



Impact statement
This study explored the reasons why people with depression in Nepal struggle to access mental healthcare, despite efforts to integrate mental health services into the existing healthcare system. By examining barriers related to service availability and individual willingness to seek help, the study established how systemic issues within the healthcare system intersect with community beliefs, economic challenges and geographical constraints. The findings underscore that accessing mental health services in Nepal remains challenging due to various factors, including limited resources, inadequate staffing, inconsistent medication availability, as well as stigma, cultural beliefs and practices and a lack of awareness regarding where and when to seek support. Many individuals experienced barriers such as long travel distances, financial burdens and uncertainty about service availability in the nearby health facilities. Additionally, healthcare providers face obstacles like insufficient infrastructure, heavy workloads and limited support for delivering mental healthcare. The study contributes to the global mental health discourse by emphasizing that simply expanding services is insufficient to bridge the treatment gap. Effective mental healthcare requires strategies that bolster healthcare systems while addressing social, cultural and economic influences on help-seeking behavior. It highlights the importance of coordinated approaches involving community engagement, stigma reduction, culturally sensitive communication, improved supply chains and enhanced workforce capacity. By identifying these interconnected barriers and opportunities, the study offers practical insights to guide more effective and contextually relevant mental health policies and programs in Nepal and similar settings.
Introduction
Despite global efforts to integrate mental health services into primary healthcare (PHC) systems, the treatment gap for mental health remains substantial, particularly in low- and middle-income countries (LMICs) (Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana and Bolton2018; Petersen et al., Reference Petersen, van Rensburg, Kigozi, Semrau, Hanlon and Abdulmalik2019; Raviola et al., Reference Raviola, Naslund, Smith and Patel2019). The World Health Organization (WHO) launched the Mental Health Gap Action Programme (mhGAP) Intervention Guide in 2010 to help with integration into primary care (WHO, 2010). While mhGAP has been implemented in over 100 countries (WHO, 2016), many individuals still do not receive treatment for common mental disorders like anxiety and mood disorders (Graham et al., Reference Graham, Hasking, Brooker, Clarke and Meadows2017; Evans-Lacko et al., Reference Evans-Lacko, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Benjet and Bruffaerts2018). Patients with mood disorders often wait between 1 and 14 years for care, while those with anxiety disorders wait 3 to 30 years (Wang et al., Reference Wang, Angermeyer, Borges, Bruffaerts and Tat Chiu2007). These delays can increase health risks, reduce medication effectiveness and lower treatment success rates (Altamura et al., Reference Altamura, Santini, Salvadori and Mundo2005, Reference Altamura, Dell’osso, D’Urso, Russo, Fumagalli and Mundo2008; de Diego-Adeliño et al., Reference de Diego-Adeliño, Portella, Puigdemont, Pérez-Egea, Alvarez and Pérez2010; Penninx et al., Reference Penninx, Nolen, Lamers, Zitman, Smit and Spinhoven2011; Bukh et al., Reference Bukh, Bock, Vinberg and Kessing2013).
Access to healthcare is a multifaceted concept that involves individuals’ ability to obtain and utilize health services effectively (Gulliford et al., Reference Gulliford, Figueroa-Munoz, Morgan, Hughes, Gibson, Beech and Hudson2002). Penchansky and Thomas define access as the alignment between patients and the health system, encompassing five dimensions: availability, accessibility, accommodation, affordability and acceptability (Penchansky and Thomas, Reference Penchansky and Thomas1981). Andersen emphasizes actual service use and factors at individual, societal and system levels (Andersen, Reference Andersen1995). Levesque, Harris and Russell expand on these models, defining access as a dynamic process shaped by health system characteristics and individual abilities (Levesque et al., Reference Levesque, Harris and Russell2013). Their framework identifies dimensions such as approachability, acceptability, availability, accommodation, affordability and appropriateness paired with individuals’ abilities to perceive, seek, reach, pay and engage.
Global initiatives often focus on addressing supply-side barriers, such as increasing service availability and workforce capacity through task-sharing approaches (Endale et al., Reference Endale, Qureshi, Ryan, Esponda, Verhey and Eaton2020; Keynejad et al., Reference Keynejad, Spagnolo and Thornicroft2021; Dumke et al., Reference Dumke, Wilker, Hecker and Neuner2024). However, research suggests that solely expanding services may not effectively reduce the treatment gap (Evans-Lacko et al., Reference Evans-Lacko, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Benjet and Bruffaerts2018; Fekadu et al., Reference Fekadu, Demissie, Birhane, Medhin, Bitew and Hailemariam2022). Barriers to mental healthcare are often oversimplified by combining demand- and supply-side factors. To effectively tackle this issue, it is crucial to differentiate between demand-side barriers and supply-side challenges and develop targeted strategies for each. For instance, public education and anti-stigma campaigns can increase willingness to seek care, while culturally sensitive interventions can enhance service delivery. Without this dual approach, investments in infrastructure and workforce may not lead to improved access and utilization, perpetuating global mental healthcare disparities (Troup et al., Reference Troup, Fuhr, Woodward, Sondorp and Roberts2021; Bilican et al., Reference Bilican, Irfan, Cox, Salaets, Sabbe and Schoenmakers2025). This study aims to explore multi-stakeholder perceptions and experiences regarding barriers to accessing mental health services in Nepal. The results are analyzed using Levesque et al.’s access framework (Levesque et al., Reference Levesque, Harris and Russell2013), which considers both individuals’ ability to seek care and health system-level barriers.
Methods
Setting
Nepal is a low- and middle-income country in South Asia with a population of approximately 29.1 million and an annual growth rate of 0.92% (National Statistics Office, 2023). It is diverse in terms of caste/ethnicity and languages, with 142 caste ethnicities and 124 languages (National Statistics Office, 2023). The country adopted a federal governance system in 2015, establishing 7 provinces, 77 districts and 753 local units. This study was conducted in three districts, Jhapa, Chitwan and Kailali, selected for their diverse populations in terms of caste/ethnicity, language and healthcare delivery contexts (Lynn et al., Reference Lynn, Dahal and Govindasamy2008). Nepal’s healthcare system comprises public, private and non-governmental sectors, with specialized mental health services remaining scarce (Luitel et al., Reference Luitel, Jordans, Adhikari, Upadhaya, Hanlon, Lund and Komproe2015; Mahat et al., Reference Mahat, Citrin and Bista2018; Rai et al., Reference Rai, Gurung and Gautam2021). Local governments deliver primary healthcare services through PHC facilities including, health posts, primary healthcare centers and hospitals. Community-based mental health services have been introduced using a task-sharing approach in collaboration with NGOs, and PHC workers in these districts have received WHO mhGAP training (Paudel et al., Reference Paudel, Chalise, Khatri, Poudel and Khanal2025).
