


Introduction
Healthcare-associated infections (HAIs) are among the most frequent adverse events affecting hospitalized patients worldwide, contributing to morbidity, mortality, prolonged length of stay, and increased costs. Reference Allegranzi, Bagheri Nejad and Combescure1,2 High-touch surfaces in patient rooms, such as door handles, tabletops, and bed rails, can harbor pathogenic organisms and serve as reservoirs for transmission. Copper surfaces possess potent antimicrobial properties, with demonstrated in vitro activity against a broad range of healthcare-associated pathogens including bacteria and viruses. Reference Warnes, Caves and Keevil3–Reference Grass, Rensing and Solioz5 In 2008, the U.S. Environmental Protection Agency (EPA) registered copper and certain copper alloys as antimicrobial materials with public health claims, capable of killing >99.9% of specific pathogens within two hours and providing continuous antimicrobial activity between routine cleaning cycles. 6,Reference Vincent, Duval, Hartemann and Engels-Deutsch7 Its efficacy was substantiated by a multicenter randomized controlled trial demonstrating significant reductions in bioburden and HAIs. Reference Schmidt, Attaway Iii, Fairey, Steed, Michels and Salgado8 Subsequent studies assessing copper surfaces in clinical environments have been observational, with mixed findings. Reference Aillón-García, Parga-Landa and Guillén-Grima9,Reference Albarqouni, Byambasuren, Clark, Scott, Looke and Glasziou10
Most studies have evaluated copper in adult settings, and generalizability to pediatric hospitals remains uncertain as they differ in patient characteristics, caregiver involvement, and contact patterns, which influence environmental contamination and transmission dynamics. Reference Zingg, Hopkins and Gayet-Ageron11,Reference Siegel and Grossman12 Rooming-in of family members, increased exposure to bodily secretions, and higher prevalence of community-acquired infections may increase transmission risk. Reference Koutlakis-Barron and Hayden13,Reference Hussein, Khakoo and Hobbs14 Evidence evaluating copper in pediatric populations is limited, with the only existing studies conducted in a Chilean pediatric intensive care unit (PICU) with high baseline microbial burden and environmental cleaning only on patient discharge. Reference Schmidt, von Dessauer and Benavente15,Reference von Dessauer, Navarrete, Benadof, Benavente and Schmidt16 These studies found reduced microbial burden after installation of copper surfaces and a nonsignificant trend toward lower HAI rates. Whether copper can provide benefits in higher-resource pediatric settings with single-occupancy rooms and daily cleaning remains unclear.
The primary objective of this observational cohort study was to assess the impact of spray-on copper coating on environmental microbial burden on high-touch surfaces of a high-acuity pediatric tertiary inpatient setting. The secondary objective was to assess the effect on HAI rates.
Methods
Study design and setting
This observational cohort study was conducted from September 2018 to April 2020 at BC Children’s Hospital, a pediatric tertiary care facility in Vancouver, Canada. The study rooms were in a new building that had opened in October 2017. Twenty single-occupancy rooms were selected: ten in the PICU and ten in the oncology, hematology, and bone marrow transplant unit. Within each unit, five rooms received spray-on copper coating on high-touch surfaces, and five comparable rooms (matched for location on the unit, layout, and other design elements) served as controls. Patients were admitted to study rooms according to routine hospital bed management practices, based on availability, clinical acuity, infection prevention and control (IPAC) requirements, and unit-specific workflows. Room assignment was not randomized or blinded, and copper-coated rooms were visually distinguishable. There were no exclusion criteria. Informed consent was not required; families were provided an information sheet during environmental sampling. The study was approved by the Children’s and Women’s Research Ethics Board (H17-01801).
