


1. Introduction
‘Integration’ has been a buzzword in the international health policy discourse, holding high appeal for scholars, practitioners, and health policymakers. Health system integration plays a pivotal role in enhancing the overall quality, efficiency, and effectiveness of healthcare delivery (Kodner and Spreeuwenberg, Reference Kodner and Spreeuwenberg2002; Maruthappu et al., Reference Maruthappu, Hasan and Zeltner2015; Toth, Reference Toth2020). By breaking down the silos between different providers, services, and systems, integration fosters seamless coordination and collaboration, leading to improved patient outcomes and experiences (Piquer-Martinez et al., Reference Piquer-Martinez, Urionagüena, Benrimoj, Calvo, Dineen-Griffin, Garcia-Cardenas, Fernandez-Llimos, Martinez-Martinez and Gastelurrutia2024). It enables a more holistic approach to healthcare, ensuring that individuals receive comprehensive and well-coordinated care. Additionally, health system integration can help optimize resource utilization, reduce duplication of services, and enhance cost-effectiveness, ultimately contributing to a more sustainable and resilient health system (Rocks et al., Reference Rocks, Berntson, Gil-Salmerón, Kadu, Ehrenberg, Stein and Tsiachristas2020; Wan et al., Reference Wan, Lin and Ma2002; WHO, 2015).
However, integrating a health system is never an easy job. While beneficial, it faces several significant barriers resulting from systemic fragmentation, bureaucratic siloism, cultural conflict, and vested interests, which often impede necessary integration (Castelli et al., Reference Castelli, Erskine, Hunter and Hungin2023). Importantly, many such barriers do not come from the health sector per se but rather are rooted in the broader bureaucratic ecology (Qian and Ramesh, Reference Qian and Ramesh2024). Successful healthcare reforms are hardly due to good technical design alone; rather, they are often explained by how the policy dimension of the reform is managed (Sparkes et al., Reference Sparkes, Bump, Ozcelik, Kutzin and Reich2019; Wat and Gilson, Reference Wat and Gilson1994). By the same token, failing to navigate within the complex political economy is often the fundamental reason behind frustrated health reforms (Hsiao, Reference Hsiao2007). Therefore, the process of integration must be scrutinized in a broader context, taking into account the policy and administrative dynamics involved. As underscored by Powell and Mannion (Reference Powell and Mannion2023), the study of health policy should be informed routinely by insights from the ‘wider policy sciences literature’ to fully account for the processual dynamics of healthcare reforms.
This present study enriches scholarly understanding of health system integration from a policy sciences perspective through analysing local pilots in China. Specifically, the concept of collective policy entrepreneurship is introduced to shed light on how difficult health system integration reforms are designed and managed, as well as the ‘success factors’ behind such reforms. The twin cases of county medical conglomerates illustrate different motivations and pathways for vertical integration at the local level. The policy entrepreneurs in these cases employed a variety of strategies to overcome hurdles that eventually brought the pilots to fruition.
The contributions of this study are threefold. First, complementing the health policy scholarship, policy science theories offer a penetrative vantage point to elucidate the complexities of real-world healthcare reforms (Wat and Gilson, Reference Wat and Gilson1994; Powell and Mannion, Reference Powell and Mannion2023). This study illuminates the profound interactions between human agency and structural conditions in shaping the outcomes of entrepreneurial reforms in the health sector. Second, numerous systematic reviews and normative discussions are documented in the health system integration literature, but there is a paucity of in-depth case studies examining the processual dynamics of such reforms, especially at the subnational level. Putting two Chinese cases under the ‘microscope’, this study fills the gap by revealing the various hurdles for integration and the strategies used to overcome such hurdles in the integration of county-level health systems. Third, the experiences derived from these two cases in terms of both design and reform strategies may offer ‘playbook’ insights for health administrators and policymakers in other low- and middle-income countries that are also contemplating health system integration.
2. Health system integration
Integrated care refers to the provision and management of health services based on consumer demand for diagnosis, treatment, long-term care, and rehabilitation, which are delivered through collaboration between institutions at different levels and locations within the health system (WHO, 2015). By fostering collaboration and communication among various healthcare stakeholders, including hospitals, primary care providers, specialists, community organizations, and public health agencies, integration creates a more connected and coordinated system of care (Maruthappu et al., Reference Maruthappu, Hasan and Zeltner2015; Miller, Reference Miller1996). This interconnectedness facilitates the seamless transfer of information, continuity of care, and the implementation of evidence-based practices across different healthcare settings (He and Tang, Reference He and Tang2021; Wan et al., Reference Wan, Lin and Ma2002).
Depending on the degree of connectedness between organizations, integrated care can take different forms: linkage, coordination, and full integrationFootnote 1 (Leutz, Reference Leutz1999). Vertical integration, typically involving the integration of primary health facilities and secondary or tertiary hospitals, has been gaining prominence in the last decade (Carlin et al., Reference Carlin, Dowd and Feldman2015; Wang et al., Reference Wang, Yang, Zheng and Yuan2024). There are primarily three reasons for the high appeal of vertical integration to policymakers. First, many health systems, especially those of high- and middle-income countries, have become highly specialized and fragmented, incapable of responding to increasing multi-morbidity, particularly among the elder population (He and Tang, Reference He and Tang2021; Tsiachristas et al., Reference Tsiachristas, Vrangbæk, Gongora-Salazar and Kristensen2023). There is a critical need to integrate not only multiple specialties along the horizontal dimension but also different levels of care to improve continuity of care. Second, despite the wide recognition of the value of primary care, such systems remain weak in many countries, leading to reduced accessibility, capacity deficit, and increased cost (Qian and Ramesh, Reference Qian and Ramesh2024). Hence, closer vertical integration is believed to be a necessary step to strengthen primary care systems through sharing resources with secondary and tertiary facilities (Baker et al., Reference Baker, Bundorf and Kessler2014; Carlin et al., Reference Carlin, Dowd and Feldman2015). Third, the rapid escalation of health expenditures worldwide is primarily driven by the curative sector, which creates huge volumes of high-cost but low-value services. Vertical integration of services can help strengthen preventive care and early intervention, thus representing a sustainable approach for cost containment (Weeks et al., Reference Weeks, Gottlieb, Nyweide, Sutherland, Bynum, Casalino, Gillies, Shortell and Fisher2010).
