


Explanatory framings for mental disorder shape both stigma and clinical decision-making. Reference Baek, Kim, Park, Lim and Kim1–Reference Kvaale, Gottdiener and Haslam3 In particular, biogenetic and neuroscientific accounts (e.g. ‘chemical imbalance’, genetic/brain difference) can reduce blame yet are consistently associated with more fatalistic or essentialist attitudes, lower confidence in psychosocial interventions and greater prognostic pessimism, whereas stress-related explanations tend to promote psychosocial approaches. Reference Acker and Warner4–Reference Nolan8 Clinician stigma is consequential: it can affect therapeutic relationships and, plausibly, outcomes, Reference Knaak, Mantler and Szeto9,Reference Karver, De Nadai, Monahan and Shirk10 and biological framings can reduce clinician empathy, Reference Lebowitz and Ahn11 yet anti-stigma interventions for healthcare professionals typically yield small-to-moderate effects, with contact-based methods outperforming education alone. Reference Lien, Lin, Lien, Tsai, Wu and Li12 For some disorders, evolutionary psychiatry is a complementary perspective Reference Hunt, Abed, St John-Smith, Abed and St John-Smith13–Reference Al-Shawaf15 offering a distinct framing in which symptoms are not simply ‘breakages’, but dysregulated or inappropriately situated evolved traits. Reference Hunt and Procyshyn16–Reference Nesse19 Despite the centrality of evolutionary theory in biology, evolutionary content is not listed as core knowledge in the UK Membership of the Royal College of Psychiatrists (MRCPsych) syllabus, whereas genetics is. 20 Empirical tests of the attitudinal impact of evolutionary framings remain limited, Reference Schroder, Devendorf and Zikmund-Fisher21,Reference Brar, Swanepoel, O’Connell and McFarland22 and none, to our knowledge, have examined clinicians’ responses to an evolutionary explanation of anxiety – despite anxiety disorders being common Reference Baxter, Scott, Vos and Whiteford23 and having a relatively sound evolutionary rationale: anxiety is a defensive mechanism that protects organisms but has been tuned towards hypersensitivity rather than hyposensitivity, because the cost of overactivating is less than that of underactivating (the ‘smoke-detector principle’ Reference Nesse19,Reference Nesse24 ). We therefore aimed to compare the impact of evolutionary versus genetic explanations of anxiety, hypothesising that the evolutionary framing would be perceived as more useful and shift clinicians’ attitudes in directions consistent with anti-stigma goals.
Method
Design and setting
We conducted a multi-site, cluster-randomised, education experiment comparing two explanatory framings for anxiety disorder: an evolutionary framing versus a genetic framing. Sessions were cluster-randomised by site, delivered within routine psychiatry teaching programmes across the UK and Ireland in 2023–2024. They were conducted either online (n = 6) or in person (n = 15), with the educational presentation itself lasting approximately 30 min. Teaching took place across a wide range of sites (spanning 17 of 51 UK psychiatric trusts, plus two community healthcare organisations in Ireland), with broad geographic dispersal across England, Wales and Scotland. Sessions were scheduled opportunistically by participating educators until no further teaching opportunities could be arranged.
Educators, participants and procedure
Educators (psychiatrists at varying training grades) were recruited through professional networks and asked to book a local teaching slot titled ‘Recent developments in explanations of anxiety disorder’. Attendees were practising mental health clinicians with a range of experience and specialisation, attending the teaching sessions as part of their local training or service education activities. Participant demographics and further method details are available in Supplementary Material 1 available at https://doi.org/10.1192/bjp.2026.10615.
At the start of each session, attendees were informed that participation in an anonymous survey linked to the teaching was optional, and that the study examined how different explanations of mental disorder influence clinicians’ perceptions. A QR code and URL were provided on the first slide. Participants completed the pre-session questionnaire, received the teaching session and then completed a post-session questionnaire. Survey items were completed on personal devices.
Randomisation and masking
Sessions were allocated to either the evolutionary or genetics condition using a random sequence generated via an online list randomiser (random.org) and assigned sequentially in the order that sessions were booked. To preserve masking and prevent bias, educators were provided with only the slide deck for their allocated condition, were not informed about the alternative condition and were not told the study hypotheses or outcome variables. Educators were asked not to discuss the study with other educators if they were in contact with any. Outcome data were collected privately via participant devices and were not visible to educators during delivery.
One investigator (T.C.) oversaw survey administration and liaison with educators during data collection, but did not access or analyse the data. Following completion of all sessions, and having an estimate of participant numbers, study progress and the analysis plan were preregistered (https://osf.io/7x98y). Only after pre-registration was the data-set transferred for analysis (by A.D.H.).
Interventions
Both conditions were designed to be plausible ‘state-of-the-art’ content suitable for psychiatric education. The evolutionary condition was derived from a chapter on anxiety by Nesse; Reference Nesse, Abed and St John-Smith25 the genetics condition was derived from a review of anxiety genetics by Ask et al. Reference Ask, Cheesman, Jami, Levey, Purves and Weber26 To maximise comparability, both presentations followed the same broad structure and were matched in format and graphics as closely as possible. Slide text was copied and pasted from the source materials and simplified for teaching delivery. Educators received slides with notes (Supplementary Material 2) but were not given a verbatim script, and were asked to keep to the material. Each educator gave only one session.