Copper surface application
Spray-on copper coating (LuminOre CopperTouchTM, 62.5% copper by weight) was applied to high-touch surfaces in five PICU rooms and five oncology rooms (‘copper rooms’) prior to study initiation (March 2018). Coated surfaces included bed rails, headboards, footboards, over-bed tables, toilet seats, and toilet grab bars (fixed and swing). Surfaces were not recoated during the study. Routine cleaning and disinfection practices were consistent across rooms and followed institutional protocols. High-touch surfaces were cleaned at least daily using hospital-approved disinfectants; sporicidal agents were used only in rooms of patients with Clostridioides difficile infection or carbapenemase-producing organisms. No additional environmental interventions (eg, ultraviolet disinfection) were implemented during the study period.
Data and sample collection
Baseline patient characteristics were retrospectively collected for up to the first five admissions per month to each study room, with fewer included when occupancy was lower. Variables potentially influencing environmental microbial burden or HAI risk were collected, including patient age, diagnosis, length of stay, colonization with antibiotic-resistant organisms (AROs), and use of central venous catheters or total parenteral nutrition.
Environmental sampling was conducted randomly on 28 occasions between January and December 2019 based on study personnel and laboratory availability. On each occasion, all study rooms that were occupied and accessible at the time of collection were sampled. Predefined 100 cm2 areas on designated high-touch surfaces were swabbed using premoistened sterile swabs and 10 x 10 cm or 4 x 25 cm plastic templates. Surfaces were swabbed with uniform pressure using five horizontal and five vertical strokes. Each swab was vortexed in Dey-Engley neutralizing broth, and 100-µL were plated on blood agar and incubated for 48 hours at 35–37°C. Reference Chai, Donnelly, Wong and Bryce17 The outcome was total microbial burden (colony-forming units [CFU]/100 cm2). The key exposure variable was room type (copper vs control). The collection date, surface, room type, and unit-level HAI rate (per 10,000 patient-days) at the time of sampling were also recorded as the potential confounders, when assessing the association between room type and total microbial burden. Sampling was not blinded to coating status and baseline environmental sampling prior to copper application was not performed.
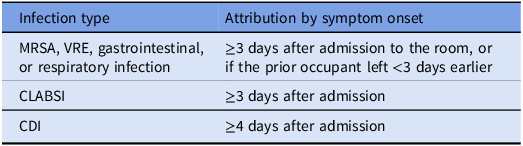
HAI data were obtained from the hospital’s surveillance database for copper rooms, control rooms, and all other inpatient rooms in the hospital. The HAIs included for analysis were those captured reliably within the surveillance system and most plausibly associated with environmental transmission. Room assignments for the seven days preceding HAI onset were reviewed and infections were attributed to the room type where the patient spent the majority of the incubation period. This attribution approach represents a pragmatic adaptation of standard surveillance definitions following institutional surveillance protocols, based on the National Healthcare Safety Network criteria (Table 1). Reference Horan, Andrus and Dudeck18
Definitions of healthcare-associated infections by timing of symptom onset

Table 1 Long description
A table with two columns and three rows. The first column is labeled Infection type and the second column is labeled Attribution by symptom onset. Row 1: Infection type, MRSA, VRE, gastrointestinal, or respiratory infection; Attribution by symptom onset, 3 days after admission to the room, or if the prior occupant left less than 3 days earlier. Row 2: Infection type, CLABSI; Attribution by symptom onset, 3 days after admission. Row 3: Infection type, CDI; Attribution by symptom onset, 4 days after admission.
MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococci; CLABSI, central line–associated bloodstream infection; CDI, Clostridioides difficile infection.
Statistical methods
Sample size calculation and statistical analysis
Sample size calculations were based on log-transformed data from Schmidt et al., indicating that 100 independent observations (50 per group) would detect an 80% reduction in average CFU/100 cm2 with adequate power. Reference Schmidt, Attaway and Sharpe19 Assuming intraclass correlation ≤ .09, a total of approximately 1,000 samples across the 20 study rooms was deemed sufficient.
Baseline characteristics analysis
Baseline characteristics were summarized using descriptive statistics. Comparison between groups used the two-sample t-test or Wilcoxon rank-sum test for continuous variables and Pearson’s χ2 test or Fisher’s exact test for categorical variables. Statistical significance was defined as P < .05.