3. Policy entrepreneurs: who are they? What do they do?
Since its inception, the concept of policy entrepreneurs has been a very important analytical heuristic to explain policy change. In John Kindgon’s (Reference Kingdon1984) seminal multiple streams framework, policy entrepreneurs, defined as individuals willing to invest their resources – time, energy, reputation, and sometimes money – in return for future policies they favour, conjoin the politics, policy, and problem streams and open the policy window. Dedicated to changing the ‘existing ways of doing things’, they creatively recombine intellectual, political, and organizational resources into new products and new courses of action for governments (Oliver and Paul-Sheehan, Reference Oliver and Paul-Shaheen1997). Policy entrepreneurs typically demonstrate several significant attributes: ambition, social acuity, defining problems, tenacity, and leading by example (Mintrom, Reference Mintrom2019; Mintrom and Norman, Reference Mintrom and Norman2009). The literature has documented a variety of entrepreneurial strategies and tactics used by policy entrepreneurs in promoting innovations, such as venue shopping, issue framing, negotiating, coalition building, and networking (Cairney, Reference Cairney2018; Petridou and Mintrom, Reference Petridou and Mintrom2021).
The health sector represents fertile ground for policy entrepreneurship for several reasons. First and foremost, this sector is a classical complex adaptive system that involves numerous interdependent components centred on core health system functions: governance, provision, financing, payment, and regulations (Roberts et al., Reference Roberts, Hsiao, Berman and Reich2003). The complex interactions between these components often lead to non-linear systemic outputs and cascade effects, hence triggering self-organization and emergent order (Husain, Reference Husain2017; Paina and Peters, Reference Paina and Peters2012). Changes in one part of the health system require complementary changes in other parts for them to be effective, eventually entrenching into a path-dependent policy gridlock (Bali et al., Reference Bali, He and Ramesh2022). For a major reform to succeed, a large constellation of activities needs to change, including the behaviours of health professionals and operational mechanisms. Such deep complexities make health reforms often defy fixed ‘blueprint’ approaches and inherently require repeated policy experimentation and continuous entrepreneurialism (He et al., Reference He, Fan and Su2022; Husain, Reference Husain2017).
Second, the high technical complexity of this domain creates certain entry barriers for ordinary policy actors while granting professionals and technocrats significant authority for entrepreneurial manoeuvres. The inherent asymmetric information in healthcare also leaves considerable room for issue framing and manipulation. There are numerous examples showing how savvy framing helps to build a favourable rhetorical space and amass critical resources for difficult health reforms (He, Reference He2018; Oborn et al., Reference Oborn, Barrett and Exworthy2011). Third, there is typically a great deal of material interest and ideological bias concentrated in the health sector. Resistance from the medical profession and the medical-industrial complex has been rather salient in impeding necessary reforms (Hsiao, Reference Hsiao2007; Pierson, Reference Pierson1994). Hence, healthcare reforms often require not only strong political will but also innovative strategies to overcome such resistance.
Most earlier studies characterized policy entrepreneurship as an elite-level phenomenon primarily active at the agenda-setting stage of the policy process, but the recent literature suggests that mid- and low-level bureaucrats, who are conventionally described as mere implementers, can also play the role of policy entrepreneurs, not only in implementation but also in policy design (Arnold, Reference Arnold2015; Shi and He, Reference Shi and He2025). The unique strength of these bureaucratic policy entrepreneurs is their professional knowledge, frontline know-how, intimate familiarity with local problems, and discretionary power, all of which allow them to mount innovative local pilots even in the absence of explicit national-level policy guidelines (Cohen and Golan-Nadir, Reference Cohen and Golan-Nadir2020; Lavee and Cohen, Reference Lavee and Cohen2019). As Cairney (Reference Cairney2018) has insightfully pointed out, policy entrepreneurs play varying roles in different political settings. In large systems, they are like surfers waiting for the big wave, whereas in small systems, especially in smaller countries or local governments, they tend to be more influential, like ‘Poseidon moving the sea’.
The recent literature has increasingly recognized the critical importance of collective policy entrepreneurship in driving complex innovations, with entrepreneurial individuals coming from within the bureaucracy in some cases (Tang et al., Reference Tang, Cheng and Cai2020; Wang et al., Reference Wang, Tang and Cai2025) and across sectoral boundaries in other ones (He and Ma, Reference He and Ma2020; He et al., Reference He, Fu and Tang2026). While we celebrate this nascent literature for its due recognition of collective agency in policy innovations, it largely remains descriptive and there is limited understanding on the texture of such policy entrepreneurship, as opposed to the ‘conventional’ (largely) individual entrepreneurship described in Mintrom and Norman (Reference Mintrom and Norman2009). A comparative case study approach is well suited to help us unpack these complexities and shed light on the nuances in terms of the internal dynamics of collective policy entrepreneurship and the ‘boundary conditions’ for its effectiveness.
4. The Chinese health system
China’s health system was afflicted by significant fragmentation, leading to disparities in service quality, accessibility, and affordability across regions and between urban and rural areas. The separation of financing, provision, and regulation further contributed to fragmentation in health governance, with multiple ministries overseeing different aspects of the health system (Hsiao, Reference Hsiao2007; Ramesh et al., Reference Ramesh, Wu and He2014). This fragmented governance structure led to overlapping responsibilities, inconsistent policies, and inefficient resource allocation. The fragmentation in health governance was considerably eased in 2018 with the establishment of the National Healthcare Security Administration (NHSA), which consolidated most authorities related to social health insurance (SHI) management and purchasing. The National Health Commission and its local arms were made responsible for regulatory oversight and professional supervision (He et al., Reference He, Bali and Ramesh2022).
Created in line with the country’s urban–rural dichotomy and the division between formal and informal sectors, China’s two major SHI programmes are administered at the prefectural levels. Despite the very high coverage of SHI (currently at 96.5% nationwide), there were hundreds of risk pools in China, thus hampering the power of strategic purchasing (Meng et al., Reference Meng, Fang, Liu, Yuan and Xu2015). The service delivery system also suffers from both horizontal and vertical fragmentation. Public hospitals, the key providers of health services in China, only receive very nominal subsidies from the government. As SHI and out-of-pocket payments constitute the lion’s share of hospitals’ incomes, the economic incentives encourage competition rather than coordination between hospitals (Yip and Hsiao, Reference Yip and Hsiao2014). The fee-for-service (FFS) payment model prevalent in China incentivizes providers to focus on volume rather than quality of care, exacerbating the fragmentation and overutilization of services. In theory, primary, secondary, and tertiary facilities are connected through the two-way referral system, which is unfortunately incompatible with the existing financial incentives that drive the behaviours of healthcare providers. It is in their financial interests to compete for patients because a higher volume of patients leads to more revenue. Weak gatekeeping mechanisms also make patients’ self-referral and doctor shopping possible, exacerbating inappropriate hospital admissions and unnecessary expenditures (Eggleston et al., Reference Eggleston, Shen, Lau, Schmid and Chan2008).
