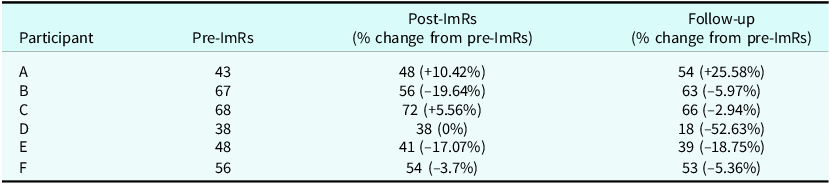
Table 4 shows participants’ PCL-5 scores and percentage change in scores at each time point. Between the pre-ImRs session and the follow-up session, participants’ mean PCL-5 scores (range 0–80) reduced by 4.5 (SD=10.09, range –11 to +20). This represents a mean reduction of 10.01% across the six participants.
Participant PCL-5 scores (scores range from 0 to 80) and percentage change in scores

Applying the RCI and CSC thresholds used by Marx et al. (Reference Marx, Lee, Norman, Bovin, Sloan, Weathers, Keane and Schnurr2022), one participant (D) demonstrated reliable improvement, evidenced by a 20-point reduction in their PCL-5 score. This participant also met criteria for clinically significant change, with post-treatment scores falling below the ≤28 threshold. No other participants demonstrated reliable improvement or met criteria for clinically significant change.
One participant (A) experienced an increase of 11 in their PCL-5 score, which they did not attribute to the intervention. When exploring potential reasons for this increase, this participant shared they had experienced a pain flare-up, and this often caused their PTSD symptoms to worsen.
Discussion
Somatic flashbacks are an acknowledged difficulty in people living with PTSD (Macdonald et al., Reference Macdonald, Salomons, Meteyard and Whalley2018), yet there is limited evidence regarding effective treatments for this symptom. This is the first study to investigate the feasibility, safety, and acceptability of a novel ImRs protocol for somatic flashbacks. It demonstrates the feasibility of delivering ImRs as an intervention specifically for somatic flashbacks and builds upon a growing body of research into the use of ImRs for symptoms of PTSD (Clarke et al., Reference Clarke, Kelly and Hardy2022; Jung and Steil, Reference Jung and Steil2013; Muller-Engelmann and Steil, Reference Muller-Engelmann and Steil2017; Napel-Schutz et al., Reference Napel-Schutz, Vroling, Mares and Arntz2022; Raabe et al., Reference Raabe, Ehring, Marquenie, Arntz and Kindt2022; Steel et al., Reference Steel, Young, Akbar, Chessell, Stevens, Vann and Arntz2023; Steil et al., Reference Steil, Jung and Stangier2011). This feasibility study shows that ImRs interventions can be successfully implemented to reduce overall disturbance associated with somatic flashbacks. On average, participants experienced a reduction in the frequency, intensity, and distress of their somatic flashbacks and an increase in their sense of coping with their somatic flashbacks. These benefits were maintained and continued at follow-up.
All participants that completed the intervention rated the intervention as acceptable and no adverse effects were reported or identified. The drop-out rate of this study (14.29%, one participant), which is inflated due to the small sample size, is in line with rates in existing ImRs research [7.1% (Murray et al., Reference Murray, Medin and Brown2021), 7.7% (Boterhoven de Haan et al., Reference Boterhoven de Haan, Lee, Fassbinder, van Es, Menninga, Meewisse, Rijkeboer, Kousemaker and Arntz2020), 0% (Alliger-Horn et al., Reference Alliger-Horn, Zimmermann and Schmucker2016), 0% (Jung and Steil, Reference Jung and Steil2013), 0% (Steil et al., Reference Steil, Jung and Stangier2011)]. In addition, the drop-out rate of this study is lower than the 22% average drop-out rate reported in a meta-analysis of trauma-focused treatments (Ehring et al., Reference Ehring, Welboren, Morina, Wicherts, Freitag and Emmelkamp2014). This suggests that a brief ImRs intervention targeting somatic flashbacks is safe, acceptable, and tolerated well by survivors of trauma.
As recommended in previous ImRs research (Steel et al., Reference Steel, Young, Akbar, Chessell, Stevens, Vann and Arntz2023), a flexible approach was taken to the delivery of the intervention. Clinical discretion was used to reschedule appointments where these were missed or cancelled. Appointments were offered in person or virtually and at a time of day the participant preferred. A female clinician was available to deliver the intervention should a participant request this. Interpreters were also available at one of the research sites. Within the context of the NHS, future research would need to demonstrate the clinical and cost-effectiveness of delivering the ImRs intervention in a flexible way with a diverse population so that commissioners and healthcare providers could justify implementing the intervention within their service. Failing to do this would risk perpetuating and compounding poorer health outcomes, particularly amongst culturally diverse populations (Napier et al., Reference Napier, Ancarno, Butler, Calabrese, Chater, Chatterjee, Guesnet, Horne, Jacyna and Jadhav2014).
