


Introduction
Parents of infants undergoing staged palliation for hypoplastic left heart syndrome and related single right ventricle anomalies face numerous stressors significantly worsening their well-being. Reference Mussatto, Van Rompay and Trachtenberg1 Stressors include medical challenges affecting their infant, such as the initial diagnosis, complex surgeries, intensive care stays, and ongoing uncertainty regarding their child’s survival and quality of life. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Nicholas, Nicholas, Allen and Cua2 These stressors not only pose immediate challenges but also place parents at heightened risk for mental health difficulties. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Kolaitis, Meentken and Utens3–Reference Golfenshtein, Hanlon, Deatrick and Medoff-Cooper6
In the Family Adaptation study, an ancillary study to the Paediatric Heart Network Single Ventricle Reconstruction trial, funded by the National Heart, Lung, and Blood Institute, parent well-being was significantly below expected population norms. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Ohye, Sleeper and Mahony7 Parent well-being encompasses mental health, emotional resilience, stress management, and broader aspects of life satisfaction and quality of life. Reference Mussatto, Van Rompay and Trachtenberg1,Reference McCubbin and Patterso8 The Family Adaptation study demonstrated that symptoms of anxiety and traumatic stress significantly contributed to diminished parental well-being, highlighting the need to further investigate the prevalence of severe anxiety along with the stress and coping mechanisms and access to resources that influence parents’ overall mental health outcomes. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Bainton, Trachtenberg and McCrindle5
Parental mental health challenges not only affect the parents themselves but also have cascading effects on their ability to care for their child, support the child’s recovery, and maintain family stability. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Roberts, Kazazian and Ford9–Reference McWhorter, Christofferson and Neely12 Understanding state anxiety—defined as a temporary emotional condition influenced by situational factors—may offer valuable insights into supporting the well-being of parents of infants with CHD during the early postpartum period, particularly throughout the critical phases of CHD repair and hospitalisation. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Bainton, Trachtenberg and McCrindle5,Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs13 While anxiety is often a normal and transient reaction to stress, it can become problematic when pervasive or excessive, contributing to conditions such as generalised anxiety disorder, panic disorder, post-traumatic stress disorder, and depressive disorders. Reference Saviola, Pappaianni, Monti, Grecucci, Jovicich and De Pisapia14
The primary aim of this study was to determine the prevalence of moderate-to-high parental-state anxiety at three key timepoints: following the Norwood procedure, after Stage II surgery, and at a final study visit when the child was approximately 14 months of age. Secondary aims included the identification of differences in state anxiety between mothers and fathers, comparison to norms, and the identification of predictors of elevated parental state anxiety. We hypothesised that greater stress exposure (e.g., parenting a child with a serious illness and family life stress) would be associated with higher parental anxiety. In contrast, psychosocial factors such as adaptive coping strategies (e.g., problem-focused coping, absence of maladaptive coping), social support, and financial security were expected to be associated with lower anxiety. Increased satisfaction with quality of life was hypothesised to be protective against elevated anxiety. Greater understanding of parental anxiety and its associated factors by healthcare providers can ultimately improve long-term mental health outcomes for parents and potentially overall outcomes for the child and family unit.
Materials and methods
Design of the study
The Family Adaptation study was an ancillary study to the Pediatric Heart Network Single Ventricle Reconstruction trial, which enrolled 555 infants to receive either a Blalock-Taussig-Thomas or a right ventricle to pulmonary artery shunt during their Norwood procedure. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Ohye, Sleeper and Mahony7 Eleven sites participated in the Family Adaptation study, which was approved by the Institutional Review Board at each site, with all parents providing written informed consent. The Family Adaptation study focused on parents’ perceptions of family function, quality of life, and well-being after their infant underwent the Norwood procedure. Reference Mussatto, Van Rompay and Trachtenberg1 Parents completed 13 self-reported questionnaires at three timepoints: post-Norwood, post-Stage II, and at a final visit when their child was a median age of 14 months. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Ohye, Sleeper and Mahony7
Participants
Parents who were fluent in English were eligible to participate. Both mothers and fathers were invited to complete individual surveys. Each parent had the opportunity to provide their responses separately. In some families, both parents completed the survey, while in others, only one parent (either the mother or the father) participated. Parents could begin participation at any survey timepoint, and missing a survey did not affect eligibility for subsequent surveys. Parents whose infants died or required heart transplantation were not approached for study participation or were automatically withdrawn if previously enrolled. Data collected prior to the infant’s death or heart transplantation were included in the analysis.