The perverse incentives cited above shaped a peculiar top-heavy structure in which China’s primary care system was significantly weakened (Li et al., Reference Li, Lu, Hu, Cheng, De Maeseneer, Meng, Mossialos, Xu, Yip, Zhang, Krumholz, Jiang and Hu2017; Qian and Ramesh, Reference Qian and Ramesh2024). Large hospitals in urban areas often experience overwhelming patient volumes, leading to long wait times, overcrowding, and reduced quality of care. Most such medical cases could be managed at the primary care level. As a result, total expenditure on health has escalated at a rapid rate while huge amounts of waste have been created in public hospitals (Eggleston et al., Reference Eggleston, Shen, Lau, Schmid and Chan2008; Yip et al., Reference Yip, Hsiao, Meng, Chen and Sun2010). Addressing the fragmentation of China’s health system requires comprehensive reforms that promote integration, coordination, and alignment of incentives across the care continuum.
The concept of integrated care started to gain prominence in China from the 2010s. The government also encouraged local pilots to experiment with various integration models based on local conditions (Feng et al., Reference Feng, Zhu and Chen2022). The county medical conglomerate has emerged as an increasingly popular model of vertical integration. There are more than 2,800 counties (or equivalent administrative divisions) in China, with an average population of 498,000. Sitting at the top of the country’s three-tier health system, county hospitals provide services to over 70% of the entire population (Zhu et al., Reference Zhu, Zhao, Dou, Guo, Gu, Gao and Wu2021). Unfortunately, weak gatekeeping has led to a drastic outflow of patients from counties to tertiary hospitals in major cities, gradually ‘hollowing out’ these cornerstones of the health system. The situation of township health centres, the second-tier facilities – is even worse. They are supposed to be the first point of contact for many rural residents seeking care, but inadequate funding, manpower shortage, and limited medical technologies has long afflicted numerous township health centres (Li et al., Reference Li, Lu, Hu, Cheng, De Maeseneer, Meng, Mossialos, Xu, Yip, Zhang, Krumholz, Jiang and Hu2017; Li et al., Reference Li, Krumholz, Yip, Cheng, De Maeseneer, Meng, Mossialos, Li, Lu, Su, Zhang, Xu, Li, Normand, Peto, Li, Wang, Yan, Gao, Chunharas, Gao, Guerra, Ji, Ke, Pan, Wu, Xiao, Xie, Zhang, Zhu, Zhu and Hu2020). As a result, the primary and secondary foundations of the health system have been severely weakened, creating a vicious cycle where county hospitals and township health centres suffer from a significant loss of patients that in turn undermines their capacity and reduces their income, while reduced capacity further weakens their attractiveness to patients. Such a sorry state of affairs has powerfully fuelled rapid cost inflation without necessarily providing higher value care (Qian and Ramesh, Reference Qian and Ramesh2024).
In a typical medical conglomerate, one or two county hospitals are appointed as the ‘lead hospitals’ to not only provide secondary and tertiary care but also coordinate care provision in the entire county. Previously disconnected from county hospitals, township health centres are now integrated with hospitals in terms of case referral, staff training, and capacity building. In some highly integrated cases, staff appointments, finance, and asset management are also streamlined to the lead hospital (Wang et al., Reference Wang, Sun, Birch, Gong, Valentijn, Chen, Zhang, Huang and Yang2018). Such a high level of integration allows stronger planning and coordination. However, conglomeration in the Chinese health system requires two institutional barriers to be overcome. The first is the fragmented health governance system. Until 2019, local health bureaus were hardly able to dominate decision-making because the social security bureaus that managed major SHI programmes tended to have different agendas and priorities (Hsiao, Reference Hsiao2007; Ramesh et al., Reference Ramesh, Wu and He2014). As a significant restructuring of the local health system, conglomeration would require cooperation from many other departments. Health policy coordination is therefore essential but difficult. Second, recent evidence indicates that vertical integration would yield limited effects in service outcome and cost containment unless the reform is accompanied by rigorous provider payment methods (Looman et al., Reference Looman, Struckmann, Köppen, Baltaxe, Czypionka, Huic, Pitter, Ruths, Stokes, Bal and Rutten-van Mölken2021; Tsiachristas et al., Reference Tsiachristas, Dikkers, Boland and Rutten-van Mölken2013; Wang et al., Reference Wang, Sun, Birch, Gong, Valentijn, Chen, Zhang, Huang and Yang2018). This is particularly the case in China, where SHI is the biggest provider of health services, and the financial incentives set through payment rules are of pivotal importance in shaping providers’ behaviours. However, FFS used to be the dominant payment method, and local social security bureaucracies have appeared hesitant in adopting alternative methods (Yip and Hsiao, Reference Yip and Hsiao2008; Yip et al., Reference Yip, Hsiao, Chen, Hu, Ma and Maynard2012). Therefore, visionary planning must be matched with strong leadership if an integration reform is to come through.
5. Methodology
Qualitative in nature, this study adopted the comparative case studies approach to investigate two county-level medical conglomeration initiatives in China. Case study research was a suitable strategy for this study for two reasons. First, it allowed the researchers to look at the phenomenon in-depth and within its real-life context so that the findings generated insights into how the phenomenon of policy entrepreneurship actually occurred within a given situation (Yin, Reference Yin2009). Second, investigating the integration reforms in their natural setting, case study research allowed the questions of why and how to be answered with a relatively full understanding of the nature and complexity of the complete phenomenon.