Measures
Outcomes were assessed before and after the session using a mix of bespoke and existing questionnaires. We pre-registered seven primary outcomes, four of which were from the bespoke Explanations for Anxiety and Stigma questionnaire (ExAnSt), intended to capture distinct clinician attitude dimensions relevant to stigma and clinical decision-making rather than a single summed stigma score. The full ExAnSt comprised eight Likert items developed for this study, drawing primarily on items from the initial pool for the Opening Minds Scale for Health Care Providers (OMS-HC Reference Kassam, Papish, Modgill and Patten27 ) and a questionnaire for ‘Assessing Perceptions of Depression in the Context of Different Causal Explanations’. Reference Deacon and Baird28 Items were not designed to be sum-scored. ExAnSt was shared for comments around our (A.D.H. and T.C.’s) academic and clinical networks to check whether they were understandable and appropriate. Full details are provided in Supplementary Material 1.
Hypotheses
Given expectations that evolutionary education would frame anxiety as more ‘natural’ than genetics education, the 4 pre-registered ExAnSt hypotheses predicted higher scores following the evolutionary education on the following items: optimism about recovery for patients presenting with anxiety disorders (H1); anticipated willingness for patients to disclose an anxiety disorder diagnosis (H2); anticipated public willingness to seek psychiatric help for anxiety (H3); and perceived efficacy of psychosocial interventions for improving outcomes (H4) (each rated on a scale of 1–7). Two additional post-session items assessed perceived usefulness of the information for patients (H5) and clinicians (H6) on a scale of 1–5 (‘not useful’ to ‘very useful’). The remaining ExAnSt items (covering perceived likelihood of improvement with combined medication and psychotherapy, perceived patient agency, symptom changeability and perceived depth of understanding) were treated as secondary/exploratory. Finally we pre-registered a hypothesis (H7) using the pre-existing Emotion Beliefs Questionnaire (EBQ Reference Becerra, Preece and Gross29 ), expecting a positive effect on the four-item ‘negative usefulness’ subscale, which measures beliefs about the usefulness of negative emotions. All results are summarised in Table 1.
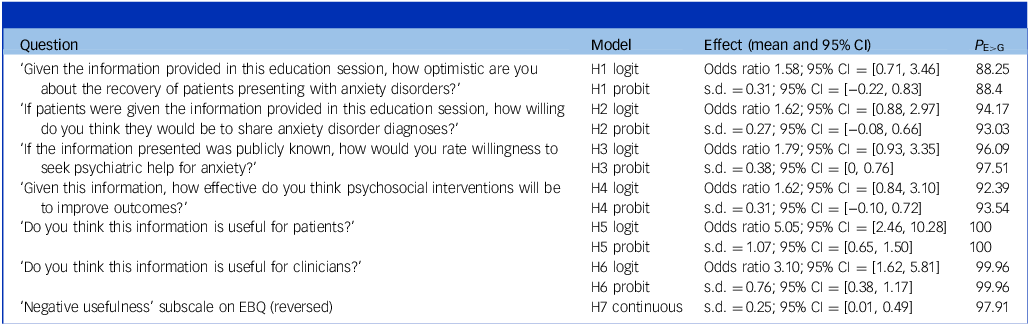
Primary results summary table

P E>G, posterior probability; H1–7, hypotheses 1–7; EBQ, Emotion Beliefs Questionnaire.
Surveys were implemented in Qualtrics, with random item order within pages and separate pages for each questionnaire. An attention-check item was embedded within both pre- and post-ExAnSt.
Prespecified analysis plan and statistical analysis
Analyses followed a prespecified plan, registered following completion of data collection but prior to any access to, or analysis of, the data-set (https://osf.io/7x98y). Data were analysed using Bayesian regression models in brms (R 4.4.1; R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/foundation/; running on Windows 11). We followed recommendations for analysis of the results as ordinal outcomes, Reference Bürkner and Vuorre30 rather than treating Likert-scale responses as continuous (avoiding assumptions that, for instance, moving from ‘4’ to ‘5’ is half as important as moving from ‘4’ to ‘6’). Effects for H1–4 were modelled using cumulative ordinal regressions of the post-session score, with a logit link as the primary analysis:
Post_Score ∼ ExplanationType + Pre_Score + LiveSession + (1|Session)
ExplanationType (evolutionary versus genetic) was the primary predictor; Pre_Score adjusted for participants’ pre-session perspectives; LiveSession controlled for delivery mode (in-person versus online); and a random intercept for session accounted for clustering effects that may have affected results in some sessions but not in others (e.g. educator enthusiasm/competence, time of day, technical issues). For post-session usefulness items (H5–6), models omitted the Pre_Score covariate. For the EBQ subscale (H7), a Gaussian model was used on standardised sum scores. Across all models we used weak, regularising priors to stabilise estimation without dominating the likelihood. Reference McElreath31
Our primary reported outcomes are odds ratios with 95% credible intervals. These represent the relative probability of choosing higher or lower Likert score ratings following the education session (i.e. an odds ratio of 2 would represent a 100% higher odds of choosing a higher Likert score after the evolutionary arm in comparison with the genetics arm – participants in the evolutionary arm were twice as likely to increase their rating than participants in the genetics arm). To indicate certainty of effect, we also report the posterior probability (P E>G). To assist interpretation, effect sizes are also reported as latent–standard deviation shifts, using probit model refits of the odds ratio logit models. Robustness checks included monotonic specifications and comparison of logit versus probit links. Full model details and results can be found in Supplementary Material 1, along with R scripts and anonymised data.