Measures
Survey measures were organised into booklets, and each participant was invited to complete one booklet per timepoint. All surveys are described in detail, including access instructions, in Supplementary Table 1. Demographic information including age, sex, race, and ethnicity was collected for all participants.
State-trait anxiety index
The state-trait anxiety index measures symptoms of anxiety and consists of two subscales: (1) STAI-S: state anxiety—temporary feelings of anxiety influenced by specific situations; and (2) STAI-T: trait anxiety—a stable disposition towards anxiety. Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs13 The study analysed STAI-S scores and examined how stress factors, psychosocial factors, and quality of life influence STAI-S to better understand parents’ situational anxiety throughout the illness journey. STAI-S scores range from 20 to 80, with higher scores indicating greater state anxiety (none/mild: 20–37; moderate: 38–44; severe: 45–80).
Inventory of life changes
The inventory of life changes measures cumulative stress resulting from 43 major life events such as divorce, death, or a job change. Reference Holmes and Rahe15 Higher scores reflect greater life changes associated with stress, with scores ≥300 indicating a significantly elevated risk of poor health outcomes as a result of stress-induced physical and mental illness. Reference Holmes and Rahe15
Paediatric inventory for parents
The paediatric inventory for parents measures the stress experienced by parents in the context of parenting a child with severe illness. Reference Streisand, Braniecki, Tercyak and Kazak16 The instrument evaluates both the frequency and perceived difficulty of stressors across four domains: (1) communication: e.g., “speaking with doctor”; (2) emotional distress: e.g., “feeling scared that my child could get very sick or die”; (3) medical care: e.g., “making decisions about medical care or medicines”; and (4) role function: e.g., “trying to attend to the needs of other family members.” Reference Streisand, Braniecki, Tercyak and Kazak16 Higher frequency subscale scores indicate that stressors related to parenting a child with severe illness occur more often, while higher difficulty subscale scores reflect a greater perceived intensity of these stressors.
Impact on family
The impact on family measures the overall stress experienced by the family as a result of managing a child’s chronic illness within the social and family system. Reference Stein and Riessman17 Example item includes “Our family gives up things because of my child’s illness.” Reference Stein and Riessman17
Coping health inventory for parents
The coping health inventory for parents measures what parents find helpful to the management of family life when a member of the family is ill, and it has three subscales: (1) family integration, cooperation, and definition of the situation, e.g., “believing that my child will get better”; (2) maintaining social support, self-esteem, and psychological stability, e.g., “getting away by myself”; and (3) understanding the health care situation through communication and consultation, e.g., “talking with the medical staff.” Reference McCubbin, McCubbin, Nevin, Cauble, McCubbin, Thompson and McCubbin18 Higher scores on the coping health inventory for parents indicate parents perceive the elements within each subscale as more helpful. Reference McCubbin, McCubbin, Nevin, Cauble, McCubbin, Thompson and McCubbin18
Inventory of parent’s experiences
The inventory of parent’s experiences measures parent satisfaction with social support networks, family, and their parenting role. Reference Crnic19 There are four subscales as follows: (1) Parental role satisfaction: e.g., “Your amount of household responsibility”; (2) Community satisfaction: e.g., “Your involvement in your neighborhood”; (3) Friendship satisfaction: e.g., “The availability of someone to share honestly with you when you are upset or angry”; (4) Family satisfaction: e.g., “The amount of help family members provide.” Reference Crnic19 Higher scores on the inventory of parent’s experiences indicate parents feel greater satisfaction with the social support domains. Reference Crnic19
Family hardiness index
The family hardiness index measures a family’s ability to withstand and adapt to stressful situations, maintain cohesion, and remain resilient. Reference McCubbin, McCubbin, Thompson, McCubbin, Thompson and McCubbin20 There are three subscales as follows: (1) commitment: e.g., “We work together to solve problems”; (2) Challenge: e.g., “We seem to encourage each other to try new things and experiences”; and (3) Control: e.g., “we realize our lives are controlled by accidents and luck”—reverse scored. Reference McCubbin, McCubbin, Thompson, McCubbin, Thompson and McCubbin20 Higher scores on the family hardiness index indicate that a parent perceives stronger levels of commitment, challenge, and control in the context of managing family life. Reference McCubbin, McCubbin, Thompson, McCubbin, Thompson and McCubbin20