Study design
We conducted in-depth individual interviews (IDIs), a qualitative method ideal for exploring personal experiences and perspectives. The interviews were semi-structured with tailored guidelines for different participant groups. Community stakeholders such as teachers, traditional healers, female community health volunteers (FCHVs) and political leaders were presented with a narrative vignette depicting a person with depression to gather their views on help-seeking practices and perceived barriers. For individuals undergoing treatment for depression or anxiety, the interviews centered on their personal experiences and pathways to care.
Participants and recruitment
The study was conducted with people receiving treatment for depression or anxiety (24), their family members (9), PHC providers (10), traditional healers (12), FCHVs, teachers and political leaders (10). Purposive sampling was used to ensure diversity in roles and experiences. Inclusion criteria were: (i) relevant role (patient, caregiver or provider), (ii) ability to communicate in Nepali, and (iii) willingness to share experiences. PHC workers and FCHVs were selected for their role in mental healthcare, while traditional healers were included to capture culturally embedded practices.
Interview guides
Separate guides were developed for each participant group. Guides for individuals and families were adapted from the McGill Illness Narrative Interview (MINI), a semi-structured protocol for exploring illness experiences (Groleau et al., Reference Groleau, Young and Kirmayer2006; Craig et al., Reference Craig, Chase and Lama2010). A vignette-based approach was used for community members to explore perceptions of depression, help-seeking pathways and available resources (Subba et al., Reference Subba, Luitel, Kohrt and Jordans2017). PHC workers were asked about diagnostic practices, treatment approaches and interactions with patients.
Interview process
Two trained researchers conducted all interviews in private settings chosen by participants to ensure comfort and confidentiality. Prior to interviews, participants received detailed information about study objectives, benefits and risks, and provided written informed consent. In adherence to the principle of non-maleficence, participants undergoing treatment for depression or anxiety were recruited through PHC workers or mental health professionals to prevent unnecessary disclosure or distress. Interviews were conducted either at participants’ homes or in a private clinical setting based on their preference to ensure their comfort and confidentiality. PHC workers were interviewed in outpatient departments during working hours. Family members were interviewed privately at home. Traditional healers were interviewed at their residences or service locations, and other community stakeholders at their workplaces. Interviewers were trained to handle discussions sensitively, and participants were informed of their right to pause, skip questions or withdraw at any point without impacting their care. Strict measures were in place to maintain privacy and confidentiality throughout the study. Participants experiencing psychological distress during the interview were offered free psychosocial support from trained counselors in their locality. Participants disclosing suicidal ideation were immediately connected with psychosocial support services. The management of suicidal ideation and other risks followed the Adverse Event Reporting and Management protocol (Singh et al., Reference Singh, Chhetri, Khanal, Maharjan, Garman and Jordans2025). Data collection occurred between January and July 2023.
Data management and analysis
Interviews were audio-recorded and transcribed immediately after each session. Professional translators translated the Nepali transcripts into English, and the first author reviewed translations for accuracy. Two researchers independently coded transcripts using NVivo 20 (QSR International). A hybrid inductive–deductive approach guided coding, informed by study objectives and emergent themes (Creswell and Poth, Reference Creswell and Poth2018). Thematic analysis was structured using the access framework by Levesque and colleagues (Levesque et al., Reference Levesque, Harris and Russell2013), which conceptualizes access as the interaction between health system characteristics (approachability, acceptability, availability/accommodation, affordability, appropriateness) and individual abilities (perceive, seek, reach, pay, engage). Certain findings were relevant to both demand- and supply-side barriers, as well as to different domains within either the demand or supply barriers. In these cases, the assignment of specific findings to multiple domains was decided through collaborative discussion and agreement between the first author and the research team.
Results
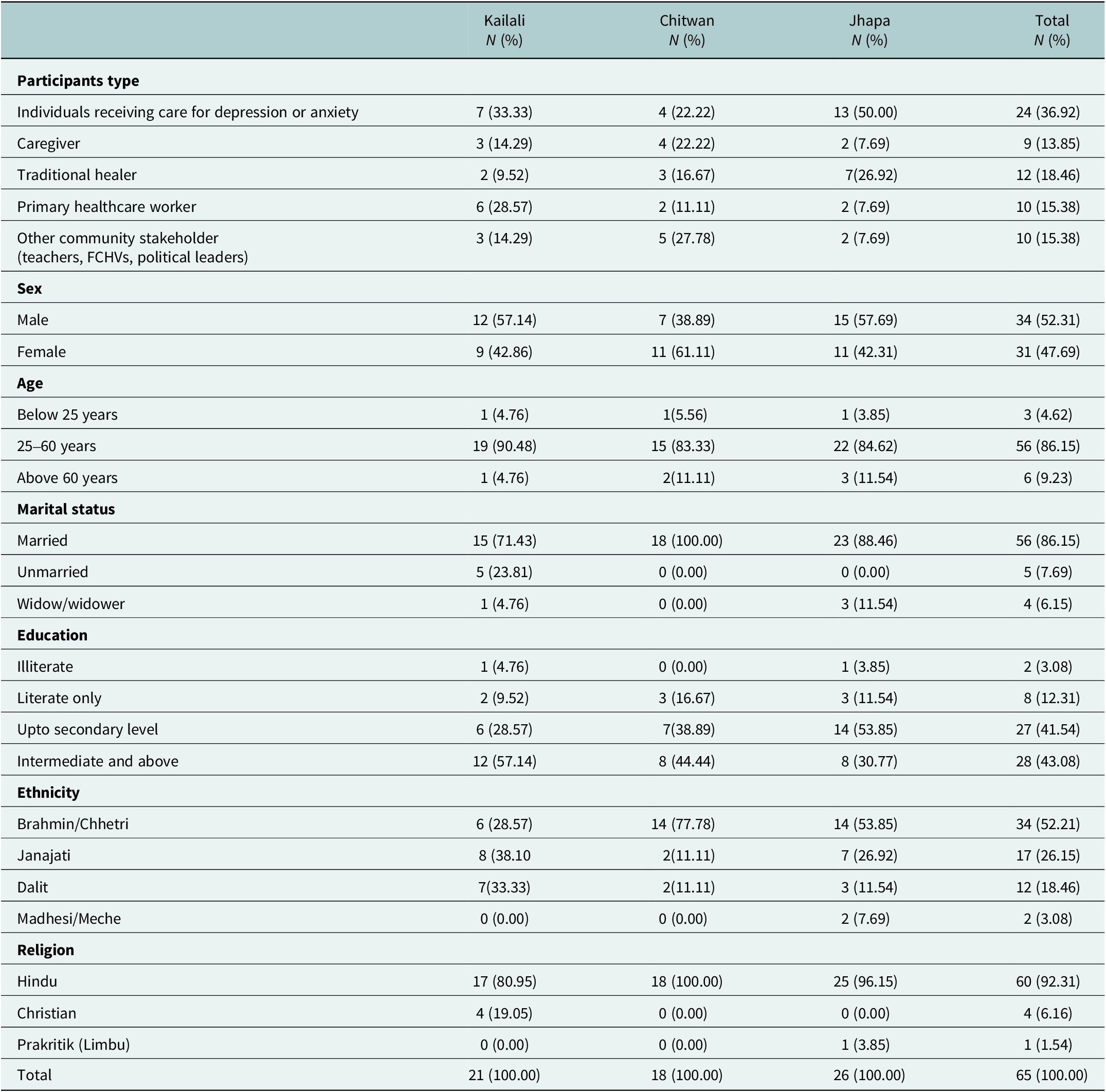
Table 1 presents the socio-demographic characteristics of the study participants. Of the participants, 37% were undergoing treatment for depression or anxiety, 18.5% were traditional healers and 15% were PHC workers. A majority of the participants were female (52%), aged between 25 and 60 years (86%), married (86%) and had completed up to a secondary level of education (41.5%). The largest percentage of participants belonged to the Brahmin/Chhetri caste (52%), followed by Janajati (26%). The majority of participants were identified as Hindu. Among the participants, 40% were from Jhapa, 32% from Kailali and 28% from Chitwan.
