


Impact statement
This study provides one of the most comprehensive national assessments of depression among older adults living with cardiovascular disease in Nigeria, offering evidence with direct relevance for patients, families, clinicians and health systems. By demonstrating an exceptionally high burden of depressive symptoms and identifying modifiable social and clinical factors associated with depression, such as medication dependence, alcohol use, comorbidities, illness duration and living arrangements, the research highlights depression as a critical yet overlooked component of cardiovascular care in aging populations. The findings support the urgent integration of routine mental health screening into cardiovascular and geriatric services, particularly in low- and middle-income countries where resources are limited and mental health needs are often unmet. The use of a culturally adapted, multilingual assessment tool shows that context-sensitive approaches are both feasible and reliable, setting a practical model for other diverse settings in sub-Saharan Africa and beyond. Beyond clinical practice, this research informs policymakers by providing nationally representative data that can guide resource allocation, workforce training and the design of integrated mental – cardiac care pathways. It also underscores the protective role of family support, reinforcing the value of low-cost, family-centered and community-based interventions. Internationally, the study contributes to global discussions on healthy aging by illustrating how mental health, chronic disease management and social context intersect, offering insights applicable to aging societies worldwide.
Introduction
With increasing global life expectancy, chronic noncommunicable diseases (NCDs), notably cardiovascular diseases (CVDs), now disproportionately affect older adults (World Health Organization [WHO], 2025). In low- and middle-income countries (LMICs) like Nigeria, this epidemiological shift has coincided with a growing yet under-addressed need for geriatric mental health services (Ojo et al., Reference Ojo, Ojji, Grobbee, Huffman and Peters2024). Depression, a prevalent neuropsychiatric disorder in later life, frequently coexists with chronic physical illnesses, especially CVD, creating a complex interplay that threatens quality of life, medication adherence, and clinical outcomes (Huffman et al., Reference Huffman, Celano, Beach, Motiwala and Januzzi2013; Yuyun et al., Reference Yuyun, Sliwa, Kengne, Mocumbi and Bukhman2020; Berimavandi et al., Reference Berimavandi, Abbasi, Khaledi-Paveh and Salari2025). Globally, depression is a leading cause of disability-adjusted life years (DALYs) among older adults, often underdiagnosed due to symptom overlap with chronic illnesses (WHO, 2025). Among older adults with CVD, depression is associated with increased morbidity, functional decline, poor treatment adherence and higher mortality (Bahall, Reference Bahall2019; Subih et al., Reference Subih, Abu Saleh and Malak2023; Komuro et al., Reference Komuro, Komuro, Kaneko, Suzuki, Okada, Fujiu, Takeda, Morita, Node, Yasunaga, Komuro, Ieda and Takeda2025). A systematic review found that older CVD patients are up to three times more likely to experience depression than those without chronic conditions (Huffman et al., Reference Huffman, Celano, Beach, Motiwala and Januzzi2013).
In sub-Saharan Africa, studies report depression prevalence rates ranging from 30% to 60% in older adults with chronic diseases (Igbokwe et al., Reference Igbokwe, Ejeh, Agbaje, Umoke, Iweama and Ozoemena2020; Falade et al., Reference Falade, Oyebanji, Oshatimi, Babatola, Orekoya, Eegunranti and Falade2022). However, nationally representative data from Nigeria, particularly on older adults with CVD, remain limited. Key risk factors such as social isolation, alcohol use and inadequate family support have been identified as major contributors to mental health decline in this group (Nakua et al., Reference Nakua, Amissah, Tawiah, Barnie, Donkor and Mock2023; Olabisi et al., Reference Olabisi, Faronbi, Adedeji, Ademuyiwa, Gambari and Lasisi2023). Importantly, depression negatively influences medication adherence. Meta-analyses have shown that depression reduces adherence by up to 40% among older adults with CVD, increasing the likelihood of disease progression and hospital readmission (Subih et al., Reference Subih, Abu Saleh and Malak2023; Berimavandi et al., Reference Berimavandi, Abbasi, Khaledi-Paveh and Salari2025).
Despite growing literature, research in Nigeria is often geographically narrow, and although many studies employ validated instruments, there remain inconsistencies in measurement approaches, and studies rarely consider the sociocultural diversity or multifactorial nature of depression in this demographic (Igbokwe et al., Reference Igbokwe, Ejeh, Agbaje, Umoke, Iweama and Ozoemena2020; Falade et al., Reference Falade, Oyebanji, Oshatimi, Babatola, Orekoya, Eegunranti and Falade2022). There is a critical need for robust, context-sensitive studies that examine the sociodemographic, clinical and psychosocial correlates of depression among older adults with CVD. This study aims to: (1) determine the prevalence of depression among older Nigerian adults receiving CVD care across Nigeria; (2) identify key demographic, clinical and lifestyle factors associated with depression; and (3) examine associations between depression and functional status, medication dependence and other psychosocial variables. Findings from this nationally representative study will inform routine depression screening, integrated mental–cardiac care models and low-cost, family-centered interventions. This research will also contribute to policy dialog and health system strengthening for aging populations in LMICs.
Methods
Study design and setting
This hospital-based, cross-sectional study was conducted between March 2024 and July 2025 across 12 federally accredited tertiary healthcare institutions in Nigeria. The selection of hospitals was strategically based on Nigeria’s six geopolitical zones to ensure national geographic, ethnic and socioeconomic representation of the older adult population. Two institutions were chosen from each zone: South East (Alex Ekwueme Federal University Teaching Hospital [AE-FUTHA], Ebonyi State; University of Nigeria Teaching Hospital [UNTH], Enugu State), North Central (University of Ilorin Teaching Hospital [UITH], Kwara State; Federal Medical Centre [FMC], Makurdi, Benue State), North East (University of Maiduguri Teaching Hospital [UMTH], Borno State; Abubakar Tafawa Balewa University Teaching Hospital [ATBUTH], Bauchi State), North West (Aminu Kano Teaching Hospital [AKTH], Kano State; Ahmadu Bello University Teaching Hospital [ABUTH], Kaduna State), South South (University of Benin Teaching Hospital [UBTH], Edo State; University of Uyo Teaching Hospital [UUTH], Akwa Ibom State) and South West (Lagos University Teaching Hospital [LUTH], Lagos State; Obafemi Awolowo University Teaching Hospitals Complex [OAUTHC], Osun State). Each hospital enrolled 77 participants, culminating in a multicenter sample drawn from 12 federally accredited tertiary hospitals across Nigeria’s six geopolitical zones.
