

1. Introduction
In the design field, understanding users is positioned as a foundation for problem identification and idea generation. Approaches such as Human-Centered Design (HCD) (ISO 2010) and co-design (Reference Sanders and Jan StappersSanders and Stappers 2008) emphasize a deep understanding of users’ experiences and contexts (Reference Probst, Ratcliffe, Molteni, Mexia, Rees, Matcham and AntonelliProbst et al. 2024). User data collected through interviews, field observations, and workshops is typically synthesized using frameworks such as the empathy map (Reference Siegel and DraySiegel & Dray 2019) and AEIOU (Reference KumarKumar 2013), supporting the generation of insights in the early design stages. Most of these frameworks focus primarily on individual perspectives and behaviors. In recent years, however, it has become increasingly important to understand not only these individual aspects but also the situations in which multiple stakeholders interact and influence one another (Reference Nielsen and BjerckNielsen & Bjerck 2022). In addition, while attempts have been made to model designers’ empathy processes, it is noted that the difficulty of empathy itself poses a challenge for HCD (Reference Li and Hölttä-OttoLi & Hölttä-Otto 2023).
These limitations become particularly salient in the domain of care, an area that has gained increasing attention as a field of design practice. With the aging population and declining birthrate, the number of people requiring daily care is increasing in diverse settings, such as homes and care facilities. Challenges arising in care settings encompass not only physical burdens but also complex issues involving psychological and social aspects. Designing in care settings, such as transfer assistance, alleviating loneliness (Reference Tunc, Nijboer, Ludden, van Velsen and TabakTunc et al. 2023), supporting caregivers, or improving communication between caregivers and care recipients (Reference Probst, Ratcliffe, Molteni, Mexia, Rees, Matcham and AntonelliProbst et al. 2024). However, most have primarily targeted either the caregiver or the care recipient as the primary user, focusing on support based on individual needs. On the other hand, caregiving is inherently a relational activity involving two or more people, and actions and judgment depend on the context of interaction with the other person (Reference Lyons, Zarit, Sayer and WhitlatchLyons et al. 2002). Even with the same caregiver-care recipient pairing, the relationship can fluctuate depending on the situation and the physical and mental states of both parties. Therefore, even when both parties involved in care intend to provide “desirable care for the other,” actions and perceptions often fail to align, frequently leading to tension and friction.This complex issue within care has long been described in major nursing theories (Reference TravelbeeTravelbee 1971) as a fundamental challenge arising from human-to-human interaction. Consequently, when designing in care settings, understanding individuals alone is insufficient; research and analysis that captures the very fluctuations in the relationship itself are necessary.
In caregiving settings, a shift from person-centered care to relationship-centered care (RCC) is discussed. RCC emphasizes that all care relationships occur within a context of mutual influence (Reference Beach and InuiBeach, Inui, and Relationship-Centered Care Research Network 2006), highlighting the importance of positive, bidirectional relationships as the foundation of quality care (Reference Gurung and ChaudhuryGurung & Chaudhury 2025). In robotic research for dementia care, it has been noted that the caregiver–care recipient relationship itself can influence design outcomes (Reference Hsu, Foster, Sabanovic and ChungHsu et al. 2025). In the design field, discussions focusing on interpersonal relationships are also emerging, yet existing design research methods primarily rely on understanding individuals (Reference Probst, Ratcliffe, Molteni, Mexia, Rees, Matcham and AntonelliProbst et al. 2024). There is a growing emphasis on viewing people not as isolated users, but as part of social networks. However, a systematic framework for incorporating the dynamic nature of relationships into design challenges and realizing designs that support these relationships without diminishing their value remains underdeveloped (Reference Nielsen and BjerckNielsen & Bjerck 2022).
Psychological theories explaining interpersonal relationships and behavior include numerous frameworks, which describe the expectations people hold toward others and the impact of their fulfillment on behavior and relationships, such as Expectancy Violation Theory (Reference BurgoonBurgoon 1978) and Expectancy-State Theory (Reference Berger, Conner and Hamit FisekBerger et al. 1974). Additionally, models explaining individual behavioral choices, such as the Theory of Planned Behavior (TPB) (Reference AjzenAjzen 1985), are also widely used. However, these often focus on specific behaviors, aspects of cognition, or individuals, and have not yet fully captured the relationship between a caregiver and a care recipient.
This study aims to develop a framework employing “expectancy misalignment” to explain conflicts arising between caregivers and care recipients. Specifically, our proposal extends the TPB, a model explaining individual behavior, to visualize the factors of expectancy misalignment. The developed framework is expected to enable treating the relationship itself as the design target. This study addresses the following research questions:
RQ1: What structures and characteristics of relational expectation misalignment underlie conflicts in care settings?