Socio-demographic characteristics of the participants

Table 1. Long description
The table is organized by row groups for participant type, sex, age, marital status, education, ethnicity, and religion. Each group contains subcategories listed in the first column. For each subcategory, counts and percentages are provided for Kailali, Chitwan, Jhapa, and the total. For participant type, individuals receiving care for depression or anxiety are 7 (33.33 percent) in Kailali, 4 (22.22 percent) in Chitwan, 13 (50.00 percent) in Jhapa, total 24 (36.92 percent). Caregivers are 3 (14.29 percent), 4 (22.22 percent), 2 (7.69 percent), total 9 (13.85 percent). Traditional healers are 2 (9.52 percent), 3 (16.67 percent), 7 (26.92 percent), total 12 (18.46 percent). Primary healthcare workers are 6 (28.57 percent), 2 (11.11 percent), 2 (7.69 percent), total 10 (15.38 percent). Other community stakeholders are 3 (14.29 percent), 5 (27.78 percent), 2 (7.69 percent), total 10 (15.38 percent). For sex, males are 12 (57.14 percent), 7 (38.89 percent), 15 (57.69 percent), total 34 (52.31 percent); females are 9 (42.86 percent), 11 (61.11 percent), 11 (42.31 percent), total 31 (47.69 percent). For age, below 25 years are 1 (4.76 percent), 1 (5.56 percent), 1 (3.85 percent), total 3 (4.62 percent); 25–60 years are 19 (90.48 percent), 15 (83.33 percent), 22 (84.62 percent), total 56 (86.15 percent); above 60 years are 1 (4.76 percent), 2 (11.11 percent), 3 (11.54 percent), total 6 (9.23 percent). For marital status, married are 15 (71.43 percent), 18 (100.00 percent), 23 (88.46 percent), total 56 (86.15 percent); unmarried are 5 (23.81 percent), 0 (0.00 percent), 0 (0.00 percent), total 5 (7.69 percent); widows are 1 (4.76 percent), 0 (0.00 percent), 3 (11.54 percent), total 9 (13.85 percent). For education, illiterate are 1 (4.76 percent), 0 (0.00 percent), 1 (3.85 percent), total 2 (3.08 percent); literate only are 2 (9.52 percent), 3 (16.67 percent), 3 (11.54 percent), total 8 (12.31 percent); up to secondary level are 6 (28.57 percent), 7 (38.89 percent), 14 (53.85 percent), total 27 (41.54 percent); intermediate and above are 12 (57.14 percent), 8 (44.44 percent), 8 (30.77 percent), total 28 (43.08 percent). For ethnicity, Brahmin/Chhetri are 6 (28.57 percent), 14 (77.78 percent), 14 (53.85 percent), total 34 (52.21 percent); Janajati are 8 (38.10 percent), 2 (11.11 percent), 7 (26.92 percent), total 17 (26.15 percent); Dalit are 7 (33.33 percent), 2 (11.11 percent), 3 (11.54 percent), total 12 (18.46 percent); Madhesi/Meche are 0 (0.00 percent), 0 (0.00 percent), 2 (7.69 percent), total 2 (3.08 percent). For religion, Hindu are 17 (80.95 percent), 18 (100.00 percent), 25 (96.15 percent), total 60 (92.31 percent); Christianity are 4 (19.05 percent), 0 (0.00 percent), 0 (0.00 percent), total 4 (6.16 percent); Prakritik (Limbu) are 0 (0.00 percent), 0 (0.00 percent), 1 (3.85 percent), total 1 (1.54 percent). The final row shows total participants: 21 (100.00 percent) in Kailali, 18 (100.00 percent) in Chitwan, 26 (100.00 percent) in Jhapa, total 65 (100.00 percent).