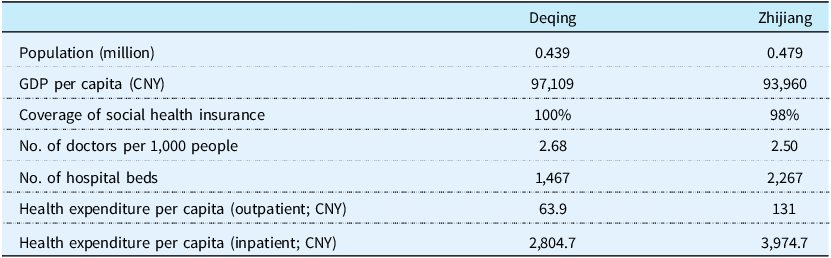
The two cases were selected through purposive sampling because it was our intention to construct a design to highlight varying pathways to health system integration based on local conditions. Deqing in Zhejiang Province and Zhijiang in Hubei Province were selected for investigation; both belong to the early cohort of medical conglomeration pilots in China. Located in coastal and central China respectively, Zhejiang is one of China’s economic powerhouses with a prosperous private economy, while Hubei – with a sizable agricultural sector – falls into the middle-income category. The profile of the two case counties and their geographic locations are presented in Table 1 and Figure 1, respectively. There are notable similarities between the two in terms of population (both very close to the average size of a county in China), GDP per capita, and SHI coverage. However, there are differences between the two in regard to the cost profile of their respective health systems prior to the reforms. Zhijiang, despite its relatively low economic status, appeared to experience a more severe cost-inflation problem.
Location of the two case counties. Source: created by the authors.

Profile of case counties

Note: data as of 2016, prior to major integration reforms.
Source: local statistical reports.
Our case selection follows a ‘most similar systems’ comparative design. The two counties share high similarity on several key potential confounding variables at the county level: population size, GDP per capita, SHI coverage, and their status as early national pilot sites. Additionally, both innovations took place before the landmark national health governance reform in 2018 when the NHSA was established. Therefore, the selection of Deqing and Zhijiang allows us to control for both locality-specific conditions and common national-level top-down factors. The critical, theoretically-informed differences lie in their broader provincial contexts and their local pre-reform system pressures. This design enables a focused investigation into how these specific differing conditions – operating within otherwise similar county-level systems – shaped divergent pathways and outcomes for health system integration.
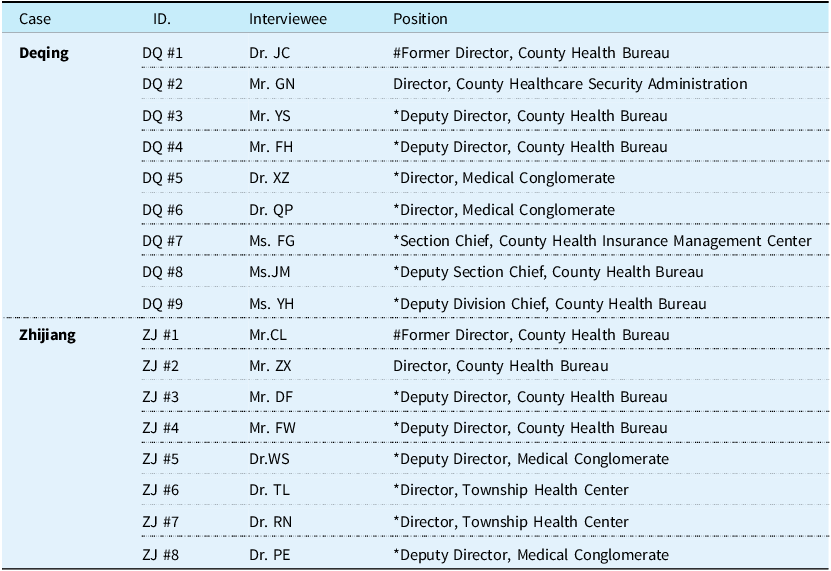
Fieldwork was conducted in mid-2023, with in-depth interviews and focus group discussions extensively used. We employed a hybrid sampling strategy, initiating with purposive sampling to identify key informants directly involved in the reform design and implementation. We then used snowball sampling to expand the participant pool, in order to capture diverse perspectives across different stakeholder groups. A total of 17 informants, including government officials, hospital managers, and health administrators, participated in either form of data collection. In both the focus group discussions and the in-depth interviews, we sought to understand the motivations of the reforms, the strategies used, and how key stakeholders interacted throughout the entire process. The profile of participants is presented in Table 2.
Profile of interviewees

Note: * conducted in the format of focused groups. # interviewed twice.
Source: the authors’ fieldwork.
One might anticipate interviews with local bureaucrats in a semi-authoritarian context to be constrained by positionality or self-censorship, potentially introducing bias. However, we found the contrary: our interviewees were remarkably outspoken, partly reflecting their entrepreneurial traits. We attribute this favourable condition to two key factors. First, the purposive and snowball sampling through trusted intermediaries generated significant social capital, fostering an environment of candour. Second, interviewing key figures on two separate occasions – in both public and private settings – served as a crucial methodological safeguard. This approach not only mitigated concerns about sensitivity but also strengthened data reliability through triangulation.
Interviews were immediately transcribed into Chinese verbatim. We then performed thematic analysis through an iterative, abductive approach, moving between empirical data and existing theoretical constructs (e.g. problem framing, policy learning, etc.). The process involved three sequential stages:
-
1. Initial coding: We first conducted open coding of the interview transcripts and documents to identify emergent themes and concepts relevant to the reform process.
-
2. Focused coding: We then developed a structured codebook around our core theoretical interests, i.e. policy entrepreneurship, based on which the initial codes were merged into broader thematic categories.
-
3. Theoretical integration: Finally, we analysed the relationships between these thematic categories to build explanations for our cases, comparing patterns within and across the two county cases to identify the causal pathways reflected in the findings.
An illustrative codebook table is exhibited in Appendix.