Data-handling, ethical standards and data availability
Analyses were conducted only on those participants who completed the questionnaire. Responses were excluded if participants did not provide consent for data use or failed the embedded attention check. Participant flow and exclusions, along with sample and session characteristics (including demographics), are reported in Supplementary Material 1.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. All procedures involving human participants were approved by the University of Limerick Education and Health Sciences Research Ethics Committee, Project ID 2023_04_02_EHS, or by the University of Glasgow College of Medical, Veterinary and Life Sciences Ethics Committee, application no. 200220083. Written informed consent was obtained from all participants.
Results
Sample characteristics
Of 479 individuals who opened the questionnaire, 280 did not complete it, predominantly dropping out before the education session began (n = 256). Drop-out rates did not differ meaningfully between the 2 arms (Bayes factor 2.81 favouring the null). After excluding non-completers, those who did not consent (n = 10) and those failing attention checks (n = 18), 171 participants remained: 101 in the evolutionary arm (9 sessions) and 70 in the genetics arm (10 sessions).
All participants were working in mental health services, the majority being psychiatrists at various training grades, with a minority of psychologists and other professionals. Full demographic breakdown is presented in Supplementary Material 1. Baseline comparisons revealed that participants in the genetics arm were older (mean difference 4.68 years) and less likely to be female (genetics, 47.8%; evolutionary, 66%). Both arms reported similar comprehension (genetics, mean 3.5 years; evolutionary, mean 3.78 on a 5-point scale).
H1–4: pre–post ExAnSt items
H1 (optimism about recovery)
Compared with clinicians in the genetics arm, clinicians exposed to the evolutionary framing showed higher post-session optimism about the recovery of patients with anxiety disorder (odds ratio 1.58, 95% credible interval [0.71, 3.46], P E>G = 88%). Interpreted under the proportional odds assumption, clinicians in the evolutionary arm had 58% higher odds of choosing any higher-optimism category (versus all lower categories), conditional on baseline and covariates. The probit refit corresponded to a 0.31 s.d. increase on the latent response scale (95% credible interval [−0.22, 0.83], P E>G = 88%).
H2 (anticipated willingness to share a diagnosis)
Evolutionary framing increased anticipated willingness for patients to disclose an anxiety disorder diagnosis (odds ratio 1.62, 95% credible interval [0.88, 2.97], P E>G = 94%), i.e. 62% higher odds of endorsing any higher-willingness category versus lower categories. Probit translation indicated a 0.27 s.d. shift (95% credible interval [−0.08, 0.66], P E>G = 93%).
H3 (willingness to seek help if information were publicly known)
This item showed the strongest evidence among H1–4 (odds ratio 1.79, 95% credible interval [0.93, 3.35], P E>G = 96%), i.e. 79% higher odds of endorsing any higher help-seeking category for the evolutionary arm. The probit refit yielded a 0.38 s.d. increase (95% credible interval [0.00, 0.76], P E>G = 97.5%).
H4 (expected efficacy of psychosocial interventions)
Estimates again favoured the evolutionary arm (odds ratio 1.62, 95% credible interval [0.84, 3.10], P E>G = 92%), i.e. 62% higher odds of endorsing any higher category for expected efficacy. The probit refit indicated a 0.31 s.d. shift (95% credible interval [−0.10, 0.72], P E>G = 94%).
To ensure the reliability of these findings we conducted several robustness checks, as pre-registered. Positive effects remained consistent across different model specifications. Furthermore, we fitted a single, comprehensive multi-level model to analyse all four hypotheses simultaneously. This approach, which helps account for multiple comparisons, strongly corroborated the individual results, showing high posterior probabilities (96–98%) of a positive effect for each of the 4 hypotheses when combined.
H5–6: usefulness ratings
H5 (useful for patients)
The evolutionary session was rated as substantially more useful (odds ratio 5.05, 95% credible interval [2.46, 10.28], P E>G = 100%), meaning that clinicians had ∼5-fold odds (505%) of endorsing any higher-usefulness category under the evolutionary framing. The probit refit indicated a 1.07 s.d. difference (95% credible interval [0.65, 1.50], P E>G = 100%).
H6 (useful for clinicians)
Ratings likewise favoured evolutionary framing (odds ratio 3.10, 95% credible interval [1.62, 5.81], P E>G = 99.96%), i.e. ∼3.1-fold odds (310%) of endorsing any higher-usefulness category after receiving evolutionary education in comparison with genetics education. The probit refit corresponded to a 0.76 s.d. difference (95% credible interval [0.38, 1.17], P E>G = 99.96%).