Environmental sampling analysis
Total microbial burden (CFU/100 cm2) on copper surfaces was compared to control surfaces. A negative binomial mixed-effects model was used to account for overdispersion and repeated measures, where potential confounders were adjusted. Results were summarized as RRs with corresponding 95% CIs and displayed graphically.
An absolute measure of effect (absolute rate difference, ARD) was also assessed, where the adjusted mean predicted counts for each arm were calculated from the model, and their absolute difference was derived. To obtain robust confidence intervals for the ARD, a nonparametric cluster bootstrap approach was applied. Specifically, rooms were resampled with replacement 1,000 times, the model was refit in each bootstrap replicate, and the adjusted means and their difference were re-estimated. The 2.5th and 97.5th percentiles of the bootstrap distribution were used to construct a 95% confidence interval for the ARD. Analyses were conducted using SAS 9.4 (SAS Institute Inc, Cary, NC).
Healthcare-associated infection analysis
HAI incidence (infection per 10,000 inpatient days) for the copper intervention was compared with those in control rooms and in non-copper rooms (ie, control rooms and other rooms in the hospital), respectively. For this comparison, the monthly count of infections was modeled using Poisson regression, with the room type included as the exposure variable and inpatient days for each month included as an offset. Effect estimates were presented as rate ratios (RRs) with corresponding 95% confidence intervals (CIs).
Results
Baseline patient characteristics
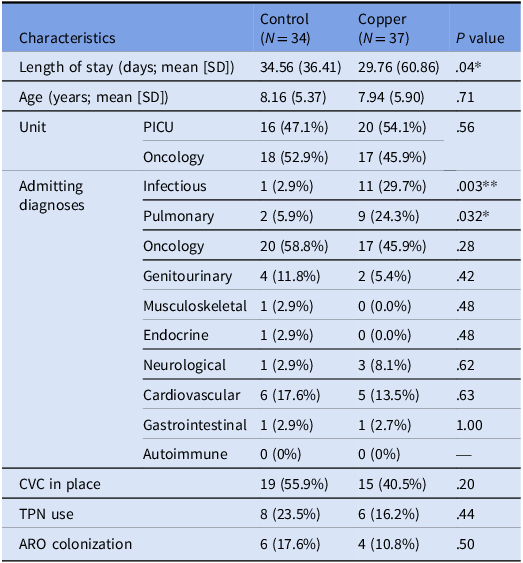
Seventy-one patients were included in this analysis—34 admitted to control rooms, 37 to intervention (copper-coated) rooms—representing up to the first five admissions per month during the study period. At baseline, patients in the intervention rooms were more likely to be admitted with an infectious diagnosis (29.7% vs 2.9%; P = .003) or pulmonary disease (24.3% vs 5.9%; P = .032) and had a shorter mean length of stay (29.76 vs 34.56 days; P = .04). No other characteristics differed significantly between groups (Table 2). There were no missing data for any baseline characteristics, environmental sampling variables, or HAI outcomes.
Demographic and clinical characteristics of the first five monthly admissions per study arm. All values shown as n (%) unless otherwise specified

Table 2 Long description
A table comparing demographic and clinical characteristics of patients in control and copper-coated rooms. The table has 15 rows and 5 columns. The columns are labeled Characteristics, Control (N = 34), Copper (N = 37), and P value. The rows are labeled with various characteristics such as Length of stay, Age, Unit, Admitting diagnoses, CVC in place, TPN use, and ARO colonization. Each row provides specific data for the Control and Copper groups, along with the P value indicating statistical significance. Notable trends include a shorter mean length of stay in the Copper group (29.76 days) compared to the Control group (34.56 days) with a P value of .04. Patients in the Copper group were more likely to be admitted with an infectious diagnosis (29.7% vs 2.9%) and pulmonary disease (24.3% vs 5.9%), with P values of .003 and .032, respectively.
LOS, length of stay; PICU, pediatric intensive care unit; ARO, antibiotic-resistant organisms; CVC, central venous catheter; TPN, total parenteral nutrition.