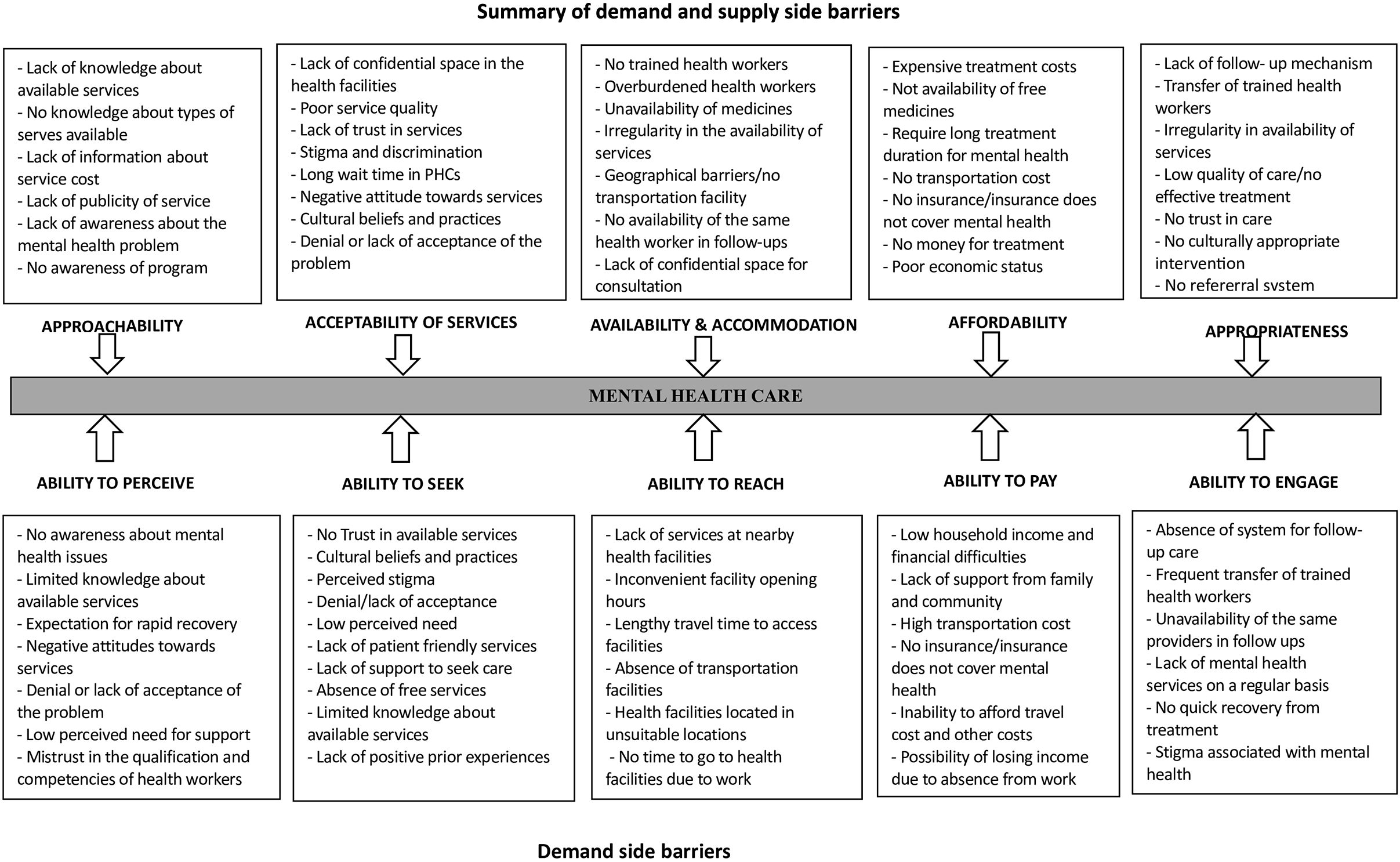
The barriers reported in the study are summarized in Figure 1 using the framework developed by Levesque and colleagues (Levesque et al., Reference Levesque, Harris and Russell2013). This framework comprises five supply-side barriers: approachability, acceptability of problems and services, availability and accommodation, affordability and appropriateness. It also includes five corresponding demand-side barriers related to perception, seeking, access, payment and engagement.
Summary of the demand- and supply side barriers.

Figure 1. Long description
From left to right, the flowchart is divided into five vertical columns: approachability, acceptability of services, availability and accommodation, affordability, and appropriateness. Each column contains two stacked boxes. The top box in each column lists supply side barriers, such as lack of knowledge about available services, lack of confidential space, no trained health workers, expensive treatment costs, and lack of follow-up mechanisms. The bottom box in each column lists demand side barriers, including no awareness about mental health issues, no trust in available services, lack of services at nearby facilities, low household income, and absence of follow-up care. Arrows connect each barrier type to a central horizontal bar labeled mental health care, which is itself divided into five segments corresponding to the five dimensions. Each segment is labeled with the associated ability: ability to perceive, ability to seek, ability to reach, ability to pay, and ability to engage. The diagram visually aligns supply and demand barriers with their respective dimensions of access to mental health care.
Supply-side barriers
Participants identified a range of supply-side barriers across approachability, acceptability, availability and accommodation, affordability and appropriateness that collectively hindered timely and continuous mental healthcare. These barriers often interacted: limited visibility and stigma reduced initial engagement; organizational and logistical constraints disrupted continuity; financial barriers undermined treatment persistence; and gaps in provider capacity, referral systems and follow-up compromised care quality.
Approachability of services
Approachability refers to how easily services can be identified and their benefits recognized. It was constrained by limited outreach and low visibility of mental health services relative to physical health programs. FCHVs reported that mental health remained a low-priority topic, reducing community awareness and proactive help-seeking. In such contexts, many community members turned to FCHVs rather than health-post staff.
The staff at the health post keep changing and come from different places. Honestly, people trust us more than the health post staff. KPBL_11
Lack of family knowledge also emerged as a major barrier, often delaying recognition of symptoms and timely access to care. One woman from Chitwan described feeling unsupported and unsure where to seek help.
If someone had informed me, I would have sought treatment earlier. No one in my family understands mental illness or guided me. PABL_11
Education level further influenced help-seeking. A health worker from Jhapa noted that individuals with more education were more likely to recognize problems and seek treatment promptly.
Educated individuals seek treatment and start medication faster. Uneducated individuals often delay. Mental illness affects both groups differently. HWBL_22
Acceptability of problems and services
Acceptability, shaped by socio-cultural norms, stigma and confidentiality concerns, was a prominent barrier. Participants described how fear of recognition and disclosure discouraged facility attendance.
When someone goes to the health post, all the staff know their condition. People worry they might tell others, so they hesitate to go. KPBL_11
PHC workers highlighted that crowded out-patient departments and the lack of private rooms hindered trust-building and open communication.
If patients don’t talk openly, it’s difficult to help them. We try to earn trust, but in OPD they rarely share their history immediately. With many patients waiting, we rush, and they avoid returning. HWBL_03
Traditional beliefs attributing distress to supernatural causes further discouraged biomedical care.
I doubt medicine will help. I think my condition may be due to ghosts, curses, or black magic, so I only consider medicine in extreme cases. PAPS_01
Preference for traditional healers reinforced delays.