To ensure the reliability of these findings we conducted several robustness checks, as pre-registered. The very strong positive effects reported for each hypothesis remained consistent across different model specifications. All model results are provided in Fig. 1.
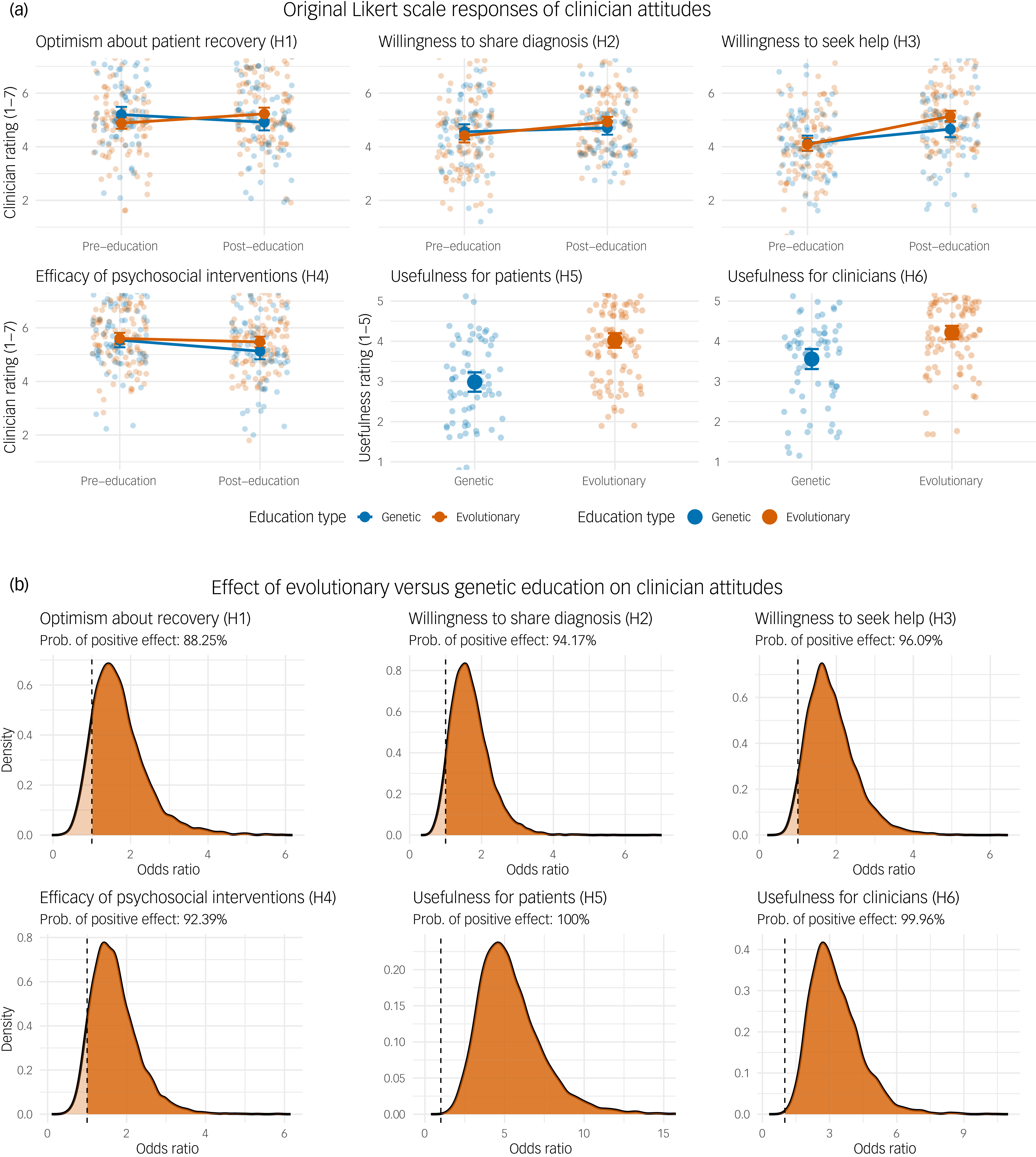
(a) Raw Likert scale responses for hypotheses 1–6 (H1–6). For H1–4, scores are shown pre- and post-education for both the genetic (blue) and evolutionary (orange (print version: grey)) arms. For H5 and H6, only post-education scores are shown. Faded points represent individual participant responses, with solid points and error bars representing the mean and 95% CI for each group. (b) Posterior distributions for the effect of evolutionary versus genetic psychoeducation on clinician attitudes (H1–6). The x axis shows the odds ratio, where values >1 favour the evolutionary arm. The dashed line at odds ratio 1 represents no difference between the groups. The dark shaded area under each curve corresponds to the posterior probability of a positive effect for the evolutionary framing, as noted in each panel. Prob., probability.

H7: EBQ negative usefulness subscale
For the negative usefulness subscale of the EBQ (higher: viewing negative emotions as less harmful/more useful), standardised sum-score analyses indicated higher post-session scores under the evolutionary framing. The mean difference was 0.25 s.d. (95% credible interval [0.01, 0.49], P E>G = 97.91%).