Study population and eligibility criteria
Participants were older adults aged 60 years and above with a confirmed diagnosis of at least one CVD, such as hypertension, coronary artery disease or heart failure. Clinical eligibility was verified through a review of medical records and consultation with attending clinicians. Inclusion criteria also required cognitive and physical ability to participate in an interviewer-administered questionnaire and the provision of informed consent either personally or through a legal representative. Individuals were excluded if they presented with acute delirium or disorientation at the time of recruitment, had a history of severe psychiatric disorders (e.g., schizophrenia or bipolar disorder), were receiving palliative or end-of-life care, had severe cognitive impairments or were experiencing acute medical conditions necessitating emergency intervention.
Sampling technique and sample size determination
A multistage sampling approach was adopted. At the first stage, the six geopolitical zones of Nigeria served as primary clusters. In the second stage, two tertiary hospitals from each zone were purposely selected based on their capacity for geriatric and cardiovascular care and documented adherence to standardized clinical protocols that ensure unbiased, professional management of older adults with CVD. Eligible participants were consecutively recruited from geriatric outpatient clinics at each selected hospital until the site quota of 77 participants was reached. Their accreditation status further justified the selection of institutions, availability of specialist-trained staff and structured care pathways that collectively support consistent and equitable provision of care across all eligible older adults.
The minimum sample size was computed using an adapted version of Cohen’s formula for estimating proportions: n = 1.2SD/M 2, where S = 6% (estimated prevalence of chronic disease among older adults; Uloko et al., Reference Uloko, Musa, Ramalan, Gezawa, Puepet, Uloko, Borodo and Sada2018), D = 94% (complement of S) and M = 0.9 (representing 15% precision of S), yielding a base sample size of 836. Adjusting for a 10% potential nonresponse rate, the final required sample was 924. A total of 918 valid responses were obtained, resulting in a high response rate of 99.4%.
Research instrument
Data collection was conducted using a culturally adapted structured questionnaire, the Depression Assessment Questionnaire (DAQ), which incorporates validated measures including Activities of Daily Living (ADLs) assessed using the Lawton Instrumental Activities of Daily Living (IADL) Scale (Lawton and Brody, Reference Lawton and Brody1969), and the Geriatric Depression Scale–Short Form (GDS-15) (Sheikh and Yesavage, Reference Sheikh and Yesavage1986). The inclusion of the Lawton IADL scale in this study was intended solely to evaluate functional status among older adults and to examine its potential association with depressive symptoms; it was not used as a diagnostic tool for frailty or dementia. All items on the ADL and IADL scales were applied to both male and female participants, with contextual adaptations to reflect culturally relevant tasks for Nigerian older adults.
The DAQ is structured into five sections: Section A: Informed consent (participant or legal proxy); Section B: Demographic information (gathered via caregivers or hospital records); Section C: Clinical history (completed by healthcare professionals); Section D: GDS-15 (administered with caregiver assistance); and Section E: Functional status. The GDS-15 served as a validated screening instrument for identifying depressive symptoms among older adults rather than a diagnostic tool for major depressive disorder. Depression was operationally defined based on the GDS-15 screening threshold, with a cutoff score of ≥5, indicating the presence of depressive symptoms. Participants who screened positive were classified accordingly based on this established cutoff. Formal psychiatric diagnostic assessment using DSM-V criteria was not conducted as part of the study protocol; therefore, findings reflect screened depressive symptomatology rather than clinically confirmed depressive disorder.
The DAQ was culturally and linguistically adapted for Nigerian populations through a rigorous multistep process to ensure semantic equivalence, cultural relevance and preservation of the validated properties of the incorporated scales. First, the instrument was translated from English into Hausa, Yoruba and Igbo by bilingual experts familiar with local sociocultural norms. Back-translation into English was performed to verify semantic accuracy, and simplified English wording was applied where necessary to enhance comprehension among older adults with varying literacy levels. Contextual modifications included adapting examples of daily activities in the ADL and IADL sections to reflect tasks commonly performed by Nigerian older adults (e.g., local food preparation methods, modes of transportation and culturally relevant social interactions). Items that could be gender-specific were reviewed and modified so that all participants, regardless of sex, could respond meaningfully.
Reliability was assessed using internal consistency for the individual scales incorporated within the DAQ rather than for the questionnaire as a whole. The GDS-15 demonstrated high internal consistency (Cronbach’s α = 0.83), indicating reliable measurement of depressive symptoms among participants, while the Lawton IADL Scale showed acceptable reliability for assessing functional status within this population. These modifications ensured that the DAQ reliably and equitably assessed both depression and functional status in the Nigerian context.
A pilot test with 20 older adults was conducted to ensure clarity and cultural relevance, and content validity was assessed by an expert panel of nine doctoral-level public health professionals. Overall reliability of the DAQ was confirmed (Cronbach’s α = 0.83), demonstrating consistent measurement of the study constructs.
Data collection procedure
Data collection was executed by 36 trained research assistants, organized into three-person teams at each participating hospital. All assistants were registered nurses employed at the respective institutions and underwent a structured 45-min training session conducted by the principal investigator. This training included demonstrations of standardized questionnaire administration, role-playing exercises, detailed guidance on informed consent procedures, strategies to minimize interviewer bias and methods for handling culturally sensitive topics. Each team also received written training manuals, and a question-and-answer session was conducted to clarify procedures. Emphasis was placed on consistent administration across all sites and strict adherence to ethical and confidentiality protocols. While not all research assistants were literate in Hausa, Yoruba and Igbo, each team was composed to ensure coverage of the local language(s) relevant to the hospital’s catchment area, allowing interviews to be conducted in participants’ preferred language without compromising comprehension or data quality. Interviews were conducted in a confidential setting during routine geriatric outpatient visits, ensuring accurate and culturally appropriate administration of the DAQ across all study sites.
Ethical considerations
The study adhered to the ethical principles outlined in the Declaration of Helsinki (World Medical Association, 2013) and the Ethical Guidelines of the American Psychological Association (2017). Ethical clearance was obtained from the Federal Ethics Committee of Nigeria (Reference: REC/FE/2024/00061), and administrative approvals were granted by the Chief Medical Directors of all participating hospitals. Written informed consent was obtained from each participant or their legal representative. Participants were assured of voluntary participation, their right to withdraw at any time and guaranteed confidentiality and anonymity. No financial or material incentives were offered.