6. Results
6.1. The case of Deqing
Located in northern Zhejiang Province, Deqing has a peculiar geography. Its short distance from Hangzhou – the provincial capital and medical hub – aggravated the rapid outflow of patients. This situation not only created increasing payment pressure on the local SHI fund but also impeded capacity building in its health system. Desperate to attract and keep patients from the shrinking local pool, the only two major county hospitals had to engage in fierce competition for the sake of survival. The entrepreneur team was comprised of Dr JC, Director of the Health Bureau, and Mr GN, Director of the Social Security Bureau. Dr JC, a medical doctor by training, had served in multiple administrative and hospital posts at the township level, while Mr GN was a rural primary school teacher prior to his government appointment. Long service at the grassroots level gave both of them down-to-earth insights into the problems of the local health system. Dr JC’s diagnosis of the problem was as follows: ‘[township] health centers should play very important roles [in health services], but they were essentially ‘isolated islands’ in the system, totally detached from county hospitals. Weak capacity didn’t allow them to offer proper treatment. In the meantime, county hospitals were desperately competing for patients. Sometimes, they even kept patients in critical conditions who they were actually incapable of offering proper treatment to. There were clinical risks.’ [DQ #1].
The trigger of the reform was local leaders’ dissatisfaction with Deqing’s health system, which was perceived to be lagging far behind its economic prosperity. Although, practically speaking, there was no burning crisis requiring immediate action, the policy entrepreneurs – like surfers awaiting the great wave in John Kingdon’s (Reference Kingdon1984) words – skilfully recognized and seized this window of opportunity to pursue a reform. Although their respective bureaucracies (health vs. social security) were long found dissonant in their interests and vision regarding health policy reforms in China (Hsiao, Reference Hsiao2007), the same policy vision and personality yoked Dr JC and Mr GN together. Forged through consensus, this entrepreneurial coalition was further solidified by their high-level mutual trust [DQ #1, #2].
Dr JC intuitively believed that some form of vertical integration was a must, without which township health centres and county hospitals would continue to deteriorate due to small patient volume and poor capacity. Yet, they were uncertain about the exact integration design that would be suitable for Deqing. Dr JC and his team paid several field visits to other localities that were experimenting with vertical integration. He knew the critical importance of political support from local leaders and made sure that the deputy magistrate overseeing health affairs was invited to join every single visit. Active policy learning certainly inspired the policy entrepreneurs, who made creative adaptation for their own integration design.
As expected, conservatism prevailed among local leaders and health administrators, who were uncertain about the prospect of such a move. The policy entrepreneurs resorted to external experts to establish the credibility of their proposal. The enthusiastic endorsement of reputable national health policy experts relieved the concerns of local leaders, who subsequently gave the green light. Dr JC made repeated efforts to persuade health administrators, citing peer experience and expected gains for their own institutions. He was astutely aware that ‘[y]ou can’t earn their support simply by issuing official directives. You must convince them through evidence-backed sincere dialogues. Knowing informal rules is crucial too because occasionally you will have to make smart use of both ‘carrots’ and ‘sticks’.’ [DQ #1].
Given the long narrow terrain of the county, policy entrepreneurs divided its health system into an eastern cluster and a western cluster, each establishing a medical conglomerate. Officially launched in late 2016, the two conglomerates each head several township health centres that in turn connect village clinics. Both policy entrepreneurs were cognisant of the fact that the ‘siloism’ of health service delivery was in part rooted in the fragmented health governance structure. Effective integration depended on realigning the whole spectrum of incentives, which could not be done without cooperation from other bureaucracies. To break down the bureaucratic impasse, they pursued institutional consolidation by merging all health-related authorities into one single office. This bold proposal was, however, boycotted by the social security bureaucracy, which was worried about losing a chunk of its power. Moreover, there was no precedent for this type of agency consolidation at the county level. The policy entrepreneurs circumvented the deadlock through a creative detour. In 2017, they convinced the local leaders to consolidate all health-related authorities into a ‘provisional’ healthcare security office that integrated most decision-making powers, making Deqing the pioneer among Chinese counties in such health governance reform. Because the office was ‘provisional’ in nature, such practice was technically not against existing administrative rules. Importantly, agency consolidation paved the way for more coherent policy interventions.
China’s health system had been traditionally relying on FFS in paying providers, which not only contributed to rapid cost inflation (Eggleston et al., Reference Eggleston, Shen, Lau, Schmid and Chan2008; Yip et al., Reference Yip, Hsiao, Meng, Chen and Sun2010) but also made care coordination rather challenging as individual providers were driven by strong incentives to compete for patients while the actual provision of care tended to be cost-inefficient (Qian and Ramesh, Reference Qian and Ramesh2024). The entrepreneurs’ solution was a bundled annual global budget bestowed to the conglomerates that could be used as a powerful lever to coordinate the provision of care within the integrated system. The conglomerates would be placed in a stronger position to realign incentives towards coordinated care. Pre-paid on an annual lump-sum basis, the conglomerates would subsequently be motivated to reorganise care provision towards coordination and cost-efficiency because ‘they would gain a surplus if costs were reduced or lose money if they continued to overspend.’ [DQ#2].
The shift towards such prospective payment mechanisms was, however, vehemently criticised by the upper-level social security bureaucracy, which was worried about the potential loss of control over SHI funds, let alone the absence of any precedent nationwide. In a confrontation between the social security officials and the entrepreneurs, the payment reform was likened to ‘committing a crime’ [DQ#2] as it was indeed not in line with national guidelines. The policy entrepreneurs responded to such unprecedented accusations with both perseverance and issue framing. The bundled global budget was justified as a pilot in a small county of less than half a million people, so the potential risks were certainly under control. Dr JC frequently used the official narratives of the central government to justify this reform, reinforcing its political legitimacy. In his own words, ‘I always wield the ‘reform banner’ to overcome resistance’ [DQ#1]. In his rebuttal to the upper-level authorities, Mr GN resolutely remarked: ‘[h]ard reforms always need someone to make a sacrifice. We are happy to shoulder any consequences if needed.’ [DQ#2]. Operating in concert, the two reformers provided mutual support within the bounds of their respective mandates to advance the shared agenda.
Figure 2 shows the integration design in Deqing. Two conglomerates serve as the flagship providers of healthcare in the county, each with a defined catchment area within which hospitals and township health centres are interconnected through referral, coaching, and financing. The five service centres streamline management affairs in relation to human resources, primary care, finance, information, education, training, and logistics. The five resource centres consolidate all resources into a common pool. Duplicated diagnostic tests can be avoided, and the economy of scale increases the efficiency of resource utilization. A global budget is paid to the conglomerates separately based on historical records, SHI income, and cost estimation. This move away from the traditional FFS model is believed to be an effective mechanism for coordinated care and cost containment.
Organization chart of medical conglomerate in Deqing. Note: Number in parentheses indicates the number of facilities. Source: adapted from official document.