In a posterior predictive check the Gaussian model showed a right-shifted distribution, probably due to some ceiling effects (participants believing, both pre- and post-session, that negative emotions are useful). Neither gamma nor log-normal models provided substantially better fit for the data.
Pre–post change within the evolutionary arm
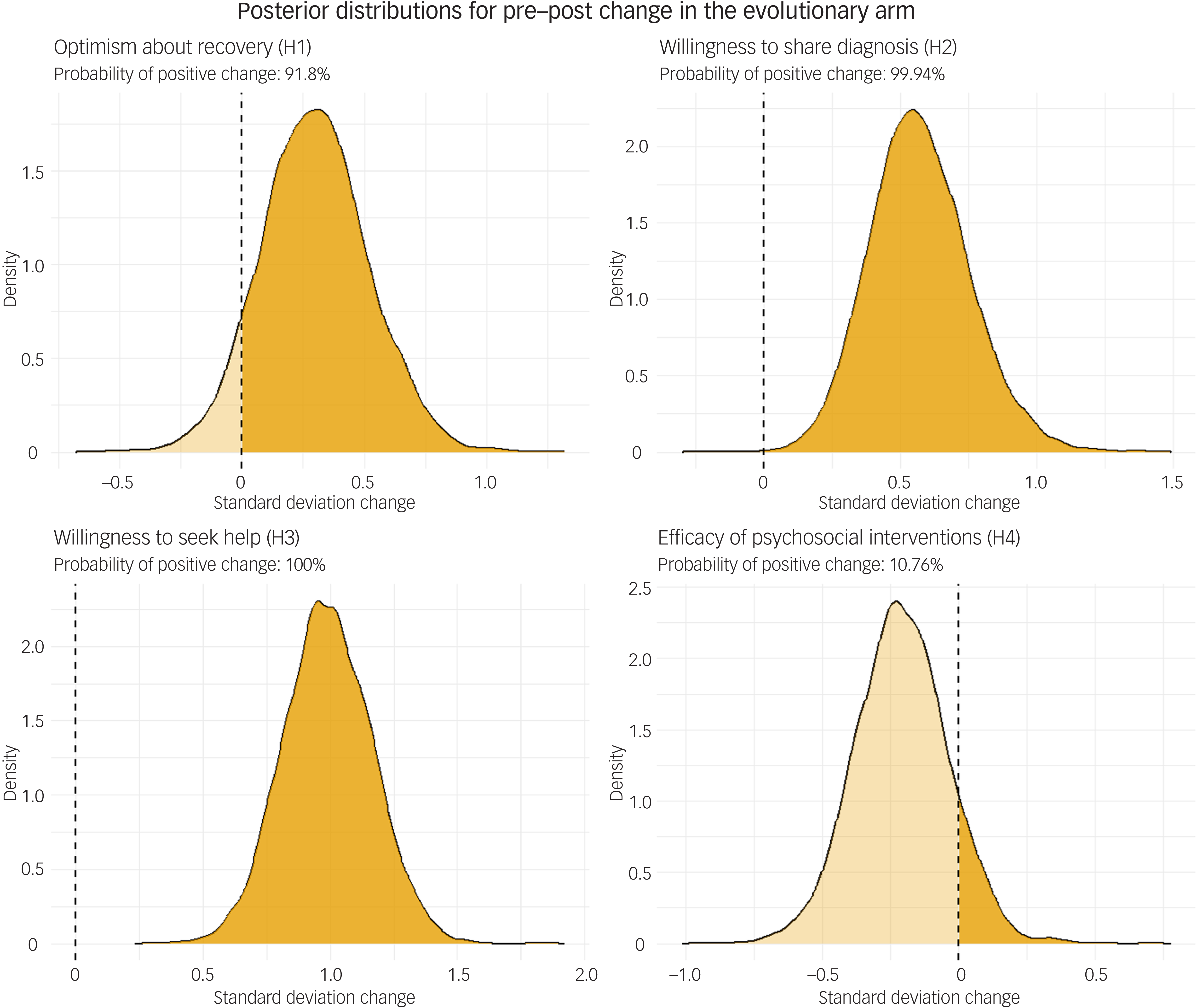
To determine whether effects were driven by evolutionary education improving attitudes or genetic education worsening them, we conducted additional pre–post analyses within the evolutionary arm (see Fig. 2); full model specification and results are given in Supplementary Material 1.
Posterior distributions for pre–post change within the evolutionary education arm for hypotheses 1–4 (H1–4), based on repeated-measures probit models. The x axis shows the change from pre- to post-education in standard deviation units, with the dashed line at 0 indicating no change. The dark shaded area corresponds to the posterior probability of a positive change, as noted in each panel.

H1 (optimism about recovery)
Evolutionary education increased optimism (odds ratio 1.70, 95% credible interval [0.80, 3.26], P(change >0) = 90.38%). The probit refit corresponded to a 0.30 s.d. increase on the latent response scale (95% credible interval [−0.12, 0.74], P(change >0) = 91.80%).