Data analysis
All data were entered and analyzed using IBM SPSS Statistics Version 28 (IBM, 2021). Descriptive statistics, including frequencies and percentages, were computed to summarize participants’ demographic and clinical characteristics. Bivariate analyses were conducted using chi-square tests to explore associations between depression and sociodemographic or clinical variables. Variables with statistically significant bivariate relationships were further examined using binary logistic regression to identify factors independently associated with depressive symptoms. Additionally, chi-square analyses were performed to examine regional differences in the prevalence of depressive symptoms across Nigeria’s six geopolitical zones. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated. Statistical significance was established at a p-value <0.05. In this study, “depression” refers to depressive symptoms identified using the GDS-15 screening threshold rather than a formal DSM-V diagnosis. Because structured psychiatric interviews were not performed, findings should be interpreted as reflecting the prevalence of depressive symptoms among older adults with cardiovascular disease. Given the cross-sectional design, regression analyses were used to examine associations rather than infer causality. The analytical procedures were sufficiently powered, achieving 80% power at a 5% significance level. Missing data were minimal (<5%) and addressed through listwise deletion. All analyses were conducted in accordance with the STROBE guidelines (von Elm et al., Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke2008).
Results
Participant characteristics
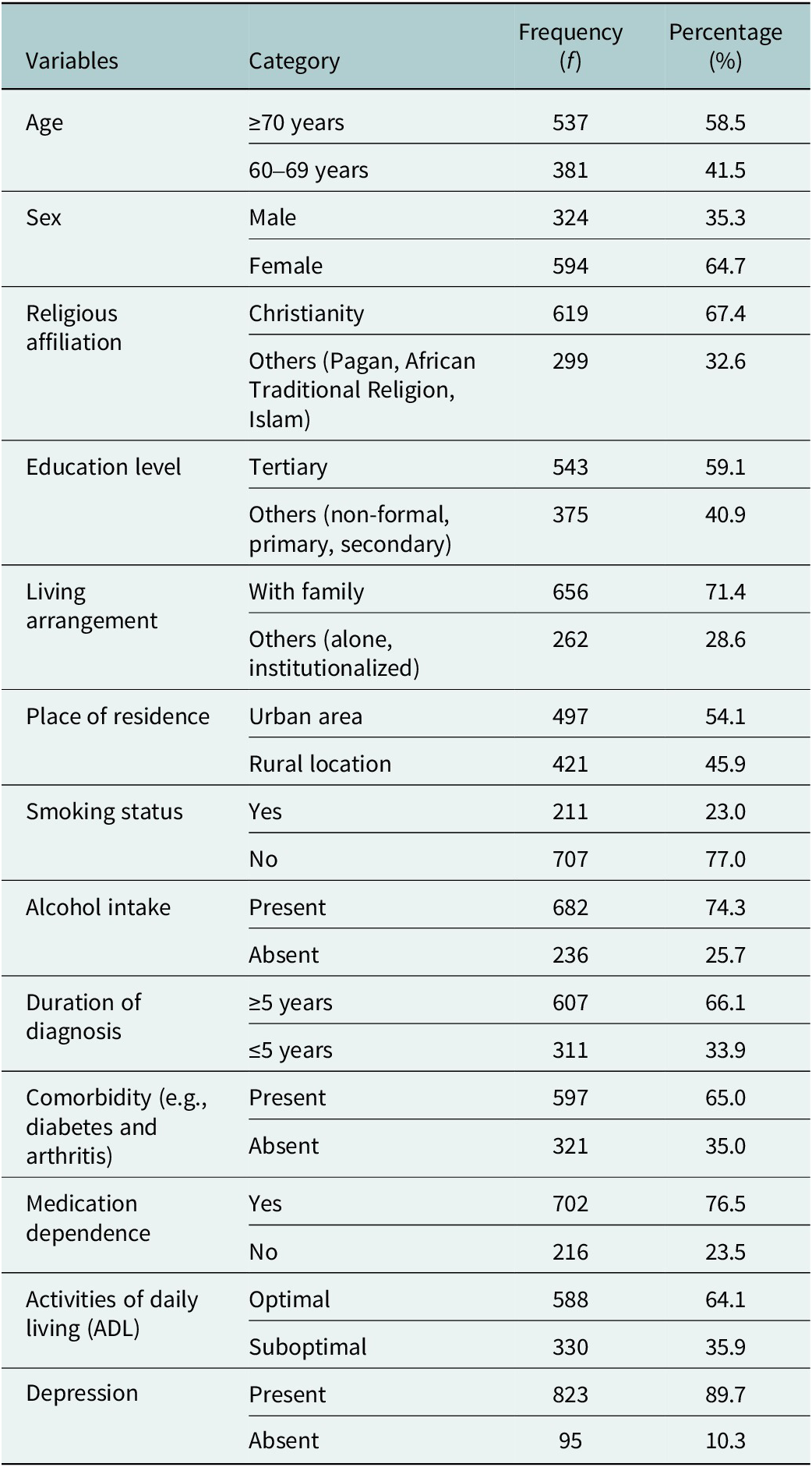
A total of 918 older adults with clinically confirmed cardiovascular diseases were successfully surveyed across 12 federally accredited tertiary hospitals in Nigeria, yielding a high response rate of 99.4%. The mean age of respondents was 71.3 years (SD = 7.2), with a majority aged 70 years and above (n = 537; 58.5%). Females represented a greater proportion of the sample (n = 594; 64.7%) compared to males (n = 324; 35.3%). Most participants identified as Christian (n = 619; 67.4%) and had attained tertiary-level education (n = 543; 59.1%). Regarding living conditions, 71.4% of respondents (n = 656) resided with family members, while the remaining 28.6% either lived alone or were institutionalized. Urban residency was reported by 54.1% of the sample (n = 497), and 45.9% (n = 421) lived in rural areas. Clinically, two-thirds of participants (n = 607; 66.1%) had been diagnosed with cardiovascular disease for 5 years or longer. A majority also reported at least one comorbid condition, such as diabetes or arthritis (n = 597; 65.0%). Dependence on prescribed medication was notably high, with 76.5% (n = 702) reporting regular medication use. Functional status varied, with 35.9% (n = 330) exhibiting suboptimal performance in Activities of Daily Living (ADL), as assessed via the validated DAQ instrument. This functional assessment was included to characterize participants’ level of independence and to explore whether functional limitations were associated with depression rather than to establish diagnoses of frailty or dementia (refer to Table 1 for details).