I also believed in superstitions, thinking my nighttime fears caused my illness. These beliefs prevent people from getting proper treatment. People need to trust science over superstition. PABL_02
Availability and accommodation
Availability and accommodation reflecting organization, staffing, infrastructure and logistics were widely cited constraints. Participants described stock-outs of free medications, frequent staff transfers, inadequately equipped facilities, crowded outpatient departments, limited confidential spaces and geographical barriers. Stock-outs particularly frustrated patients expecting free medicines at public facilities.
Patients go where they can get medicines. Just yesterday, one woman said, “we go to government facilities but don’t get medicines, so we end up buying them privately”. HWBL_03
Human resources were insufficient for demand, and frequent rotation of trained providers disrupted continuity and trust.
My colleagues aren’t trained in mental health. They need my advice even after seeing patients because I’m the only trained prescriber. HWPS_11
Lack of private consultation rooms limited open disclosure.
They feel hesitant. They may meet neighbors at the facility and don’t feel safe. There’s no separate department or room, so they can’t share everything. I’ve seen this often. HWBL_04
Overcrowding and overworked staff led to rushed consultations, discouraging return visits.
The doctor had many patients and came only once every 1–2 months. There were over 200 patients; we were seen at midnight. The consultation was rushed—just a few questions, no proper counseling. PABL_24
Limited awareness of mental health services in primary care led some individuals to seek treatment outside Nepal.
I didn’t know mental health services were available in Nepal. My friend and I went to India because he also didn’t know he could get treatment from primary health workers. PAPS_01
Affordability of services
Affordability constraints, including medicine costs, travel expenses and inconsistent insurance coverage – compromised treatment initiation and adherence. Health workers described how the lack of free psychotropic medicines in public facilities forced patients to rely on out-of-pocket purchases over long periods, often leading to treatment discontinuation.
He [patient] has to take medicine regularly. He said he could buy it once or twice, but buying it every time is difficult. HWPS_11
Traditional healers were viewed as more affordable, influencing care-seeking pathways.
People avoid doctors thinking it will cost a lot. Going to a traditional healer cost much less… Poor people cannot afford a doctor. KPBL_21
Travel costs further restricted follow-up and continuity.
I was advised to go to Kathmandu or Nepalgunj for possible neurological illness, but I couldn’t afford the travel. Kailali has no neurological doctors, so finances limited my access to specialized care. PAPS_08
Insurance gaps added to these affordability barriers, with inconsistent availability of mental health services in government hospitals and many private hospitals not accepting insurance.
Most government hospitals accept insurance, but many private ones, including the hospital I visited, don’t. I’m also not aware which government hospitals provide mental health services. PABL_24
Supply-side financing and procurement issues further contributed to medicine shortages.
There may be a dozen free mental health medicines, but they don’t reach our center. Local governments now manage purchases, but they haven’t consulted us. HWBL_22
Appropriateness of services
Appropriateness covering fit, quality, continuity and timeliness was weakened by perceived gaps in provider’s competence, inconsistent service delivery and management limitations. Some patients questioned professionalism and clinical quality.
When I shared my symptoms, he kept asking questions, writing, and calling his superior to ask what to do. Sometimes he looked at his phone. I didn’t feel confident; he seemed too young and inexperienced. PABL_42
PHC workers described how few trained service providers led to heavy workloads, delays and limited follow-up.
The lack of proper management, few trained staff, and inadequate lab facilities may be the reason. People also don’t come for follow-up on their own. HWPS_11
Frequent staff transfers disrupted continuity, leaving gaps when trained personnel moved away.
We sent one staff for training in Dadeldhura, but he was transferred soon after. If a trained worker stays, services improve, but once they leave, quality drops. HWBL_03
Medication supply issues such as delayed delivery, limited stock and short-expiry medicines further undermined care.
When we ask the municipality about mental health medicines, they say the province purchases them. But the medicines often arrive with only six months’ expiry left… and we must discard them after that. HWBL_11
Participants emphasized the lack of structured follow-up and referral systems, leading to discontinuities, mistrust and severe outcomes.
There was a postpartum depression case. I suspected a mental health issue and informed the nurses. We provided counseling, but while trying to link her to a doctor, she committed suicide. This happened because we lack a proper referral mechanism. We can diagnose cases, but without a system to connect them to treatment, we face serious challenges. HWBL_22
Demand side barriers
Demand-side barriers encompass five dimensions: perception, seeking, access, affordability and engagement, hindering the consistent utilization of mental health services. These barriers are rooted in socio-cultural norms, financial constraints and systemic shortcomings, leading to delays, gaps and distrust in the healthcare system.
Ability to perceive
The ability to perceive refers to individuals’ capacity to recognize mental health needs and the importance of care. Cultural beliefs, stigma and low perceived need were major obstacles. A strong reliance on traditional practices and superstitions often delayed or prevented professional care:
I, too, have faith in superstitions. This dependence on superstitions can prevent individuals from seeking appropriate medical treatment. These beliefs have been handed down through generations and greatly influence our healthcare choices. PABL_02
Traditional healers also reported that many individuals consult them before visiting hospitals.
In the past, it was common to seek the help of traditional healers (Dhami-jhakri) and have faith in their healing abilities. This tradition continues today, as people still visit traditional healers and perform rituals before seeking medical treatment at hospitals. KPBL_41
Stigma and discrimination further shaped perceptions, discouraging help-seeking. Patients feared being labeled “mad” and concealed their illness.
I lied to the villagers, telling them I was taking medicine for headaches to avoid negative judgment. Nobody wants to be labeled as mad. PABL_42
Low perceived need was another barrier. Many patients delayed treatments until symptoms became severe.
Mostly I go to the hospital only when it becomes very difficult, otherwise I go when my medicines are finished. If the pain is tolerable, then I do not go to the hospital. PABL_11
Denial of illness was repeatedly cited as a major barrier, contributing to delayed treatment and dropout cases.
First of all, none of the mental health patients ever feel that they have a mental health illness or that they have a mental health problem. They never accept this fact. HWBL_03
Lack of awareness about mental health was pervasive. Patients often misunderstood symptoms, assuming physical causes such as heart problems and sought treatment accordingly.
If someone has depression, they are usually unaware of it. They start visiting doctors thinking they have heart issues. HWBL_21
Patients themselves echoed this struggle of a lack of awareness about mental health issues.
I didn’t understand what was happening to me or what I should do. I never imagined I would go through this. PABL_11
Ability to seek
The ability to seek reflects individuals’ capacity to identify and choose appropriate services. Participants mentioned barriers such as frequent staff turnover, lack of private spaces, poor facility conditions, distrust in services and stigma. The absence of privacy made individuals hesitant to disclose information.