* Statistically significant at P < .05.
** Statistically significant at P < .01.
Environmental sampling
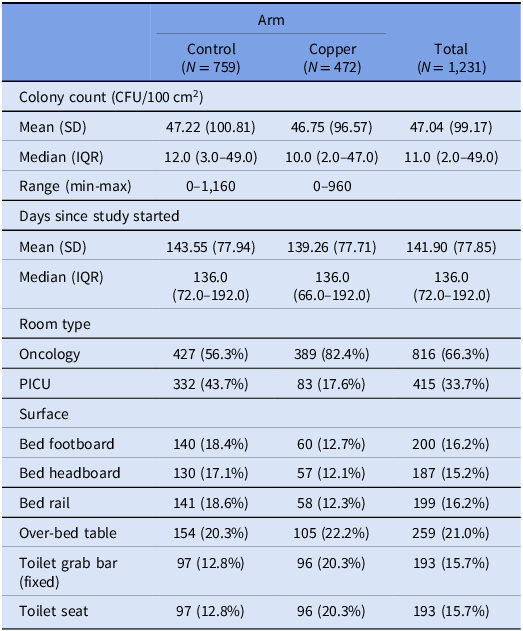
A total of 1,231 surface samples were collected: 759 from control rooms and 472 from copper-treated rooms (Table 3). Mean CFU counts were similar between groups, with substantial variability (mean [SD]: 47.22 [100.81] in control rooms vs 46.75 [96.57] in copper (Figure 1)). Most samples originated from oncology rooms (66.3% overall), with a higher proportion in the copper arm (82.4% copper vs 56.3% control). Sampling was distributed throughout the study period, with more frequent sampling early in the study (median 136 days after study initiation).
Scatterplot of raw colony-forming unit (CFU) counts/100 cm2 by study day and intervention arm. Each point represents a surface sample collected on a given day since study initiation. Control (circles, top panel) and copper-treated (crosses, bottom panel) rooms show substantial variability in bioburden over time, with several high outliers observed in both groups. Sampling was distributed throughout the one-year study period, with more frequent data collection occurring earlier in the study.

Figure 1 Long description
The image contains two scatterplots. Panel A: The top scatterplot represents the control group. The x-axis is labeled Days since Study Start, ranging from 0 to 360. The y-axis is labeled Raw CFU Count, ranging from 0 to 1250. Each point represents a surface sample collected on a given day, marked with open circles. The data shows substantial variability in bioburden over time, with several high outliers observed. Panel B: The bottom scatterplot represents the copper-treated group. The x-axis is labeled Days since Study Start, ranging from 0 to 360. The y-axis is labeled Raw CFU Count, ranging from 0 to 1250. Each point represents a surface sample collected on a given day, marked with crosses. The data also shows substantial variability in bioburden over time, with several high outliers observed. Sampling was distributed throughout the one-year study period, with more frequent data collection occurring earlier in the study.