The policy entrepreneurs used every opportunity to showcase the outcomes of the reformFootnote 2 to senior officials. They approached officials in the provincial departments through both formal and informal channels. During a local site visit made by the Vice Governor, the policy entrepreneurs seized the opportunity to present the achievements of the integration reform. These achievements impressed the Vice Governor, who later invited Dr JC to the provincial taskforce for health reform design. Officiated by the Provincial Party Secretary and Governor, a high-profile onsite promotion conference was held in Deqing in 2018, signifying the high recognition of the reform. The State Council also officially commended Deqing for contributing an innovative model for national health system reform.
6.2. The case of Zhijiang
As an upper-middle income county in central Hubei Province, Zhijiang’s relatively better-off socioeconomic status was not reflected in its health system. As a result of dwindling patient volume and income, most township health centres were even struggling with paying health workers’ basic salaries. Extremely low morale and a brain drain escalated into a crisis, and many health centres were ‘at the brink of bankruptcy’ [ZJ#1, #2, #3]. Forced to take urgent measures, the health bureau embarked on a path of ‘loose integration’ in 2012. Entrusted to be the ‘custodian’ of township health centres, the county hospital sent its management team to take over day-to-day operations. Senior doctors were also stationed in the centres on a rotational basis. Such an approach led to a considerable backflow of patients, while the coaching by county doctors also improved the capacity of their township peers. This model essentially represented ‘loose integration’ as all health facilities continued to operate in isolation, without unified management or finance.
Although this ‘custodianship’ model managed to allow Zhijiang to muddle through the crisis, the fundamental problems of its health system remained as local patients continued to vote with their feet, seeking health services elsewhere. Meanwhile, perverse incentives for overprescription and other forms of waste persisted in health facilities. The cost profile of Zhijiang’s health system shown in Table 1 provides a snapshot of the situation. These dual factors resulted in a deficit in the health insurance fund in Zhijiang, igniting another crisis [ZJ#4]. The model of basic integration adopted in 2012 inspired local officials to embark on more ambitious reforms. Two medical conglomerates were launched in 2016.
The entrepreneur team consisted of Mr L, (Chinese Communist) Party Secretary of Zhijiang, and Mr CL, Director of the Health Bureau. Different from Deqing, where the conglomeration thrived in a bottom-up fashion, the Zhijiang case is clearly characterised by a top-down model as the local leaders, particularly Mr L, assumed the leading role right from the start. Yet, the dynamics within this coalition were markedly different from those manifested in the Deqing case, as the two key reformers appeared to operate primarily through hierarchy. Mr L – acting as a Poseidon-like figure (Cairney, Reference Cairney2018) who could command the very tides of local politics – provided the strategic authority and political cover necessary for bold reform. Mr CL, in turn, translated this vision into operational reality through creative administration and tactical coordination, navigating the currents set in motion.
Like their counterparts in Deqing, the policy entrepreneurs in Zhijiang also embraced active policy learning when formulating the reform blueprint. Both Mr L and Mr CL were career civil servants with limited knowledge about the health sector, so the team visited several pioneer cities, trying to garner peer experience. The final model adopted involved closely integrated conglomerates. Similar to the case of Deqing, the policy entrepreneurs knew that vertical integration of the delivery system does not necessarily lead to better care coordination or cost containment unless the provider payment mechanisms are revamped. Evidence from Tianchang, a county in neighbouring Anhui Province, indicated that a bundled global budget for medical conglomerates would create better aligned incentives for both the lead hospitals and township health centres. But again, such a ‘bold’ idea was rejected by the social security bureau. As Mr CL recalled, ‘We had many rounds of ‘fights’ with them.’ [ZJ #1]. Mr L, as the top leader of the county, firmly backed the proposal, exclaiming in a meeting ‘Tianchang is governed by the Communist Party and so is Zhijiang. What they have done can be done here too!’ [ZJ#3].
The policy entrepreneurs understood that the social security bureaucracy’s concerns were not illegitimate because most of the clinical practices in the local health system were prone to cost inflationary behaviours. As the steward of health insurance funds, the social security bureau was the ultimate party responsible for the financial safety of the funds. Mr CL and his team had persistent negotiations with them, striving to address most of their concerns. The health bureau laid down a detailed protocol of cost containment measures, including comprehensive clinical pathways, which eventually convinced the social security bureau that if paid prospectively by an annual global budget, health facilities in the conglomerates would not ‘game’ the new system with other forms of cost inflationary behaviours; rather, the new incentives created would actually encourage the cost-efficient delivery of services. The surplus left over at the end of each year would be distributed between lead hospitals, township health centres, and village clinics in a 6:3:1 ratio (ZJ#3). The new payment model was eventually introduced with the consent of the social security bureau.
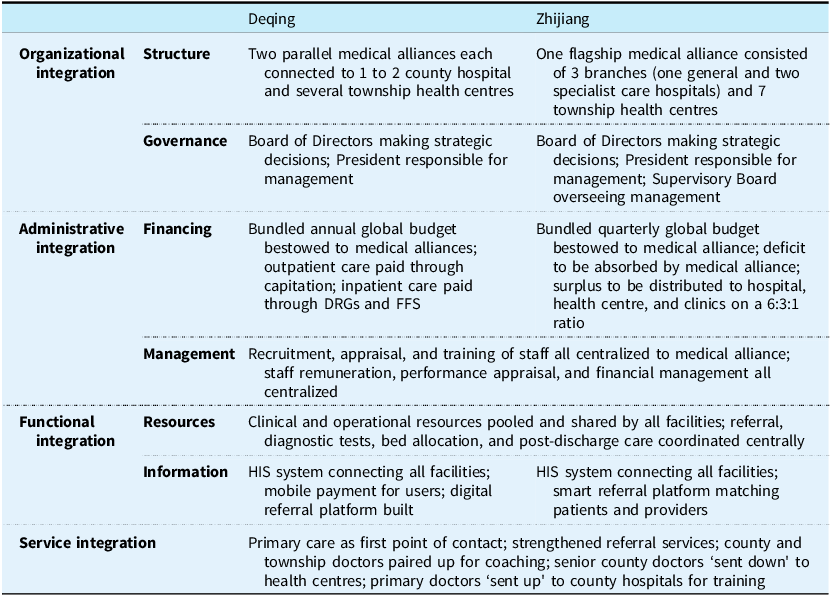
One year after the launch of the two medical conglomerates, policy entrepreneurs found that the two-conglomerate model was still not optimal because both were continuing to compete for patients from the small local pool. Given the compact geography of the county, one single conglomerate was conceived to be a more suitable model. Thus, the twin conglomerates were merged into one in 2017, with three major hospitals converted into branches of the conglomerate’s general hospital. Each of these hospitals specializes in a certain domain: general western acute care, traditional Chinese medicine, and maternal care and childcare. The finance of the three hospitals was centralized to the conglomerate so that the incentives for competition and duplication were reduced. Relieved from the pressure of unhealthy competition, the three branches can concentrate on their own specialty, providing secondary and tertiary care to all residents in the county. The general hospital directly manages township health centres, which in turn connect village clinics (see Figure 3). Similar to the practice of Deqing, Zhijiang also established a county-level diagnostic centre, allowing all facilities to share common diagnostic resources. Human resources management and finance are also centralized to the conglomerate. As compared to the two-conglomerate and ten-centre design in Deqing, the Zhijiang model is lower in functional differentiation. Government officials and health administrators maintain that such a design is most suitable for local conditions [ZJ#1, #3, #5]. A systematic comparison of the two models is presented in Table 3.