RQ2: To what extent can the proposed relational expectation misalignment model adequately describe and explain actual conflict cases?
RQ3: What kinds of insights are gained when stakeholders apply the proposed model to analyze their own experiences?
As an initial validation of the model, interviews were conducted with two professional care practitioners and one family caregiver. Additionally, the First author’s own caregiving experience was analyzed as a case study. Interpretations and insights emerging during the case analysis process were also evaluated to examine how the model contributes to participants’ introspection and understanding of their situation. Based on these findings, we discuss the structure and characteristics of expectation mismatch, the explanatory power of the model, and the potential for participants to generate reinterpretations and insights.
2. Proposed framework
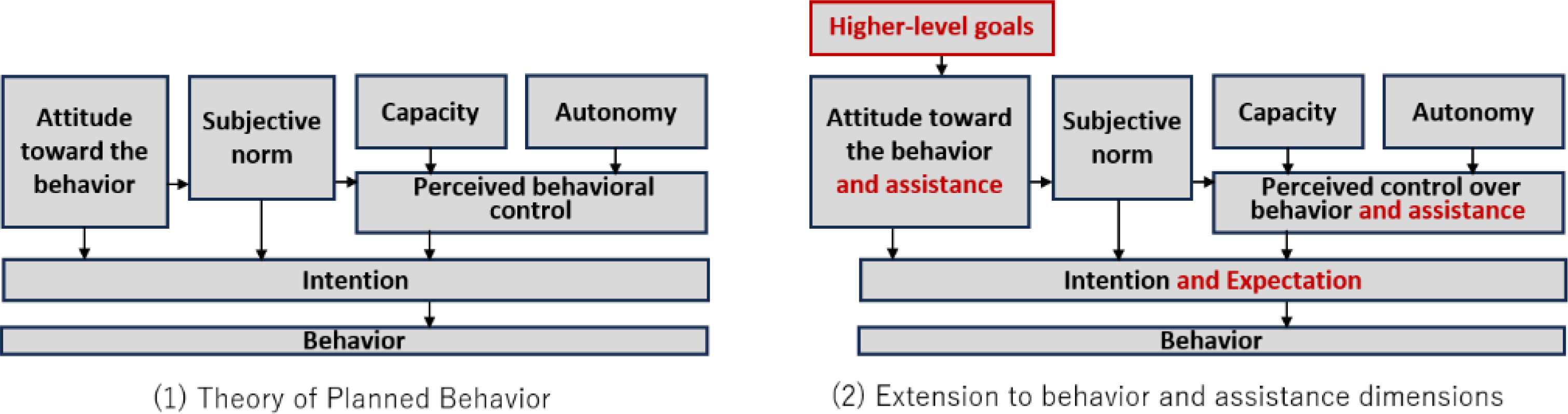
The Theory of Planned Behavior (TPB) (Reference AjzenAjzen 1985) was proposed as a theory that explains how behavioral intentions are formed when an individual performs a particular action (Figure 1-1). The framework analyzes the factors underlying human behavior through three components: attitude, subjective norms, and perceived behavioral control. Attitude refers to the extent to which an individual feels positively or negatively about performing the behavior. Subjective norms capture how the individual perceives others’ evaluations regarding the behavior, representing perceived expectations or social pressure. Perceived behavioral control reflects the degree to which the individual feels capable of performing the behavior and is shaped by both internal capacity and external constraints. These three components collectively influence the formation of behavioral intention, which subsequently leads to the actual behavior.
Traditionally, TPB has conceptualized the psychological determinants of behavioral choice as processes internal to each individual. In existing research on dyadic relationships, two TPB models have been placed side by side to compare the behavioral intentions of each person involved (Reference Howland, Farrell, Simpson, Rothman, Burns, Fillo and WlaschinHowland et al. 2016). However, caregiving interactions are inherently dyadic relationships, and behavioral intentions do not remain confined within each individual. Caregivers and care receivers form their intentions while continuously inferring each other’s expectations and motivations. Therefore, simply juxtaposing two individual TPB models is insufficient for understanding the mechanisms through which relational misalignments and frictions arise in caregiving contexts.
In this study, TPB is extended to relational contexts by modeling how the expectations that two individuals hold toward one another influence their attitudes, subjective norms, and perceived behavioral control. Expectancy Violations Theory (Reference BurgoonBurgoon 1978) and Expectation States Theory (Reference Berger, Conner and Hamit FisekBerger et al. 1974) show that people constantly form expectations about others’ behaviors and that relationships change depending on whether these expectations are fulfilled or violated. Building on these theories, this study conceptualizes not only the formation of one’s own behavioral intention, which reflects how one intends to act, but also the formation of relational intention, which reflects how one wants the other person to act.