Family inventory of resources for management
The family inventory of resources for management assesses parents’ resources for stress management and includes four subscales: (1) esteem and communication: e.g., “In our family we understand what help we can expect from each other”; (2) mastery and health: e.g., “It is hard to get family members to cooperate with each other”; (3) extended family social support: e.g., “Our relatives are willing to listen to our problems”; and (4) financial well-being: e.g., “We seem to have little or no trouble paying our bills on time.” Reference McCubbin, Comeau, Harkins, McCubbin, Thompson and McCubbin21 Higher scores on the family inventory of resources for management indicate that parents perceive their family as having the skills and resources to effectively manage stress. Reference McCubbin, Comeau, Harkins, McCubbin, Thompson and McCubbin21
Perceived quality of life
The perceived quality of life measures an individual’s degree of satisfaction with their physical, social, and cognitive health and their happiness. Reference Patrick, Kinne, Engelberg and Pearlman22 The measure includes four subscales: (1) physical health, e.g., “The amount of walking you do”; (2) social health, e.g., “How respected you are by others”; (3) cognitive health, e.g., “How well you think and remember”; and (4) happiness: e.g., “How happy you are.” Reference Patrick, Kinne, Engelberg and Pearlman22
Statistical analysis
All analyses were conducted using Microsoft Excel (Microsoft Corporation, Redmond, WA), with p-values < 0.05 considered statistically significant. Continuous variables are presented as means ± standard deviations or medians (IQR), while categorical variables are expressed as frequencies (counts) and percentages. Variables were assessed visually for normality using histograms and skew. Mean ± standard deviations were reported for normally distributed data, while median (IQR) was used for skewed data.
To analyse differences between mothers and fathers, two-tailed independent t-tests were conducted on subdomain stress, psychosocial, and quality of life measures by timepoint. To assess differences in STAI-S between parents in the same family, one-tailed paired t-tests were used, and linear regression was used to test for a relationship between partners’ scores. Finally, two-tailed z-tests were used to compare mean STAI-S, stress, psychosocial, and quality of life measures scores to published normative or comparator data, separately for mothers and fathers, by timepoint.
Bivariate linear regression models were used to evaluate the relationships between parent STAI-S scores (dependent variable) and stress, psychosocial, and quality of life subscale scores (independent variables). Analysis was performed by timepoint, separately for mothers and fathers. Missing data was handled using a complete-case analysis approach, with the proportion of missing data assessed and found to be low. The overall sample size remained sufficient to ensure statistical reliability. The coefficient of determination (R 2) was calculated for each bivariate linear model to quantify the proportion of variance in the STAI-S outcome variable explained by the independent stress, psychosocial, or quality of life variables. R 2 range interpretation was 0.00 ≤ 0.10: very weak relationship; 0.10 ≤ 0.30: weak relationship; and 0.30 ≤ 0.50: moderate relationship.
Results
Participant demographic information
Participants included 215 parents (143 mothers and 72 fathers) representing 146 infants. Approximately seventy per cent of CHD was diagnosed prenatally, and most of the pregnancies were planned (Table 1). Maternal median age was 28.7 years (IQR: 24.4–32.4), and paternal median age was 29.7 years (IQR: 26.4–34.6) at the time of their infant’s birth. The median birth order was 2 (IQR: 1–2), and parents reported knowing their spouse or partner for a median of 7 years (IQR: 4–11).
Demographic variables for mothers, fathers, and infants in the Family Adaptation study. Values are presented as n/N (%). N represents the total number of participants available for each group (mothers, fathers, or infants) at each timepoint. n indicates the number of observed cases for the specific variable. Survey completion 1–7 days prior to discharge. Long LOS in the Norwood group skews post-Norwood age at survey

The majority of infants, 90.4%, had hypoplastic left heart syndrome, and 9.6% had other single right ventricle malformations. Infants underwent the Norwood procedure at a median age of 6 days (IQR: 5–8) with 56.1% receiving a right ventricle to pulmonary artery conduit and 43.9% receiving a Blalock-Taussig-Thomas shunt as part of their Norwood operation. Four infants (2.7%) underwent heart transplant during the study (median age: 203 days; IQR: 193–301), with two following the Norwood and two after the Stage II procedure. Eleven infants (7.5%) died (median age: 97 days; IQR: 82–134), including one who had received a heart transplant. Of these deaths, ten occurred after the Norwood procedure and one occurred after the Stage II procedure.