Environmental sampling descriptive analysis. All values shown as n (%) unless otherwise specified

Table 3 Long description
A table comparing environmental sampling data between control and copper-treated rooms. The table has 12 rows and 5 columns. Column headers are Arm, Colony count (CFU/100 cm2), Days since study started, Room type, and Surface. Row labels include Control (N = 759), Copper (N = 472), and Total (N = 1,231). Row 1: Colony count (CFU/100 cm2), Mean (SD), Control: 47.22 (100.81), Copper: 46.75 (96.57), Total: 47.04 (99.17). Row 2: Colony count (CFU/100 cm2), Median (IQR), Control: 12.0 (3.0–49.0), Copper: 10.0 (2.0–47.0), Total: 11.0 (2.0–49.0). Row 3: Colony count (CFU/100 cm2), Range (min-max), Control: 0–1,160, Copper: 0–960, Total: 0–1,160. Row 4: Days since study started, Mean (SD), Control: 143.55 (77.94), Copper: 139.26 (77.71), Total: 141.90 (77.85). Row 5: Days since study started, Median (IQR), Control: 136.0 (72.0–192.0), Copper: 136.0 (66.0–192.0), Total: 136.0 (72.0–192.0). Row 6: Room type, Oncology, Control: 427 (56.3 percent), Copper: 389 (82.4 percent), Total: 816 (66.3 percent). Row 7: Room type, PICU, Control: 332 (43.7 percent), Copper: 83 (17.6 percent), Total: 415 (33.7 percent). Row 8: Surface, Bed footboard, Control: 140 (18.4 percent), Copper: 60 (12.7 percent), Total: 200 (16.2 percent). Row 9: Surface, Bed headboard, Control: 130 (17.1 percent), Copper: 57 (12.1 percent), Total: 187 (15.2 percent). Row 10: Surface, Bed rail, Control: 141 (18.6 percent), Copper: 58 (12.3 percent), Total: 199 (16.2 percent). Row 11: Surface, Over-bed table, Control: 154 (20.3 percent), Copper: 105 (22.2 percent), Total: 259 (21.0 percent). Row 12: Surface, Toilet grab bar (fixed), Control: 97 (12.8 percent), Copper: 96 (20.3 percent), Total: 193 (15.7 percent). Row 13: Surface, Toilet seat, Control: 97 (12.8 percent), Copper: 96 (20.3 percent), Total: 193 (15.7 percent).
CFU, colony-forming units; IQR, interquartile range; PICU, pediatric intensive care unit.
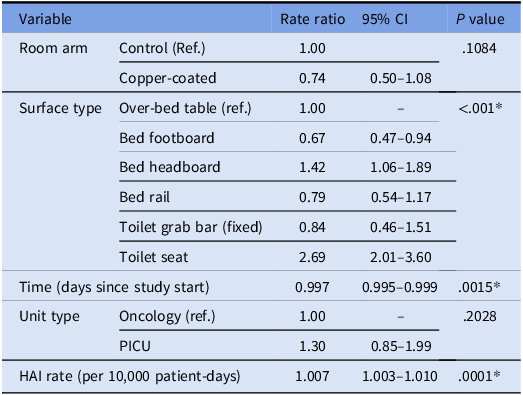
After adjusting for HAI and room type covariates, the colony count in copper rooms was 26% lower than in control rooms, though this difference was not statistically significant (RR 0.74; 95% CI .50–1.08; P = .11; Table 4, Figure 2; ARD -12.25; 95% CI -26.12–2.10). Colony counts varied significantly by surface type: compared to over-bed tables, the footboard had 33% lower counts (RR 0.67; 95% CI 0.47–0.94; P < .001), and the headboard had 42% higher counts (RR 1.42, 95% CI 1.06–1.89; P < .001). The toilet seat had the highest colony counts—169% higher than the over-bed table (RR 2.69; 95% CI 2.01–3.60; P < .001). There was a decrease in colony counts over time (0.3% per day; RR 0.997, 95% CI 0.995–0.999; P = .0015) and higher HAI rates were associated with higher colony counts (RR 1.007 per 10,000 inpatient days; 95% CI 1.003–1.010; P = .0001).
A conditional effect plot showing the trend of colony-forming unit (CFU) counts in copper and control rooms by surface type, controlling for the covariates of healthcare-associated infections and room type. Lines represent modeled CFU trends, with shaded areas indicating 95% confidence intervals. Dashed lines indicate copper-treated surfaces; solid lines indicate control surfaces. CFU, colony forming units; CI, confidence interval.

Figure 2 Long description
The image contains six line graphs showing the trend of estimated colony-forming unit (CFU) counts on different surfaces in healthcare settings over time. Each graph represents a different surface type: Bed foot board, Bed head board, Bed rail, Over bed table, Toilet grab bar (fixed), and Toilet seat. The x-axis represents days since the study start, ranging from 0 to 3600 days. The y-axis represents the estimated CFU count, ranging from 0 to 250. Each graph includes two lines: a solid line for control surfaces and a dashed line for copper-treated surfaces. Shaded areas around the lines indicate 95% confidence intervals. The graphs show a general trend of decreasing CFU counts over time for both control and copper-treated surfaces, with copper-treated surfaces consistently showing lower CFU counts compared to control surfaces.