H2 (anticipated willingness to share a diagnosis)
Evolutionary education increased clinicians’ anticipation of patients’ willingness to share a diagnosis (odds ratio 2.48, 95% credible interval [1.40, 4.34], P(change >0) = 99.95%). The probit model indicated a 0.57 s.d. shift on the latent response scale (95% credible interval [0.23, 0.96], P(change >0) = 99.94%).
H3 (willingness to seek help if information were publicly known)
This item showed the largest pre–post change after evolutionary education (odds ratio 5.15, 95% credible interval [2.84, 8.71], P(change >0) = 100.00%). The probit refit yielded a substantial 0.99 s.d. increase on the latent scale (95% credible interval [0.65, 1.33], P(change >0) = 100.00%).
H4 (expected efficacy of psychosocial interventions)
In contrast to the other measures, there was no evidence of a positive change for this item; in fact, the point estimate was negative (odds ratio 0.76, 95% credible interval [0.44, 1.28], P(change >0) = 12.64%). The probit refit similarly indicated a small negative shift of −0.21 s.d. on the latent scale (95% credible interval [−0.55, 0.12], P(change >0) = 10.76%). This indicates that the positive effect of the evolutionary arm versus the genetics arm was driven by genetic explanations having a relatively larger negative effect on the expected efficacy of psychosocial interventions.
Further stigmatisation items
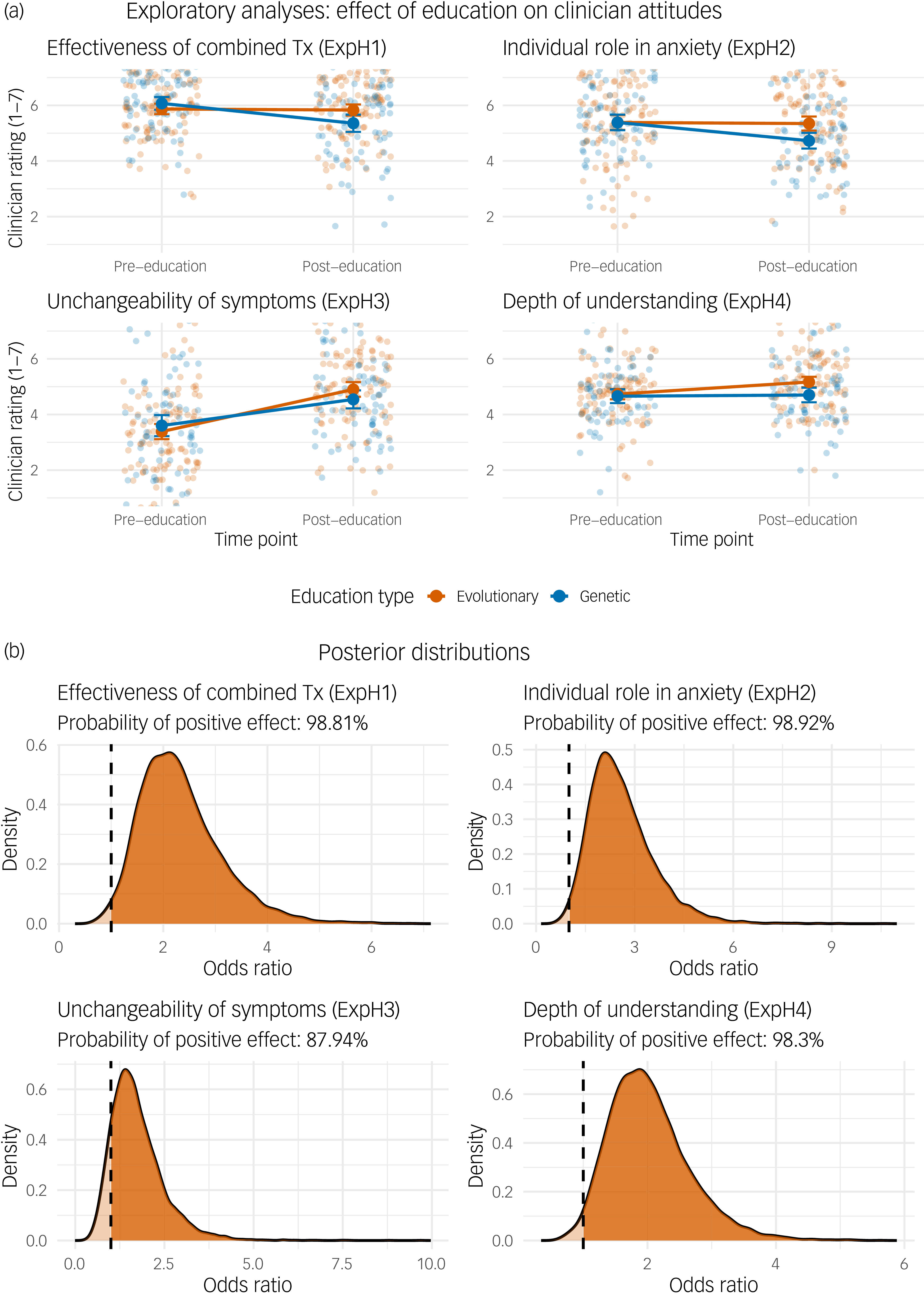
We conducted exploratory analyses on the four additional ExAnSt items not included in our pre-registered hypotheses. For each item, we compared the evolutionary and genetics arms (Fig. 3), then examined the pre–post effect of the evolutionary arm alone. Full model specification and results are provided in Supplementary Material 1.