Parents completed the post-Norwood visit when infants were at a median age of 24 days (IQR: 16–42). Post-Stage II surveys were completed when infants had a median age of 157 days (IQR: 124–201), and the final visit surveys were completed when the child was a median age of 432 days (IQR: 411–508). Data from 69 families (47%) represented both mother’s and father’s perspectives for at least one timepoint, as both parents completed surveys. Data from 74 families (51%) represented the mothers’ perspective only, while data from 3 families (2%) represented the fathers’ perspective only.
Parental STAI-S scores and severity categories
Mothers’ mean state anxiety scores were significantly elevated at all timepoints: 47.7 ± 13.2 post-Norwood, 45.9 ± 12.1 post-Stage II, and 42.1 ± 13.0 at the final study visit (North American Female Norm: 37.6 ± 11.8; p < 0.05 for all timepoints; Table 2). Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs13 Fathers’ mean state anxiety scores were significantly elevated post-Norwood and post-Stage II (43.5 ± 11.8 and 42.3 ± 13.0, respectively) compared to the North American male norm (36.9 ± 9.1; p < 0.05 for both), but not at the final visit (39.0 ± 9.6; p = 0.22; Table 2). Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs13 Mothers’ average state anxiety scores were significantly higher than fathers’ scores post-Norwood (p = 0.03), but not post-Stage II (p = 0.08) or at the final visit (p = 0.14) (Table 2).
Subscale scores as means ± sd. Higher values for stress variables indicate greater sources of stress. Higher values for psychosocial variables indicate greater satisfaction with or perceived benefit of a coping mechanism or more protective factors. Higher values for quality of life indicate greater satisfaction within the subscale domain. No comparison for ILC, IoF, PQoL. No gender norms for PIP, IPE, and FIRM. 1 values in bold indicate a significant difference (p < 0.05) from the comparison group score; an * indicates a significant difference (p < 0.05) between mothers versus fathers

Bold values indicate significantly different from the comparison group.
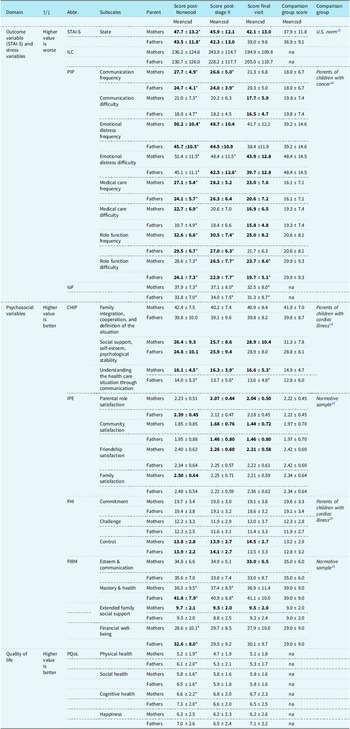
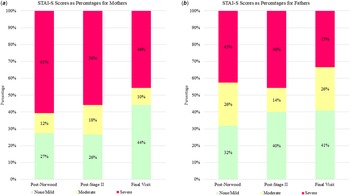
Post-Norwood, a substantial proportion of parents fell into a high-risk category of anxiety, with 61% of mothers and 43% of fathers reporting severe symptoms (Figure 1 (a) and (b)). At the time of the final visit, 46% of mothers and 33% of fathers reported severe symptoms of anxiety (Figure 1 (a) and (b)). Of the 68 mothers who completed more than one STAI-S assessment, close to half (43%) continued to report scores in the severe range across timepoints, indicating a pattern of persistent severe anxiety. For mothers with fluctuating patterns, 19% of mothers showed improvement (i.e., non-severe scores upon repeat assessment), and 12% experienced worsening symptoms (i.e., non-severe scores elevated to severe upon repeat assessment). A subset of mothers, 26%, had scores consistently in the range of no clinical concern. Of the 29 fathers who had completed more than one STAI-S measure, 21% reported scores in the severe range across all timepoints. For fathers with fluctuating patterns of response, 28% of fathers showed improvement (i.e., a non-severe score upon repeat measure), and 14% experienced worsening anxiety over time (i.e., non-severe scores elevated to severe upon reassessment). A subset of fathers, 38%, had scores consistently in the range of no clinical concern.