Sociodemographic and clinical characteristics of older adults receiving CVD care (N = 918)

Table 1. Long description
From the top row downward, the table has four columns: Variables, Category, Frequency (f), and Percentage (%). For Age, 537 are 70 years or older (58.5 percent), 381 are 60 to 69 years (41.5 percent). For Sex, 324 are male (35.3 percent), 594 are female (64.7 percent). Religious affiliation shows 619 are Christian (67.4 percent), 299 are other religions (32.6 percent). Education level: 543 have tertiary education (59.1 percent), 375 have non-formal, primary, or secondary education (40.9 percent). Living arrangement: 656 live with family (71.4 percent), 262 live alone or are institutionalized (28.6 percent). Place of residence: 497 are in urban areas (54.1 percent), 421 in rural locations (45.9 percent). Smoking status: 211 are smokers (23.0 percent), 707 are non-smokers (77.0 percent). Alcohol intake: 682 present (74.3 percent), 236 absent (25.7 percent). Duration of diagnosis: 607 have five years or more (66.1 percent), 311 have five years or less (33.9 percent). Comorbidity: 597 present (65.0 percent), 321 absent (35.0 percent). Medication dependence: 702 yes (76.5 percent), 216 no (23.5 percent). Activities of daily living: 588 optimal (64.1 percent), 330 suboptimal (35.9 percent). Depression: 823 present (89.7 percent), 95 absent (10.3 percent).
Keys: n = sample size, () = bracket sign, ≥ = greater than sign, ≤ = less than sign, f = frequency, % = percentage, CVD = cardiovascular disease.
Prevalence of depression
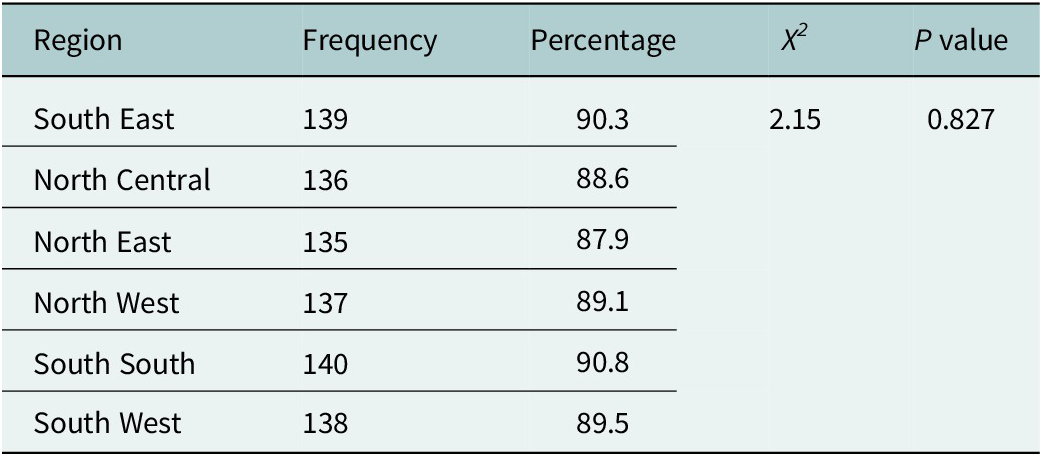
Findings revealed a high prevalence of depression among the study population. Based on the Geriatric Depression Scale–Short Form (GDS-15), 89.7% of participants (n = 823) exhibited symptoms indicative of depression, suggesting a significant mental health burden among older adults with cardiovascular conditions in Nigeria. These findings represent the prevalence of depressive symptoms identified through a screening instrument rather than clinically confirmed diagnoses of depression. To address potential regional variation, depressive symptom prevalence was examined by geopolitical zone. The proportion of participants with depressive symptoms was: South East 90.3%, North Central 88.6%, North East 87.9%, North West 89.1%, South South 90.8% and South West 89.5%. Chi-square analysis indicated no statistically significant differences in depressive symptom frequencies across regions (χ 2 = 2.15, p = 0.827), suggesting that the high burden of depression was consistently distributed nationwide (Table 2 extended).
Extension: Prevalence of depression by region

Table 2. Long description
From top to bottom, the table lists regions as South East, North Central, North East, North West, South South, and South West. For South East, frequency is 139 and percentage is 90.3. North Central has 136 and 88.6. North East has 135 and 87.9. North West has 137 and 89.1. South South has 140 and 90.8. South West has 138 and 89.5. The chi-square value for all regions is 2.15 and the P value is 0.827. The percentages of depression prevalence are closely clustered across all regions.
Keys: X 2 = Chi-square.
Bivariate associations with depression
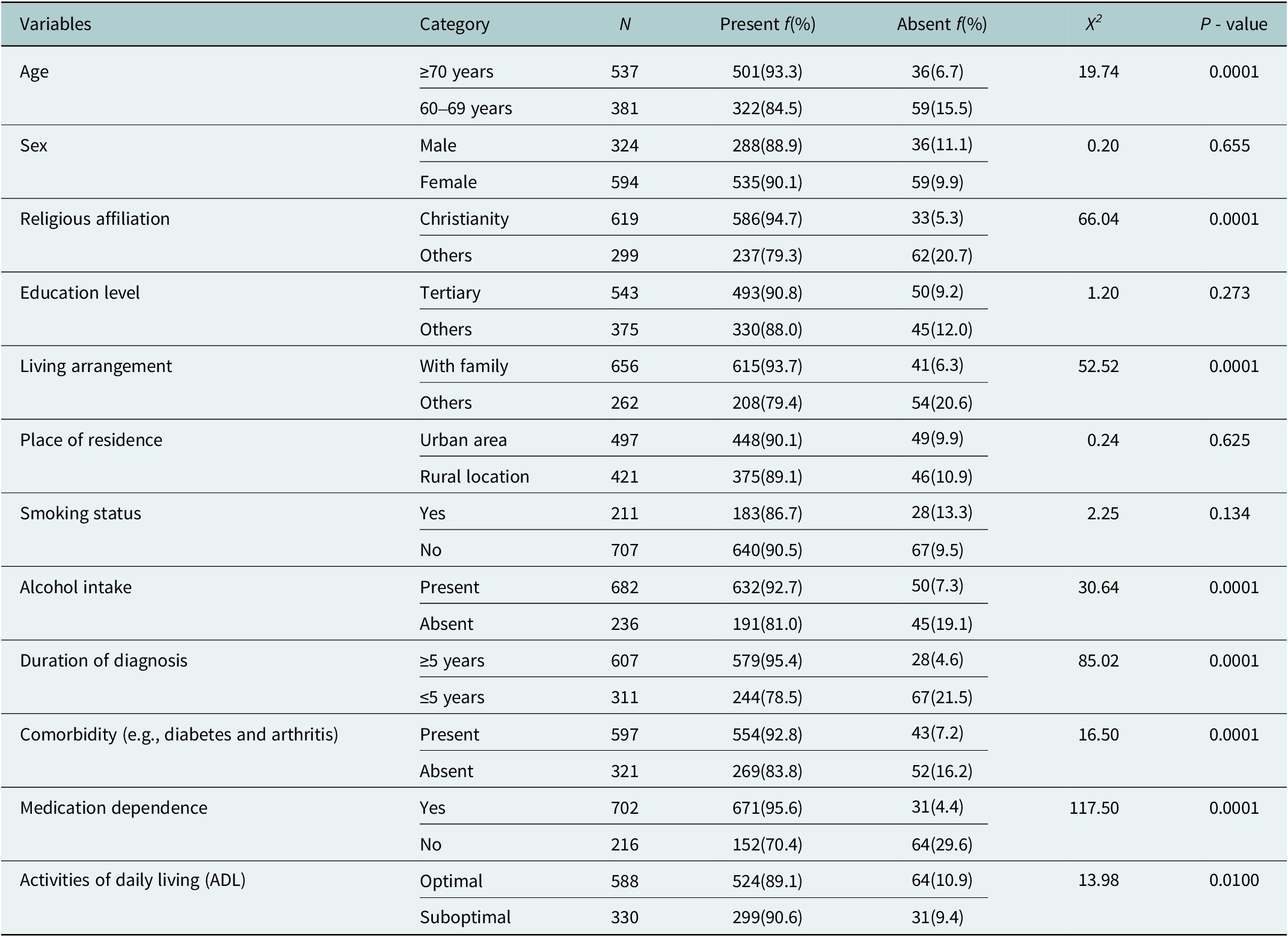
Chi-square analyses were conducted to explore associations between depression and various sociodemographic, lifestyle and clinical variables. Several variables showed statistically significant associations with depression. Older age was significantly associated with greater depression. Among participants aged 70 years and above, 93.3% reported depression, compared to 84.5% among those aged 60–69 years (χ 2 = 19.74, p = 0.0001). Religious affiliation was also strongly associated with depression, with Christians showing a significantly higher prevalence (94.7%) compared to participants adhering to other faiths, including Islam, traditional African religions or pagan beliefs (79.3%) (χ 2 = 66.04, p = 0.0001). Living arrangement emerged as a significant factor. Those living with family had a lower prevalence of depression (93.7%) than individuals who lived alone or were institutionalized (79.4%) (χ 2 = 52.52, p = 0.0001). Alcohol consumption was significantly associated with depression, with 92.7% of current alcohol users experiencing