Factors associated with microbial burden (using a negative binomial mixed-effects model)

Table 4 Long description
The table presents data on factors associated with microbial burden using a negative binomial mixed-effects model. It has 6 rows and 4 columns. The columns are labeled Variable, Rate ratio, 95% CI, and P value. The variables include Room arm, Surface type, Time (days since study start), Unit type, and HAI rate (per 10,000 patient-days). Row 1: Room arm, Control (Ref.), 1.00, .1084. Row 2: Room arm, Copper-coated, 0.74, 0.50–1.08. Row 3: Surface type, Over-bed table (ref.), 1.00, <.001*. Row 4: Surface type, Bed footboard, 0.67, 0.47–0.94. Row 5: Surface type, Bed headboard, 1.42, 1.06–1.89. Row 6: Surface type, Bed rail, 0.79, 0.54–1.17. Row 7: Surface type, Toilet grab bar (fixed), 0.84, 0.46–1.51. Row 8: Surface type, Toilet seat, 2.69, 2.01–3.60. Row 9: Time (days since study start), 0.997, 0.995–0.999, .0015*. Row 10: Unit type, Oncology (ref.), 1.00, .2028. Row 11: Unit type, PICU, 1.30, 0.85–1.99. Row 12: HAI rate (per 10,000 patient-days), 1.007, 1.003–1.010, .0001*.
CI, confidence interval; Ref., reference value; PICU, pediatric intensive care unit; HAI, healthcare-associated infection.
* Statistically significant at P < .01.
Healthcare-associated infection (HAI) rates
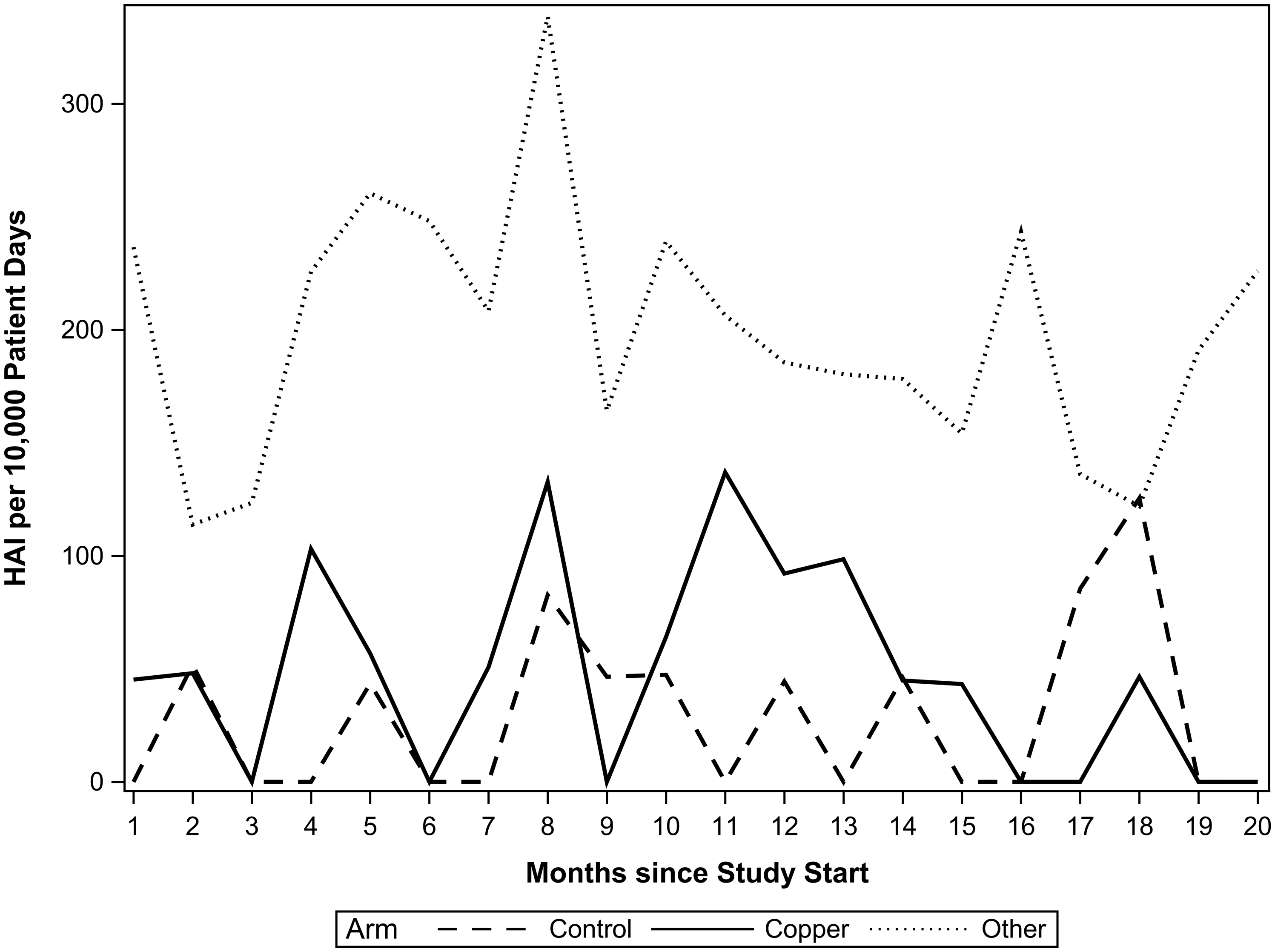
HAI rates were higher in intervention rooms compared to control rooms, though this difference was not statistically significant (48.2 vs 30.5 cases per 10,000 patient-days; risk ratio 1.58; 95% CI: 0.78–3.20; P = .20; Figure 3). When compared to all other hospital rooms combined (including control and non-study rooms), copper-coated rooms had significantly lower HAI rates (48.2 vs 146.5 cases per 10,000 patient days; RR 0.33; 95% CI 0.21–0.53; P < .0001).