( a ) The bar graph illustrates the percentage of mothers with none/mild, moderate, and severe symptoms of anxiety at three timepoints. A majority, 61%, of mothers reported severe symptoms of anxiety post-Norwood (infant median age: 24 days; IQR: 16–42). The proportion of mothers with severe symptoms lessens over time, with severe symptoms reported by 56% of mothers post-Stage II (infant median age 157 days; IQR: 124–201) and 46% of mothers at the final visit (child median age 432 days; IQR 411–508). ( b ) The bar graph illustrates the percentage of fathers with none/mild, moderate, and severe symptoms of anxiety at three timepoints. Severe symptoms were reported in 43% of fathers post-Norwood, 46% of fathers post-Stage II and 33% of fathers by the final visit.

STAI-S scores in couples
Paired STAI-S data was available for 66 couples for at least one timepoint (39 couples completed surveys once, 17 twice, and 10 three times). Post-Norwood, married/coupled mothers” mean state anxiety scores were significantly higher than their spouse/partner, 47.3 ± 14.7 versus 43.3 ± 12.2, respectively (p < 0.05), but not post-Stage II or at the final visit.
A weak but statistically significant association was observed between partners’ STAI-S scores, indicating that one partner’s anxiety level was modestly related to the others. This association was evident post-Norwood (R 2 = 0.19, β = 0.52, SE = 0.16, p < 0.01) and post-Stage II (R 2 = 0.22, β = 0.50, SE = 0.17, p < 0.01), but not at the final visit (R 2 = 0.06, β = 0.33, SE = 0.27, p = 0.23).
Inventory of life changes findings
Parents reported sources of stress pertaining to their day-to-day lives, in addition to significant stress related to infants’ illness. Mother’s average inventory of life changes scores did not differ significantly from fathers at any timepoint (Table 2). Approximately 34% (48 of 143) of mothers and 36% (26 of 72) of fathers reported life changes scores greater than or equal to 300, which is a cut-off for increased risk of stress-related physical or mental health illness in the future. Reference Holmes and Rahe15 Only mother’s inventory of life changes scores were very weakly associated with STAI-S post-Norwood (R 2 = 0.08; Table 3), but not at later timepoints, and father’s inventory of life changes scores were never associated with their STAI-S scores.
Bivariate regression modelling between STAI-S (dependent variable) and stress or psychosocial or quality of life variables (independent variables). R 2 range interpretation (0.00 < 0.10: very weak relationship; 0.10 < 0.30: weak relationship; 0.30 < 0.50: moderate (mod.) relationship). Stress variables are ILC, PIP, and IoF. Psychosocial variables are CHIP, IPE, FHI, FIRM. The quality of life measure is PQoL. NS, not significant

Paediatric inventory for parents findings
Post-Norwood, mothers reported significantly higher (worse) communication, emotional distress, medical care, and role function frequency and difficulty subdomain scores compared to fathers (Table 2). Mother’s role function difficulty scores were consistently higher (worse) than fathers across all timepoints. Compared to parents of children with cancer, communication, emotional distress, medical care, and role function frequency subdomain scores were significantly higher, indicating that stressful events pertaining to parenting a child with a serious illness were occurring more frequently for CHD parents (Table 2). Reference Streisand, Braniecki, Tercyak and Kazak16
Mothers’ communication, emotional distress, medical care, and role function frequency and difficulty subscale scores were significantly associated with STAI-S at all timepoints, the highest association observed for emotional distress frequency and difficulty post-Norwood (R 2 = 0.49; Table 3). In comparison, paediatric inventory for parents subdomain scores were less consistently associated with father’s STAI-S scores, with the highest association observed post-Stage II in the subdomain emotional distress difficulty (R 2 = 0.40; Table 3).
Impact on family findings
Mothers’ impact on family scores was significantly higher (worse) than fathers’ scores at all timepoints (Table 2). Impact on family was consistently associated with mothers’ STAI-S scores, with the highest association post-Norwood (R 2 = 0.27; Table 3), while fathers’ impact on family scores was significantly associated with STAI-S only post-Norwood and post-Stage II, with the highest association post-Norwood (R 2 = 0.17; Table 3).