depression, compared to 81.0% among non-users (χ 2 = 30.64, p = 0.0001). The duration of cardiovascular diagnosis was also significant; 95.4% of those diagnosed for 5 years or more were depressed, versus 78.5% of those diagnosed for <5 years (χ 2 = 85.02, p = 0.0001). The presence of comorbidities was associated with a higher rate of depression (92.8%) compared to those without comorbid conditions (83.8%) (χ 2 = 16.50, p = 0.0001). Similarly, medication dependence showed a strong association, with 95.6% of those reliant on medication reporting depression versus 70.4% among those who were not (χ 2 = 117.50, p = 0.0001). Conversely, no significant associations were found between depression and sex (χ 2 = 0.20, p = 0.655), education level (χ 2 = 1.20, p = 0.273), place of residence (χ 2 = 0.24, p = 0.625) or smoking status (χ 2 = 2.25, p = 0.134). Functional status (ADL) showed borderline statistical significance (χ 2 = 13.98, p = 0.0100), suggesting a weak association. This finding indicates that while functional limitations were examined as a potential correlate of depression, functional impairment was not the primary outcome of the study (refer to Table 3 for details).
Bivariate associations between depression and sociodemographic, lifestyle and clinical variables (N = 918)

Table 3. Long description
From top to bottom, the table lists variables in the first column, each split into categories in the second column. For age, participants aged 70 years or older (n equals 537) had 93.3 percent without depression and 6.7 percent with depression, while those aged 60 to 69 years (n equals 381) had 84.5 percent without and 15.5 percent with depression. The chi-squared value is 19.74, p-value 0.0001. For sex, males (n equals 324) had 88.9 percent without and 11.1 percent with depression, females (n equals 594) had 90.1 percent without and 9.9 percent with depression, chi-squared 0.20, p-value 0.655. Religious affiliation: Christianity (n equals 619) had 94.7 percent without and 5.3 percent with depression, others (n equals 299) had 79.3 percent without and 20.7 percent with depression, chi-squared 66.04, p-value 0.0001. Education level: tertiary (n equals 543) had 90.8 percent without and 9.2 percent with depression, others (n equals 375) had 88.0 percent without and 12.0 percent with depression, chi-squared 1.20, p-value 0.273. Living arrangement: with family (n equals 656) had 93.7 percent without and 6.3 percent with depression, others (n equals 262) had 79.4 percent without and 20.6 percent with depression, chi-squared 52.52, p-value 0.0001. Place of residence: urban (n equals 497) had 90.1 percent without and 9.9 percent with depression, rural (n equals 421) had 89.1 percent without and 10.9 percent with depression, chi-squared 0.24, p-value 0.625. Smoking status: yes (n equals 211) had 86.7 percent without and 13.3 percent with depression, no (n equals 707) had 90.5 percent without and 9.5 percent with depression, chi-squared 2.25, p-value 0.134. Alcohol intake: present (n equals 682) had 92.7 percent without and 7.3 percent with depression, absent (n equals 236) had 81.0 percent without and 19.1 percent with depression, chi-squared 30.64, p-value 0.0001. Duration of diagnosis: 5 years or more (n equals 607) had 95.4 percent without and 4.6 percent with depression, 5 years or less (n equals 311) had 78.5 percent without and 21.5 percent with depression, chi-squared 85.02, p-value 0.0001. Comorbidity: present (n equals 597) had 92.8 percent without and 7.2 percent with depression, absent (n equals 321) had 83.8 percent without and 16.2 percent with depression, chi-squared 16.50, p-value 0.0001. Medication dependence: yes (n equals 702) had 95.6 percent without and 4.4 percent with depression, no (n equals 216) had 70.4 percent without and 29.6 percent with depression, chi-squared 117.50, p-value 0.0001. Activities of daily living: optimal (n equals 588) had 89.1 percent without and 10.9 percent with depression, suboptimal (n equals 330) had 90.6 percent without and 9.4 percent with depression, chi-squared 13.98, p-value 0.0100. Statistically significant associations (p-value less than 0.05) are observed for age, religious affiliation, living arrangement, alcohol intake, duration of diagnosis, comorbidity, medication dependence, and activities of daily living.