Trends in healthcare-associated infection (HAI) rates per 10,000 patient days over time by study arm: control (dashed line), copper (solid line), and other (dotted line), from September 2018 to April 2020. In this model, “Other” is all the non-study rooms in the hospital (neither control nor copper). HAI, healthcare-associated infections.

Discussion
In this observational cohort study, spray-on copper applied to high-touch surfaces did not significantly reduce microbial load or HAI rates. Effect estimates for microbial load (RR 0.50–1.08) suggest a possible reduction in surface contamination, whereas HAI risk ratios (0.78–3.20) indicate a nonsignificant trend toward higher infection rates, with greater uncertainty around this outcome. Several contextual factors likely contributed to these findings. First, the study was conducted in a newly constructed building with low baseline bioburden. Median colony counts on control surfaces (∼47 CFU/100 cm2) were substantially lower than prior studies used for sample size calculations, which reported CFU counts in the thousands, thus limiting measurable reductions and statistical power. Second, more frequent cleaning (once- or twice-daily) compared to previously published studies (terminal cleaning only) may have reduced the incremental benefit of copper surfaces. Third, single-bed room design likely reduced cross-contamination compared with multibed settings previously studied. Differences in geography, demographics, microbiology, and specific copper products used may have further contributed to the absence of statistically significant benefit.