Furthermore, in caregiving contexts, higher-level goals are understood to shape individual behaviors, extending beyond specific caregiving tasks to encompass broader purposes embedded in daily living and caregiving practices (Reference Low, Fletcher, Goodenough, Jeon, Etherton-Beer, MacAndrew and BeattieLow et al. 2015). This study explicitly incorporates such higher-level goals into the model so that differences in values and overarching aims, not merely differences in behavioral tendencies, can be recognized as background factors that contribute to expectation misalignment.(Figure 1-2)
Extension of the theory of planned behavior

Model visualizing the structure of expectation discrepancies within a caregiving dyad
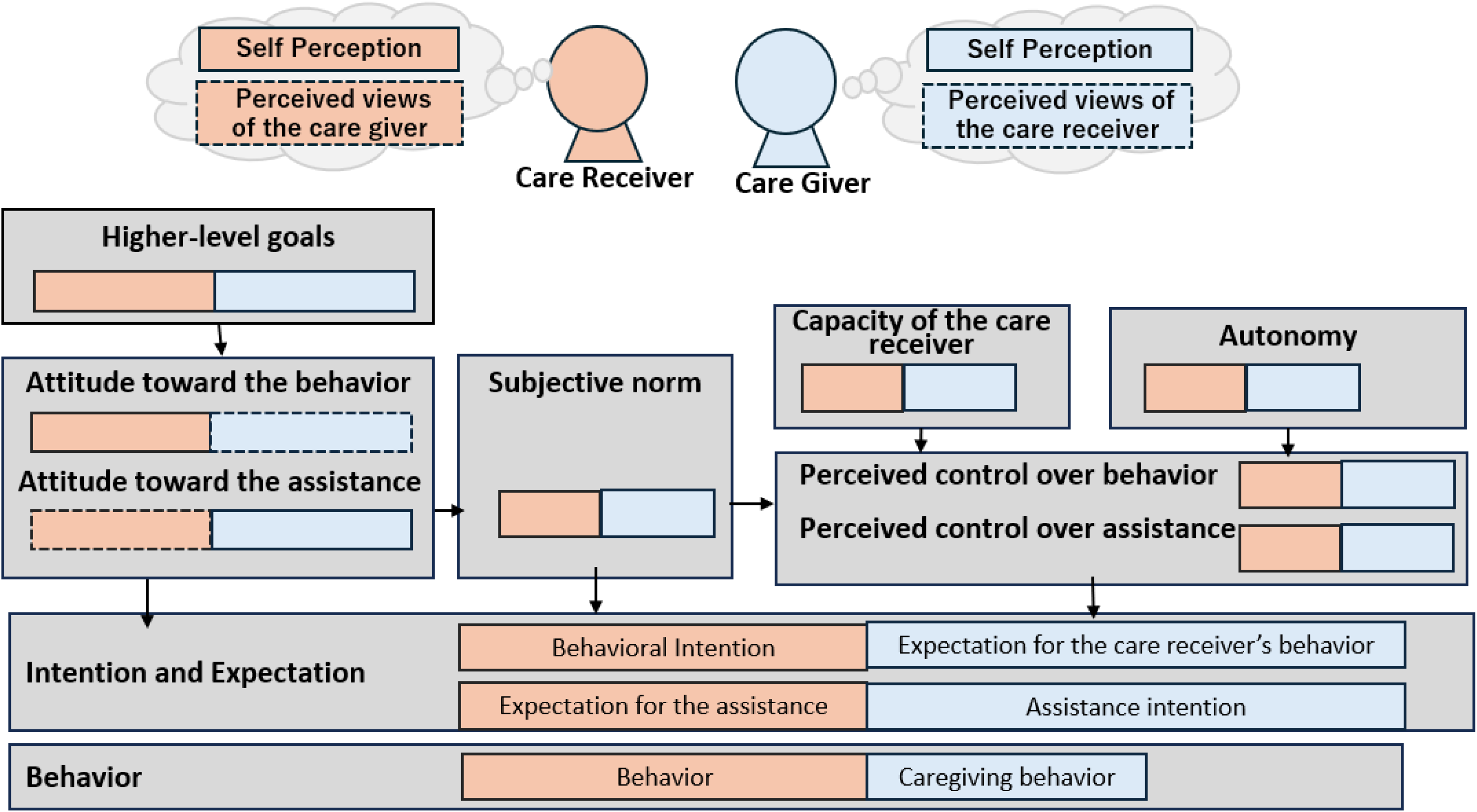
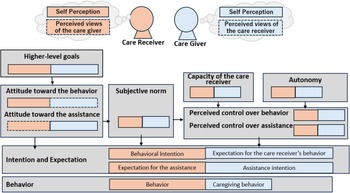
Drawing on these insights, this study develops a model that augments the traditional TPB with two additional elements, namely relational behavioral intention and higher-level goals, to visualize the structure of expectation misalignment in dyadic caregiving relationships (Figure 2). On the caregiver side, the elements leading to behavioral intention are based on how the caregiver personally feels about the target behavior or caregiving activity, including attitude, subjective norms, and perceived behavioral control. In contrast, the elements leading to the caregiver’s intention for how the care receiver should act stem from how the caregiver infers the care receiver’s feelings, evaluations, and constraints regarding the same behavior.