Organization chart of medical conglomerates in Zhijiang. Note: Number in parentheses indicates the number of facilities. Source: adapted from official document.

Comparison of medical conglomeration designs of the two counties

To mitigate conservatism in the bureaucracy, the policy entrepreneurs proactively sought political support from upper-level authorities. Mr L and his team paid several visits to the provincial health commission to report on their work. As Mr DF recalled: ‘It’s very rare for a local party secretary to lead such trips [to the provincial capital] according to administrative custom. Since he took the lead in communicating [with provincial authorities], it became more likely to spark chemistry and let the provincial officials recognize our reform.’ [ZJ#3]. Although the conglomeration reform lawfully fell into the scope of the county government’s autonomy, the policy entrepreneurs astutely switched the ‘maneuver venue’ to the province, attempting to create a more favourable environment. Such a strategy worked as the provincial government subsequently designated Zhijiang as the pilot of county-level health reforms. Earning such a status is very useful in the Chinese bureaucracy because it not only confers some sort of legitimacy on the reform but also helps to earn more resources. Backed by remarkable outcomesFootnote 3 , the Zhijiang model was subsequently scaled up to the rest of Hubei Province over the next few years [ZJ#1, #2].
6.3. Discussion
This study has sought to explain the development of an integrated care system in China through the perspective of policy entrepreneurship, a prominent analytical concept in policy sciences. Despite the significant value of health system integration, building such a system must overcome a variety of hurdles within the bureaucratic system. It is typically not within the disciplinary realm of health policy or health services research to examine such processual dynamics. Employing a comparative case studies method, this study investigates how entrepreneurial reformers in two Chinese counties developed the motivation to pursue a vertical integration of their respective health systems, how they designed the reform incrementally, and how they employed various strategies to get things done.
The two cases have yielded three key observations. First, located in different parts of the country, the two cases examined in this study were among the pioneer cohort of county-level medical conglomeration pilots. Notwithstanding the common pursuit of vertical integration, the momentum behind reform was considerably different in the two cases. While Zhijiang was driven by a burning crisis, the reformers in Deqing chose to initiate such a pilot even though they had neither a strong top-down mandate nor a pressing crisis. This difference manifests two distinctive pathways of subnational health policy dynamism, shaped by the interplay of collective agency and institutional context. Zhijiang’s crisis-driven pragmatism, propelled by decisive political leadership, demonstrates how perceived urgency can legitimize bolder, more directive interventions. In contrast, Deqing’s voluntary entrepreneurialism, characterised by incremental, consensus-driven adjustments, reflects a reform logic where technocratic expertise and formal mandates jointly guide local policy innovations. These diverging trajectories underline that within China’s distinctive experimentalist governance structure, which simultaneously provides both top-down mandates and local discretionary space, the specific configuration of political leadership, bureaucratic coalitions, and problem pressures conjuncturally produces meaningfully varied reform pathways.
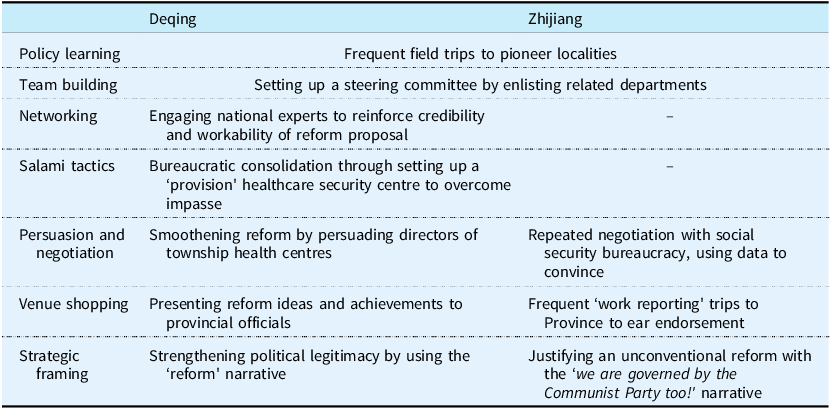
Second, both cases present clear marks of collective policy entrepreneurship in which a team of local bureaucrats worked to pursue a shared vision. The key difference between the two is that the policy entrepreneurs in Zhijiang included both a local leader and a middle-level bureaucrat, whereas their counterparts in Deqing were both technocratic entrepreneurs. The two entrepreneurial coalitions operated through hierarchy and consensus, respectively. Throughout the entire process of reform, these collective policy entrepreneurs showed remarkable entrepreneurial qualities, such as strategic thinking in the sense that a closely integrated conglomerate was conceived to be a good solution to the longstanding problems of the local health system, as well as tenacity that drove them through multiple sources of resistance. Summarized in Table 4, the various entrepreneurial strategies used by the policy entrepreneurs helped them develop their innovative ideas, amass support, and overcome challenges. Policy entrepreneurs in both cases extensively used policy learning in developing and fine-tuning their integration designs, again highlighting the existence of frequent peer learning as a powerful catalyst of policy innovations (He et al., Reference He, Fan and Su2022; Husain, Reference Husain2017). Setting up a steering committee by enlisting related departments appears to be the standard protocol of policy reforms in China, and such practice is seen in both cases. Additionally, we observed noticeable differences in their use of other entrepreneurial strategies, such as venue shopping, framing, and persuasion. Such differences are shaped not only by the traits of individual actors but also by their respective reform trajectories. For instance, employing a classic salami tactic – the strategy of advancing a major goal through a series of incremental, seemingly modest steps (Zahariadis, Reference Zahariadis2003) – the policy entrepreneurs in Deqing successfully ‘co-opted’ the social security bureaucracy, thereby facilitating the implementation of the global budget payment. In comparison, policy entrepreneurs in Zhijiang had repeated negotiations with the social security bureaucracy, extensively using data to convince them of the workability of the global budget payment.