Evidence in pediatric settings remains limited. The Chilean PICU study reported a 99% reduction in microbial burden (1.996 log10 reduction) following installation of solid copper alloys on five high-touch surfaces, contrasting with our findings. Reference Schmidt, von Dessauer and Benavente15 As highlighted above, differences in baseline bioburden, cleaning practices, and room design likely explain these discrepancies. Copper efficacy also varies by formulation. EPA-registered copper alloys, copper-impregnated materials, and spray coatings differ in antimicrobial durability. Our study used a spray-coated product selected for cost and feasibility, whereas other studies used solid alloys. Prior work suggests that integral or alloy-based copper demonstrate more consistent and durable antimicrobial activity compared with coating-based applications. Reference Bryce, Velapatino and Donnelly-Pierce20,Reference Bryce, Velapatino and Donnelly-Pierce21 Variability in coating composition and application technique (eg, cold spray application) can further influence performance. Reference Champagne and Helfritch22 We did not independently verify antimicrobial efficacy postapplication and cannot exclude variability in coating effectiveness contributing to the lack of observed effect in our study.
Evidence for HAI outcomes in pediatric studies is also sparse. A follow-up analysis of the Chilean PICU cohort found a nonsignificant trend toward lower HAI rates in copper rooms (relative risk reduction 0.26; 90% CI −0.06–0.48). Reference von Dessauer, Navarrete, Benadof, Benavente and Schmidt16 In contrast, our data showed a nonsignificant increase in HAIs in copper rooms compared to controls (48.2 vs 30.48 cases per 10,000 patient days). This may reflect baseline differences between patients rather than a true adverse effect. Patients admitted to copper rooms more often had infectious or pulmonary diagnoses, suggesting higher HAI risk. Nonrandomized allocation and lack of blinding may have contributed to this imbalance. The low overall number of HAI cases further limited statistical power to detect true differences between groups. While the study was powered for environmental sampling, it was not designed to detect differences in HAI rates. Notably, both copper and control rooms exhibited lower HAI rates than the hospital-wide average, suggesting that newer infrastructure and enhanced IPAC practices in these units may have played a role. These findings underscore the complex interplay between environmental interventions and system-level variables when evaluating infection prevention strategies.
This study has several limitations. The lack of randomization introduces potential allocation bias, as patients at higher risk of infection may have been preferentially assigned to copper rooms. This is supported by baseline imbalances in patient characteristics. Although analyses adjusted for available covariates, residual confounding likely remains, limiting causal interpretation. However, detection bias was limited by a standardized hospitalwide surveillance program. We could not account for prior healthcare exposure or contamination from previous room occupants, including AROs. Baseline environmental sampling was not performed, preventing within-room comparisons. Low event counts precluded organism-specific analyses. Sampling imbalance between study arms may have influenced microbial estimates. Adherence to cleaning, hand hygiene, and other IPAC measures were not measured and may have contributed to residual confounding. Finally, the low baseline bioburden may have constrained detection of meaningful effects.
Before widespread implementation, cost-effectiveness analyses are warranted, given the uncertain benefit of copper surfaces in pediatric settings with strong IPAC programs. Real-world studies such as this provide valuable insight into performance under routine conditions. Given the multifactorial nature of HAI transmission, environmental interventions such as copper should be considered within the context of broader IPAC strategies.
In summary, spray-coated copper surfaces in a pediatric tertiary care hospital were not associated with statistically significant reductions in microbial burden or HAIs, although surface contamination trended lower in copper-treated rooms. The apparent trend toward increased HAI rates may reflect baseline differences, low HAI incidence, and variability in coating efficacy rather than a true adverse effect. These findings suggest limited incremental benefit of copper surfaces in settings with low baseline bioburden and robust IPAC practices. However, the results do not exclude potential benefit in other clinical settings. Future research should prioritize randomized designs, longer follow-up, and higher risk pediatric settings to better define the role of copper in HAI prevention.
Acknowledgements
The authors thank Jeffrey Bone, PhD, for his contributions to the statistical analysis.
Financial support
This work was funded by the Provincial Health Services Authority of British Columbia. QM received a summer student research award from the University of British Columbia Department of Pathology and Laboratory Medicine.
Competing interests
DMG received a speaker honorarium from Roche diagnostics. The other authors report no conflicts of interest relevant to this article.



 Open access
Open access