They feel reluctant… There is no secure and separate area or room; they are unable to share all their information. HWBL_04
Patients with depression found crowded and noisy facilities stressful.
They couldn’t manage to go to the hospital alone… It would only increase their stress if they went alone. The hospital is noisy and crowded, adding to their stress. CGPS_12
Participants also highlighted stigma and misconceptions, which hindered help-seeking.
In rural areas, many conceal mental health issues out of fear of being labeled as ’crazy’ or ’half-brained.’ They seek help from traditional healers for problems like insomnia, attributing it to divine displeasure. KPPS_01
Ability to reach
Ability to reach refers to individuals’ capacity to physically access services. Geographic barriers – such as long distances, poor road conditions and limited transportation were among the most frequently cited challenges. Health workers noted that long travel distances discourage patients from visiting health facilities. Unpaved roads and lengthy travel times make regular visits inconvenient.
We still have challenges, as the roads are not all paved, and the patients have to travel on foot till here, which takes a long time. HWBL_05
Several participants reported that traveling to India was easier than reaching Kathmandu.
Lucknow is near… it takes only five hours. To reach Kathmandu from here, it takes 18–22 hours. Distance is also the reason they go to India… and it is easily accessible. HWBL_06
Patients from Kailali noted that treatment in India is considered more accessible, affordable and technologically advanced.
India is close to here, and when comparing, it’s also cheaper than Kathmandu. Traveling back and forth is easier. PABL_05
Ability to pay
Financial constraints were a major barrier to maintaining treatment. The lack of free medicines, high travel costs and insufficient family support often resulted in treatment discontinuation. Family financial difficulties compounded these issues.
When I went for a check-up for my depression, my husband and mother-in-law refused to give me money… I couldn’t go to the follow-up because I didn’t have the money and I also had to discontinue the medication. PAPS_04
Even when families were willing to provide support, secrecy surrounding illness made it difficult for patients to ask for help.
It should be free. Even if I have to pay for the medicine, I ought to take it. So, I lie to my son, I lie to my daughter-in-law and tell them, ‘I have to go somewhere today. Please give me money for the bus fare.’ And from that money, I buy my medicine. PABL_12
Traditional healers observed that financial hardship drives patients toward more affordable traditional practices.
Patients don’t go to doctors thinking it will cost a lot. Visiting a traditional healer (dhami) is cheap. If the healer can cure them, why face trouble at the hospital? Poor people can’t afford doctors; that’s why they go to healers. KPBL_21
Ability to engage
Ability to engage refers to individuals’ motivation and capacity to participate in decision-making and remain committed to treatment. Major barriers included mistrust in services, financial constraints, geographical challenges and systemic issues. Participants frequently reported doubts about health workers’ competence, particularly when diagnoses were unclear or poorly communicated, leaving them uncertain about their medications.
When I first started taking the medicine… I came across a similar one used for depression. Then doubts came to my mind, like whether this medicine will harm me or whether they are concealing my real condition. PABL_02
Frequent transfers of PHC workers disrupted continuity of care and discouraged follow-up, compounded by limited trained staff and lack of refresher training.
Some health workers were transferred or promoted… Seeing different staff at each visit made the process less reliable and discouraged treatment. HWBL_11
Financial barriers also restricted engagement. Many patients sought government services only after depleting resources at private hospitals. The absence of free medicines further diminished trust.
If free medicines are not available, they lose trust in the health system and are discouraged from seeking further treatment. HWBL_05
Similarly, a traditional healer from Jhapa highlighted the role of financial hardship and cultural beliefs in disengagement.
To visit the doctor, you need a bit more money and many people don’t even have money. Now not much money is required for ritual blowing (jharfuk), so they trust it, have blind faith, and go there. So many accidents have occurred going to such places too. KPBL_44
Participants also highlighted compromised services and a lack of patient-friendly environments at health posts. Crowded, noisy facilities made patients anxious and discouraged visits.
Hospitals are noisy and crowded. It increases tension for patients. CGPS_12
Discussion
The findings indicate that access to mental health services in Nepal is constrained by interlinked supply- and demand-side barriers. On the supply side, acceptability is limited by stigma, confidentiality concerns, traditional beliefs and spiritual explanatory models (Kohrt et al., Reference Kohrt, Kunz, Baldwin, Koirala, Sharma and Nepal2005; Luitel et al., Reference Luitel, Lamichhane, Koirala, Sainju, Ghimire and Gautam2025) while privacy, dignity and social status strongly influence help-seeking behaviors (Brenman et al., Reference Brenman, Luitel, Mall and Jordans2014; Gurung et al., Reference Gurung, Poudyal, Wang, Neupane, Bhattarai and Wahid2022). Affordability issues arise from the lack of free medications, out-of-pocket expenses and travel costs, due to under-funding and inconsistent medicine availability (Brenman et al., Reference Brenman, Luitel, Mall and Jordans2014; Paudel et al., Reference Paudel, Chalise, Khatri, Poudel and Khanal2025). Limited outreach and visibility of mental health services compared to physical health programs contribute to reduced approachability, leading to awareness gaps even among educated individuals (Brenman et al., Reference Brenman, Luitel, Mall and Jordans2014; Khanal et al., Reference Khanal, Selvamani and Sapkota2025). Availability and accommodation are hindered by stock-outs, staff transfers, high workloads, inadequate confidential spaces and geographic constraints (Khanal et al., Reference Khanal, Selvamani and Sapkota2025; Paudel et al., Reference Paudel, Chalise, Khatri, Poudel and Khanal2025). Perceived gaps in provider competence and unreliable medication supply compromise appropriateness and trust (Hynie et al., Reference Hynie, Jaimes, Oda, Rivest-Beauregard, Perez Gonzalez and Ives2022). On the demand side, stigma and supernatural beliefs limit perceived need, while mistrust, distance, transportation costs, financial hardship and discontinuity of care impede service uptake and sustained engagement (Gurung et al., Reference Gurung, Poudyal, Wang, Neupane, Bhattarai and Wahid2022; van den Broek et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia and Patel2023).