For the care receiver, the structure is reversed. Their behavioral intention is shaped by their own evaluation of the target behavior, while the intention they hold for the caregiver’s behavior is shaped by how they infer the caregiver’s thoughts, expectations, and constraints. By modeling this reciprocal inference process, the model makes it possible to identify mismatches between the behavior performed and the behavior desired by the other person on both sides. These mismatches constitute the expectation misalignment and can be visualized in terms of which elements diverge.
By explicitly integrating relational expectations into the framework, the model situates relational cognitions, such as expectations toward the other person and assumptions about how the other interprets the situation, within the TPB structure of attitudes, subjective norms, and perceived behavioral control. Expectation misalignment can therefore be understood by identifying where misalignments emerge across these elements. This provides a theoretical foundation for visualizing how both the caregiver and the care receiver (1) make sense of each other’s behavior, (2) interpret relational obligations and role norms, and (3) assess the abilities and constraints of themselves and the other. Through this structure, the model captures how expectation misalignment emerges and how it triggers psychological and relational responses. This provides a basis for explaining the mechanisms of caregiving relationships and offers potential directions for design interventions aimed at improving them.
3. Method
This study evaluated the applicability of the proposed model for describing caregiving situations. We conducted interviews with three individuals involved in caregiving, including professional caregivers and family caregivers in Japan. In addition, the first author applied the model to his own caregiving experience employing an autoethnographic approach.
To address RQ1, we conducted 1-hour online interviews with two professionals working in caregiving industries: an occupational therapist (expert A) and a music therapist (expert B). The interview aimed to understand the contexts where relational expectation misalignment tends to arise in caregiving settings. The interviews were in an exploratory open-ended format, asking questions, such as “Have you experienced episodes when miscommunication occurred?” and “What kinds of actions or statements did the other person display?”. Each interview was conducted by the first author, recorde,d and transcribed. The first author closely reviewed the transcripts to gain a deep understanding of their content and then analyzed them by mapping the statements to the components of the proposed model, categorizing the situations in which relational expectation misalignment emerged. The analysis was primarily conducted by the first author and finalized through discussion with the other authors. Expert A is an occupational therapist with approximately 20 years of experience who visits households to provide rehabilitation support for maintaining and improving physical function. In daily practice, expert A interacts closely with care recipients and their families while assisting with activities of daily living and adjusting rehabilitation goals. Expert B is a music therapist with 23 years of experience at nursing homes for older adults. Expert B conducts music therapy sessions three times per week, including singing and handbell ensemble programs. The therapy takes place within a group organized according to the participants’ care needs and cognitive functioning.
To address RQ2, we examined two cases of family caregivers (Cases C and D) to evaluate how the proposed model appropriately describes the actual cases. These cases were analyzed to identify specific examples of relational expectation misalignment that arise in home-based caregiving. Case C was obtained through a one-hour semi-structured interview with a family caregiver. Case D was constructed based on the first author’s experience, which follows an autoethnography approach. In each case, the first author analyzed the material by mapping the content to the components of the proposed model, after which the analysis was reviewed and refined through discussion with the other researchers. Caregiver C is a woman who cares for her father in his 80s (Case C). The care recipient, her father, now lives alone at his home but requires support in daily life after his illness and subsequent rehabilitation. Caregiver C visits the care recipient regularly, alternating with her sister, to provide household and daily living assistance. A remote monitoring camera is installed in the care recipient’s home, allowing the caregiver to check his condition from a distance. Caregiver D involved the first author, and the case is an experience with his mother (Case D). Caregiver D’s mother became ill approximately three years ago. Although she has no cognitive impairment, she lives in a wheelchair due to lower-body paralysis. While engaging in regular rehabilitation, she aims to gradually regain mobility. Caregiver D lives apart from the care recipient, and caregiving is primarily carried out by the caregiver D’s father (the care recipient’s husband).
Case D was also used to address RQ3. Since Case D draws on the first author’s own caregiving experience, this study employed autoethnography in ethnographic research (Reference Ellis, Adams and BochnerEllis, Adams, and Bochner 2010) and autobiographical design in human-computer interaction (Reference Neustaedter and SengersNeustaedter & Sengers 2012). Since caregiving is a sensitive topic to which external observers have limited access, autoethnography is well-suited for this exploratory study, enabling a deep understanding of the ways in which the proposed model affects caregiving stakeholders. The first author reflects on his experience analyzing his own case, and these reflections are presented in the results section.