Coping health inventory for parents findings
No difference was observed between mothers’ scores versus fathers’ scores for family integration, cooperation, and definition of the situation and social support, self-esteem, and psychological stability (Table 2). Compared to parents of children with cardiac illness (any type), this study population’s social support, self-esteem and psychological stability were significantly worse (Table 2). Reference McCubbin, McCubbin, Nevin, Cauble, McCubbin, Thompson and McCubbin18 Mothers’ understanding of the healthcare situation through communication scores was significantly higher (better) than fathers” and the comparator population” at all timepoints (Table 2).
Mothers’ family integration, cooperation, and definition of the situation subscale scores were significantly associated with STAI-S post-Norwood and at the final visit, with the highest association at the final visit (R 2 = 0.15; Table 3). Mothers’ social support, self-esteem, and psychological stability subscale scores were significantly associated with STAI-S at all timepoints, with the highest association at the final visit (R 2 = 0.11; Table 3). Understanding the healthcare situation through communication was not associated with mothers’ STAI-S.
Fathers’ family integration, cooperation, and definition of the situation scores were significantly associated with STAI-S post-Norwood and post-Stage II, the highest post-Norwood (R 2 = 0.13; Table 3). Fathers’ social support, self-esteem, and psychological stability scores were significantly associated with STAI-S post-Stage II only (R 2 = 0.25; Table 3). Fathers’ understanding of the health care situation through communication scores was significantly associated with STAI-S post-Norwood and at the final visit, highest at the final visit (R 2 = 0.18; Table 3).
Inventory of parent’s experiences findings
Inventory of parent’s experiences subdomain scores did not differ significantly between mothers and fathers (Table 2). Mother’s parental role, community, and friendship scores were significantly lower (worse) than the norm post-Stage II and by final visit, while father’s community scores were significantly lower (worse) than the norm post-Stage II and by final visit (Table 2), but family satisfaction scores were similar to norms. Reference Pek23
Mothers’ parental role scores were significantly associated with STAI-S post-Norwood and at final follow-up, highest at the final visit (R 2 = 0.24; Table 3). Mothers’ community scores were not significantly associated with STAI-S. Mothers’ friendship scores were significantly associated with STAI-S post-Norwood and at the final visit, with the highest association at the final follow-up (R 2 = 0.12; Table 3). Mothers’ family scores were significantly associated with STAI-S post-Norwood and post-Stage II, highest post-Stage II (R 2 = 0.06; Table 3).
Fathers’ parental role satisfaction was consistently associated with STAI-S, highest at the final visit (R 2 = 0.34; Table 3), but otherwise only friendship satisfaction was associated with fathers’ STAI-S post-Norwood (R 2 = 0.12; Table 3). Fathers’ community and family scores were not significantly associated with STAI-S.
Family hardiness index findings
Mothers’ mean family hardiness index subscale scores did not differ significantly from fathers (Table 2). Commitment and challenge subscale scores did not differ from the comparison group, but control subscale scores were significantly higher (better) (Table 2). Reference McCubbin, McCubbin, Thompson, McCubbin, Thompson and McCubbin20
Mothers’ commitment scores were significantly associated with STAI-S at all timepoints, with the strongest association at the final visit (R 2 = 0.18; Table 3). Mothers’ challenge scores were significantly associated with STAI-S post-Stage II and at the final visit, with the strongest association at the final visit (R 2 = 0.10; Table 3). Mothers’ control scores were significantly associated with STAI-S post-Stage II and at the final visit, highest at the final visit (R 2 = 0.14; Table 3).
Fathers’ commitment scores were significantly associated with STAI-S at all timepoints, highest post-Norwood (R 2 = 0.29; Table 3). Fathers’ challenge scores were significantly associated with STAI-S at all timepoints, highest at the final visit (R 2 = 0.28; Table 3). Fathers’ control scores were significantly associated with STAI-S post-Norwood (R 2 = 0.21; Table 3).