(a) Pre- and post-intervention clinician ratings for the four exploratory hypotheses, by psychoeducation type. The panels show clinician ratings on a 7-point scale before and after receiving either evolutionary (orange (print version: grey)) or genetic (blue) psychoeducation. Individual points are jittered raw scores from each participant. The solid lines connect the group means at each time point, with the surrounding error bars representing 95% CIs. (b) Posterior distributions of odds ratios for the effect of evolutionary (versus genetic) psychoeducation from the four exploratory analyses. Each curve represents the posterior probability density of the odds ratio. The vertical dashed line at odds ratio 1 indicates the point of no effect. The shaded area to the right of this line represents the posterior probability that the evolutionary arm had a more positive effect than the genetic arm (odds ratio >1), the value of which is reported as a percentage in each panel’s subtitle.

ExpH1 (effectiveness of combined therapy)
Evolutionary explanations increased belief in the effectiveness of combined medication and psychotherapy compared with genetic explanations (odds ratio 2.21, 95% credible interval [1.14, 4.20], P E>G = 99%; probit: 0.51 s.d., 95% credible interval [0.13, 0.89]). However, the pre–post effect of evolutionary education alone showed only 36.14% probability of a positive effect, indicating that between-arm difference was primarily driven by a negative effect of genetic education.
ExpH2 (individual’s role in anxiety)
Evolutionary explanations increased belief that individuals can instigate or mitigate their anxiety (odds ratio 2.43, 95% credible interval [1.17, 4.91], P E>G = 99%; probit: 0.56 s.d., 95% credible interval [0.10, 0.99]). Again, the pre–post effect of evolutionary education alone showed only 28.99% probability of a positive effect, with the between-arm difference driven by a negative effect of genetic education.
ExpH3 (symptom unchangeability)
Evolutionary explanations were associated with viewing symptoms as being more unchangeable, although evidence was weaker (odds ratio 1.60, 95% credible interval [0.71, 3.53], P E>G = 88%; probit: 0.24 latent s.d., 95% credible interval [−0.28, 0.75]). The pre–post effect of evolutionary education alone showed 100% probability of a positive effect. Note that higher scores indicate greater perceived unchangeability; both arms increased this perception, with evolutionary education having a larger effect.
ExpH4 (depth of understanding)
Evolutionary explanations increased self-rated depth of understanding of anxiety disorders (odds ratio 1.94, 95% credible interval [1.06, 3.49], P E>G = 98%; probit: 0.45 s.d., 95% credible interval [0.09, 0.80]). The pre–post effect of evolutionary education alone showed 99.88% probability of a positive effect, indicating that this between-arm difference was driven by a positive effect of evolutionary education.
Discussion
Explanatory frameworks for mental disorders shape clinical attitudes, and also potentially therapeutic relationships and patient outcomes. This multi-site, cluster-randomised trial provides robust evidence that evolutionary explanations of anxiety shift clinicians’ attitudes in directions consistent with destigmatisation, particularly when compared with genetic explanations. Across the primary pre-registered outcomes, evolutionary education yielded higher odds of endorsing optimistic recovery expectations, greater anticipated patient willingness to disclose diagnoses and increased public willingness to seek help. Clinicians also perceived psychosocial interventions as more effective following evolutionary education, although exploratory analysis revealed that this difference was partly driven by a negative effect of genetic education (which suggests that our participants made the common mistake of equating genetic evidence with fixedness or pathology). The subscale of negative usefulness shifted in the expected direction, consistent with evolutionary framing helping clinicians view negative affect as functional rather than inherently pathological.
Most strikingly, clinicians rated evolutionary explanations as substantially more useful – approximately 5-fold higher odds for patients (P E>G = 100%) and 3-fold for clinicians. These represent very large effect sizes (d = 1.07 and 0.76, respectively). One question that cannot be answered with these data is the precise source of this usefulness. Is enhanced usefulness for clinicians merely due to deepening understanding, or did they expect it to translate into different clinical interactions and outcomes? Expected usefulness to patients may derive from factors tested (e.g. willingness to share diagnosis or seek help), or from broader implications of employing evolutionary explanations in clinical interactions or public messaging. Investigating this further – and directly measuring the impact of such explanations on patients – is an obvious next step.
These findings address a gap in the literature on explanatory framing and stigma. Meta-analyses consistently show that mechanistic biological explanations reduce blame but increase essentialist beliefs, perceived dangerousness, social distance and prognostic pessimism. Reference Kvaale, Gottdiener and Haslam3,Reference Angermeyer, Holzinger, Carta and Schomerus5,Reference Loughman and Haslam7 Experimental work demonstrates that biological explanations specifically reduce clinician empathy. Reference Lebowitz and Ahn11 Our results show that evolutionary explanations offer an alternative biological framework that avoids these negative consequences – framing anxiety as a calibrated defence system that can become dysregulated, rather than as genetic pathology.