Keys: ≥ = greater than sign, ≤ = less than sign, () = bracket sign, n = sample size, p = probability. Educational level: Others (non-formal, primary, secondary), living arrangement: Others (alone, institutionalized), religious affiliation: others (Pagan, African Traditional Religion, Islam).
Multivariate logistic regression analysis
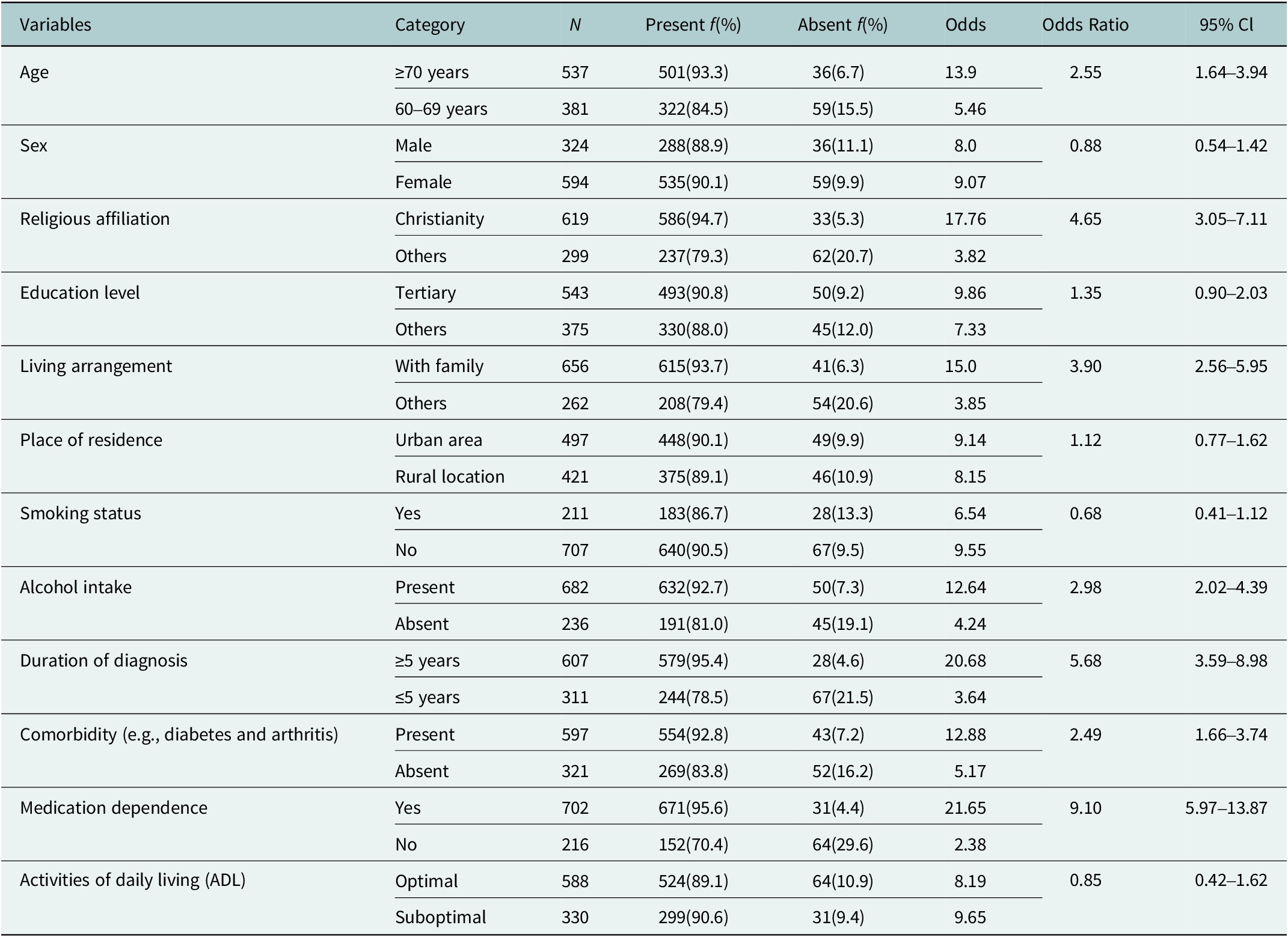
To examine independent factors associated with depression, a multivariate logistic regression model was developed using variables that showed significant associations in the bivariate analysis. The model identified several variables that were independently associated with depressive symptoms. Participants aged 70 years and above had significantly higher odds of experiencing depression compared to those aged 60–69 years (adjusted odds ratio [AOR] = 2.55; 95% confidence interval [CI]: 1.64–3.94; p < 0.001). Christian participants had significantly higher odds of depression compared to those of other religious affiliations (AOR = 4.65; 95% CI: 3.05–7.11; p < 0.001); this finding reflects a statistical association and should not be interpreted as causal. Living with family was associated with significantly higher odds of depression (AOR = 3.90; 95% CI: 2.56–5.95; p < 0.001), indicating that it functioned as a risk factor rather than a protective factor in this study population. Alcohol use was associated with nearly three times higher odds of depression (AOR = 2.98; 95% CI: 2.02–4.39; p < 0.001). A longer duration of cardiovascular illness (≥5 years) was significantly associated with higher odds of depression (AOR = 5.68; 95% CI: 3.59–8.98; p < 0.001), as was the presence of comorbidities (AOR = 2.49; 95% CI: 1.66–3.74; p < 0.001). The most prominent factor associated with depression was medication dependence, which was associated with over nine times higher odds of depression (AOR = 9.10; 95% CI: 5.97–13.87; p < 0.001). Other variables, including sex (AOR = 0.88; p = 0.655), education level (AOR = 1.35; p = 0.273), residence type (AOR = 1.12; p = 0.625), smoking status (AOR = 0.68; p = 0.134) and functional status (ADL) (AOR = 0.85; p = 0.561), were not statistically significant factors associated with depression in the adjusted model (refer to Table 4 for details).