Family inventory of resources for management findings
Mastery and health scores were significantly lower (worse) for mothers than fathers (Table 2) and the norm (Table 2). Reference McCubbin, Comeau, Harkins, McCubbin, Thompson and McCubbin21 Mothers’ extended family social support was higher (better) than the norm (Table 2). Reference McCubbin, Comeau, Harkins, McCubbin, Thompson and McCubbin21 Fathers’ mastery and health and financial well-being were higher (better) than the norm (Table 2). Reference McCubbin, Comeau, Harkins, McCubbin, Thompson and McCubbin21
Mothers’ esteem and communication scores were significantly associated with STAI-S at all timepoints, highest at the final visit (R 2 = 0.19; Table 3). Mothers’ mastery and health scores were significantly associated with STAI-S at all timepoints, highest post-Stage II (R 2 = 0.15; Table 3). Mothers’ extended family scores were significantly associated with STAI-S at the final visit (R 2 = 0.13; Table 3). Mothers’ financial well-being scores were significantly associated with STAI-S at all timepoints, highest at the final visit (R 2 = 0.09; Table 3).
Fathers’ esteem and communication scores were significantly associated with STAI-S at all timepoints, highest post-Stage II (R 2 = 0.19; Table 3). Fathers’ mastery and health scores were significantly associated with STAI-S at all timepoints, with the strongest association at the final visit (R 2 = 0.40; Table 3). Fathers’ extended family scores were significantly associated with STAI-S post-Stage II (R 2 = 0.12; Table 3). Fathers’ financial well-being scores were significantly associated with STAI-S post-Norwood (R 2 = 0.17; Table 3).
Perceived quality of life findings
Post-Norwood, mothers’ physical, social, and cognitive health scores were significantly lower (worse) than father’s scores (Table 2), but mothers’ scores did not differ from fathers’ scores post-Stage II or at the final visit.
Mothers’ physical, social, and cognitive health and happiness scores were significantly associated with STAI-S at all timepoints, all having strong associations post-Norwood (physical: R 2 = 0.28; social: R 2 = 0.27; cognitive: R 2 = 0.19; happiness: R 2 = 0.31; Table 3).
Fathers’ physical health scores showed significant associations with STAI-S post-Norwood and post-Stage II, with the strongest correlation post-Stage II (R 2 = 0.32; Table 3). Fathers’ social health scores were significantly associated with STAI-S at all timepoints, highest post-Stage II (R 2 = 0.46; Table 3). Fathers’ cognitive health scores were significantly associated with STAI-S post-Norwood and post-Stage II, highest post-Stage II (R 2 = 0.21; Table 3). Fathers’ happiness scores were significantly associated with STAI-S at all timepoints, highest post-Stage II (R 2 = 0.51; Table 3).
Discussion
Parents of infants with single-ventricle CHD who underwent the Norwood procedure reported elevated state anxiety with a substantial proportion falling within the severe range, highlighting the significant emotional toll during this challenging postoperative period. While anxiety levels decreased over time, many parents continued to experience severe symptoms many months after their infant’s surgical procedures, underscoring the need for ongoing emotional support throughout all stages of care. Early screening for anxiety should be integrated into routine clinical care, including prenatal care, and continue longitudinally to monitor changes. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Bainton, Trachtenberg and McCrindle5,Reference Accortt and Wong24–Reference Grunberg, Geller, Hoffman, Njoroge, Ahmed and Patterson26 Electronic medical records could facilitate mental health screening of parents by incorporating brief self-reported questionnaires to identify needs, flag concerns, and provide resources. Reference Lauritzen, Kolmannskog and Iversen27,Reference Popov, Phoenix and King28 Serial screenings might identify parents at the highest risk for mental health disorders, enabling timely interventions to mitigate the long-term emotional impact of caring for a child with complex CHD. Reference Popov, Phoenix and King28
Our findings highlight notable differences in how stress, psychosocial, and quality of life factors relate to state anxiety among mothers and fathers of children with complex CHDs. A moderate number of parents reported life changes above a threshold that indicated a risk of stress-induced mental and physical illness in the near future. Reference Holmes and Rahe15 While there is a growing awareness of the impact of stress on parent mental health, the relationship between stress and physical health outcomes for parents remains less explored. Mothers exhibited worse stress-related scores than fathers, with emotional distress tied to the child’s illness emerging as a consistent predictor of their anxiety across timepoints. Maternal anxiety both before and after childbirth is a risk factor for developing a major depressive disorder. Reference Dennis, Singla and Brown29 Unlike mothers, whose anxiety was predominantly linked to emotional distress and stress tied to the experience of parenting a child with serious illness, fathers’ anxiety was more strongly influenced by psychosocial factors. Specifically, satisfaction with the parenting role, commitment, challenge, esteem, and mastery were consistent predictors of father’s STAI-S scores. These findings underscore the need for tailored psychological support that accounts for the distinct stressors and coping mechanisms of each parent. While interventions aimed at reducing emotional distress may be beneficial, particularly for mothers, supporting fathers in fostering a feeling of cohesion and adaptive coping strategies may help mitigate their anxiety.