Entrepreneurial strategies used in the two reforms

Source: summarized by the authors based on fieldwork.
Third, the two counties differed substantially in their reform trajectories. The policy entrepreneurs in Deqing adopted salami tactics by establishing a ‘provisional’ healthcare security centre to consolidate bureaucratic power within the county government before initiating the provider payment reform. Such a strategy was highly intelligent because it smoothed the payment reform process which would otherwise have been much harder due to interdepartmental negotiations, as seen in the case of Zhijiang. In comparison, Zhijiang essentially underwent three episodes of integration reforms: the ‘custodian’ model in 2012, the two-conglomerate model in 2016, and the one-conglomerate model in 2017. The one-conglomerate three-branch model that was eventually adopted in 2017 represents both vertical integration among three tiers of the delivery pyramid and horizontal integration between clinical specialties. Such a trajectory embodies active trial-and-error efforts and continuous adaptation. The two distinctive integration designs are reflective of the varying local conditions.
When examining these two cases from a broader political economy perspective, it must be noted that county level is the relatively low echelon in China’s titanic bureaucracy and the integration of county-level health system well falls into the autonomy of county governments. Given its low political sensitivity, such medical conglomeration initiatives are typically within the ‘safe zone’ of local government innovations where bureaucratic entrepreneurship becomes not only possible but also vibrant. We maintain that such a combination of low political sensitivity and high administrative autonomy constitutes the boundary conditions for the type of policy entrepreneurship as revealed in this study.
7. Concluding remarks
Health system integration has been advocated for more than a decade, yielding various models worldwide (Toth, Reference Toth2020). A prominent model flourishing in China is county-level medical conglomerates that integrate tertiary, secondary, and primary care through organizational restructuring. A high degree of integration is achieved through resource sharing, unified finance, centralized governance, streamlined service delivery, and a common information infrastructure. Importantly, the bundled global budget gives a medical conglomerate a powerful lever to align the financial incentives of individual provider units within the conglomerate. In the past few years, such a closely integrated model has been rapidly scaled up in China from several pioneer counties (Wang et al., Reference Wang, Yang, Zheng and Yuan2024). As reiterated by the Minister of Health, county-level medical conglomerates represent one of the key health system reform strategies to be adopted in China in the years to come.
The implications of this study for other middle- and low-income countries are threefold. First, vertical integration represents a promising model for health systems afflicted by fragmentation and weakened primary care, but the path toward such a goal is associated with significant complexities, requiring active learning, trial and error, and adaptation. It took China more than a decade to experiment with various pilot models, most of which thrived in a bottom-up fashion, allowing the central government to compare and synthesize. This active subnational experimentation has provided fertile ground for the medical conglomeration innovations to emerge and eventually be recognized by national policymakers. Therefore, a framework of conducive intergovernmental relations, combined with versatile policy piloting and learning, is a pivotal institutional structure for health system innovations in multilevel governance systems.
Second, no policy reforms can happen without active human agency (Mintrom and Norman, Reference Mintrom and Norman2009). This study, together with other cases from the health sector, highlights the critical importance of policy entrepreneurs in catalysing innovations (He, Reference He2018; Oborn et al., Reference Oborn, Barrett and Exworthy2011). We do believe that context matters in the actual manifestation of health policy entrepreneurship, but many of the entrepreneurial strategies revealed in this study – such as venue shopping, framing, team building, and policy learning – represent general tactics that health policy reformers in other contexts can also pursue.
Third, the actual technical design of integration requires full consideration of local conditions and defies a ‘one-off’ solution. Continuous fine-tuning is vital. As Tsiachristas et al. (Reference Tsiachristas, Vrangbæk, Gongora-Salazar and Kristensen2023) rightly pointed out, financing and delivery models of predispose health systems to fragmentation and therefore a customized approach is needed to any integration reforms. The cases from China suggest that in health systems with a strong SHI presence, a bundled global budget may present a useful tool to combine with organizational structuring.
This study has adopted an explanatory rather than normative stance in analysis. We recognize that such systemic integration reforms may entail inherent trade-offs, presenting both the potential for coordinated efficiency and the risks of monopolistic power, bureaucratic interference, and diminished frontline autonomy. The precise outcomes, however, must be subject to rigorous evaluation that is beyond the scope of this current study.
This study is certainly not without limitations. It explicitly focuses on the policy formulation and early implementation process, which led us to prioritize interviewing the key architects and managerial stakeholders of the reforms. While we gathered frontline perspectives from administrative officials of health facilities, we acknowledge that the relative lack of direct voices from grassroots health workers and patients is a limitation. Furthermore, while this study has illuminated the distinct entrepreneurial pathways that enabled health system integration in two pioneering counties, it also surfaces a critical, forward-looking question: through what mechanisms are such local innovations scaled to inform provincial and possibly national policy in China’s hybrid governance regime? Analysing these scaling dynamics is the next step plan in our research agenda.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1744133126100516.
Acknowledgements
The authors are grateful to all individuals who facilitated the fieldwork. The research assistance provided by Muyu He is appreciated. Highly useful comments from two anonymous reviewers are thankfully acknowledged.
Financial support
This study was funded by the General Research Fund (Ref. 18621522) of the Research Grants Council of Hong Kong.
Competing interests
None declared.
Author contributions
AJH: conception of the work; data collection; data analysis and interpretation; drafting the article.
MJL: data collection; data analysis and interpretation.
XTL: conception of the work; data collection.
NT: conception of the work; data collection.
Ethical standards
Ethical clearance was granted by The Hong Kong University of Science and Technology.






 Open access
Open access