This converges with Schroder et al’s Reference Schroder, Devendorf and Zikmund-Fisher21 finding that evolutionary framings reduce self-stigma in people with depression, particularly regarding openness about diagnosis. However, our exploratory analyses reveal that evolutionary explanations are not uniformly beneficial: they increased the perception of symptom unchangeability. These results are seemingly at odds with simultaneously increasingly optimistic expectations for recovery. This contradiction could be reconciled if evolutionary explanations simultaneously imply that symptoms of anxiety are somewhat natural, unavoidable and hard to alter in an immediate moment (hence unchangeable; and also explaining pessimism about psychosocial approaches), but are not ‘breakages’ and a reason for long-term cynicism. This should, however, clarify the fact that evolutionary explanations do not inherently lead to depathologisation.
Implications for clinical education
The exceptionally high usefulness ratings have direct implications for psychiatric training. Despite evolutionary theory’s foundational role in the biological sciences, the MRCPsych curriculum does not list evolutionary content as core knowledge 20 whereas genetic methods feature prominently. Our findings suggest that this represents a missed opportunity and that integration of evolutionary perspectives into clinical education could foster more hopeful and therapeutically empowering attitudes among clinicians – with probable downstream benefits for the patients they serve. Despite the framing of this study as pitting them against each other, genetic and evolutionary explanations are complementary. Both are consistent with understanding anxiety as a disorder worthy of treatment and psychosocial intervention, and teaching them alongside one another is a natural step forward.
Importantly, the effect sizes observed here compare favourably with established anti-stigma interventions. Meta-analyses of interventions for healthcare professionals show that contact-based approaches – typically the most effective – yield standardised mean differences of approximately −0.35, whereas education alone achieves only −0.10. Reference Lien, Lin, Lien, Tsai, Wu and Li12 Several of our outcomes matched or exceeded these benchmarks through a single, 30 min educational session. This suggests that evolutionary content could be a high-leverage, scalable addition to existing curricula, complementing rather than replacing contact-based approaches.
These findings support long-standing proposals that evolutionary perspectives deserve greater integration into psychiatric education. Reference Abed, Ayton, St John-Smith, Swanepoel and Tracy32,Reference Nesse, Bergstrom, Ellison, Flier, Gluckman and Govindaraju33 The practical barriers are low: evolutionary explanations require no additional clinical resources, can be delivered within existing teaching structures and – as our study demonstrates – are readily understood and valued by clinicians. Given the low implementation costs and large observed effects, serious consideration of evolutionary psychiatry’s role in training is warranted.
Strengths and limitations
Strengths include wide geographic dispersal across UK and Irish sites; substantial masking, with educators and participants unaware of hypotheses and arms; cluster adjustment for session effects; baseline-adjusted ordinal modelling appropriate to measurement level; and adherence to a pre-registered analysis plan.
Several limitations warrant consideration. First, we measured attitudes immediately post-session; whether effects persist or translate into clinical behaviour remains unknown. Second, despite randomisation, the genetics arm was older and with a higher proportion of male participants, although baseline adjustment should mitigate this. Third, attrition was substantial, as is common in educational research, although drop-out rates did not differ meaningfully between arms. Fourth, educators were recruited through professional networks including an evolutionary psychiatry event, potentially affecting presentation enthusiasm, although masking to outcomes and session random effects should limit bias. Fifth, our bespoke questionnaire, while drawing on validated instruments, requires further psychometric evaluation. Finally, this study focused solely on anxiety; generalisability to other disorders requires testing.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10615
Data availability
All the (anonymised) data and analytic code are available via Supplementary Material 1.
Acknowledgements
We thank Jordan Martin, Camila Scaff, Riadh Abed, Randolph Nesse, Paul St-John Smith and Lukas Gunschera for relevant discussions. In memory of Dan Stein.
Author contributions
A.D.H. contributed to the conception and design of the study, data analysis and interpretation and drafted the manuscript. T.C. contributed to the conception and design of the study and organised data collection. C.R. contributed to study design. L.A.-S. contributed to study design. A.V.J. contributed to study design. G.B. contributed to data collection. T.K. contributed to data analysis. G.G. contributed to data interpretation. N.C. contributed to data interpretation. D.B., M.B., A.D., B.d.B., A.E., S.G., B.G., B.I., S.I., U.J., M. Kamran, M. Kelly, H.O., R.S.P., C.S., A.S., E.T.-C., S.V., M.V. and T.W. contributed to data collection. All authors reviewed the manuscript critically for important intellectual content, gave final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
A.D.H. was funded by University of Zurich Forschungskredit (grant no. FK-21-06) and the Swiss National Science Foundation (grant no. P500PS_222068).
Declaration of interest
None.
Transparency declaration
A.D.H. affirms that the manuscript is an honest, accurate and transparent account of the study being reported, that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.



 Open access
Open access
eLetters
No eLetters have been published for this article.