4. Result
4.1. Types of conflict due to expectation discrepancy
Based on interviews with two experts (A and B), we analyzed the types of situations in which expectation misalignment tends to occur in caregiving settings and identified characteristic patterns underlying these misalignments.
Expert A pointed out that relational expectation misalignment in caregiving can be understood at two distinct levels: misalignment at the behavioral level and misalignment at the life level, which is overarching goals or guiding principles in daily life. As an example of a behavioral-level misalignment, expert A described the relationship between an older woman receiving care and her daughter as the caregiver. The care receiver was physically able to stand up from the toilet independently but required assistance with pulling her pants up and down. The care receiver valued autonomy and preferred to perform tasks “as much as possible by myself,” requesting help only where necessary. In contrast, the caregiver perceived risks of falling and felt pressured by time, leading her to intervene more actively. According to expert A, such misalignments in expectations resulted in frustration for the care receiver (“She does not let me do things the way I want”) and a sense of burden for the caregiver (“She does not listen to me”).
As an example of life level misalignment, expert A described a case involving an older woman with right hemiplegia after a stroke and her daughter. The care receiver was undergoing rehabilitation at a facility, aspiring to “return home and resume living there.” The care receiver believed that using a wheelchair would allow her to return home sooner and wanted to spend her time doing the things she enjoyed. The caregiver, however, hoped that her mother would “come home only after regaining the ability to walk” and worried that using a wheelchair at home would reduce physical activity compared to life at the rehabilitation facility. In this case, differences in the overarching goals and values of caregiving created misalignment, sometimes causing the caregiver to feel unable to accept the care receiver’s wishes or leading the care receiver to lose motivation when faced with goals the care receiver considered overly demanding.
Expert A emphasized that, in both types of misalignment, a common underlying factor was a difference in how the caregiver and care receiver perceived the environment and the care receiver’s physical and cognitive abilities. Expert A also noted that, in practice, home visiting nurses and care managers play an important role in mediating these differences, adjusting perceptions, and helping reconstruct shared expectations. “Supporting this type of perceptual coordination,” Expert A stated, “is a crucial responsibility of healthcare and care professionals in home care settings.”
In the context of music-based activities facilitated by Expert B, relational expectation misalignment also appeared frequently. For example, instructions such as “turn the page” were sometimes not understood, and requests such as “please hum” were occasionally interpreted as an invitation to sing lyrics aloud. Expert B explained that her approach was not to correct or scold but to embrace a stance of acceptance. Instances were also observed in which other participants stepped in spontaneously to offer assistance, creating mutually supportive relationships among care receivers during the activity.
Expert B identified several factors contributing to relational expectation misalignment: difficulty hearing due to reduced auditory function, strong personal preferences for “doing things my own way,” and, in some cases, past interpersonal relationships influencing current perceptions. For example, some care receivers misidentified staff members as family figures, such as a deceased mother. Furthermore, Expert B noted that relationships among care receivers could influence their relationships with caregivers. For instance, when Expert B responded carefully to a male participant who tended to assert himself strongly, a female participant displayed jealousy, saying, “You only listen to him.” This suggests that relational expectation misalignment is not limited to dyadic caregiver–care receiver interactions but may also arise within multi-person relational dynamics.
Expert B also mentioned that, based on observations of caregiving scenes outside of music activities, relational expectation misalignment frequently occurs during bathing or toileting. These activities involve bodily exposure and physical contact, and they carry safety risks such as falls, which may contribute to heightened sensitivity. Additionally, Expert B pointed out that care receivers often show respect toward medical professionals (such as nurses or physical therapists) while viewing care workers as “people who should attend to my requests,” which can contribute to misaligned expectations.
Across the expert interviews, several common tendencies emerged regarding relational expectation misalignment in caregiving settings. Expert A highlighted misalignments at both the level of individual tasks and the level of overall life goals. Expert B’s experiences further demonstrated that misalignments can arise not only between caregivers and care receivers but also among care receivers themselves. Both interviews indicated that situations involving bathing, toileting, or other activities requiring physical contact and considerations of dignity and safety are particularly prone to expectation misalignment.
4.2. Application of the framework to cases of conflicts in care
4.2.1. A case in which the care recipient engaged in an activity beyond the caregiver’s ability to support — family caregiver C
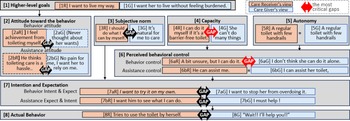
The relational expectation misalignment in this case concerns an incident in which the care receiver, an older father, used an oil heater despite being prohibited from doing so by the caregiver. A brief overview of the incident is as follows. Due to a heart condition, the father was restricted from bending forward or lifting heavy objects. Because the oil heater required refueling, its use posed cardiovascular strain and a risk of fire, leading the caregiver to prohibit its use. However, footage from a monitoring camera revealed that the father had taken out the heater and was heating food on it. The father had enjoyed preparing simmered dishes during winter and had likely resumed this familiar routine. This case represents a relational expectation misalignment arising from differing value priorities: the caregiver emphasized “safety and health above all,” whereas the care receiver prioritized “enjoyment of daily life and self-determination,” Figure 3 shows the application of the model to this case.