Multivariate logistic regression analysis of predictors of depression in older adults receiving CVD care (n = 918)

Table 4. Long description
The table lists variables in the first column, each with two categories in adjacent rows. For age, greater than or equal to 70 years (n 537) had 501 present cases (93.3 percent), odds 13.9, odds ratio 2.55, 95 percent confidence interval 1.64 to 3.94; 60 to 69 years (n 381) had 322 present (84.5 percent), odds 5.46. For sex, male (n 324) had 288 present (88.9 percent), odds 8.0, odds ratio 0.88, 95 percent confidence interval 0.54 to 1.42; female (n 594) had 535 present (90.1 percent), odds 9.07. Religious affiliation: Christianity (n 619) had 586 present (94.7 percent), odds 17.76, odds ratio 4.65, 95 percent confidence interval 3.05 to 7.11; others (n 299) had 237 present (79.3 percent), odds 3.82. Education level: tertiary (n 543) had 493 present (90.8 percent), odds 9.86, odds ratio 1.35, 95 percent confidence interval 0.90 to 2.03; others (n 375) had 330 present (88.0 percent), odds 7.33. Living arrangement: with family (n 656) had 615 present (93.7 percent), odds 15.0, odds ratio 3.90, 95 percent confidence interval 2.56 to 5.95; others (n 262) had 208 present (79.4 percent), odds 3.85. Place of residence: urban area (n 497) had 448 present (90.1 percent), odds 9.14, odds ratio 1.12, 95 percent confidence interval 0.77 to 1.62; rural location (n 421) had 375 present (89.1 percent), odds 8.15. Smoking status: yes (n 211) had 183 present (86.7 percent), odds 6.54, odds ratio 0.68, 95 percent confidence interval 0.41 to 1.12; no (n 707) had 640 present (90.5 percent), odds 9.55. Alcohol intake: present (n 682) had 632 present (92.7 percent), odds 12.64, odds ratio 2.98, 95 percent confidence interval 2.02 to 4.39; absent (n 236) had 191 present (81.0 percent), odds 4.24. Duration of diagnosis: greater than or equal to 5 years (n 607) had 579 present (95.4 percent), odds 20.68, odds ratio 5.68, 95 percent confidence interval 3.59 to 8.98; less than or equal to 5 years (n 311) had 244 present (78.5 percent), odds 3.64. Comorbidity: present (n 597) had 554 present (92.8 percent), odds 12.88, odds ratio 2.49, 95 percent confidence interval 1.66 to 3.74; absent (n 321) had 269 present (83.8 percent), odds 5.17. Medication dependence: yes (n 702) had 671 present (95.6 percent), odds 21.65, odds ratio 9.10, 95 percent confidence interval 5.97 to 13.87; no (n 216) had 152 present (70.4 percent), odds 2.38. Activities of daily living: optimal (n 588) had 524 present (89.1 percent), odds 8.19, odds ratio 0.85, 95 percent confidence interval 0.42 to 1.62; suboptimal (n 330) had 299 present (90.6 percent), odds 9.65. Odds ratios above 1 indicate higher odds of depression for the reference category. The highest odds ratios are for medication dependence, duration of diagnosis greater than or equal to 5 years, living with family, Christianity, and alcohol intake.
Keys: ≥ = greater than sign, ≤ = less than sign, () = bracket sign, n = sample size, Cl = confidence level. Educational level: Others (non-formal, primary, secondary), living arrangement: Others (alone, institutionalized), religious affiliation: others (Pagan, African Traditional Religion, Islam), CVD = cardiovascular disease.
Discussion
Our study uncovered a remarkably high prevalence of depression (89.7%) among older Nigerian adults receiving CVD care in geriatric outpatient clinics. This rate significantly exceeds previous estimates reported in similar sub-Saharan African populations, which typically range between 30% and 60% (Bahall, Reference Bahall2019; Igbokwe et al., Reference Igbokwe, Ejeh, Agbaje, Umoke, Iweama and Ozoemena2020; Falade et al., Reference Falade, Oyebanji, Oshatimi, Babatola, Orekoya, Eegunranti and Falade2022). This marked difference warrants careful methodological and contextual consideration. First, the use of the GDS-15 as a screening rather than diagnostic instrument may have contributed to an overestimation of prevalence, as it is designed to maximize sensitivity and may capture subclinical depressive symptoms. Second, the application of a cutoff score of ≥5, while widely used, may further increase case identification in medically ill populations, where somatic and psychological symptoms often overlap. Third, the hospital-based nature of the sample, comprising older adults actively receiving care for cardiovascular disease, likely reflects a population with higher disease burden, functional limitations and psychological vulnerability than community-dwelling older adults. Together, these factors may partially explain the substantially elevated prevalence observed in this study. This discrepancy nevertheless suggests a potentially underrecognized and under-addressed mental health burden among older adults with chronic illnesses in Nigeria. Globally, depression is a leading cause of disability among older populations and is particularly pronounced in individuals managing chronic conditions such as CVD (Huffman et al., Reference Huffman, Celano, Beach, Motiwala and Januzzi2013; Yuyun et al., Reference Yuyun, Sliwa, Kengne, Mocumbi and Bukhman2020; WHO, 2025). In Nigeria, where the prevalence of hypertension and other cardiovascular risk factors is rising rapidly (Ojo et al., Reference Ojo, Ojji, Grobbee, Huffman and Peters2024; WHO Africa, 2025), our findings emphasize the dual burden of physical and mental health demands in geriatric care.
In line with prior geriatric literature, we found that participants aged 70 and above had significantly higher odds of depression (AOR = 2.55; 95% CI: 1.64–3.94; p < 0.001), a pattern consistent with evidence that aging increases vulnerability to psychological distress due to declining physical function, isolation and cognitive decline (Zhang et al., Reference Zhang, Chen and Ma2018; Forbes et al., Reference Forbes, Lotfaliany, Mohebbi, Reynolds, Woods, Orchard, Chong, Agustini, O’Neil, Ryan and Berk2024; Komuro et al., Reference Komuro, Komuro, Kaneko, Suzuki, Okada, Fujiu, Takeda, Morita, Node, Yasunaga, Komuro, Ieda and Takeda2025). Similarly, a longer duration of cardiovascular illness (≥5 years) was a strong factor associated with depression (AOR = 5.68; 95% CI: 3.59–8.98; p < 0.001), reinforcing the role of chronic disease duration as a driver of sustained psychological burden (Ejim et al., Reference Ejim, Okafor, Emehel, Mbah, Onyia, Egwuonwu, Akabueze and Onwubere2011; Bahall, Reference Bahall2019). Medication dependence emerged as the most potent independent factor associated with depression (AOR = 9.10; 95% CI: 5.97–13.87; p < 0.001). This underscores the psychological toll of polypharmacy and complex drug regimens, especially in settings where financial strain and medication side effects are prevalent concerns (Subih et al., Reference Subih, Abu Saleh and Malak2023; Berimavandi et al., Reference Berimavandi, Abbasi, Khaledi-Paveh and Salari2025). Depression has been shown to reduce medication adherence by as much as 40% in older CVD populations (Brimavandi et al., Reference Brimavandi, Abbasi, Khaledi-Paveh and Salari2023), creating a bidirectional risk loop where poor mental health exacerbates physical illness and vice versa (Chin et al., Reference Chin, Ghosh, Subramaniam and Beishon2023).