Low detection of mental health problems by trained PHC workers is a global phenomenon (Fekadu et al., Reference Fekadu, Demissie, Birhane, Medhin, Bitew and Hailemariam2022; Kohrt et al., Reference Kohrt, Gurung, Singh, Rai, Neupane and Turner2025), and Nepal is no exception to this global situation. Existing studies in Nepal have revealed that trained PHC workers were able to detect less than one in four people (Jordans et al., Reference Jordans, Luitel, Kohrt, Rathod, Garman and De Silva2019; Kohrt et al., Reference Kohrt, Ojagbemi, Luitel, Bakolis, Bello and McCrone2025), which is much higher than the rate reported in other countries (Fekadu et al., Reference Fekadu, Demissie, Birhane, Medhin, Bitew and Hailemariam2022). The lack of a confidential space for diagnosis, counseling and treatment, especially for mental healthcare services at local health facilities, has been identified as a major barrier that reduces access to mental healthcare services and increases dropout rates among service users (Luitel et al., Reference Luitel, Jordans, Subba and Komproe2020; Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). Our study also found that the lack of confidential space is a significant barrier preventing service users from seeking mental healthcare treatment, which ultimately impacts the quality and effectiveness of the services provided. The absence of separate and confidential consultation rooms leads to a loss of trust among service users regarding the confidentiality of their information, especially discouraging patients who are concerned about their privacy. This finding is consistent with other studies (Luitel et al., Reference Luitel, Jordans, Subba and Komproe2020; Devkota et al., Reference Devkota, Basnet, Thapa and Subedi2021).
Another supply-side barrier highlighted in the study is the frequent transfer of trained PHC workers in local healthcare facilities. This practice not only disrupts the delivery of mental healthcare services but also contributes to high dropout rates and community mistrust (Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). The shortage of experienced PHC workers in facilities creates challenges in offering consistent mental health services (Jordans et al., Reference Jordans, Luitel, Kohrt, Rathod, Garman and De Silva2019; Luitel et al., Reference Luitel, Breuer, Adhikari, Kohrt, Lund, Komproe and Jordans2020; Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020; Devkota et al., Reference Devkota, Basnet, Thapa and Subedi2021). This issue has been extensively addressed in previous studies and reports on expanding mental health services (Luitel et al., Reference Luitel, Breuer, Adhikari, Kohrt, Lund, Komproe and Jordans2020; Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). The resulting lack of trust between mental health service providers and users due to frequent staff transfers significantly impacts mental health service utilization in Nepal (Devkota et al., Reference Devkota, Basnet, Thapa and Subedi2021).
Demand-side factors also significantly impact the utilization of mental healthcare services. The low perceived need for treatment among individuals seeking help has been consistently identified as a major barrier to accessing mental healthcare services in Nepal, leading to a significant treatment gap (Luitel et al., Reference Luitel, Jordans, Kohrt, Rathod and Komproe2017). Factors such as mental health stigma, lack of awareness and the prioritization of other health issues over mental health contribute to this low perceived need for treatment among service users (Luitel et al., Reference Luitel, Jordans, Kohrt, Rathod and Komproe2017, Reference Luitel, Garman, Jordans and Lund2019; Rai et al., Reference Rai, Gurung and Gautam2021), resulting in delayed or inadequate treatment seeking. Moreover, the perception of ineffective treatment among service users is another barrier to service utilization in Nepal. Studies have shown that the decision to seek mental health treatment and engage with it is closely linked to patients’ concerns about the effectiveness of mental health interventions (Luitel et al., Reference Luitel, Jordans, Kohrt, Rathod and Komproe2017, Reference Luitel, Jordans, Subba and Komproe2020). This perception may be influenced by cultural beliefs about mental health and treatment efficacy, as well as past negative experiences, further discouraging individuals from accessing services (Luitel et al., Reference Luitel, Jordans, Subba and Komproe2020).
The findings of this study could have implications for improving access to mental health services in Nepal. Despite the Government of Nepal’s efforts to integrate mental health into the PHC system, our findings suggest that simply making services available does not automatically lead to increased utilization. This aligns with previous studies that have shown integration efforts facing systemic barriers beyond individual provider skills (Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). Persistent challenges on the supply-side, such as frequent staff turnover, shortages of mhGAP-trained personnel, inadequate supervision structures and insufficient private spaces in health facilities, continue to hinder effective access (Luitel et al., Reference Luitel, Breuer, Adhikari, Kohrt, Lund, Komproe and Jordans2020). Addressing these issues requires strengthening workforce stability by integrating WHO mhGAP training into the pre-service education of future healthcare providers, providing in-service clinical supervision and refresher training and strengthening local governance to ensure the stable placement of trained PHC workers at the community level. Additionally, establishing supportive supervision mechanisms and upgrading infrastructure to include confidential consultation rooms are essential (Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). Second, ensuring a reliable supply chain of psychotropic medicines is crucial. Frequent stock-outs and short expiry periods disrupt treatment continuity and discourage ongoing care. The Nepal health facility survey has reported low psychotropic medicine readiness scores (around 30%), indicating weaknesses in procurement and distribution systems (Acharya et al., Reference Acharya, Singh, Karki, Cleary and Thapa2025). Third, financial reforms are necessary to reduce out-of-pocket expenses for medications, transportation and referrals. Many patients turn to traditional healers or discontinue biomedical treatment due to the high costs involved (Dhimal et al., Reference Dhimal, Dahal, Adhikari, Koirala, Bista and Luitel2022). Strengthening national health insurance programs by including psychotropic medicines and subsidizing travel expenses for specialist referrals could help alleviate the burden of catastrophic health expenditures. These priorities are in line with WHO recommendations and recent analyses of systemic constraints in Nepal (Paudel et al., Reference Paudel, Chalise, Khatri, Poudel and Khanal2025).
On the demand side, addressing stigma, cultural explanatory models of mental health problems and low levels of mental health literacy is equally critical. Stigma remains a dominant barrier, contributing to delayed care-seeking and high dropout rates (Upadhaya et al., Reference Upadhaya, Regmi, Gurung, Luitel, Petersen, Jordans and Komproe2020). Community-based programs, including anti-stigma activities delivered by trusted local actors such as FCHVs, teachers, religious leaders and community representatives, could encourage early identification and help-seeking behaviors. To overcome geographical barriers and challenges in follow-up care, telepsychiatry and structured teleconsultation using e-mhGAP tools (Kohrt et al., Reference Kohrt, Ojagbemi, Luitel, Bakolis, Bello and McCrone2025) can extend specialist input to peripheral facilities and support continuity of care when trained staff are rotated (Shakya, Reference Shakya2021). Early pilots of mobile-based mhGAP tools in Nepal demonstrate feasibility, acceptability and the potential to improve diagnostic consistency; however, sustained investments in digital infrastructure and supervision fidelity remain essential (Luitel et al., Reference Luitel, Pudasaini, Pokhrel, Lamichhane, Gautam and Adhikari2023). Finally, aligning national mhGAP roll-out with the updated 2023 WHO guidelines (WHO, 2023) and Nepal’s evolving National Mental Health Strategy and Action Plan (MoHP, 2020) can help standardize care pathways and strengthen accountability across federal, provincial and municipal tiers.