Methodological limitations and future considerations
This study has a number of methodological limitations which should be addressed in future research.
The ImRs intervention protocol only focused on one somatic flashback, even if a participant reported experiencing several. Future studies should explore whether offering more sessions of ImRs leads to a greater reduction in symptoms for people experiencing multiple somatic flashbacks or people who had had high numbers of traumatic experiences.
The TASS outcome measure (Milosevic et al., Reference Milosevic, Levy, Alcolado and Radomsky2015) has three items which asked participants to rate how distressing, exhausting, and intrusive they found the intervention. Participants reflected that whilst they felt the intervention was distressing, exhausting, and intrusive, this felt unavoidable when working with their PTSD memories and did not make the intervention feel less acceptable to them. This context is not captured within the TAAS scores and can result in a score that suggests the intervention was less acceptable than what participants experienced. Using a mixed method approach in future research, considered a more valuable strategy in feasibility research (Donald, Reference Donald2018), would gather rich qualitative data about how the intervention is experienced and give context to ratings on the TAAS.
In addition to the limitations mentioned above of the VAS measure, as mentioned in Clarke et al. (Reference Clarke, Kelly and Hardy2022), the VAS used in this study did not specify specific emotions. Any changes in scores, therefore, do not capture shifts in emotions. This is important to capture as certain emotions (such as guilt and shame) can play a role in maintaining PTSD symptoms (Cunningham, Reference Cunningham2020), and a shift away from these emotions may indicate the positive processing and updating of the trauma memory. Future research would benefit from specifying the emotion(s) being rated within the VAS. The VAS used in this study also did not specify the main sensations experienced during the somatic flashback, such as pressure and heat. Future research could benefit from recording the main sensations experienced during the somatic flashback to understand if certain sensations respond to the ImRs intervention more than others.
Due to the small sample size in the study and lack of control, secondary outcome results should be interpreted with caution. Future research should use an increased sample and a more rigorous study design (randomised control trial).
Conclusion
In conclusion, this study suggests that a brief ImRs intervention for somatic flashbacks is feasible, safe, and acceptable. All six participants who completed the intervention rated it as acceptable, and overall improvements were observed in their somatic flashback symptoms. The findings build upon the existing literature, indicating that ImRs is an effective intervention for symptoms of PTSD. The ImRs intervention for somatic flashbacks could complement existing therapies and lead to more effective treatment protocols for a specific symptom that has been overlooked in the existing literature. It could be used as a brief but effective intervention and integrated into existing treatments (Tf-CBT or EMDR) or developed into a stand-alone intervention. Future research is needed to explore the prevalence of somatic flashbacks, how to measure these more effectively, the underlying mechanisms of ImRs, the optimal intervention protocol, and if this can be integrated into existing trauma therapies.
Key practice points
-
(1) The brief ImRs intervention for somatic flashbacks was feasible, safe, and acceptable.
-
(2) Overall improvements were observed in somatic flashback symptoms.
-
(3) The ImRs intervention for somatic flashbacks could complement existing therapies and lead to more effective treatment protocols.
-
(4) Further research into ImRs interventions for somatic flashbacks is needed to explore its efficacy.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1754470X26100610
Data availability statement
The data that support the findings of this study are openly available in figshare at: http://doi.org/10.6084/m9.figshare.29963297
Acknowledgements
None.
Author contributions
Joe Campbell: Conceptualization (equal), Data curation (lead), Formal analysis (lead), Investigation (lead), Methodology (equal), Project administration (lead), Writing - original draft (lead), Writing - review & editing (equal); Livia Ottisova: Conceptualization (equal), Methodology (equal), Supervision (lead), Writing - original draft (supporting), Writing - review & editing (equal); Kerry Ann Young: Conceptualization (supporting), Methodology (supporting), Supervision (supporting), Writing - review & editing (equal); Francesca Brady: Conceptualization (equal), Methodology (equal), Supervision (supporting), Writing - original draft (supporting), Writing - review & editing (equal).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
All authors abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. Ethical approval was obtained from the East of England-Essex Research Ethics Committee (REF: 23/EE/0125) and the Health Research Authority (HRA). The protocol was registered on clinicaltrials.gov (REF: NCT05996913). All participants recruited into the study provided informed consent. There was a potential ethical issue that taking part in the ImRs intervention could destabilise a participant whilst they were on the waiting list for trauma-focused therapy (i.e. they might experience an increase in PTSD symptoms and distress associated with this). This was closely monitored by the researcher delivering the intervention (J.C.), a trainee clinical psychologist and registered Cognitive Behavioural Therapy therapist and EMDR therapist.



 Open access
Open access
Comments
No Comments have been published for this article.