In the caregiver’s process of forming behavioral intention, the caregiver held a desire to respect the father’s enjoyment of heating food [1G], and therefore did not have a negative attitude toward the act of using the heater itself [2bG]. At the same time, living apart from the father led to an awareness of the difficulty of responding to sudden health changes or accidents [5G], and the caregiver felt limited in the ability to support the father remotely [6bG]. These perceptions led the caregiver to form the behavioral intention to avoid situations involving a potentially dangerous heater [7bG].
The caregiver also inferred how the care receiver perceived heater use. The caregiver assumed that the father strongly wished to use the heater [2aG] and believed, perhaps mistakenly, that he could manage it independently based on perceived rehabilitation progress [4G]. Consequently, the caregiver formed the expectation that the father should refrain from using the heater because he was overestimating his abilities [6aG]. This led the caregiver to put the heater away [8G].
In the care receiver’s intention formation process, the father enjoyed heating food with the heater [1R] and held a positive attitude toward using it [2aR]. Progress in rehabilitation had increased his confidence in his physical abilities [4R], leading him to believe that he could handle the heater independently [6aR]. As a result, he formed the intention to take out the heater and enjoy cooking on his own [7aR].
He also inferred how the caregiver viewed his heater use. Knowing that he was prohibited from using it, he assumed that the caregiver disliked his use of the heater [2bR]. At the same time, he believed that remote monitoring [5R] would make it difficult for the caregiver to help him directly [6bR]. These perceptions shaped his expectation that the caregiver should not interfere too much with what he wanted to do [7bR], resulting in his action of taking out and using the heater when alone [8R].
Through visualization using this model, it becomes clear that misalignments occurred across many elements. Among them, a particularly significant factor was the misalignment in perceived behavioral control, rooted in differing interpretations of capacity. By visualizing these structures, it is suggested that design interventions may not need to focus solely on suppressing so-called “problematic behaviors” of care receivers. Instead, the model can be interpreted as offering alternative designable elements, such as adjusting the care receiver’s perceived behavioral control, thus expanding the range of possible interventions.
Model applied to case C
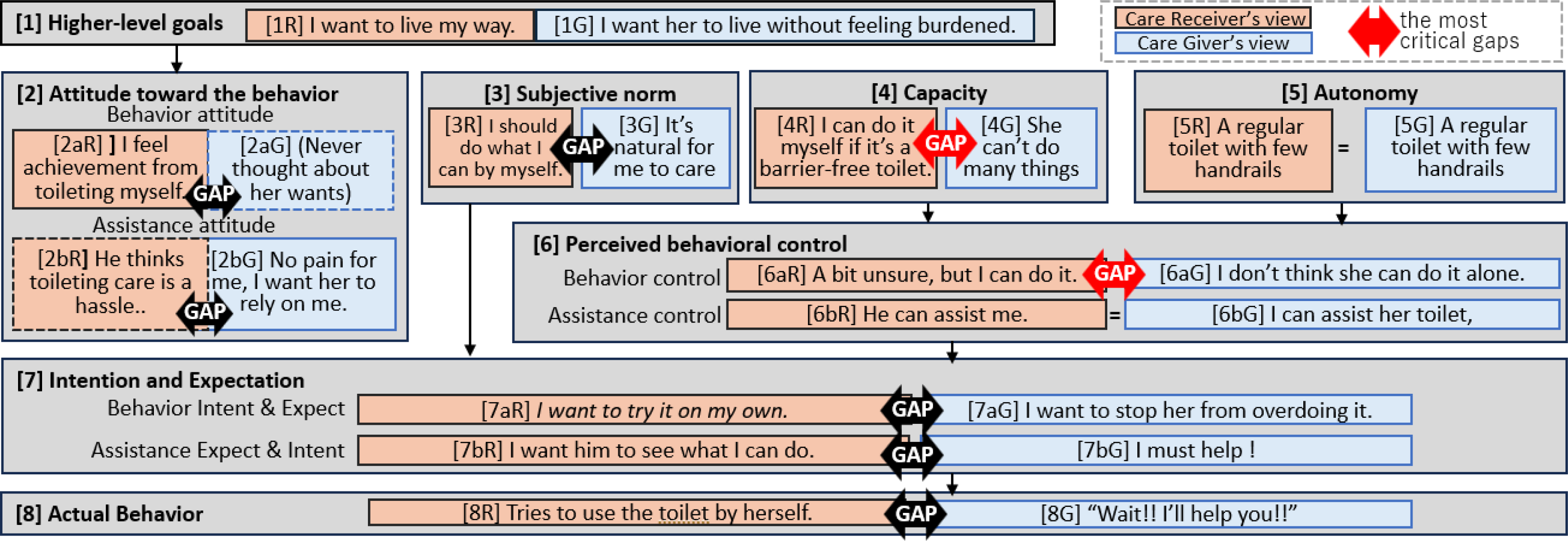
Figure 3 Long description
A diagram representing the psychological factors influencing the behavior of a caregiver and a care recipient. Panel A: Higher-level goals. Panel B: Attitude toward the behavior. Panel C: Subjective norm. Panel D: Capacity. Panel E: Autonomy. Panel F: Perceived behavioral control. Panel G: Intention and expectation. Panel H: Actual behavior. Each panel contains various labeled components that describe the attitudes, norms, capacities, and intentions of both the care receiver and the caregiver. Arrows indicate the flow and relationships between these components, highlighting the gaps in understanding and behavior between the two parties.