Parents scored highly on coping strategies related to staying organised, working well with others, and making sense of their situation. Mothers also showed strong understanding of their child’s health care needs—together suggesting an active and engaged approach to coping. Strategies to boost fathers’ understanding of the health care situation through communication could mitigate their anxiety. For parents, lower scores in the area of self-care, esteem, and social support indicate potential areas for improvement. Also, low satisfaction in parent role, community, and friendships suggests challenges in maintaining social connections and feeling adequately supported within their broader social circles, highlighting the need for strategies to strengthen social support and personal well-being.
The challenge of addressing the infant’s medical care and clinical management is paramount; it is also important to consider parent stress and coping, influenced by complex, multifactorial elements. Parental responses and behaviours are shaped by their life experiences, external pressures, and coping abilities on top of the stress related to their child’s medical journey, and some of these factors are not always visible to the healthcare provider. An understanding of the complex interplay of factors is valuable for all providers, especially novice providers, who may struggle to face the challenge of managing the child’s clinical needs while supporting family-clinician interactions. Reference Grunberg, Vranceanu, Lerou and Pediatr25,Reference Grunberg, Geller, Hoffman, Njoroge, Ahmed and Patterson26 By being aware of patterns in stress and coping in parents, clinicians can better support parents” mental health, fostering a more holistic and empathetic approach to care.
These findings should be interpreted in light of the key strengths and limitations of the study. The use of multiple measures at different timepoints and participation from both mothers and fathers are notable strengths, allowing for a more comprehensive understanding of parental experiences over time. However, all study measures were developed and validated for English-speaking populations, and the perspectives of non-English-speaking individuals are not represented. Selection bias is also a potential limitation in our study, due to both the decision to enrol in the study and differential participation of parents across the three visits. Parents who declined participation may have differed from those who enrolled.
Conclusion
Many parents of infants undergoing staged palliation for hypoplastic left heart syndrome and related single right ventricle anomalies report moderate to severe anxiety. A child’s health cannot be treated in isolation from their family environment. Research has consistently shown that poor parent mental health, like high anxiety, can significantly affect a parent’s ability to care for an ill child and manage familial responsibilities, influencing the child’s development and overall health. Reference Mussatto, Van Rompay and Trachtenberg1,Reference Roberts, Kazazian and Ford9–Reference McWhorter, Christofferson and Neely12 Notably, stress and coping factors differed in their predictive value between mothers and fathers, suggesting the need for tailored clinical approaches that account for parent-specific patterns of distress and adaptation. Our findings highlight the importance of recognising parental stress, with notable differences between mothers and fathers in anxiety levels and the distinct stress and psychosocial factors influencing anxiety, as critical elements in the family dynamic. Clinicians are encouraged to assess the mental health of the entire family, identifying parents who may benefit from additional support in managing anxiety and coping. By adopting a holistic approach, healthcare providers can promote better outcomes not only for the child but also for the entire family.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126111809.
Acknowledgements
We would like to express our sincere gratitude to the 215 mothers and fathers who participated in this study. Their willingness to share their experiences during such a difficult time in their lives, as they navigated their infant’s illness, was invaluable. Without their involvement, this research would not have been possible.
Financial support
This study is supported by grants (HL135680, HL135685, HL135683, HL135689, HL135646, HL135665, HL135678, HL135682, HL135666, HL135691, and HL068270) from the NHLBI, NIH. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the paper and its final contents. The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the U.S. Department of Health and Human Services.
Competing interests
None.
Ethical Standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation, including the Department of Health and Human Services Code of Federal Regulations (45 CFR 46) Policy for Protection of Human Research Subjects and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional committees (Children’s Hospital of Wisconsin; Columbia University Irving Medical Center/Morgan Stanley Children’s Hospital of New York-Presbyterian; The Congenital Heart Institute of Florida; Arkansas Children’s Hospital; The Hospital for Sick Children; Toronto; Children’s Hospital of Philadelphia; University of Michigan Health System; Boston Children’s Hospital; Medical University of South Carolina Health University Medical Center; and Cincinnati Children’s Hospital and Medical Center).





 Open access
Open access