The presence of comorbid conditions significantly increased the likelihood of depression (AOR = 2.49; 95% CI: 1.66–3.74), consistent with studies indicating that multimorbidity compounds psychological strain and functional limitations (Igbokwe et al., Reference Igbokwe, Ejeh, Agbaje, Umoke, Iweama and Ozoemena2020; Falade et al., Reference Falade, Oyebanji, Oshatimi, Babatola, Orekoya, Eegunranti and Falade2022; Alfaifi et al., Reference Alfaifi, Elmahdy, El-Setouhy and Alfaifi2024). Our findings further validate this association in the Nigerian context, where healthcare access barriers may amplify the psychological cost of managing multiple chronic illnesses. Alcohol use was associated with nearly three times higher odds of depression (AOR = 2.98; 95% CI: 2.02–4.39), aligning with extensive research linking substance use with exacerbated mental health outcomes in late life (Nakua et al., Reference Nakua, Amissah, Tawiah, Barnie, Donkor and Mock2023; Assefa et al., Reference Assefa, Ali, Mussa, Misgana, Abdi, Zewudie and Temesgen2025; Mohebbi et al., Reference Mohebbi, Davoodian, Ganjali, Beilin, Berk, Forbes, McNeil, Nelson, Ryan, Wolfe, Woods and Lotfaliany2025). Such behaviors may serve as maladaptive coping mechanisms in the face of illness-related distress and deserve attention in clinical screenings. Contrary to initial interpretation, living with family was associated with increased odds of depression (AOR = 3.90; 95% CI: 2.56–5.95), indicating a risk relationship in this cohort. This finding may reflect contextual realities such as caregiving strain, financial dependency or interpersonal stress within multigenerational households, rather than the traditionally assumed protective effect of co-residence (Chiao et al., Reference Chiao, Weng and Botticello2011; Falade et al., Reference Falade, Oyebanji, Oshatimi, Babatola, Orekoya, Eegunranti and Falade2022; Olabisi et al., Reference Olabisi, Faronbi, Adedeji, Ademuyiwa, Gambari and Lasisi2023). These results suggest that the quality of social support, rather than mere cohabitation, is critical in influencing mental health outcomes.
A notable and perhaps counterintuitive finding was that Christian affiliation was associated with increased odds of depression (AOR = 4.65; 95% CI: 3.05–7.11). Given the observational and cross-sectional nature of this study, this association should be interpreted with caution and not as evidence of a causal relationship. It is possible that unmeasured or residual confounding factors, such as socioeconomic status, health-seeking behavior, regional differences or varying levels of social support (McFarland, Reference McFarland2010), may have influenced this association. The present study was not designed to explore the underlying mechanisms driving this relationship, and therefore, no definitive explanations can be established. Rather than attributing causality, this finding highlights the need for further research, particularly longitudinal or mixed-methods studies, to better understand the contextual and psychosocial factors that may underlie this association in the Nigerian setting (Desmet et al., Reference Desmet, Dezutter, Vandenhoeck and Dillen2022).
Clinical implications
Our findings suggest several urgent and actionable recommendations: (1) Routine depression screening: Implementing standardized tools like the GDS-15 in geriatric outpatient clinics is essential for early identification. However, positive screens should ideally be followed by a clinical diagnostic assessment to reduce misclassification. (2) Medication review and simplification: Efforts to reduce polypharmacy and simplify drug regimens may alleviate the psychological toll and improve adherence. (3) Integrated social support interventions: Community-based and family-inclusive programs could provide low-cost buffers against depression in older adults. Importantly, interventions should focus on improving the quality of family support rather than assuming co-residence is protective. (4) Management of multimorbidity: Structured multimorbidity protocols can help reduce the cumulative psychological strain of coexisting chronic conditions. (5) Targeted interventions for high-risk groups: Older adults with long-standing illness, high medication burden or limited social support require priority psychosocial screening and targeted referrals.
A major strength of this study is its large, nationally representative sample drawn from 12 tertiary hospitals across Nigeria’s six geopolitical zones, enhancing generalizability. The use of validated instruments (GDS-15 and Lawton IADL), rigorous cultural and linguistic adaptation, standardized training of research assistants and a high response rate strengthen internal validity and data quality. However, several methodological factors may have contributed to the high observed prevalence, including reliance on a screening tool without diagnostic confirmation, the selected cutoff threshold and the hospital-based sampling frame, which may limit comparability with community-based studies. The cross-sectional design limits causal inference, and the hospital-based setting may underrepresent older adults not accessing tertiary care. Self-reported measures are subject to recall and social desirability bias, and depression was not confirmed by clinical diagnostic interviews.
Conclusion
This nationally representative study demonstrates an alarmingly high prevalence of depression among older Nigerians living with cardiovascular diseases, underscoring a substantial yet under-recognized mental health burden. This high prevalence should be interpreted in light of methodological considerations, including the use of a screening instrument and the clinical characteristics of the study population. Advanced age, longer duration of CVD, comorbidities, alcohol use, religious affiliation and medication dependence were identified as significant factors associated with depression, while living with family was associated with increased odds of depression rather than a protective effect. These findings highlight the strong interplay between psychosocial, lifestyle and clinical factors in late-life depression among CVD patients. Integrating routine depression screening, culturally sensitive psychosocial support and family-centered interventions into cardiovascular care is essential to improve quality of life, treatment adherence and overall outcomes for Nigeria’s rapidly aging population.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10218.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors gratefully acknowledge the management and clinical staff of the 12 participating tertiary hospitals across Nigeria for their institutional support. We sincerely thank the trained research assistants for their dedication and professionalism, and the older adults and caregivers who generously contributed their time and experiences. Their cooperation made this nationally representative study possible.
Author contribution
All the authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by U.C.U., A.N.O., C.M.J. and O.C.E. The first draft of the manuscript was written by U.C.U., and all the authors commented on previous versions of the manuscript. All the authors have read and approved the final manuscript.
Financial support
No funding was received for conducting this study.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Ethical approval for the study was obtained from the Federal Ethics Committee of Nigeria (Reference: REC/FE/2024/00061), in accordance with the tenets of the Declaration of Helsinki. Administrative approvals were also obtained from the Chief Medical Directors of all participating hospitals. Informed consent was obtained from all individual participants included in the study.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Consent for publication was obtained from all participants, and they agreed to the anonymized presentation of their data in this manuscript.

 Open access
Open access