Several limitations warrant consideration. First, although the study was conducted in three districts covering the eastern, central and western parts of the country, considering the diversity of Nepal in terms of geography, culture, caste/ethnicity and languages, the result of the study may not be representative of the entire country. Second, social desirability and fear of disclosure may have led to under-reporting of stigma or provider behaviors, particularly given confidentiality concerns that participants themselves described. Third, as the study was conducted in the districts where mental health services were available, the results could be different in the districts where those services are not available. Fourth, in this study, our focus was primary with depression; the challenges and barriers reported in this study could be different for other disorders, particularly for severe mental health problems.
Finally, while we used Levesque’s framework to synthesize the results, this framework does not explicitly capture multiple dimensions of help-seeking barriers, such as external and internal contextual factors, the intervention itself, its implementation and interactions between users and the intervention.
Conclusion
This study reveals persistent and inter-related supply- and demand-side barriers that significantly hinder access to mental healthcare in Nepal. On the supply side, challenges include inconsistent staffing, frequent medication shortages, inadequate infrastructure and limited prioritization of mental health within the health system. Demand-side barriers are shaped by stigma, cultural misconceptions, financial hardship and geographic inaccessibility. Addressing these obstacles requires a coordinated, multi-sectoral/multi-level response: strengthening health system capacity through workforce development, reliable procurement and distribution of psychotropic medications and improved clinical infrastructure; coordination and collaboration with non-health sectors, alongside targeted community-level strategies such as culturally sensitive awareness campaigns, stigma reduction initiatives, financial protection measures and active community engagement. Closing Nepal’s mental health treatment gap demands a comprehensive, integrated approach that not only addresses structural limitations but also respects socio-cultural realities.
Abbreviations
- FCHV
-
Female Community Health Volunteer
- HP
-
Health Post
- mhGAP-IG
-
Mental Health Gap Action Programme Intervention Guide
- NGO
-
Non-governmental Organization
- OPD
-
Outpatient Department
- PHC
-
Primary Healthcare
- WHO
-
World Health Organization
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10236.
Data availability statement
Interested individuals can contact the principal investigator of this study to express their interest in collaboration and request access to the dataset analyzed here by emailing: luitelnp@gmail.com.
Acknowledgements
We are grateful to the participants for sharing valuable information, even on personal matters. This study would not have been possible without their cooperation. We would like to thank Dr. Sandarba Adhikari and Dr. Avash Niraula for their support in identifying participants for interviews. We also thank Ms. Kabita Sah for her support in data entry.
Author contribution
N.P.L. designed the study, supervised data collection, and drafted the manuscript. P.S. and B.L. conducted interviews and were involved in data analysis. R.K. supported data analysis and contributed to drafting the manuscript. K.G. provided input and feedback on the study design and manuscript development. All authors reviewed and approved the final version of the manuscript.
Financial support
This work was supported by the National Institute for Health Research (NIHR) (using the UK’s Official Development Assistance (ODA) Funding) and Wellcome [222001_Z_20_Z] under the NIHR-Wellcome Partnership for Global Health Research. The views expressed are those of the authors and not necessarily those of Wellcome, the NIHR or the Department of Health and Social Care.
Competing interests
The authors declare that they have no competing interests.
Ethics statements
This study was conducted in compliance with the Declaration of Helsinki and received ethical approval from the Nepal Health Research Council (NHRC) (Registration number: 527/2022 P). Each participant signed a written informed consent form before enrolling in the study. Only those who voluntarily agreed to participate were included in the study.

 Open access
Open access
Comments
3 February 2026
Kathmandu, Nepal
To:
The Editor-in-Chief
Cambridge Prisms: Global Mental Health
Re: Submission of manuscript titled “Breaking down barriers: a qualitative study of demand- and supply-side barriers to depression care in Nepal”
Dear Editor-in-Chief,
I am pleased to submit our manuscript, “Breaking down barriers: a qualitative study of demand- and supply-side barriers to depression care in Nepal” for consideration in Cambridge Prisms: Global Mental Health.
Depression remains a major public health concern globally, particularly in low- and middle-income countries such as Nepal, where access to mental health services is limited. While global initiatives often prioritize strengthening supply-side factors—such as expanding service availability and building workforce capacity through task-sharing—evidence indicates that supply-side improvements alone may be insufficient to narrow the treatment gap. Barriers are frequently oversimplified by combining both demand- and supply-side constraints, masking the distinct strategies required to effectively address each. Public education and anti-stigma efforts can increase willingness to seek care, whereas culturally sensitive and contextually grounded service delivery approaches can enhance the effectiveness of available services. In this study, we explored multi-stakeholder perceptions and experiences related to these barriers in Nepal.
Our findings highlight a complex interplay of persistent supply- and demand-side barriers that hinder access to depression care. Supply-side challenges include inconsistent staffing, recurrent medication stockouts, inadequate infrastructure, and limited prioritization of mental health within the broader health system. Demand-side barriers are shaped by stigma, cultural beliefs, financial constraints, and geographic inaccessibility. Addressing these barriers requires a coordinated, multi-sectoral and multi-level response—one that strengthens health system capacity, ensures a reliable supply chain for psychotropic medications, and improves infrastructure, while simultaneously promoting culturally sensitive awareness campaigns, stigma reduction efforts, financial protection mechanisms, and active community engagement. Closing Nepal’s mental health treatment gap will require an integrated approach that addresses structural limitations while also respecting socio-cultural contexts.
We affirm that the work presented in this manuscript is original, has not been published previously, and is not under consideration by any other journal. The authors declare that they have no competing interests to disclose.
We hope that our findings will contribute meaningfully to the growing body of global mental health literature and inform more effective strategies for improving access to depression care in similar resource-limited settings. We respectfully request that you consider our manuscript for publication in Cambridge Prisms: Global Mental Health.
Thank you for your consideration.
Yours sincerely,
Nagendra P. Luitel (luitelnp@gmail.com)
Poonam Sainju
Bishnu Lamichhane
Rajen Khadgi
Kamal Gautam