4.2.2. A case in which the care recipient acts without waiting for the caregiver’s assistance – family caregiver D
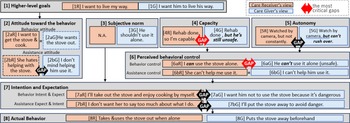
The relational expectation misalignment in this case concerns toileting assistance. While staying at a hotel, the care receiver needed to use the restroom, and the caregiver present attempted to assist. At home, the care receiver was usually able to toilet independently due to installed handrails and other supports. However, the hotel restroom lacked adequate support, making independent movement difficult. The caregiver judged that assistance was necessary for safety, whereas the care receiver wished to maintain independence and refused help. Although the care receiver eventually accepted assistance after the caregiver’s encouragement, the situation clearly demonstrated a relational expectation misalignment between a caregiver who prioritized safety and a care receiver who wanted to preserve autonomy. Figure 4 shows the application of the model.
In the caregiver’s process of forming behavioral intention, the caregiver felt no resistance or inconvenience regarding toileting assistance and was positive toward providing it [2bG]. Having previously observed the father assisting the care receiver [3G], the caregiver believed he was physically capable of offering adequate support [6bG]. These perceptions led the caregiver to form the intention to provide substantial assistance during toileting [7bG].
The caregiver also inferred how the care receiver perceived the toileting task. Considering factors such as the physical effort required for toileting, the care receiver’s lower-body paralysis [4G], and the limited supports available in the hotel restroom [5G], the caregiver judged that the care receiver would find toileting difficult [6aG]. Consequently, the caregiver formed the expectation that the care receiver should avoid overexertion and remain as comfortable as possible [7aG], which led to the verbal request “Please wait, I will help you” [8G].
In the care receiver’s intention formation process, she felt a sense of accomplishment from toileting independently and approached the task with positive feelings [2sR]. Praise from visiting care workers regarding her rehabilitation progress also contributed to her confidence, leading her to believe she could toilet independently in an accessible restroom [4R], which increased her perceived behavioral control [6aR]. However, she also felt some anxiety about the lack of support in the hotel restroom [5R]. These elements combined to form the intention to attempt toileting independently [7aR].
The care receiver also inferred how the caregiver perceived her toileting. She assumed that the caregiver might find it troublesome because he did not normally assist her [2bR], yet she also believed that the caregiver had sufficient physical ability to assist if needed [6bR]. These perceptions shaped her expectations that the caregiver should “watch and allow me to do what I can” [7bR], which led her to first attempt toileting on her own [8R].
This analysis reveals misalignments across numerous elements, including differences in how the caregiver interpreted his own attitude toward assisting and differences in the care receiver’s perceived behavioral control regarding toileting. There were also misalignments in subjective norms that neither party recognized. This suggests that the design opportunities extend beyond the physical restroom environment. Because it is unrealistic to make every restroom universally accessible, expanding the design focus beyond environmental modifications could lead to solutions that better support both caregivers and care receivers.
Finally, when the author applied the model to her own lived experience, one of the most meaningful insights was the value of distinguishing and examining elements separately. For example, what had previously been interpreted as a matter of “my mother’s personality” became, through the process of mapping elements onto the model, identifiable as an issue related to capacity within perceived behavioral control. This reframing revealed that what appeared to be a personality-based issue could instead stem from a structural misalignment arising from the author’s insufficient understanding of the care receiver’s actual abilities.
Model applied to case D

5. Discussion
5.1. Applicability of the model to the design process
This study conceptualized caregiving as a dyadic process and proposed a model that visualizes the psychological reasons underlying dyadic misalignment (Reference Lyons, Zarit, Sayer and WhitlatchLyons et al. 2002) between caregivers and care recipients. By introducing relational expectations as a lens of analysis and decomposing relational expectations into psychological components such as attitude, subjective norm, and perceived behavioral control, the model provides a structural framework that describes how misalignment arises within dyadic relationships.
Applying the model to the three interviews, as well as to the first author’s own care experience, suggested that the model can describe conflicts occurring in caregiving contexts and make visible the relational expectations misalignment between caregivers and care recipients. The results imply that the model clarifies the factors contributing to conflict in caregiving. In the context of design, the model may function as a compass for designers when exploring relational aspects of care. In the user understanding phase of HCD (Reference Li and Hölttä-OttoLi & Hölttä-Otto 2023), the model may serve as a ladder that enables designers to examine interpersonal dynamics. Traditionally, design methods have tended to focus on the individual (Reference Siegel and DraySiegel & Dray 2019), and thus, methods for incorporating the dynamic and evolving nature of relationships into design remain insufficient (Reference Nielsen and BjerckNielsen & Bjerck 2022). The proposed model may offer one approach for positioning relations as a target of design.
The proposed model may also be applicable to co-design. As seen in case D, the process of articulating the distinct viewpoints of caregivers and care recipients can itself prompt reflection for participants. Since co-design places emphasis on eliciting tacit knowledge (Reference Sanders and Jan StappersSanders & Stappers 2008), the process of completing the framework may support the articulation of tacit knowledge. However, it may be difficult for non-researcher participants to complete the framework without support. Thus, it seems necessary to design stepwise guides that allow participants to engage with each component more easily. When extending the model to co-design settings, an important issue is how to collect input from care recipients. Prior studies, such as research involving co-design with people living with dementia (Reference Hsu, Foster, Sabanovic and ChungHsu et al. 2025), may serve as useful references, but these remain subjects for future work. At the same time, collecting direct input from care recipients is often difficult. In such cases, caregivers may become the primary source of information, and the use of the model may help them deepen their understanding of the care recipient’s perspective. These considerations suggest that the process of engaging with the model may provide participants with an opportunity to reconstruct their own relationships. This insight can be applied to design processes that address participants’ inner states and relationships; for example, the model could be implemented in tools such as worksheets to serve as a “framework for reflection” for caregivers to review their own caregiving behaviors.This aligns with observations that co-design can influence relations among stakeholders (Reference Light and AkamaLight & Akama 2014), while also indicating the need for careful examination of its impact on care relationships. Such application and verification of the model as a tool represent important future research topics for applying co-design in caregiving contexts.
5.2. Limitation and future direction
This study focused on the mutual expectations of caregivers and care recipients and explored the nature of expectation misalignment and its underlying factors. However, the model presented in this study remains at the stage of applying the framework to the relationships identified through interviews, and does not yet elucidate the mechanisms that explain how expectations are formed or how misalignment develops over time and through causal processes. Although stepwise coding based on Grounded Theory and the construction of process models that describe relational change would be effective for such an analysis, the present study has not advanced to the level of detailed theorization. Future work should extend the model to a wider range of dyadic relationships, such as those between caregivers and multiple care recipients or between care recipients themselves, and systematically clarify, using methods such as Grounded Theory, what factors give rise to expectation misalignment and how such misalignment may be repaired.Additionally, it should be noted that the cases analyzed in this study are limited to the specific cultural and geographical context of caregiving in urban areas of Japan.Furthermore, evaluating the applicability of the model within design processes and extending it into a more design-friendly form are important directions for future research. Demonstrating the model in actual design projects will be necessary to assess the impact it has on designers and co-designers.
6. Conclusion
This study is an exploratory investigation that examines the complex conflicts present in caregiving contexts through the lens of relational expectations misalignment, with the aim of developing a framework that treats relationships themselves as objects of design. A key contribution is the extension of the Theory of Planned Behavior to dyadic relationships and the proposal of a relational expectations alignment that structurally visualizes the mismatch between one’s expectations of the other and one’s own behavior. Analysis of expert interviews suggested that expectation misalignment can be interpreted as comprising two layers: the “behavioral level” and the “life-level” domain. Furthermore, applying the model to two cases of family caregiving conflicts demonstrated its potential to describe and analyze the structure of actual tensions emerging in caregiving interactions. These findings suggest that the model may serve as a method for analyzing relational dynamics within HCD. In contrast to conventional HCD approaches that primarily focus on understanding individual users, this study offers a perspective that positions dyadic relationships as targets of design intervention, thereby contributing to the advancement of design methods that address relational phenomena.
Acknowledgement
The authors would like to express their sincere gratitude to all the participants who kindly cooperated in the interviews for this study.

 Open access
Open access